The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity



Abstract
1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Laparoscopic Sleeve Gastrectomy (SG)
2.3. Chemicals and Instruments
2.4. Preparation and Treatments of Whole Blood
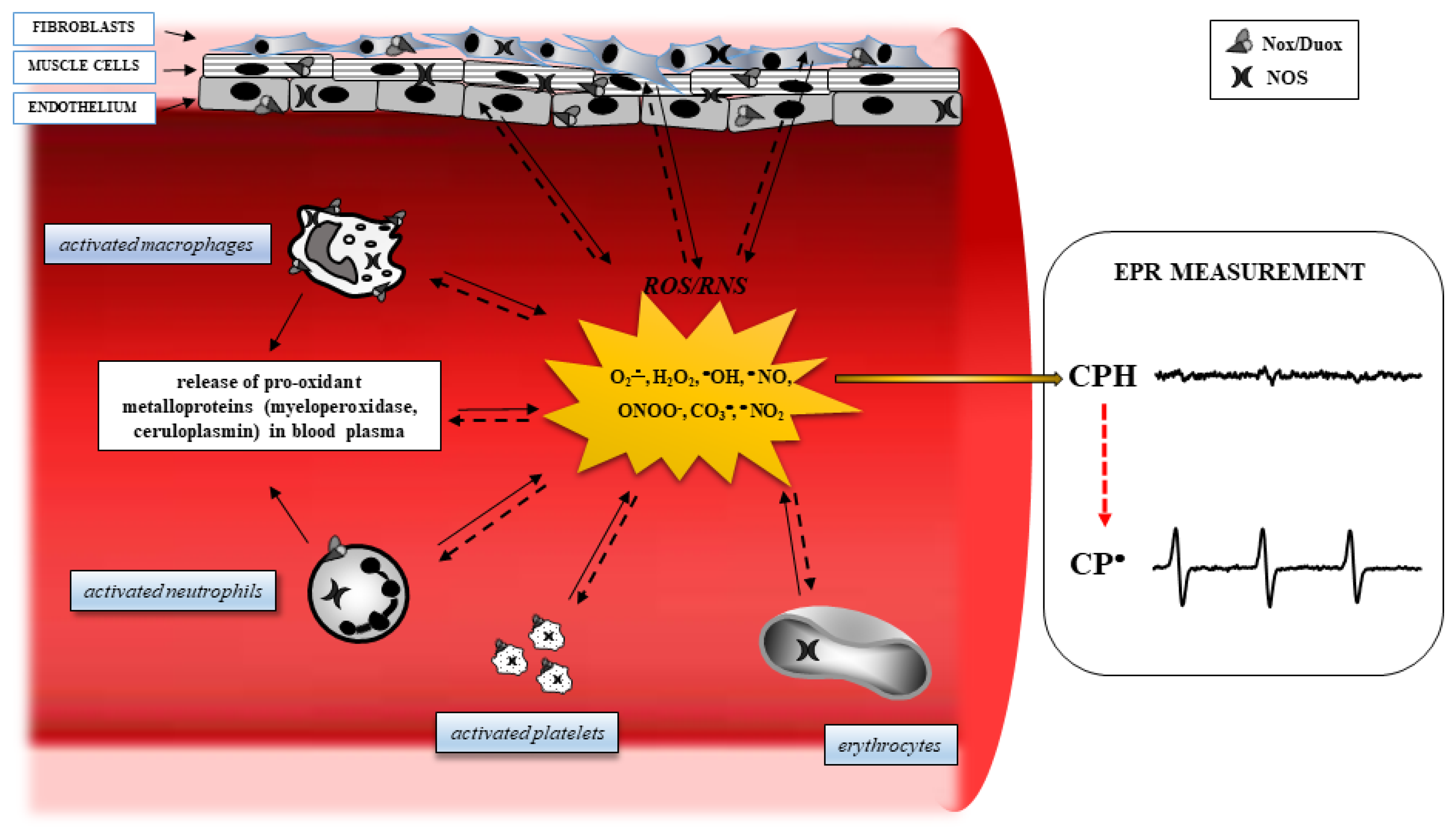
2.5. Analysis of Oxidative Stress Biomarkers by the EPR Technique
2.6. Statistical Analysis
3. Results
3.1. SG Outcomes
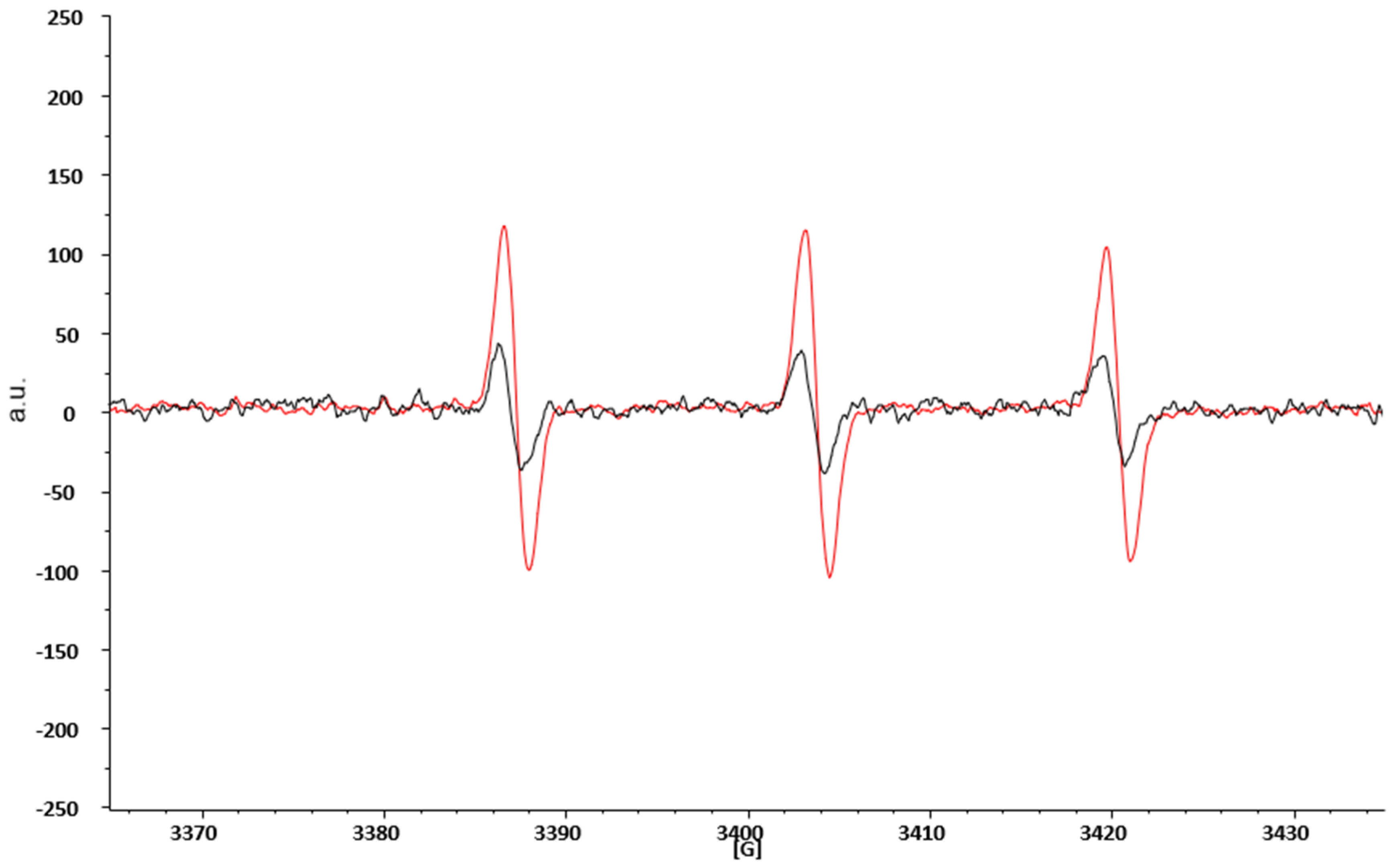
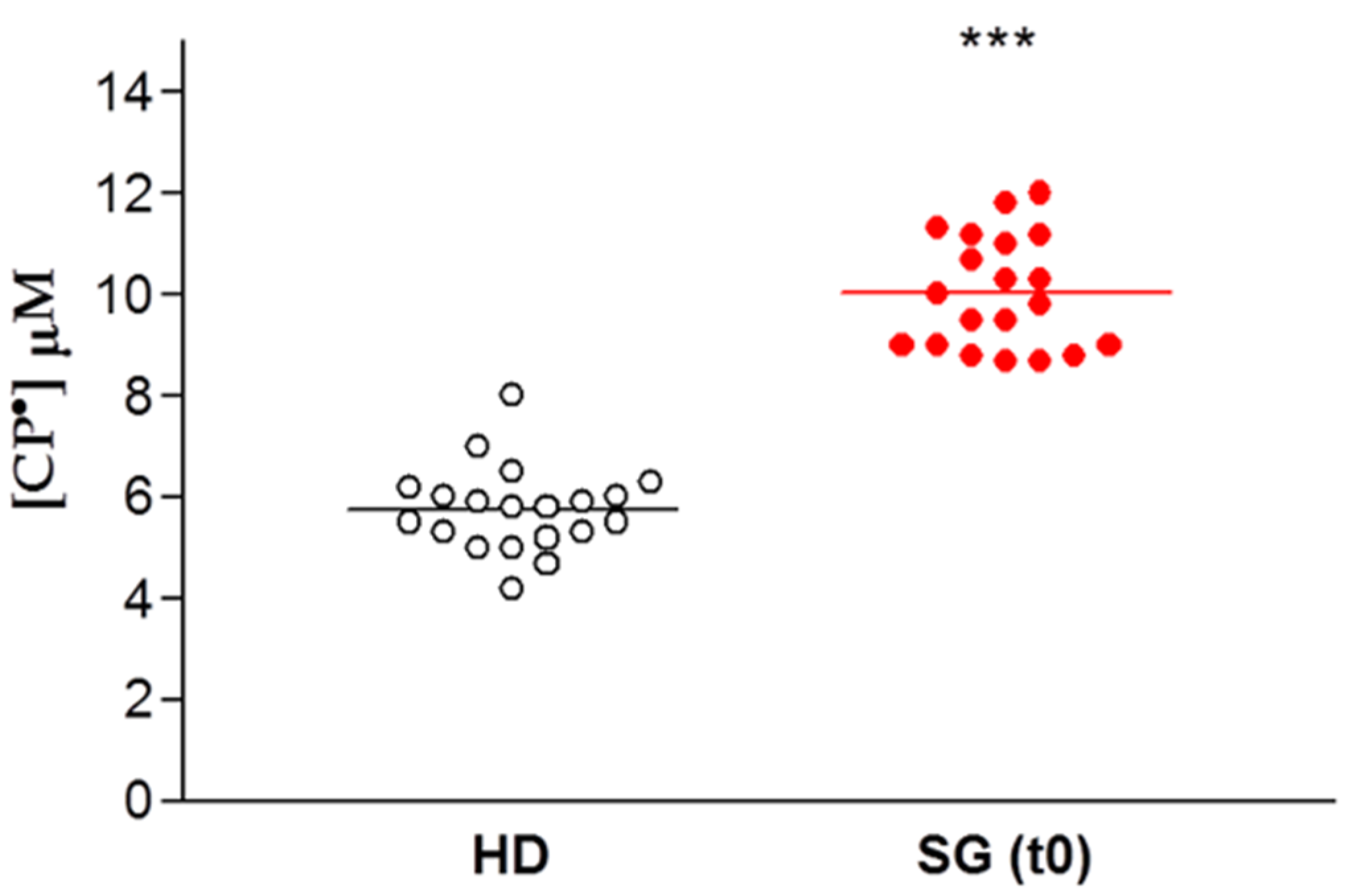
3.2. EPR-Spin Probing Analysis of Oxidative Stress in Blood
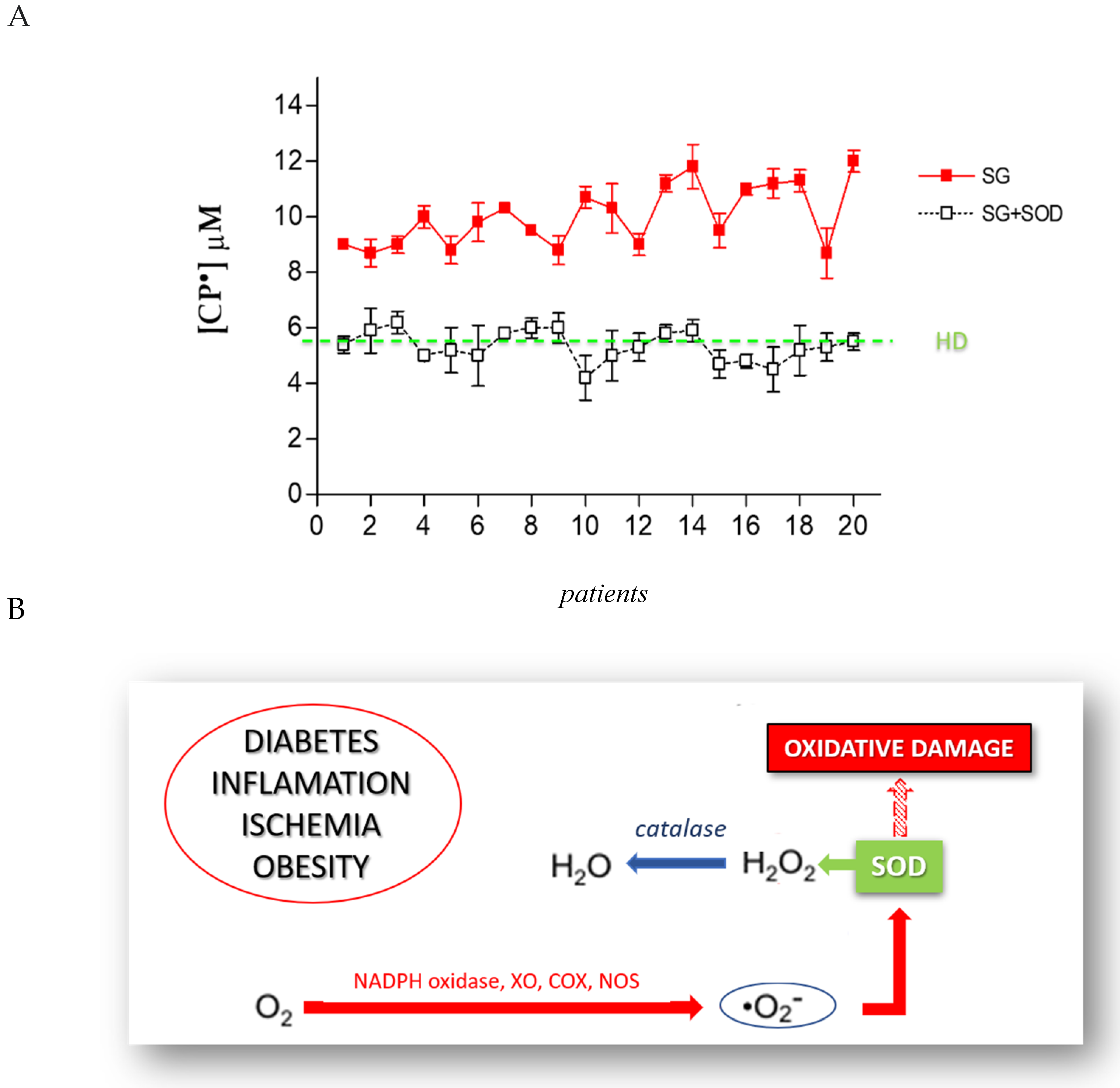
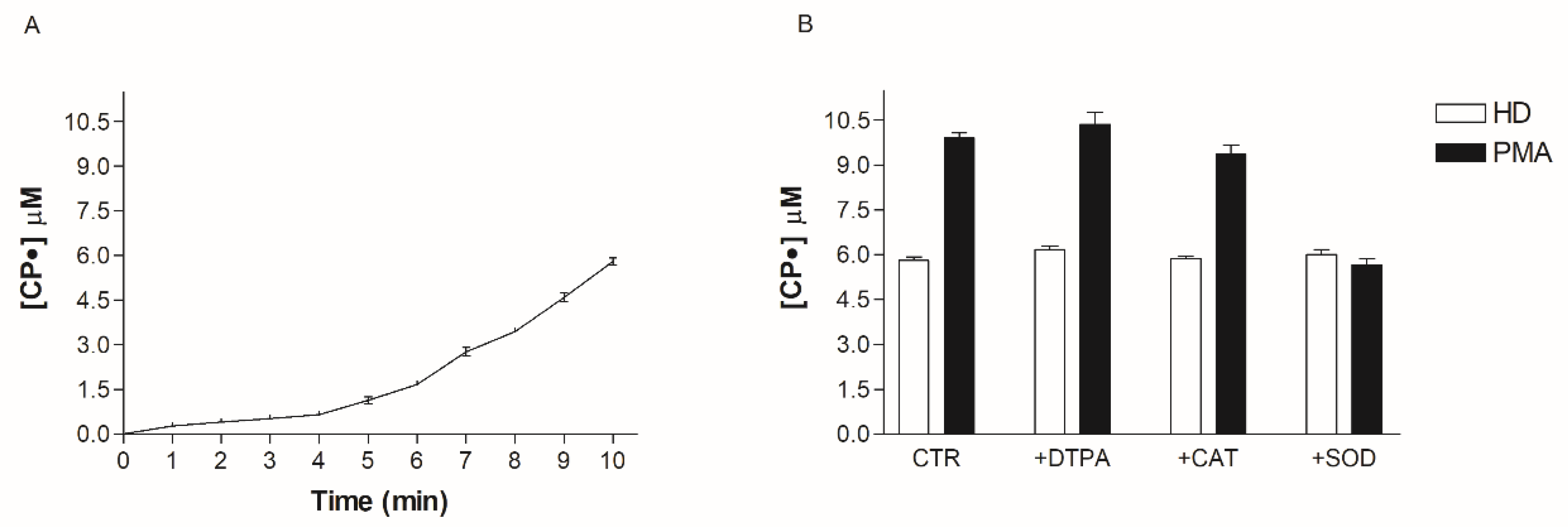
3.3. Identification of the Oxidative Species Responsible for Oxidative Stress in Obese Patients
3.4. Effect of SOD, Cat, DTPA, and PMA on CPH Oxidation
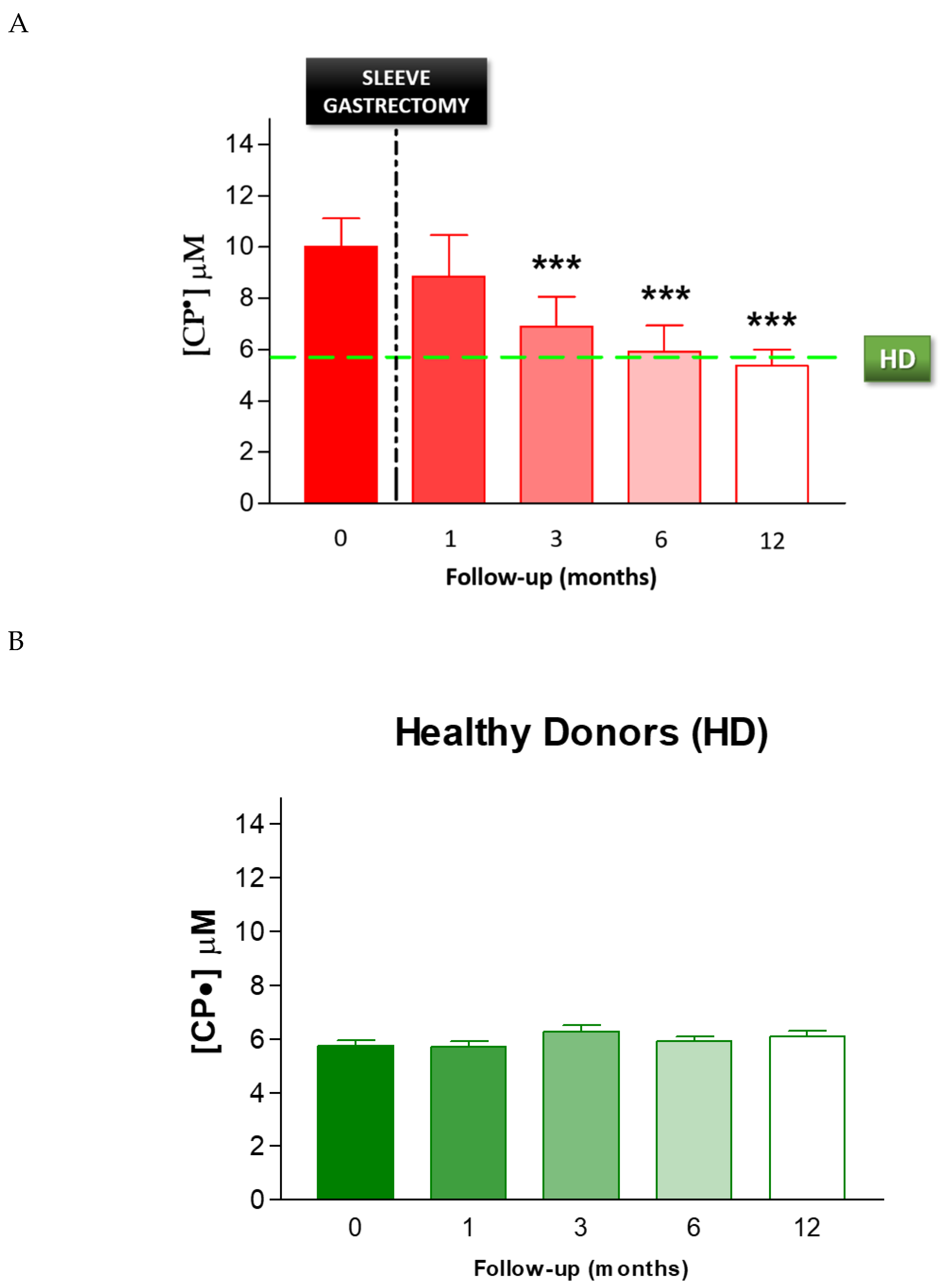
3.5. Effect of Sleeve Gastrectomy on Oxidative Stress
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lavie, C.J.; Milani, R.V.; Ventura, H.O. Obesity and cardiovascular disease: Risk factor, paradox, and impact of weight loss. J. Am. Coll. Cardiol. 2009, 53, 1925–1932. [Google Scholar] [CrossRef]
- Allott, E.H.; Hursting, S.D. Obesity and cancer: Mechanistic insights from transdisciplinary studies. Endocr. Relat. Cancer 2015, 22, R365–R386. [Google Scholar] [CrossRef]
- The, L. The link between cancer and obesity. Lancet 2017, 390, 1716. [Google Scholar] [CrossRef]
- Rahman, S.T.; Pandeya, N.; Neale, R.E.; McLeod, D.S.A.; Bain, C.J.; Baade, P.D.; Youl, P.H.; Allison, R.; Leonard, S.; Jordan, S.J. Obesity is associated with BRAFV600E-mutated thyroid cancer. Thyroid 2020. [Google Scholar] [CrossRef]
- Wilson, K.M.; Cho, E. Obesity and Kidney Cancer. Recent Results Cancer Res. 2016, 208, 81–93. [Google Scholar] [CrossRef]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef]
- Pothuraju, R.; Rachagani, S.; Junker, W.M.; Chaudhary, S.; Saraswathi, V.; Kaur, S.; Batra, S.K. Pancreatic cancer associated with obesity and diabetes: An alternative approach for its targeting. J. Exp. Clin. Cancer Res. 2018, 37, 319. [Google Scholar] [CrossRef]
- Vidal, A.C.; Freedland, S.J. Obesity and Prostate Cancer: A Focused Update on Active Surveillance, Race, and Molecular Subtyping. Eur. Urol. 2017, 72, 78–83. [Google Scholar] [CrossRef]
- Mackintosh, M.L.; Crosbie, E.J. Obesity-driven endometrial cancer: Is weight loss the answer? BJOG 2013, 120, 791–794. [Google Scholar] [CrossRef]
- Keaney, J.F.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J.; et al. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham Study. Arter. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef]
- Zhang, P.Y.; Xu, X.; Li, X.C. Cardiovascular diseases: Oxidative damage and antioxidant protection. Eur. Rev. Med. Pharm. Sci. 2014, 18, 3091–3096. [Google Scholar]
- Straface, E.; Marchesi, A.; Gambardella, L.; Metere, A.; Tarissi de Jacobis, I.; Viora, M.; Giordani, L.; Villani, A.; Del Principe, D.; Malorni, W.; et al. Does oxidative stress play a critical role in cardiovascular complications of Kawasaki disease? Antioxid Redox Signal. 2012, 17, 1441–1446. [Google Scholar] [CrossRef]
- Liu, H.; Liu, X.; Zhang, C.; Zhu, H.; Xu, Q.; Bu, Y.; Lei, Y. Redox Imbalance in the Development of Colorectal Cancer. J. Cancer 2017, 8, 1586–1597. [Google Scholar] [CrossRef]
- Wu, X.; Cheng, J.; Wang, X. Dietary Antioxidants: Potential Anticancer Agents. Nutr. Cancer 2017, 69, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Caglayan, A.; Katlan, D.C.; Selçuk Tuncer, Z.; Yüce, K.; Sayal, H.B.; Coşkun Salman, M.; Kocer-Gumusel, B. Impaired antioxidant enzyme functions with increased lipid peroxidation in epithelial ovarian cancer. Iubmb. Life 2017. [Google Scholar] [CrossRef]
- Ding, Y.; Yao, H.; Yao, Y.; Fai, L.Y.; Zhang, Z. Protection of dietary polyphenols against oral cancer. Nutrients 2013, 5, 2173–2191. [Google Scholar] [CrossRef]
- Stafeev, I.S.; Vorotnikov, A.V.; Ratner, E.I.; Menshikov, M.Y.; Parfyonova, Y.V. Latent Inflammation and Insulin Resistance in Adipose Tissue. Int. J. Endocrinol. 2017, 2017, 5076732. [Google Scholar] [CrossRef]
- Sansbury, B.E.; Hill, B.G. Regulation of obesity and insulin resistance by nitric oxide. Free Radic. Biol. Med. 2014, 73, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Radi, R. Peroxynitrite, a stealthy biological oxidant. J. Biol. Chem. 2013, 288, 26464–26472. [Google Scholar] [CrossRef]
- Metere, A.; Iorio, E.; Pietraforte, D.; Podo, F.; Minetti, M. Peroxynitrite signaling in human erythrocytes: Synergistic role of hemoglobin oxidation and band 3 tyrosine phosphorylation. Arch. Biochem. Biophys. 2009, 484, 173–182. [Google Scholar] [CrossRef]
- Dixit, V.D. Adipose-immune interactions during obesity and caloric restriction: Reciprocal mechanisms regulating immunity and health span. J. Leukoc. Biol. 2008, 84, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Engin, A. Human Protein Kinases and Obesity. Adv. Exp. Med. Biol. 2017, 960, 111–134. [Google Scholar] [CrossRef]
- Engin, A. The Pathogenesis of Obesity-Associated Adipose Tissue Inflammation. Adv. Exp. Med. Biol. 2017, 960, 221–245. [Google Scholar] [CrossRef]
- Vilarrasa, N.; Rubio, M.A.; Miñambres, I.; Flores, L.; Caixàs, A.; Ciudin, A.; Bueno, M.; García-Luna, P.P.; Ballesteros-Pomar, M.D.; Ruiz-Adana, M.; et al. Long-Term Outcomes in Patients with Morbid Obesity and Type 1 Diabetes Undergoing Bariatric Surgery. Obes. Surg. 2017, 27, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Fouse, T.; Brethauer, S. Resolution of Comorbidities and Impact on Longevity Following Bariatric and Metabolic Surgery. Surg. Clin. N. Am. 2016, 96, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Gallart-Aragón, T.; Fernández-Lao, C.; Galiano-Castillo, N.; Cantarero-Villanueva, I.; Lozano-Lozano, M.; Arroyo-Morales, M. Improvements in Health-Related Quality of Life and Pain: A Cohort Study in Obese Patients After Laparoscopic Sleeve Gastrectomy. J. Laparoendosc. Adv. Surg. Tech. A 2017. [Google Scholar] [CrossRef]
- Lucchese, M.; Borisenko, O.; Mantovani, L.G.; Cortesi, P.A.; Cesana, G.; Adam, D.; Burdukova, E.; Lukyanov, V.; Di Lorenzo, N. Cost-Utility Analysis of Bariatric Surgery in Italy: Results of Decision-Analytic Modelling. Obes. Facts 2017, 10, 261–272. [Google Scholar] [CrossRef]
- Quan, S.F.; Gillin, J.C.; Littner, M.R.; Shepard, J.W. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999, 22, 667–689. [Google Scholar]
- Dikalov, S.; Skatchkov, M.; Bassenge, E. Spin trapping of superoxide radicals and peroxynitrite by 1-hydroxy-3-carboxy-pyrrolidine and 1-hydroxy-2,2,6, 6-tetramethyl-4-oxo-piperidine and the stability of corresponding nitroxyl radicals towards biological reductants. Biochem. Biophys. Res. Commun. 1997, 231, 701–704. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Gussoni, M.; Montorsi, M.; Porcelli, S.; Vezzoli, A. Assessment of a standardized ROS production profile in humans by electron paramagnetic resonance. Oxid. Med. Cell Longev. 2012, 2012, 973927. [Google Scholar] [CrossRef] [PubMed]
- Dikalov, S.I.; Kirilyuk, I.A.; Voinov, M.; Grigor’ev, I.A. EPR detection of cellular and mitochondrial superoxide using cyclic hydroxylamines. Free Radic. Res. 2011, 45, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Rius-Pérez, S.; Torres-Cuevas, I.; Millán, I.; Ortega, Á.; Pérez, S. PGC-1. Oxid. Med. Cell Longev. 2020, 2020, 1452696. [Google Scholar] [CrossRef] [PubMed]
- Korda, M.; Kubant, R.; Patton, S.; Malinski, T. Leptin-induced endothelial dysfunction in obesity. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1514–H1521. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Tchernova, J.; Whincup, P.; Lowe, G.D.; Kelly, A.; Rumley, A.; Wallace, A.M.; Sattar, N. Plasma leptin: Associations with metabolic, inflammatory and haemostatic risk factors for cardiovascular disease. Atherosclerosis 2007, 191, 418–426. [Google Scholar] [CrossRef]
- Cho, Y.L.; Tan, H.W.S.; Saquib, Q.; Ren, Y.; Ahmad, J.; Wahab, R.; He, W.; Bay, B.H.; Shen, H.M. Dual role of oxidative stress-JNK activation in autophagy and apoptosis induced by nickel oxide nanoparticles in human cancer cells. Free Radic. Biol. Med. 2020, 153, 173–186. [Google Scholar] [CrossRef]
- Yung, J.H.M.; Giacca, A. Role of c-Jun N-terminal Kinase (JNK) in Obesity and Type 2 Diabetes. Cells 2020, 9. [Google Scholar] [CrossRef]
- Styskal, J.; Van Remmen, H.; Richardson, A.; Salmon, A.B. Oxidative stress and diabetes: What can we learn about insulin resistance from antioxidant mutant mouse models? Free Radic. Biol. Med. 2012, 52, 46–58. [Google Scholar] [CrossRef]
- Chen, C.C.; Sun, Y.T.; Chen, J.J.; Chiu, K.T. TNF-alpha-induced cyclooxygenase-2 expression in human lung epithelial cells: Involvement of the phospholipase C-gamma 2, protein kinase C-alpha, tyrosine kinase, NF-kappa B-inducing kinase, and I-kappa B kinase 1/2 pathway. J. Immunol. 2000, 165, 2719–2728. [Google Scholar] [CrossRef]
- Lin, C.C.; Hsiao, L.D.; Chien, C.S.; Lee, C.W.; Hsieh, J.T.; Yang, C.M. Tumor necrosis factor-alpha-induced cyclooxygenase-2 expression in human tracheal smooth muscle cells: Involvement of p42/p44 and p38 mitogen-activated protein kinases and nuclear factor-kappaB. Cell Signal. 2004, 16, 597–607. [Google Scholar] [CrossRef]
- Bryan, S.; Baregzay, B.; Spicer, D.; Singal, P.K.; Khaper, N. Redox-inflammatory synergy in the metabolic syndrome. Can. J. Physiol. Pharm. 2013, 91, 22–30. [Google Scholar] [CrossRef]
- Kander, M.C.; Cui, Y.; Liu, Z. Gender difference in oxidative stress: A new look at the mechanisms for cardiovascular diseases. J. Cell Mol. Med. 2017, 21, 1024–1032. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before | SG | 1 | M | After | SG | 3 | M | After | SG | 6 | M | After | SG | 12 | M | After | SG | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | AGE | SEX | H (m) | W (Kg) | BMI | AHT | OSA | W (Kg) | BMI | AHT | OSA | W (Kg) | BMI | AHT | OSA | W (Kg) | BMI | AHT | OSA | W (Kg) | BMI | AHT | OSA |
| 1 | 49 | F | 1.6 | 106 | 41.4 | n | 0 | 89 | 34.8 | n | 0 | 72.8 | 28.4 | n | 0 | 65 | 25.4 | n | 0 | 52 | 20.3 | n | 0 |
| 2 | 49 | F | 1.75 | 140 | 45.7 | n | 1 | 113 | 36.9 | n | 1 | 95 | 31.0 | n | 0 | 85 | 27.8 | n | 1 | 82 | 26.8 | n | 0 |
| 3 | 40 | M | 1.58 | 103 | 41.3 | n | 0 | 91 | 36.5 | n | 0 | 71 | 28.4 | n | 0 | 68 | 27.2 | n | 0 | 63 | 25.2 | n | 0 |
| 4 | 27 | F | 1.6 | 110 | 43.0 | n | 0 | 95 | 37.1 | n | 0 | 75 | 29.3 | n | 0 | 71 | 27.7 | n | 0 | 65 | 25.4 | n | 0 |
| 5 | 42 | F | 1.54 | 107 | 45.1 | n | 0 | 97 | 40.9 | n | 0 | 78 | 32.9 | n | 0 | 70 | 29.5 | n | 0 | 60 | 25.3 | n | 0 |
| 6 | 51 | F | 1.52 | 108 | 46.7 | n | 0 | 95 | 41.1 | n | 0 | 72 | 31.2 | n | 0 | 71 | 30.5 | n | 0 | 67 | 29.0 | n | 0 |
| 7 | 49 | F | 1.78 | 120 | 37.9 | y | 2 | 103 | 32.5 | y | 2 | 80 | 25.2 | y | 1 | 77 | 24.3 | y | 0 | 76 | 24.0 | y | 0 |
| 8 | 55 | M | 1.6 | 93 | 36.3 | y | 0 | 85 | 33.2 | y | 0 | 74 | 28.9 | y | 0 | 64 | 25.0 | n | 0 | 60 | 23.4 | n | 0 |
| 9 | 39 | F | 1.5 | 91 | 40.4 | n | 0 | 82 | 36.4 | n | 0 | 75 | 33.3 | n | 0 | 66 | 29.3 | n | 0 | 58 | 25.8 | n | 0 |
| 10 | 39 | F | 1.56 | 105 | 43.1 | n | 0 | 96 | 39.3 | n | 0 | 81.5 | 33.5 | n | 0 | 74 | 30.4 | n | 0 | 67 | 27.5 | n | 0 |
| 11 | 37 | F | 1.77 | 144 | 46.0 | n | 0 | 123 | 39.3 | n | 0 | 98 | 31.3 | n | 0 | 88 | 28.1 | n | 0 | 85 | 27.1 | n | 0 |
| 12 | 39 | M | 1.7 | 135 | 46.7 | n | 0 | 115 | 39.8 | n | 0 | 98 | 33.9 | n | 0 | 85 | 29.4 | n | 0 | 78 | 27.0 | n | 0 |
| 13 | 46 | F | 1.7 | 110 | 38.1 | y | 0 | 103 | 35.6 | y | 0 | 88 | 30.4 | y | 0 | 78 | 27.0 | y | 0 | 72 | 24.9 | n | 0 |
| 14 | 42 | F | 1.66 | 125 | 45.4 | n | 2 | 114 | 41.4 | n | 2 | 97 | 35.2 | n | 2 | 85 | 30.8 | n | 1 | 76 | 27.6 | n | 0 |
| 15 | 42 | M | 1.83 | 129 | 38.5 | y | 0 | 115 | 34.3 | y | 0 | 102 | 30.5 | y | 0 | 88 | 26.3 | y | 0 | 72 | 21.5 | n | 0 |
| 16 | 42 | F | 1.65 | 115 | 42.2 | n | 0 | 98 | 36.0 | n | 0 | 82 | 30.1 | n | 0 | 71 | 26.1 | n | 0 | 65 | 23.9 | n | 0 |
| 17 | 51 | F | 1.62 | 106 | 40.4 | n | 0 | 88 | 33.5 | n | 0 | 71 | 27.1 | n | 0 | 65 | 24.8 | n | 0 | 59 | 22.5 | n | 0 |
| 18 | 39 | F | 1.5 | 98 | 43.6 | n | 0 | 89 | 39.6 | n | 0 | 79 | 35.1 | n | 0 | 68 | 30.2 | n | 0 | 57 | 25.3 | n | 0 |
| 19 | 49 | F | 1.7 | 123 | 42.6 | n | 0 | 105 | 36.3 | n | 0 | 88 | 30.4 | n | 0 | 76 | 26.3 | n | 0 | 65 | 22.5 | n | 0 |
| 20 | 40 | F | 1.68 | 118 | 41.8 | n | 0 | 91 | 32.2 | n | 0 | 86 | 30.5 | n | 0 | 76 | 26.9 | n | 0 | 72 | 25.5 | n | 0 |
| Mean | 43.4 | 114.3 | 42.3 | 99.3 | 36.8 | 83.2 | 30.8 | 74.5 | 27.7 | 67.6 | 25.0 | ||||||||||||
| ±SD | 6.5 | 14.8 | 3.1 | 11.6 | 2.9 | 10.2 | 2.6 | 8.0 | 2.1 | 8.9 | 2.2 | ||||||||||||
| min | 27.0 | 91.0 | 36.3 | 82.0 | 32.2 | 71.0 | 25.2 | 64.0 | 24.3 | 52.0 | 20.3 | ||||||||||||
| max | 55.0 | 144.0 | 46.7 | 123.0 | 41.4 | 102.0 | 35.2 | 88.0 | 30.8 | 85.0 | 29.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metere, A.; Graves, C.E.; Pietraforte, D.; Casella, G. The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity. Biomedicines 2020, 8, 168. https://doi.org/10.3390/biomedicines8060168
Metere A, Graves CE, Pietraforte D, Casella G. The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity. Biomedicines. 2020; 8(6):168. https://doi.org/10.3390/biomedicines8060168
Chicago/Turabian StyleMetere, Alessio, Claire E. Graves, Donatella Pietraforte, and Giovanni Casella. 2020. "The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity" Biomedicines 8, no. 6: 168. https://doi.org/10.3390/biomedicines8060168
APA StyleMetere, A., Graves, C. E., Pietraforte, D., & Casella, G. (2020). The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity. Biomedicines, 8(6), 168. https://doi.org/10.3390/biomedicines8060168