Effectiveness of Glecaprevir/Pibrentasvir for Hepatitis C: Real-World Experience and Clinical Features of Retreatment Cases

 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
1. Introduction
2. Methods
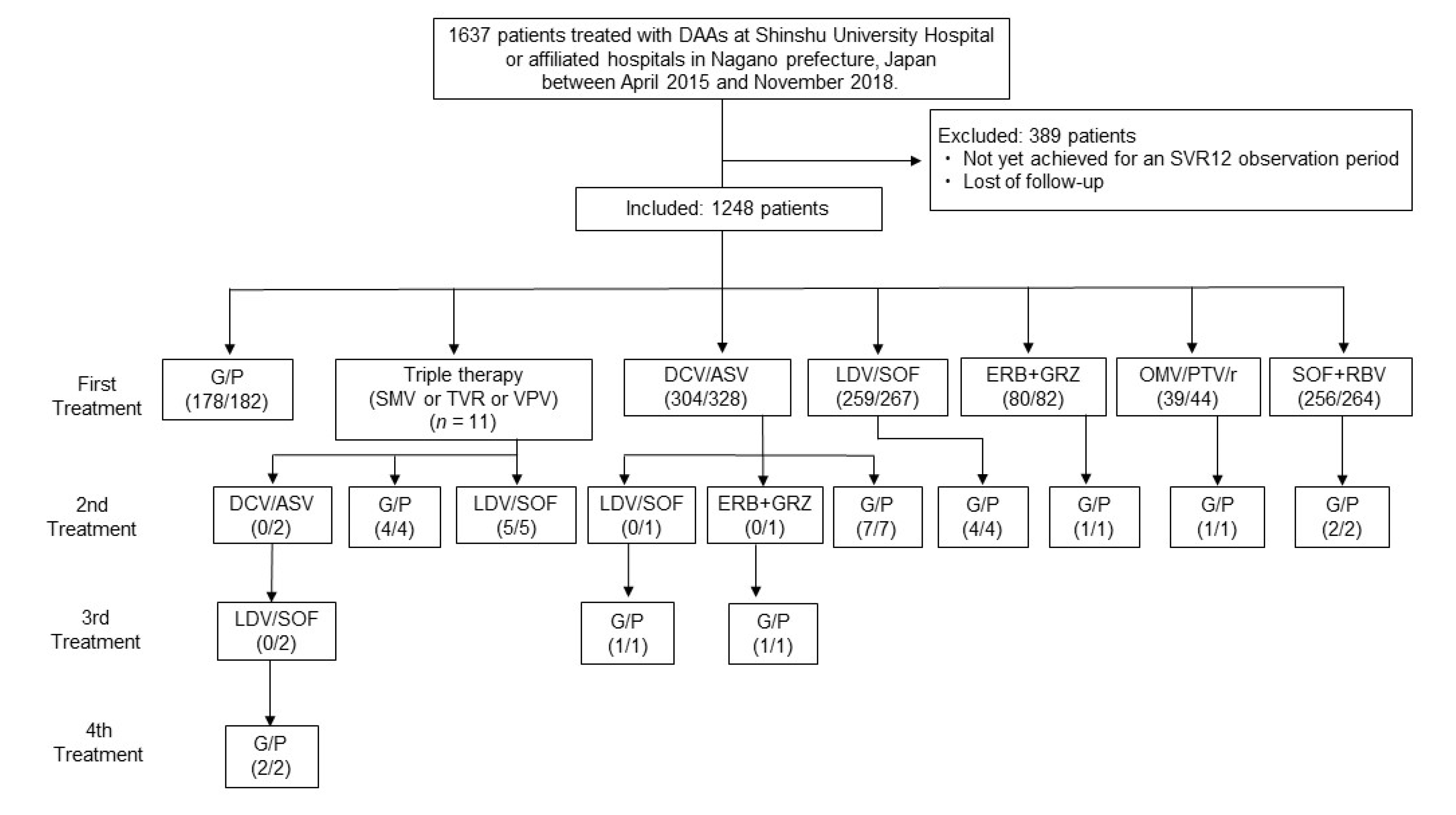
2.1. Patients and Methods
2.2. Laboratory Testing
2.3. Testing for RAS of the HCV-RNA Genome
2.4. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. G/P Outcomes
3.3. Comparisons between First Treatment and Retreatment Groups
3.4. RASs in HCV-RNA Genome in Retreatment Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kiyosawa, K.; Sodeyama, T.; Tanaka, E.; Gibo, Y.; Yoshizawa, K.; Nakano, Y.; Furuta, S.; Akahane, Y.; Nishioka, K.; Purcell, R.H.; et al. Interrelationship of blood transfusion, non-A, non-B hepatitis and hepatocellular carcinoma: Analysis by detection of antibody to hepatitis C virus. Hepatology 1990, 12, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Kiyosawa, K.; Tanaka, E.; Sodeyama, T.; Furuta, S. Natural History of Hepatitis C. Intervirology 1994, 37, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Kiyosawa, K. Natural history of acute hepatitis C. J. Gastroenterol. Hepatol. 2000, 15, E97–E104. [Google Scholar] [CrossRef] [PubMed]
- Kiyosawa, K.; Umemura, T.; Ichijo, T.; Matsumoto, A.; Yoshizawa, K.; Gad, A.; Tanaka, E. Hepatocellular carcinoma: Recent trends in Japan. Gastroenterology 2004, 127, S17–S26. [Google Scholar] [CrossRef]
- D’Ambrosio, R.; Pasulo, L.; Puoti, M.; Vinci, M.; Schiavini, M.; Lazzaroni, S.; Soria, A.; Gatti, F.; Menzaghi, B.; Aghemo, A.; et al. Real-world effectiveness and safety of glecaprevir/pibrentasvir in 723 patients with chronic hepatitis C. J. Hepatol. 2019, 70, 379–387. [Google Scholar] [CrossRef]
- Ogawa, E.; Furusyo, N.; Nakamuta, M.; Nomura, H.; Satoh, T.; Takahashi, K.; Koyanagi, T.; Kajiwara, E.; Dohmen, K.; Kawano, A.; et al. Glecaprevir and pibrentasvir for Japanese patients with chronic hepatitis C genotype 1 or 2 infection: Results from a multicenter, real-world cohort study. Hepatol. Res. 2019, 49, 617–626. [Google Scholar] [CrossRef]
- Sezaki, H.; Suzuki, F.; Hosaka, T.; Fujiyama, S.; Kawamura, Y.; Akuta, N.; Kobayashi, M.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Initial- and re-treatment effectiveness of glecaprevir and pibrentasvir for Japanese patients with chronic hepatitis C virus-genotype 1/2/3 infections. J. Gastroenterol. 2019, 54, 916–927. [Google Scholar] [CrossRef]
- Toyoda, H.; Atsukawa, M.; Uojima, H.; Nozaki, A.; Tamai, H.; Takaguchi, K.; Fujioka, S.; Nakamuta, M.; Tada, T.; Yasuda, S.; et al. Trends and Efficacy of Interferon-Free Anti-hepatitis C Virus Therapy in the Region of High Prevalence of Elderly Patients, Cirrhosis, and Hepatocellular Carcinoma: A Real-World, Nationwide, Multicenter Study of 10 688 Patients in Japan. Open Forum Infect. Dis. 2019, 6, ofz185. [Google Scholar] [CrossRef]
- Asahina, Y.; Izumi, N.; Hiromitsu, K.; Kurosaki, M.; Koike, K.; Suzuki, F.; Takikawa, H.; Tanaka, A.; Tanaka, E.; Tanaka, Y.; et al. JSH Guidelines for the Management of Hepatitis C Virus Infection: A 2016 update for genotype 1 and 2. Hepatol. Res. 2016, 46, 129–165. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. Comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Castera, L.; Vergniol, J.; Foucher, J.; Le Bail, B.; Chanteloup, E.; Haaser, M.; Darriet, M.; Couzigou, P.; De Ledinghen, V. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005, 128, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, F.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Seko, Y.; Kawamura, Y.; Hosaka, T.; Kobayashi, M.; Saito, S.; Arase, Y.; et al. Prevalence of hepatitis C virus variants resistant to NS3 protease inhibitors or the NS5A inhibitor (BMS-790052) in hepatitis patients with genotype 1b. J. Clin. Virol. 2012, 54, 352–354. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Yasui, S.; Nakamura, M.; Suzuki, E.; Arai, M.; Haga, Y.; Sasaki, R.; Wu, S.; Nakamoto, S.; Imazeki, F.; et al. Daclatasvir plus Asunaprevir Treatment for Real-World HCV Genotype 1-Infected Patients in Japan. Int. J. Med. Sci. 2016, 13, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Miura, M.; Maekawa, S.; Sato, M.; Komatsu, N.; Tatsumi, A.; Takano, S.; Amemiya, F.; Nakayama, Y.; Inoue, T.; Sakamoto, M.; et al. Deep sequencing analysis of variants resistant to the non-structural 5A inhibitor daclatasvir in patients with genotype 1b hepatitis C virus infection. Hepatol. Res. 2014, 44, E360–E367. [Google Scholar] [CrossRef]
- Goossens, N.; Negro, F. Is genotype 3 of the hepatitis C virus the new villain? Hepatology 2014, 59, 2403–2412. [Google Scholar] [CrossRef]
- Zeuzem, S.; Foster, G.R.; Wang, S.; Asatryan, A.; Gane, E.; Feld, J.J.; Asselah, T.; Bourliere, M.; Ruane, P.J.; Wedemeyer, H.; et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection. N. Engl. J. Med. 2018, 378, 354–369. [Google Scholar] [CrossRef] [PubMed]
- Kumada, H.; Watanabe, T.; Suzuki, F.; Ikeda, K.; Sato, K.; Toyoda, H.; Atsukawa, M.; Ido, A.; Takaki, A.; Enomoto, N.; et al. Efficacy and safety of glecaprevir/pibrentasvir in HCV-infected Japanese patients with prior DAA experience, severe renal impairment, or genotype 3 infection. J. Gastroenterol. 2017, 53, 566–575. [Google Scholar] [CrossRef]
- Sugiura, A.; Joshita, S.; Umemura, T.; Yamazaki, T.; Fujimori, N.; Kimura, T.; Matsumoto, A.; Igarashi, K.; Usami, Y.; Wada, S.; et al. Past history of hepatocellular carcinoma is an independent risk factor of treatment failure in patients with chronic hepatitis C virus infection receiving direct-acting antivirals. J. Viral Hepat. 2018, 25, 1462–1471. [Google Scholar] [CrossRef]
- Reddy, K.R.; Lim, J.K.; Kuo, A.; Di Bisceglie, A.M.; Galati, J.S.; Morelli, G.; Everson, G.T.; Kwo, P.Y.; Brown, R.S.J.; Sulkowski, M.S.; et al. All-oral direct-acting antiviral therapy in HCV-advanced liver disease is effective in real-world practice: Observations through HCV-TARGET database. Aliment. Pharmacol. Ther. 2017, 45, 115–126. [Google Scholar] [CrossRef]
- Zeuzem, S.; Dusheiko, G.M.; Salupere, R.; Mangia, A.; Flisiak, R.; Hyland, R.H.; Illeperuma, A.; Svarovskaia, E.; Brainard, D.M.; Symonds, W.T.; et al. Sofosbuvir and Ribavirin in HCV Genotypes 2 and 3. N. Engl. J. Med. 2014, 370, 1993–2001. [Google Scholar] [CrossRef]
- Probst, A.; Dang, T.; Bochud, M.; Egger, M.; Negro, F.; Bochud, P.-Y. Role of Hepatitis C virus genotype 3 in liver fibrosis progression—A systematic review and meta-analysis. J. Viral Hepat. 2011, 18, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Lemm, J.A.; O’Boyle, D.; Liu, M.; Nower, P.T.; Colonno, R.; Deshpande, M.S.; Snyder, L.B.; Martin, S.W.; St Laurent, D.R.; Serrano-Wu, M.H.; et al. Identification of hepatitis C virus NS5A inhibitors. J. Virol. 2010, 84, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Uchida, Y.; Kouyama, J.; Naiki, K.; Tsuji, S.; Sugawara, K.; Nakao, M.; Motoya, D.; Nakayama, N.; Imai, Y.; et al. NS5A-P32 deletion as a factor involved in virologic failure in patients receiving glecaprevir and pibrentasvir. J. Gastroenterol. 2019, 54, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Osawa, M.; Imamura, M.; Teraoka, Y.; Uchida, T.; Morio, K.; Fujino, H.; Nakahara, T.; Ono, A.; Murakami, E.; Kawaoka, T.; et al. Real-world efficacy of glecaprevir plus pibrentasvir for chronic hepatitis C patient with previous direct-acting antiviral therapy failures. J. Gastroenterol. 2019, 54, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Nitta, S.; Asahina, Y.; Kato, T.; Tsuchiya, J.; Inoue-Shinomiya, E.; Sato, A.; Tsunoda, T.; Miyoshi, M.; Kawai-Kitahata, F.; Murakawa, M.; et al. Impact of novel NS5A resistance-associated substitutions of hepatitis C virus detected in treatment-experienced patients. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Patients (n = 182) | ||
|---|---|---|
| Median | IQR | |
| Age at entry (years) | 68 | (18–93) |
| Gender (male/female) | 77/105 | |
| HCV genotype | ||
| 1/2/3/1 + 2/ND | 86/66/4/1/25 | |
| Chronic hepatitis/liver cirrhosis | 155/27 | |
| Laboratory data | ||
| White blood cells (μ/L) | 4910 | (1360–9010) |
| Hemoglobin (g/dL) | 13.7 | (8.7–18.5) |
| Platelet count (×109/L) | 176 | (12–369) |
| Albumin (g/dL) | 4.1 | (2.7–4.8) |
| AST (U/L) | 33 | (11–259) |
| ALT (U/L) | 29 | (7–281) |
| Total bilirubin (mg/dL) | 0.7 | (0.2–2.0) |
| AFP (ng/mL) | 4.0 | (1.2–193.0) |
| Cre (mg/dL) | 0.7 | (0.4–11.4) |
| eGFR (mL/min/1.73 m2) | 68.1 | (3.0–118.1) |
| Fibrosis markers | ||
| FIB-4 index | 2.3 | (0.3–27.2) |
| APRI | 0.5 | (0.1–17.5) |
| Y93H mutation * | 50.0% | |
| Complications | ||
| Hypertension | 37.0% | |
| Diabetes | 15.6% | |
| Dyslipidemia | 8.7% | |
| Hemodialysis | 5.0% | |
| Experienced | ||
| Prior IFN | 18.0% | |
| Prior DAAs | 13.6% | |
| Prior HCC | 6.2% | |
| Outcome | ||
| SVR (ITT) | 178/182 (97.8%) | |
| SVR (PP) | 178/179 (99.4%) | |
| Discontinuation | 3/182 (0.16%) |
| First Treatment (n = 159) | Retreatment (n = 23) | p-Value | |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Age at entry (years) | 68 | 68 | 0.362 |
| Gender (male/female) | 68/91 | 9/14 | 0.705 |
| HCV genotype | |||
| 1/2/3/1 + 2/ND | 66/63/4/1/25 | 19/4/0/0/0 | |
| Chronic hepatitis/liver cirrhosis | 135/24 | 20/3 | 0.357 |
| Laboratory data | |||
| White blood cells (μ/L) | 4900 (1360–9010) | 4920 (2310–8670) | 0.937 |
| Hemoglobin (g/dL) | 13.5 (8.7–17.6) | 14.3 (8.7–18.5) | 0.111 |
| Platelet count (×109/L) | 176 (12–369) | 174 (34–343) | 0.249 |
| Albumin (g/dL) | 4.1 (2.7–4.8) | 4.1 (2.8–4.7) | 0.653 |
| AST (U/L) | 33 (11–259) | 33 (19–90) | 0.580 |
| ALT (U/L) | 30 (7–281) | 27 (15–141) | 0.458 |
| Total bilirubin (mg/dL) | 0.6 (0.2–2.0) | 0.7 (0.4–1.5) | 0.399 |
| AFP (ng/mL) | 4.0 (1.2–193.0) | 5.0 (1.7–24.6) | 0.455 |
| Cre (mg/dL) | 0.8 (0.5–11.1) | 0.7 (0.5–3.0) | 0.180 |
| eGFR (mL/min/1.73 m2) | 66.9 (3.0–115.7) | 78.3 (17.8–118.1) | 0.061 |
| Fibrosis markers | |||
| FIB-4 index | 2.2 (0.3–27.3) | 2.6 (0.8–9.7) | 0.592 |
| APRI | 0.5 (0.1–17.5) | 0.5 (0.1–3.8) | 0.805 |
| Y93H mutation * | 25.0% | 75.0% | <0.001 |
| Complications | |||
| Hypertension | 37.0% | 36.8% | 0.991 |
| Diabetes | 17.4% | 5.0% | 0.158 |
| Dyslipidemia | 9.2% | 5.3% | 0.567 |
| Hemodialysis | 5.8% | 0% | 0.236 |
| Experienced | |||
| Prior IFN | 12.3% | 52.2% | <0.001 |
| Prior HCC | 5.8% | 8.7% | 0.593 |
| Case | Age | Gender | Prior DAA Treatment | NS5A | NS3 | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genotype 1 | L23 | Q24 | L28 | R30 | L31 | P32 | F37 | Q54 | P58 | Q62 | A92 | Y93 | V36 | F43 | T54 | V55 | N77 | Q80 | S122 | R155 | A156 | D168 | V170 | |||
| 1 | 55 | F | DCV/ASV | - | - | - | - | M | - | - | - | S | - | - | H | - | - | - | - | - | - | - | - | - | - | - |
| 2 | 69 | M | DCV/ASV | - | K | M | R/A/G/T | - | - | - | - | - | - | - | - | - | - | - | - | - | L | G | - | - | - | - |
| 3 | 74 | F | DCV/ASV | - | - | - | - | F | - | - | H | - | - | V | H | - | - | - | - | - | - | G | - | - | - | - |
| 4 | 75 | F | DCV/ASV | - | K | T | H | - | - | - | - | - | - | - | - | - | - | - | - | - | - | G | - | - | - | I |
| 5 | 34 | F | DCV/ASV | - | - | - | - | V | - | L | G | - | - | - | H | - | - | - | - | - | L | - | - | - | E | I |
| 6 | 68 | F | DCV/ASV | - | K | M/V | H/Q | - | - | - | - | - | - | - | Y/H | - | - | - | - | - | Q/R | - | - | - | E | I |
| 7 | 70 | F | DCV/ASV | - | - | - | - | - | - | - | Y | - | - | - | H | - | - | - | - | - | - | G | - | - | - | - |
| 8 | 76 | F | LDV/SOF | - | - | - | - | L/M | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | I |
| 9 | 37 | M | LDV/SOF | - | K | M | Q | - | - | L | N | - | - | - | H/N | - | - | - | - | - | - | S/N | - | - | - | I |
| 10 | 70 | F | LDV/SOF | - | - | - | - | - | - | F/L | - | - | - | - | H | - | - | - | - | - | - | N | - | - | - | - |
| 11 | 68 | F | EBR + GRZ | - | - | - | - | V | - | L | H | - | - | - | H | - | - | - | - | - | - | - | - | - | - | - |
| 12 | 65 | F | OBV/PTV/r | - | - | - | - | - | - | - | H | - | D | - | Y/H | - | - | - | - | - | - | T | - | - | - | I |
| 13 | 76 | M | DCV/ASV followed by LDV/SOF | - | K | M | Q | - | - | L | R | - | E | - | H | - | - | - | - | - | - | - | - | - | - | I |
| 14 | 58 | M | DCV/ASV followed by LDV/SOF | - | - | - | - | V | - | L | - | - | - | - | H | - | - | - | - | - | L | C | - | - | E | I |
| 15 | 82 | M | DCV/ASV followed by EBR + GRZ | - | K | M | Q | V | - | - | - | - | - | - | F | - | - | - | - | - | - | - | - | - | - | - |
| 16 | 63 | M | SMV followed by DCV/ASV followed by LDV/SOF | - | - | - | - | I/M | - | L | H | - | - | - | Y/H | - | - | - | - | - | L | - | - | - | D/E | I |
| 17 * | 28 | M | VPV | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT |
| 18 * | 70 | F | SMV | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT |
| 19 * | 57 | F | SMV | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT | NT |
| Major RAS | L23 | Q24K | L28M | R30Q | L31M | P32 | F37L | Q54H | P58S | Q62 | A92V | Y93H | V36 | F43 | T54 | V55 | N77 | Q80L | S122G | R155 | A156 | D168E | V170I | |||
| Frequency | 0 | 37.5% | 31.2% | 25.0% | 18.7% | 0 | 43.7% | 25.0% | 6.2% | 0 | 6.2% | 75.0% | 0 | 0 | 0 | 0 | 0 | 25.0% | 25.0% | 0 | 0 | 25.0% | 56.2% |
| Case | Age | Gender | Prior DAA Treatment | NS5B | ||||
|---|---|---|---|---|---|---|---|---|
| Genotype 2 | L159 | S282 | C316 | L320 | V321 | |||
| 20 | 59 | M | SOF + RBV | - | - | - | - | - |
| 21 | 50 | M | SOF + RBV | - | - | - | - | - |
| 22 | 77 | F | SOF + RBV | - | - | - | - | - |
| 23 | 53 | M | SOF + RBV | - | - | - | - | - |
| Major RAS | L159 | S282 | C316N | L320 | V321 | |||
| Frequency | 0 | 0 | 0 | 0 | 0 | |||
| G/P failure case | 75 | M | Before G/P | NT | NT | NT | NT | NT |
| After G/P | - | - | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugiura, A.; Joshita, S.; Yamashita, Y.; Yamazaki, T.; Fujimori, N.; Kimura, T.; Matsumoto, A.; Wada, S.; Mori, H.; Shibata, S.; et al. Effectiveness of Glecaprevir/Pibrentasvir for Hepatitis C: Real-World Experience and Clinical Features of Retreatment Cases. Biomedicines 2020, 8, 74. https://doi.org/10.3390/biomedicines8040074
Sugiura A, Joshita S, Yamashita Y, Yamazaki T, Fujimori N, Kimura T, Matsumoto A, Wada S, Mori H, Shibata S, et al. Effectiveness of Glecaprevir/Pibrentasvir for Hepatitis C: Real-World Experience and Clinical Features of Retreatment Cases. Biomedicines. 2020; 8(4):74. https://doi.org/10.3390/biomedicines8040074
Chicago/Turabian StyleSugiura, Ayumi, Satoru Joshita, Yuki Yamashita, Tomoo Yamazaki, Naoyuki Fujimori, Takefumi Kimura, Akihiro Matsumoto, Shuichi Wada, Hiromitsu Mori, Soichiro Shibata, and et al. 2020. "Effectiveness of Glecaprevir/Pibrentasvir for Hepatitis C: Real-World Experience and Clinical Features of Retreatment Cases" Biomedicines 8, no. 4: 74. https://doi.org/10.3390/biomedicines8040074
APA StyleSugiura, A., Joshita, S., Yamashita, Y., Yamazaki, T., Fujimori, N., Kimura, T., Matsumoto, A., Wada, S., Mori, H., Shibata, S., Yoshizawa, K., Morita, S., Furuta, K., Kamijo, A., Iijima, A., Kako, S., Maruyama, A., Kobayashi, M., Komatsu, M., ... Umemura, T. (2020). Effectiveness of Glecaprevir/Pibrentasvir for Hepatitis C: Real-World Experience and Clinical Features of Retreatment Cases. Biomedicines, 8(4), 74. https://doi.org/10.3390/biomedicines8040074