
Angiotensin-Converting Enzyme 2 Protein Is Overexpressed in a Wide Range of Human Tumour Types: A Systematic Tissue Microarray Study on >15,000 Tumours

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Microarray
2.2. Immunohistochemistry
2.3. Statistics
3. Results
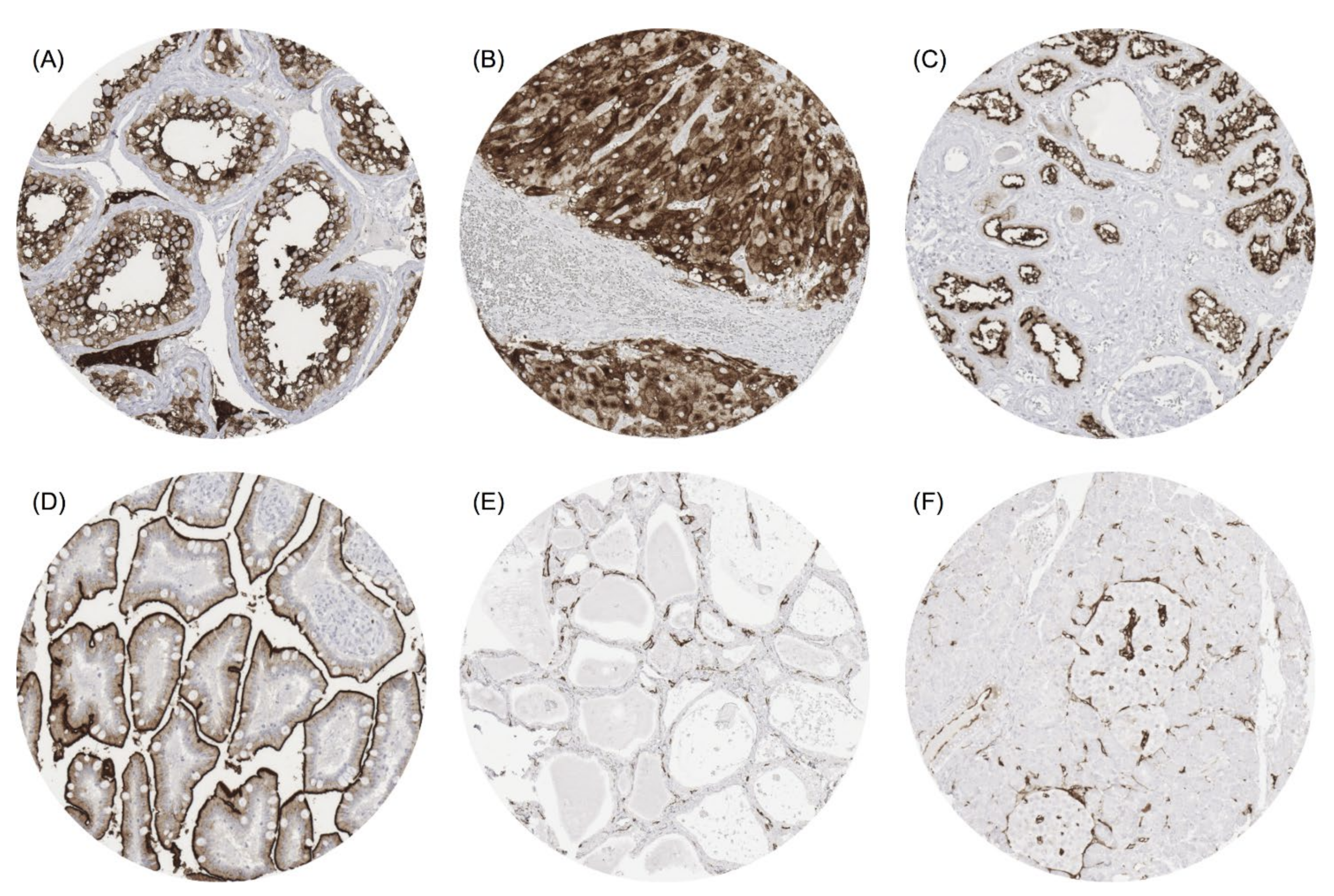
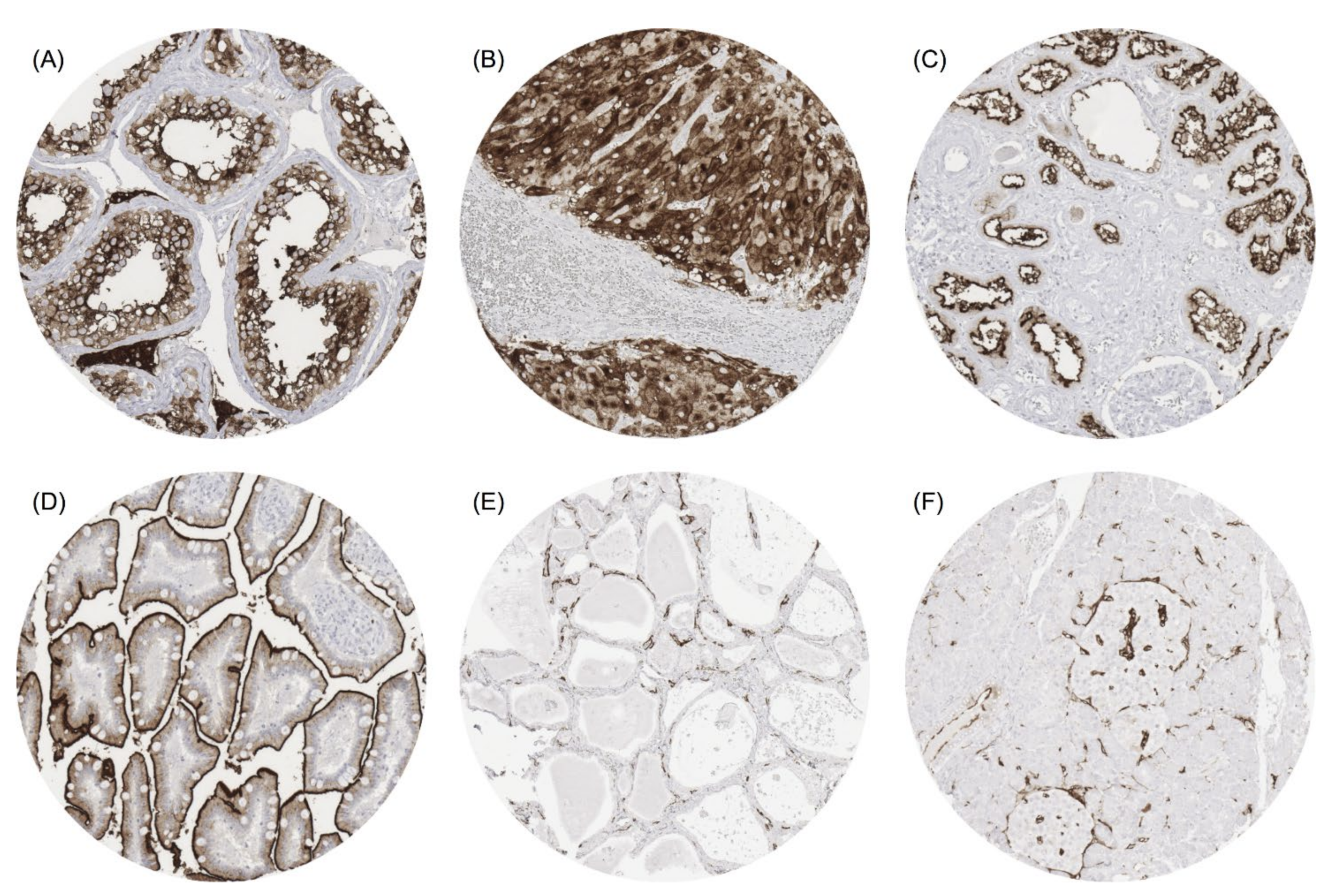
3.1. ACE2 in Normal Tissue
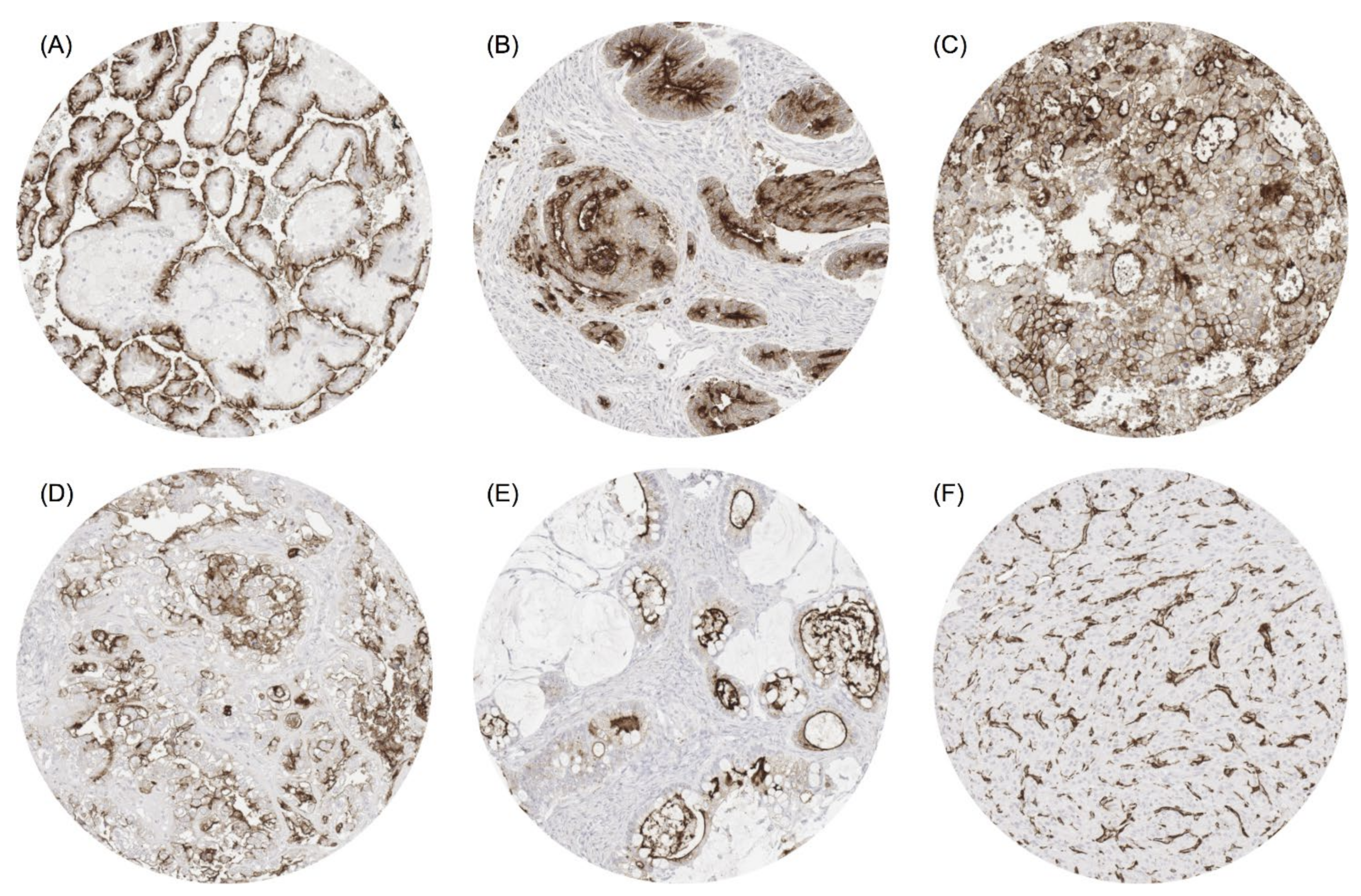
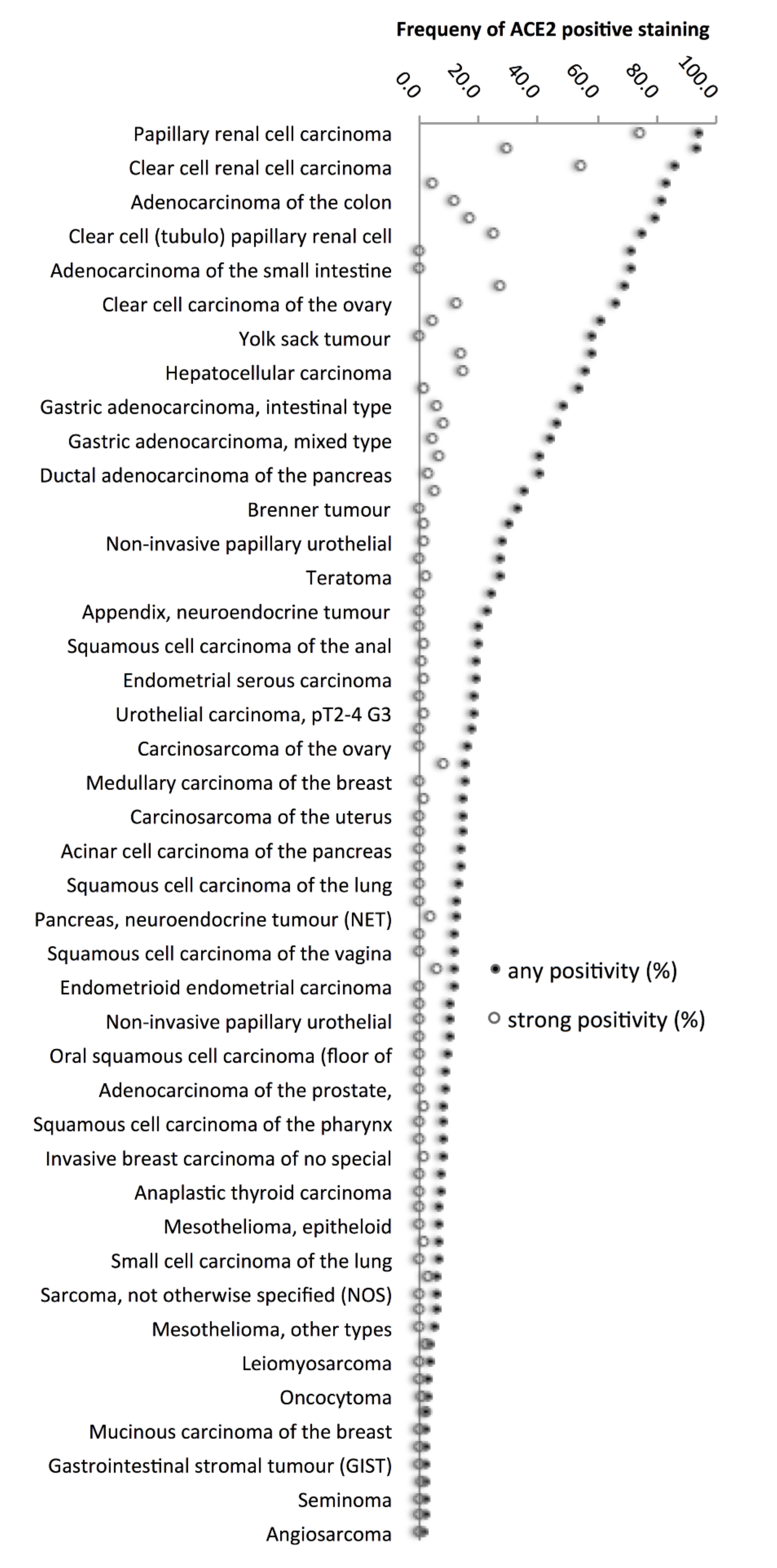
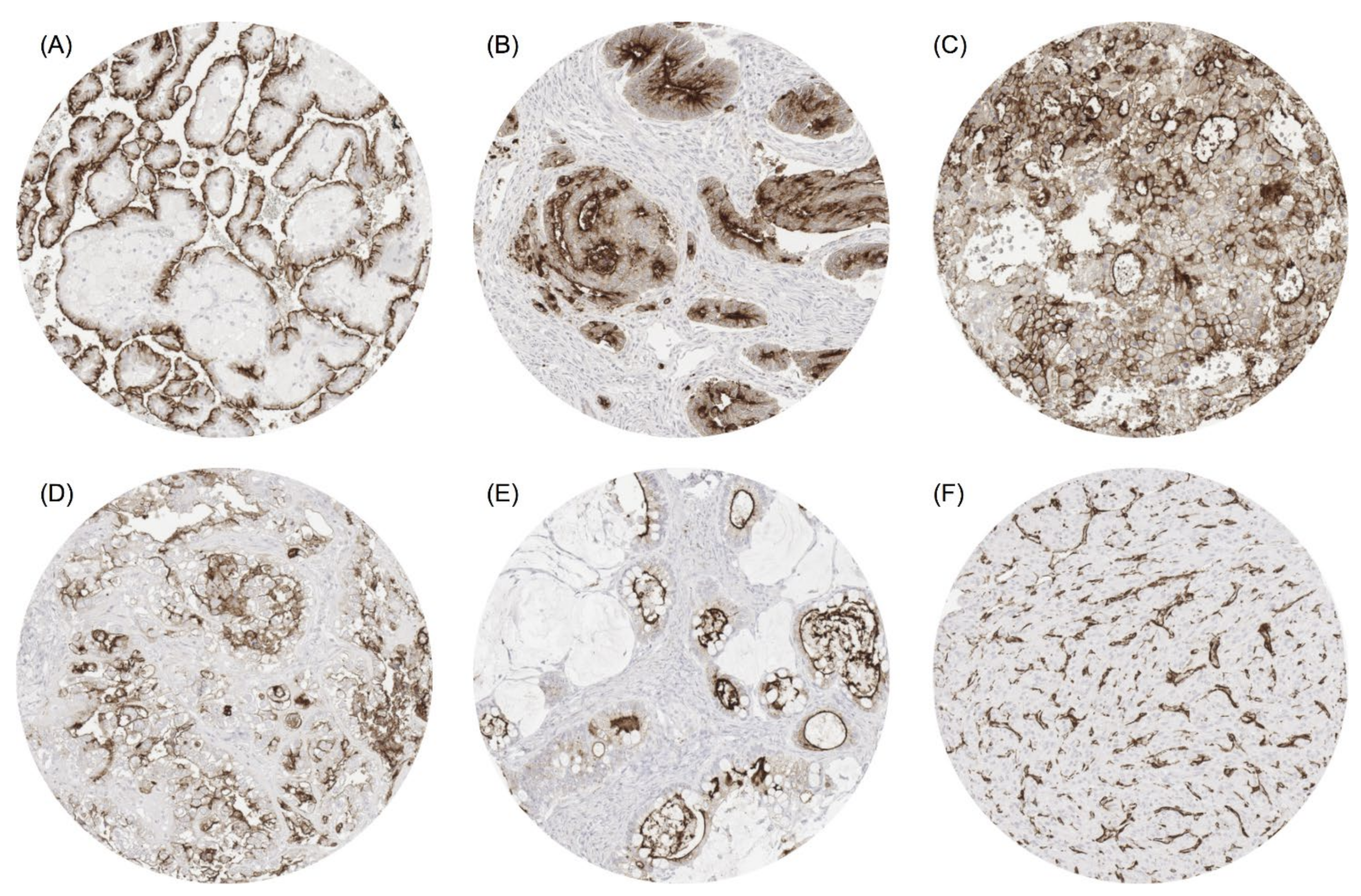
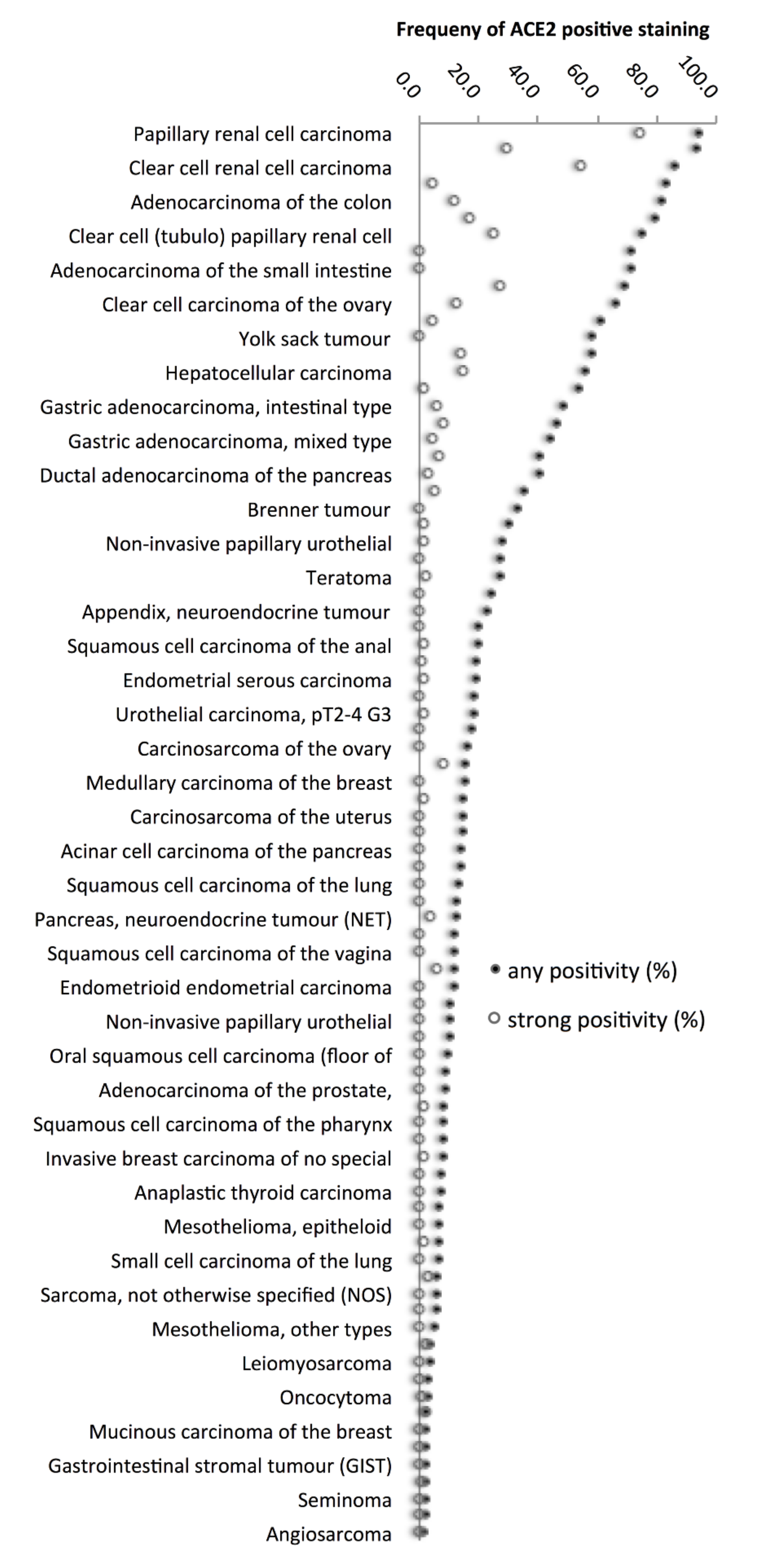
3.2. ACE2 in Cancer
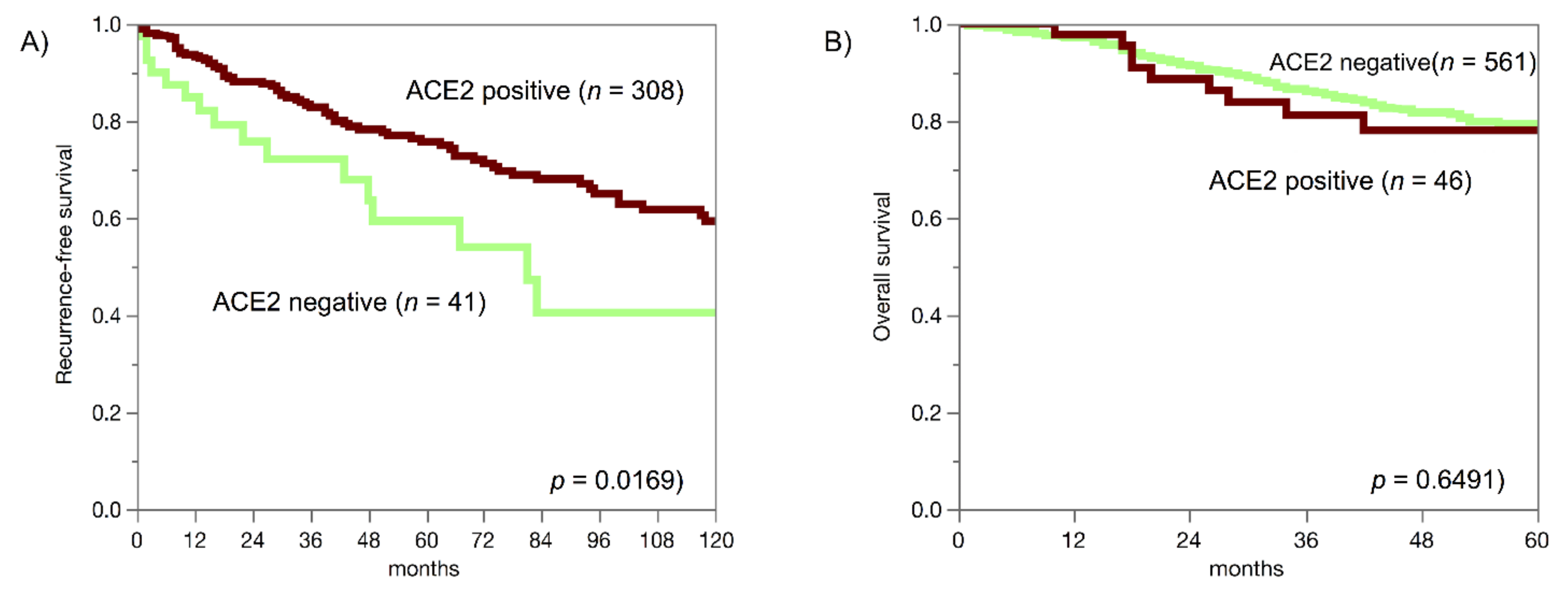
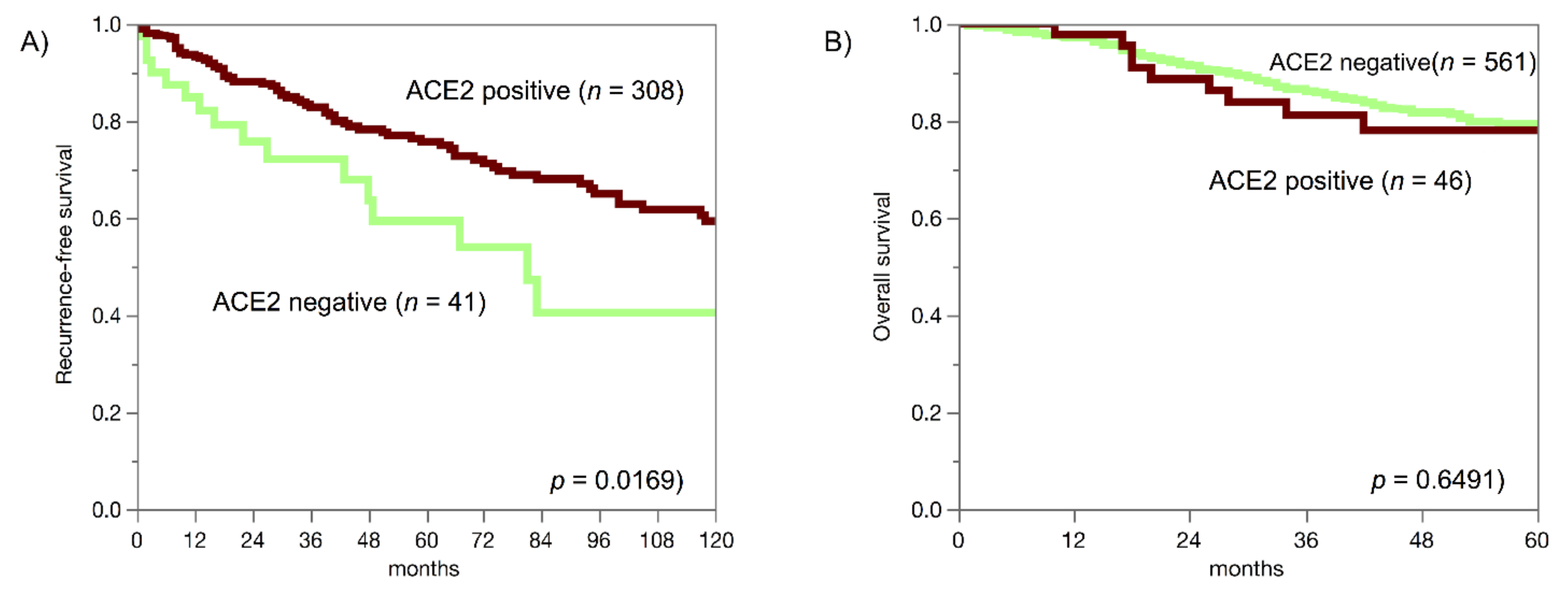
3.3. ACE2, Cancer Phenotype and Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donoghue, M.; Hsieh, F.; Baronas, E.; Godbout, K.; Gosselin, M.; Stagliano, N.; Donovan, M.; Woolf, B.; Robison, K.; Jeyaseelan, R.; et al. A Novel Angiotensin-Converting Enzyme–Related Carboxypeptidase (ACE2) Converts Angiotensin I to Angiotensin 1–9. Circ. Res. 2000, 87, E1–E9. [Google Scholar] [CrossRef]
- Tipnis, S.R.; Hooper, N.M.; Hyde, R.; Karran, E.; Christie, G.; Turner, A.J. A human homolog of angiotensin-converting enzyme. Cloning and functional expression as a captopril-insensitive carboxypeptidase. J. Biol. Chem. 2000, 275, 33238–33243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Han, T.; Kang, J.; Li, G.; Ge, J.; Gu, J. Analysis of 2019-nCoV receptor ACE2 expression in different tissues and its significance study. Ann. Transl. Med. 2020, 8, 1077. [Google Scholar] [CrossRef] [PubMed]
- Hikmet, F.; Méar, L.; Edvinsson, Å.; Micke, P.; Uhlén, M.; Lindskog, C. The protein expression profile of ACE2 in human tissues. Mol. Syst. Biol. 2020, 16, e9610. [Google Scholar] [CrossRef]
- Vickers, C.; Hales, P.; Kaushik, V.; Dick, L.; Gavin, J.; Tang, J.; Godbout, K.; Parsons, T.; Baronas, E.; Hsieh, F.; et al. Hydrolysis of biological peptides by human angiotensin-converting enzyme-related carboxypeptidase. J. Biol. Chem. 2002, 277, 14838–14843. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, S.C.; Deshmukh, V.; Creighton, C.J.; Patil, A. Renal Carcinoma Is Associated with Increased Risk of Coronavirus Infections. Front. Mol. Biosci. 2020, 7, 579422. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, L.; Li, M.; Wang, X. The SARS-CoV-2 host cell receptor ACE2 correlates positively with immunotherapy response and is a potential protective factor for cancer progression. Comput. Struct. Biotechnol. J. 2020, 18, 2438–2444. [Google Scholar] [CrossRef]
- Samad, A.; Jafar, T.; Rafi, J.H. Identification of angiotensin-converting enzyme 2 (ACE2) protein as the potential biomarker in SARS-CoV-2 infection-related lung cancer using computational analyses. Genomics 2020, 112, 4912–4923. [Google Scholar] [CrossRef]
- Song, J.; Han, J.; Liu, F.; Chen, X.; Qian, S.; Wang, Y.; Jia, Z.; Duan, X.; Zhang, X.; Zhu, J. Systematic Analysis of Coronavirus Disease 2019 (COVID-19) Receptor ACE2 in Malignant Tumors: Pan-Cancer Analysis. Front. Mol. Biosci. 2020, 7, 569414. [Google Scholar] [CrossRef]
- Tang, Q.; Wang, Y.; Ou, L.; Li, J.; Zheng, K.; Zhan, H.; Gu, J.; Zhou, G.; Xie, S.; Zhang, J.; et al. Downregulation of ACE2 expression by SARS-CoV-2 worsens the prognosis of KIRC and KIRP patients via metabolism and immunoregulation. Int. J. Biol. Sci. 2021, 17, 1925–1939. [Google Scholar] [CrossRef] [PubMed]
- Narayan, S.S.; Lorenz, K.; Ukkat, J.; Hoang-Vu, C.; Trojanowicz, B. Angiotensin converting enzymes ACE and ACE2 in thyroid cancer progression. Neoplasma 2020, 67, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Tang, W.; Wang, Y.; Shen, Q.; Wang, B.; Cai, C.; Meng, X.; Zou, F. Downregulation of ACE2/Ang-(1-7)/Mas axis promotes breast cancer metastasis by enhancing store-operated calcium entry. Cancer Lett. 2016, 376, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yang, Z.L.; Ren, X.; Zou, Q.; Yuan, Y.; Liang, L.; Chen, M.; Chen, S. ACE2 and FZD1 are prognosis markers in squamous cell/adenosquamous carcinoma and adenocarcinoma of gallbladder. J. Mol. Histol. 2014, 45, 47–57. [Google Scholar] [CrossRef]
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Singh, C.; Aneja, R. SARS-CoV-2 Infection in Cancer Patients: Effects on Disease Outcomes and Patient Prognosis. Cancers 2020, 12, 3266. [Google Scholar] [CrossRef]
- Gosain, R.; Abdou, Y.; Singh, A.; Rana, N.; Puzanov, I.; Ernstoff, M.S. COVID-19 and Cancer: A Comprehensive Review. Curr. Oncol. Rep. 2020, 22, 53. [Google Scholar] [CrossRef]
- Liu, C.; Wang, K.; Zhang, M.; Hu, X.; Hu, T.; Liu, Y.; Hu, Q.; Wu, S.; Yue, J. High expression of ACE2 and TMPRSS2 and clinical characteristics of COVID-19 in colorectal cancer patients. NPJ Precis. Oncol. 2021, 5, 1. [Google Scholar] [CrossRef]
- Menz, A.; Bauer, R.; Kluth, M.; Marie von Bargen, C.; Gorbokon, N.; Viehweger, F.; Lennartz, M.; Völkl, C.; Fraune, C.; Uhlig, R.; et al. Diagnostic and prognostic impact of cytokeratin 19 expression analysis in human tumors: A tissue microarray study of 13,172 tumors. Hum. Pathol. 2021, 115, 19–36. [Google Scholar] [CrossRef]
- Weidemann, S.; Gagelmann, P.; Gorbokon, N.; Lennartz, M.; Menz, A.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Blessin, N.C.; Fraune, C.; et al. Mesothelin Expression in Human Tumors: A Tissue Microarray Study on 12,679 Tumors. Biomedicines 2021, 9, 397. [Google Scholar] [CrossRef]
- Dancau, A.M.; Simon, R.; Mirlacher, M.; Sauter, G. Tissue Microarrays. Methods Mol. Biol. 2016, 1381, 53–65. [Google Scholar] [CrossRef]
- Kononen, J.; Bubendorf, L.; Kallioniemi, A.; Barlund, M.; Schraml, P.; Leighton, S.; Torhorst, J.; Mihatsch, M.J.; Sauter, G.; Kallioniemi, O.P. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat. Med. 1998, 4, 844–847. [Google Scholar] [CrossRef]
- Menz, A.; Weitbrecht, T.; Gorbokon, N.; Büscheck, F.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Hinsch, A.; Höflmayer, D.; Weidemann, S.; et al. Diagnostic and prognostic impact of cytokeratin 18 expression in human tumors: A tissue microarray study on 11,952 tumors. Mol. Med. 2021, 27, 16. [Google Scholar] [CrossRef]
- Aitken, R.J. COVID-19 and human spermatozoa-Potential risks for infertility and sexual transmission? Andrology 2021, 9, 48–52. [Google Scholar] [CrossRef]
- Wong, T.C.; Lee, Z.Y.; Sia, T.L.L.; Chang, A.K.W.; Chua, H.H. Miscarriage Risk in COVID-19 Infection. SN Compr. Clin. Med. 2020, 2, 1449–1452. [Google Scholar] [CrossRef]
- Nair, M.G.; Prabhu, J.S.; Ts, S. High expression of ACE2 in HER2 subtype of breast cancer is a marker of poor prognosis. Cancer Treat. Res. Comun. 2021, 27, 100321. [Google Scholar] [CrossRef]
- Feng, Y.; Ni, L.; Wan, H.; Fan, L.; Fei, X.; Ma, Q.; Gao, B.; Xiang, Y.; Che, J.; Li, Q. Overexpression of ACE2 produces antitumor effects via inhibition of angiogenesis and tumor cell invasion in vivo and in vitro. Oncol. Rep. 2011, 26, 1157–1164. [Google Scholar] [CrossRef]
- Yang, J.; Li, H.; Hu, S.; Zhou, Y. ACE2 correlated with immune infiltration serves as a prognostic biomarker in endometrial carcinoma and renal papillary cell carcinoma: Implication for COVID-19. Aging 2020, 12, 6518–6535. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M. COVID-19 and the endocrine system: Exploring the unexplored. J. Endocrinol. Investig. 2020, 43, 1027–1031. [Google Scholar] [CrossRef]
- Lundholm, M.D.; Poku, C.; Emanuele, N.; Emanuele, M.A.; Lopez, N. SARS-CoV-2 (COVID-19) and the Endocrine System. J. Endocr. Soc. 2020, 4, bvaa144. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumour Type | Fraction of Tumours (%) with ACE2-Positive Blood Vessels |
|---|---|
| Pancreas, neuroendocrine tumour | 70.3 |
| Adenoma of the thyroid gland | 52.8 |
| Medullary thyroid carcinoma | 48.4 |
| Ileum, neuroendocrine tumour | 43.2 |
| Lung, neuroendocrine tumour | 35.3 |
| Adrenal cortical adenoma | 34.1 |
| Follicular thyroid carcinoma | 27.7 |
| Ganglioneuroma | 25.0 |
| Pancreas, neuroendocrine carcinoma | 21.4 |
| Colorectal, neuroendocrine tumour | 20.0 |
| Colorectal, neuroendocrine carcinoma | 20.0 |
| Papillary thyroid carcinoma | 16.5 |
| Gastrointestinal stromal tumour | 16.3 |
| Oncocytoma | 15.5 |
| Chromophobe renal cell carcinoma | 11.3 |
| Paraganglioma | 10.8 |
| Leiomyoma | 8.3 |
| Adrenal cortical carcinoma | 7.7 |
| Teratoma | 6.8 |
| Embryonal carcinoma of the testis | 5.0 |
| Warthin tumour of the parotid gland | 4.5 |
| Mesothelioma, epitheloid | 3.3 |
| Pancreatic/Ampullary adenocarcinoma | 2.6 |
| Yolk sack tumour | 2.6 |
| Leiomyosarcoma | 2.4 |
| Seminoma | 2.4 |
| Adenocarcinoma of the prostate (recurrence) | 2.4 |
| Endometrioid carcinoma of the ovary | 2.1 |
| Ductal adenocarcinoma of the pancreas | 1.8 |
| Mucinous carcinoma of the ovary | 1.3 |
| Adenocarcinoma of the prostate, Gleason 5+5 | 1.3 |
| Hodgkin Lymphoma | 1.2 |
| Clear cell renal cell carcinoma | 0.2 |
| Cancer | Phenotype | Class | N | Negative | Weak | Moderate | Strong | p |
|---|---|---|---|---|---|---|---|---|
| Invasive breast carcinoma of no special type | Total | 1213 | 92.2 | 4.1 | 2 | 1.7 | ||
| Tumour stage | pT1 | 599 | 93.8 | 2.7 | 2 | 1.5 | 0.0903 | |
| pT2 | 412 | 90.8 | 5.8 | 1.9 | 1.5 | |||
| pT3-4 | 86 | 87.2 | 8.1 | 1.2 | 3.5 | |||
| Grade | G1 | 179 | 98.9 | 0.6 | 0.6 | 0 | <0.0001 | |
| G2 | 584 | 95.7 | 1.9 | 1 | 1.4 | |||
| G3 | 376 | 83.2 | 9.8 | 3.7 | 3.2 | |||
| Nodal stage | pN0 | 514 | 91.6 | 3.3 | 3.3 | 1.8 | 0.0959 | |
| pN1 | 227 | 93.4 | 4.4 | 0.9 | 1.3 | |||
| pN2 | 70 | 90 | 5.7 | 1.4 | 2.9 | |||
| pN3 | 54 | 85.2 | 11.1 | 0 | 3.7 | |||
| HER2 status | Negative | 850 | 93.6 | 3.2 | 1.6 | 1.5 | <0.0001 | |
| Positive | 119 | 79.8 | 13.4 | 4.2 | 2.5 | |||
| ER status | Negative | 202 | 67.8 | 15.8 | 8.4 | 7.9 | <0.0001 | |
| Positive | 715 | 98.5 | 1.3 | 0.1 | 0.1 | |||
| PR status | Negative | 391 | 80.6 | 10.2 | 4.9 | 4.3 | <0.0001 | |
| Positive | 569 | 99.1 | 0.7 | 0.2 | 0 | |||
| Triple negative | No | 753 | 96 | 2.8 | 0.7 | 0.5 | <0.0001 | |
| Yes | 135 | 67.4 | 14.1 | 9.6 | 8.9 | |||
| Colorectal adenocarcinoma | Total | 1645 | 18.7 | 43.5 | 26.2 | 11.7 | ||
| Tumour stage | pT1 | 63 | 7.9 | 46 | 28.6 | 17.5 | 0.0004 | |
| pT2 | 309 | 17.5 | 40.8 | 28.5 | 13.3 | |||
| pT3 | 867 | 16.8 | 44.1 | 27.2 | 11.9 | |||
| pT4 | 315 | 27.9 | 42.9 | 20.3 | 8.9 | |||
| Nodal stage | pN0 | 798 | 17.9 | 41.6 | 27.8 | 12.7 | 0.1796 | |
| pN+ | 741 | 20.2 | 44.7 | 24.3 | 10.8 | |||
| Localization | Left colon | 1129 | 16.6 | 42.5 | 26.9 | 14 | <0.0001 | |
| Right colon | 432 | 25.2 | 45.6 | 23.1 | 6 | |||
| MMR status | Defective | 73 | 49.3 | 38.4 | 11 | 1.4 | <0.0001 | |
| Proficient | 1065 | 14.2 | 44.2 | 28.8 | 12.8 | |||
| RAS status | Mutated | 302 | 20.9 | 47.7 | 23.2 | 8.3 | 0.0004 | |
| Wild type | 419 | 13.4 | 41.5 | 29.4 | 15.8 | |||
| BRAF status | Mutated | 18 | 66.7 | 27.8 | 5.6 | 0 | 0.0002 | |
| Wild type | 112 | 17.9 | 45.5 | 24.1 | 12.5 | |||
| Clear cell renal cell carcinomas | Total | 572 | 14.3 | 17.8 | 13.6 | 54.2 | ||
| ISUP stage | 1 | 181 | 9.9 | 26.5 | 13.8 | 49.7 | <0.0001 | |
| 2 | 182 | 8.8 | 15.4 | 15.4 | 60.4 | |||
| 3 | 165 | 18.2 | 9.1 | 13.9 | 58.8 | |||
| 4 | 36 | 50 | 27.8 | 2.8 | 19.4 | |||
| Fuhrman grade | 1 | 26 | 11.5 | 19.2 | 15.4 | 53.8 | <0.0001 | |
| 2 | 332 | 8.4 | 20.2 | 15.1 | 56.3 | |||
| 3 | 169 | 17.2 | 13 | 13 | 56.8 | |||
| 4 | 44 | 50 | 18.2 | 4.5 | 27.3 | |||
| Thoenes grade | 1 | 202 | 8.9 | 23.8 | 15.3 | 52 | <0.0001 | |
| 2 | 314 | 12.7 | 14.3 | 14 | 58.9 | |||
| 3 | 55 | 43.6 | 16.4 | 5.5 | 34.5 | |||
| UICC stage | 1 | 255 | 11.8 | 18.8 | 15.7 | 53.7 | 0.2557 | |
| 2 | 27 | 14.8 | 11.1 | 7.4 | 66.7 | |||
| 3 | 73 | 19.2 | 12.3 | 12.3 | 56.2 | |||
| 4 | 61 | 23 | 18 | 8.2 | 50.8 | |||
| pT stage | pT1 | 333 | 11.4 | 19.2 | 16.5 | 52.9 | 0.068 | |
| pT2 | 58 | 12.1 | 19 | 8.6 | 60.3 | |||
| pT3-4 | 176 | 19.3 | 14.8 | 10.2 | 55.7 | |||
| pN stage | pN0 | 98 | 22.4 | 14.3 | 12.2 | 51 | 0.342 | |
| pN ≥ 1 | 11 | 27.3 | 0 | 18.2 | 54.5 | |||
| Endometroid endometrial carcinoma | Total | 222 | 88.3 | 11.7 | 0 | 0 | ||
| Tumour stage | pT1 | 111 | 90.1 | 9.9 | 0 | 0 | 0.3277 | |
| pT2 | 24 | 79.2 | 20.8 | 0 | 0 | |||
| pT3-4 | 33 | 84.8 | 15.2 | 0 | 0 | |||
| Nodal stage | pN0 | 50 | 78 | 22 | 0 | 0 | 0.0651 | |
| pN+ | 29 | 93.1 | 6.9 | 0 | 0 | |||
| Serous ovarian carcinomas | Total | 474 | 89.7 | 10.3 | 0 | 0 | ||
| Tumour stage | pT1 | 29 | 93.1 | 6.9 | 0 | 0 | 0.5892 | |
| pT2 | 41 | 87.8 | 12.2 | 0 | 0 | |||
| pT3 | 244 | 86.9 | 13.1 | 0 | 0 | |||
| Nodal stage | pN0 | 74 | 90.5 | 9.5 | 0 | 0 | 0.737 | |
| pN1 | 156 | 89.1 | 10.9 | 0 | 0 | |||
| Pancreatic ductal adenocarcinomas | Total | 454 | 59.7 | 32.4 | 4.8 | 3.1 | ||
| Tumour stage | pT1 | 13 | 46.2 | 46.2 | 0 | 7.7 | 0.5988 | |
| pT2 | 54 | 57.4 | 31.5 | 5.6 | 5.6 | |||
| pT3 | 302 | 63.9 | 29.8 | 4 | 2.3 | |||
| pT4 | 19 | 57.9 | 36.8 | 0 | 5.3 | |||
| Grade | 1 | 13 | 53.8 | 23.1 | 15.4 | 7.7 | 0.612 | |
| 2 | 270 | 63 | 31.5 | 3 | 2.6 | |||
| 3 | 83 | 61.4 | 31.3 | 3.6 | 3.6 | |||
| Nodal stage | pN0 | 81 | 69.1 | 25.9 | 2.5 | 2.5 | 0.4772 | |
| pN+ | 305 | 60 | 32.5 | 4.3 | 3.3 | |||
| Thyroid carcinomas | Papillary | Total | 357 | 92.2 | 7.6 | 0.3 | 0 | |
| Tumour stage | pT1 | 114 | 92.1 | 7.9 | 0 | 0 | 0.1363 | |
| pT2 | 64 | 85.9 | 14.1 | 0 | 0 | |||
| pT3-4 | 84 | 95.2 | 4.8 | 0 | 0 | |||
| Nodal stage | pN0 | 76 | 92.1 | 7.9 | 0 | 0 | 0.126 | |
| pN+ | 105 | 97.1 | 2.9 | 0 | 0 | |||
| Follicular | Total | 141 | 80.1 | 19.9 | 0 | 0 | ||
| Tumour stage | pT1 | 11 | 72.7 | 27.3 | 0 | 0 | 0.5715 | |
| pT2 | 29 | 69 | 31 | 0 | 0 | |||
| pT3-4 | 31 | 80.6 | 19.4 | 0 | 0 | |||
| Nodal stage | pN0 | 22 | 90.9 | 9.1 | 0 | 0 | 0.5462 | |
| pN+ | 2 | 100 | 0 | 0 | 0 |
| Cancer | Phenotype | Class | N | Negative | Positive | p |
|---|---|---|---|---|---|---|
| Papillary thyroid carcinoma | Tumour stage | pT1 | 139 | 79.9 | 20.1 | 0.0446 |
| pT2 | 76 | 81.6 | 18.4 | |||
| pT3-4 | 92 | 91.3 | 8.7 | |||
| Nodal stage | pN0 | 84 | 89.3 | 10.7 | 0.933 | |
| pN+ | 116 | 89.7 | 10.3 | |||
| Neuroendocrine tumour | Total | 133 | 53.4 | 46.6 | 0.0006 | |
| Neuroendocrine cancer | Total | 25 | 88 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meiners, J.; Jansen, K.; Gorbokon, N.; Büscheck, F.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Höflmayer, D.; Weidemann, S.; Fraune, C.; et al. Angiotensin-Converting Enzyme 2 Protein Is Overexpressed in a Wide Range of Human Tumour Types: A Systematic Tissue Microarray Study on >15,000 Tumours. Biomedicines 2021, 9, 1831. https://doi.org/10.3390/biomedicines9121831
Meiners J, Jansen K, Gorbokon N, Büscheck F, Luebke AM, Kluth M, Hube-Magg C, Höflmayer D, Weidemann S, Fraune C, et al. Angiotensin-Converting Enzyme 2 Protein Is Overexpressed in a Wide Range of Human Tumour Types: A Systematic Tissue Microarray Study on >15,000 Tumours. Biomedicines. 2021; 9(12):1831. https://doi.org/10.3390/biomedicines9121831
Chicago/Turabian StyleMeiners, Jan, Kristina Jansen, Natalia Gorbokon, Franziska Büscheck, Andreas M. Luebke, Martina Kluth, Claudia Hube-Magg, Doris Höflmayer, Sören Weidemann, Christoph Fraune, and et al. 2021. "Angiotensin-Converting Enzyme 2 Protein Is Overexpressed in a Wide Range of Human Tumour Types: A Systematic Tissue Microarray Study on >15,000 Tumours" Biomedicines 9, no. 12: 1831. https://doi.org/10.3390/biomedicines9121831
APA StyleMeiners, J., Jansen, K., Gorbokon, N., Büscheck, F., Luebke, A. M., Kluth, M., Hube-Magg, C., Höflmayer, D., Weidemann, S., Fraune, C., Möller, K., Bernreuther, C., Lebok, P., Menz, A., Jacobsen, F., Clauditz, T., Sauter, G., Uhlig, R., Wilczak, W., ... Steurer, S. (2021). Angiotensin-Converting Enzyme 2 Protein Is Overexpressed in a Wide Range of Human Tumour Types: A Systematic Tissue Microarray Study on >15,000 Tumours. Biomedicines, 9(12), 1831. https://doi.org/10.3390/biomedicines9121831