Dose-Independent Therapeutic Benefit of Bone Marrow Stem Cell Transplantation after MI in Mice

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Bone Marrow Aspiration
2.2. Cell Isolation
2.3. Experimental Design of the Animal Model
2.4. Generation of Reperfused MI in Mice and Stem Cell Implantation
2.5. Left Ventricular Catheterization and Heart Tissue Analyses
2.6. Statistical Analysis
3. Results
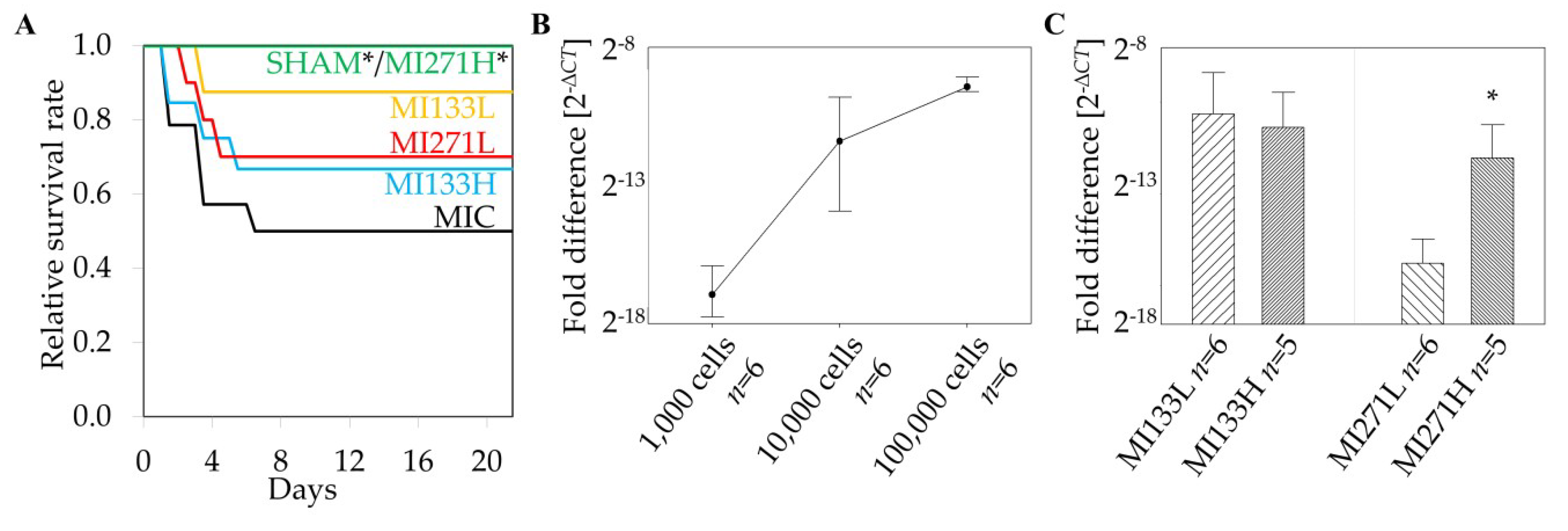
3.1. Survival Rate
3.2. Retention of Human Stem Cells in the Infarcted Heart
3.3. Hemodynamic Functions
3.4. Cardiac Remodeling
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Asahara, T.; Murohara, T.; Sullivan, A.; Silver, M.; van der Zee, R.; Li, T.; Witzenbichler, B.; Schatteman, G.; Isner, J.M. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997, 275, 964–967. [Google Scholar] [CrossRef] [PubMed]
- Nesselmann, C.; Kaminski, A.; Steinhoff, G. Cardiac stem cell therapy. Herz 2011, 36, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Clifford, D.M.; Fisher, S.A.; Brunskill, S.J.; Doree, C.; Mathur, A.; Watt, S.; Martin-Rendon, E. Stem cell treatment for acute myocardial infarction. Cochrane Database Syst. Rev. 2012, 2, CD006536. [Google Scholar] [CrossRef]
- Matar, A.A.; Chong, J.J. Stem cell therapy for cardiac dysfunction. SpringerPlus 2014, 3, 440. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chou, S.H.; Lin, S.Z.; Kuo, W.W.; Pai, P.; Lin, J.Y.; Lai, C.H.; Kuo, C.H.; Lin, K.H.; Tsai, F.J.; Huang, C.Y. Mesenchymal stem cell insights: Prospects in cardiovascular therapy. Cell Transplant. 2014, 23, 513–529. [Google Scholar] [CrossRef]
- Stamm, C.; Westphal, B.; Kleine, H.D.; Petzsch, M.; Kittner, C.; Klinge, H.; Schümichen, C.; Nienaber, C.A.; Freund, M.; Steinhoff, G. Autologous bone-marrow stem-cell transplantation for myocardial regeneration. Lancet 2003, 361, 45–46. [Google Scholar] [CrossRef]
- Ma, N.; Ladilov, Y.; Moebius, J.M.; Ong, L.; Piechaczek, C.; Dávid, A.; Kaminski, A.; Choi, Y.H.; Li, W.; Egger, D.; et al. Intramyocardial delivery of human CD133+ cells in a SCID mouse cryoinjury model: Bone marrow vs. cord blood-derived cells. Cardiovasc. Res. 2006, 71, 158–169. [Google Scholar] [CrossRef]
- Stamm, C.; Kleine, H.D.; Choi, Y.H.; Dunkelmann, S.; Lauffs, J.A.; Lorenzen, B.; Dávid, A.; Liebold, A.; Nienaber, C.; Zurakowski, D.; et al. Intramyocardial delivery of CD133+ bone marrow cells and coronary artery bypass grafting for chronic ischemic heart disease: Safety and efficacy studies. J. Thorac. Cardiovasc. Surg. 2007, 133, 717–725. [Google Scholar] [CrossRef]
- Kfoury, Y.; Scadden, D.T. Mesenchymal cell contributions to the stem cell niche. Cell Stem Cell 2015, 16, 239–253. [Google Scholar] [CrossRef]
- Behfar, A.; Crespo-Diaz, R.; Terzic, A.; Gersh, B.J. Cell therapy for cardiac repair--lessons from clinical trials. Nat. Rev. Cardiol. 2014, 11, 232–246. [Google Scholar] [CrossRef]
- Kasper, G.; Dankert, N.; Tuischer, J.; Hoeft, M.; Gaber, T.; Glaeser, J.D.; Zander, D.; Tschirschmann, M.; Thompson, M.; Matziolis, G.; et al. Mesenchymal stem cells regulate angiogenesis according to their mechanical environment. Stem Cells 2007, 25, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Chen, L.; Fan, L.; Wu, L.; Chen, X.; Li, W.; Lin, Y.; Wang, W. Enhanced therapeutic effects of mesenchymal stem cells on myocardial infarction by ischemic postconditioning through paracrine mechanisms in rats. J. Mol. Cell. Cardiol. 2011, 51, 839–847. [Google Scholar] [CrossRef]
- Majumdar, M.K.; Thiede, M.A.; Mosca, J.D.; Moorman, M.; Gerson, S.L. Phenotypic and functional comparison of cultures of marrow-derived mesenchymal stem cells (MSCs) and stromal cells. J. Cell. Physiol 1998, 176, 57–66. [Google Scholar] [CrossRef]
- Chen, L.; Tredget, E.E.; Wu, P.Y.; Wu, Y. Paracrine factors of mesenchymal stem cells recruit macrophages and endothelial lineage cells and enhance wound healing. PLoS ONE 2008, 3, e1886. [Google Scholar] [CrossRef]
- Hsiao, S.T.F.; Asgari, A.; Lokmic, Z.; Sinclair, R.; Dusting, G.J.; Lim, S.Y.; Dilley, R.J. Comparative analysis of paracrine factor expression in human adult mesenchymal stem cells derived from bone marrow, adipose, and dermal tissue. Stem Cells Dev. 2012, 21, 2189–2203. [Google Scholar] [CrossRef]
- Zisa, D.; Shabbir, A.; Suzuki, G.; Lee, T. Vascular endothelial growth factor (VEGF) as a key therapeutic trophic factor in bone marrow mesenchymal stem cell-mediated cardiac repair. Biochem. Biophys. Res. Commun. 2009, 390, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.L.B.K.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The international society for cellular therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Furlani, D.; Li, W.; Pittermann, E.; Klopsch, C.; Wang, L.; Knopp, A.; Jungebluth, P.; Thedinga, E.; Havenstein, C.; Westien, I.; et al. A transformed cell population derived from cultured mesenchymal stem cells has no functional effect after transplantation into the injured heart. Cell Transplant. 2009, 18, 319–331. [Google Scholar] [CrossRef]
- Hanley, P.J.; Mei, Z.; da Graca Cabreira-Hansen, M.; Klis, M.; Li, W.; Zhao, Y.; Durett, A.G.; Zheng, X.; Wang, Y.; Gee, A.P.; et al. Manufacturing mesenchymal stromal cells for phase I clinical trials. Cytotherapy 2013, 15, 416–422. [Google Scholar] [CrossRef][Green Version]
- Phinney, D.G.; Galipeau, J. MSC committee of the international society of cell and gene therapy. Manufacturing mesenchymal stromal cells for clinical applications: A survey of Good Manufacturing Practices at U.S. academic centers. Cytotherapy 2019, 21, 782–792. [Google Scholar] [CrossRef]
- Herzog, E.L.; Chai, L.; Krause, D.S. Plasticity of marrow-derived stem cells. Blood 2003, 102, 3483–3493. [Google Scholar] [CrossRef] [PubMed]
- Pomeraniec, L.; Benayahu, D. Mesenchymal Cell Growth and Differentiation on a New Biocomposite Material: A Promising Model for Regeneration Therapy. Biomolecules 2020, 10, 458. [Google Scholar] [CrossRef] [PubMed]
- Quirici, N.; Soligo, D.; Bossolasco, P.; Servida, F.; Lumini, C.; Deliliers, G.L. Isolation of bone marrow mesenchymal stem cells by anti-nerve growth factor receptor antibodies. Exp. Hematol. 2002, 30, 783–791. [Google Scholar] [CrossRef]
- Lemcke, H.; Gaebel, R.; Skorska, A.; Voronina, N.; Lux, C.A.; Petters, J.; Sasse, S.; Zarniko, N.; Steinhoff, G.; David, R. Mechanisms of stem cell based cardiac repair-gap junctional signaling promotes the cardiac lineage specification of mesenchymal stem cells. Sci. Rep. 2017, 7, 9755. [Google Scholar] [CrossRef]
- Sadraddin, H.; Gaebel, R.; Skorska, A.; Lux, C.A.; Sasse, S.; Ahmad, B.; Vasudevan, P.; Steinhoff, G.; David, R. CD271+ human mesenchymal stem cells show antiarrhythmic effects in a novel murine infarction model. Cells 2019, 8, 1474. [Google Scholar] [CrossRef]
- Sasse, S.; Skorska, A.; Lux, C.A.; Steinhoff, G.; David, R.; Gaebel, R. Angiogenic potential of bone marrow derived CD133+ and CD271+ intramyocardial stem cell trans-plantation post MI. Cells 2020, 9, 78. [Google Scholar] [CrossRef]
- Kai, H.; Kuwahara, F.; Tokuda, K.; Imaizumi, T. Diastolic Dysfunction in Hypertensive Hearts: Roles of Perivascular Inflammation and Reactive Myocardial Fibrosis. Hypertens. Res. 2005, 28, 483–490. [Google Scholar] [CrossRef]
- Poggioli, T.; Sarathchandra, P.; Rosenthal, N.; Santini, M.P. Intramyocardial cell delivery: Observations in murine hearts. JoVE (J. Vis. Exp.) 2014, 24, e51064. [Google Scholar] [CrossRef]
- Leong, Y.Y.; Ng, W.H.; Ellison-Hughes, G.M.; Tan, J.J. Cardiac Stem Cells for Myocardial Regeneration: They Are Not Alone. Front. Cardiovasc. Med. 2017, 17, 4–47. [Google Scholar] [CrossRef]
- Donndorf, P.; Kaminski, A.; Tiedemann, G.; Kundt, G.; Steinhoff, G. Validating intramyocardial bone marrow stem cell therapy in combination with coronary artery bypass grafting, the PERFECT Phase III randomized multicenter trial: Study protocol for a randomized controlled trial. Trials 2012, 13, 99. [Google Scholar] [CrossRef]
- Abdel-Latif, A.; Bolli, R.; Tleyjeh, I.M.; Montori, V.M.; Perin, E.C.; Hornung, C.A.; Zuba-Surma, E.K.; Al-Mallah, M.; Dawn, B. Adult bone marrow-derived cells for cardiac repair: A systematic review and meta-analysis. Arch. Intern. Med. 2007, 167, 989–997. [Google Scholar] [CrossRef]
- Quyyumi, A.A.; Waller, E.K.; Murrow, J.; Esteves, F.; Galt, J.; Oshinski, J.; Lerakis, S.; Sher, S.; Vaughan, D.; Perin, E.; et al. CD34(+) cell infusion after ST elevation myocardial infarction is associated with improved perfusion and is dose dependent. Am. Heart J. 2011, 161, 98–105. [Google Scholar] [CrossRef]
- van der Spoel, T.I.; Jansen of Lorkeers, S.J.; Agostoni, P.; van Belle, E.; Gyöngyösi, M.; Sluijter, J.P.; Cramer, M.J.; Doevendans, P.A.; Chamuleau, S.A.J. Human relevance of pre-clinical studies in stem cell therapy: Systematic review and meta-analysis of large animal models of ischaemic heart disease. Cardiovasc. Res. 2011, 91, 649–658. [Google Scholar] [CrossRef]
- Iwasaki, H.; Kawamoto, A.; Ishikawa, M.; Oyamada, A.; Nakamori, S.; Nishimura, H.; Sadamoto, K.; Horii, M.; Matsumoto, T.; Murasawa, S.; et al. Dose-dependent contribution of CD34-positive cell transplantation to concurrent vasculogenesis and cardiomyogenesis for functional regenerative recovery after myocardial infarction. Circulation 2006, 113, 1311–1325. [Google Scholar] [CrossRef] [PubMed]
- Hare, J.M.; Fishman, J.E.; Gerstenblith, G.; Velazquez, D.L.D.; Zambrano, J.P.; Suncion, V.Y.; Tracy, M.; Ghersin, E.; Johnston, P.V.; Brinker, J.A.; et al. Comparison of allogeneic vs. autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: The POSEIDON randomized trial. JAMA 2012, 308, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Hamamoto, H.; Gorman, J.H., III; Ryan, L.P.; Hinmon, R.; Martens, T.P.; Schuster, M.D.; Plappert, T.; Kiupel, M.; John-Sutton, M.G.S.; Itescu, S.; et al. Allogeneic mesenchymal precursor cell therapy to limit remodeling after myocardial infarction: The effect of cell dosage. Ann. Thorac. Surg. 2009, 87, 794–801. [Google Scholar] [CrossRef]
- Rizk, M.; Monaghan, M.; Shorr, R.; Kekre, N.; Bredeson, C.N.; Allan, D.S. Heterogeneity in Studies of Mesenchymal Stromal Cells to Treat or Prevent Graft-versus-Host Disease: A Scoping Review of the Evidence. Biol. Blood Marrow Transplant. 2016, 22, 1416–1423. [Google Scholar] [CrossRef]
- Cuthbert, R.; Boxall, S.A.; Tan, H.B.; Giannoudis, P.V.; McGonagle, D.; Jones, E. Single-platform quality control assay to quantify multipotential stromal cells in bone marrow aspirates prior to bulk manufacture or direct therapeutic use. Cytotherapy 2012, 14, 431–440. [Google Scholar] [CrossRef]
- Ganguly, P.; El-Jawhari, J.J.; Burska, A.N.; Ponchel, F.; Giannoudis, P.V.; Jones, E.A. The Analysis of In Vivo Aging in Human Bone Marrow Mesenchymal Stromal Cells Using Colony-Forming Unit-Fibroblast Assay and the CD45lowCD271+ Phenotype. Stem Cells Int. 2019, 2019, 5197983. [Google Scholar] [CrossRef]
- Cox, G.; Boxall, S.A.; Giannoudis, P.V.; Buckley, C.T.; Roshdy, T.; Churchman, S.M.; McGonagle, D.; Jones, E. High abundance of CD271(+) multipotential stromal cells (MSCs) in intramedullary cavities of long bones. Bone 2012, 50, 510–517. [Google Scholar] [CrossRef]
- Hernigou, P.; Poignard, A.; Beaujean, F.; Rouard, H. Percutaneous autologous bone-marrow graftingfor nonunions. Influence of the number and concentration of progenitor cells. J. Bone Joint. Surg. Am. 2005, 87, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Galleu, A.; Riffo-Vasquez, Y.; Trento, C.; Lomas, C.; Dolcetti, L.; Cheung, T.S.; von Bonin, M.; Barbieri, L.; Halai, K.; Weng, L.; et al. Apoptosis in mesenchymal stromal cells induces in vivo recipient-mediated immunomodulation. Sci. Transl. Med. 2017, 9, eaam7828. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Condition | SH (n = 7) | MIC (n = 7) | MI133H (n = 8) | MI133L (n = 7) | MI271H (n = 7) | MI271L (n = 7) |
| dPmax [mmHg/s] | 4159.10* ± 325.24 | 2613.64 ± 372.44 | 2809.09 ± 126.14 | 3869.36 ± 688.17 | 3510.26 ± 552.77 | 3868.91* ± 290.33 |
| LVEF [%] | 55.60* ± 5.44 | 25.81 ± 2.76 | 37.53 ± 4.37 | 41.11* ± 4.73 | 40.01 ± 3.91 | 45.66* ± 2.04 |
| dPmin [mmHg)/s] | −3835.77* ± 242.96 | −2227.65 ± 395.24 | −2352.85 ± 129.00 | −3353.57 ± 650.47 | −3241.84 ± 548.76 | −3222.29 ± 269.63 |
| τ (Tau) [ms] | 7.40 ± 1.14 | 7.72 ± 1.85 | 9.44 ± 2.65 | 8.00 ± 3.02 | 11.63 ± 4.45 | 7.59 ± 1.58 |
| LVEDP [mmHg] | 3.10 ± 0.85 | 2.35 ± 0.77 | 2.72 ± 2.96 | 2.54 ± 1.09 | 4.69 ± 2.22 | 2.60 ± 0.45 |
| Stress condition | SH (n = 7) | MIC (n = 7) | MI133H (n = 8) | MI133L (n = 7) | MI271H (n = 7) | MI271L (n = 7) |
| dPmax [mmHg/s] | 12794.03* ± 813.35 | 7776.74 ± 1209.54 | 7152.38 ± 1102.03 | 9588.91 ± 1417.98 | 9489.74 ± 920.56 | 9399.51 ± 873.92 |
| LVEF [%] | 85.63* ± 4.46 | 46.86 ± 8.20 | 58.53 ± 9.03 | 57.23 ± 5.21 | 74.37 ± 6.00 | 65.57 ± 5.91 |
| dPmin [mmHg/s] | −11828.26* ± 1948.01 | −6372.09 ± 1349.94 | −5400.93 ± 845.98 | −7214.74 ± 1031.34 | −6499.11 ± 752.13 | −5975.43 ± 555.27 |
| τ (Tau) [ms] | 4.11 ± 0.41 | 6.14 ± 1.32 | 6.88 ± 2.00 | 6.03 ± 2.17 | 5.66 ± 2.46 | 3.43 ± 0.24 |
| LVEDP [mmHg] | 2.51 ± 0.26 | 5.71 ± 2.80 | 4.90 ± 4.47 | 2.69 ± 1.51 | 3.66 ± 2.09 | 2.09 ± 0.28 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarniko, N.; Skorska, A.; Steinhoff, G.; David, R.; Gaebel, R. Dose-Independent Therapeutic Benefit of Bone Marrow Stem Cell Transplantation after MI in Mice. Biomedicines 2020, 8, 157. https://doi.org/10.3390/biomedicines8060157
Zarniko N, Skorska A, Steinhoff G, David R, Gaebel R. Dose-Independent Therapeutic Benefit of Bone Marrow Stem Cell Transplantation after MI in Mice. Biomedicines. 2020; 8(6):157. https://doi.org/10.3390/biomedicines8060157
Chicago/Turabian StyleZarniko, Nicole, Anna Skorska, Gustav Steinhoff, Robert David, and Ralf Gaebel. 2020. "Dose-Independent Therapeutic Benefit of Bone Marrow Stem Cell Transplantation after MI in Mice" Biomedicines 8, no. 6: 157. https://doi.org/10.3390/biomedicines8060157
APA StyleZarniko, N., Skorska, A., Steinhoff, G., David, R., & Gaebel, R. (2020). Dose-Independent Therapeutic Benefit of Bone Marrow Stem Cell Transplantation after MI in Mice. Biomedicines, 8(6), 157. https://doi.org/10.3390/biomedicines8060157