Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression

 , and
, and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Clinical Examination and Periodontal Treatment
2.3. GCF Sampling and Multiplex Bead Immunoassay Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Findings
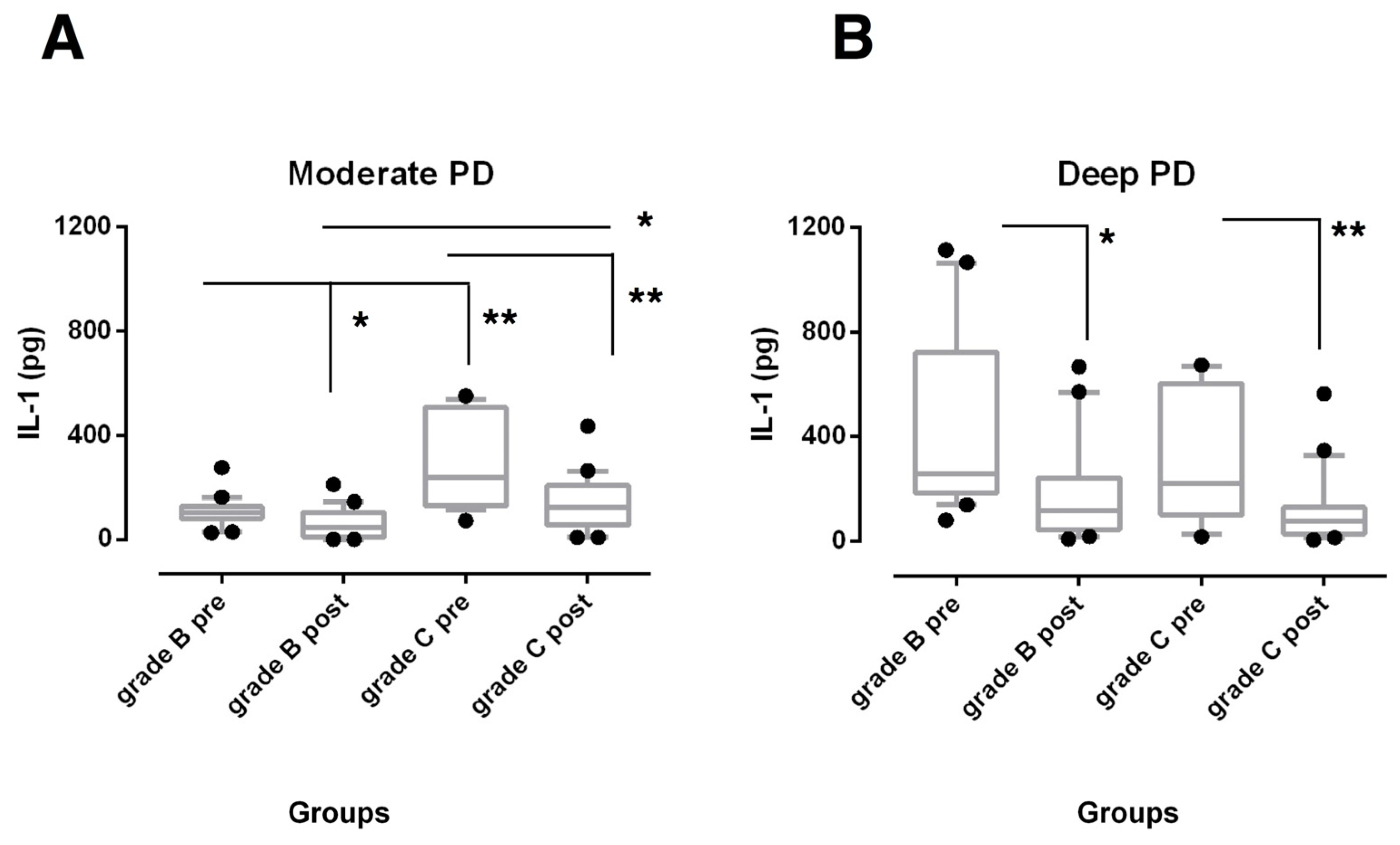
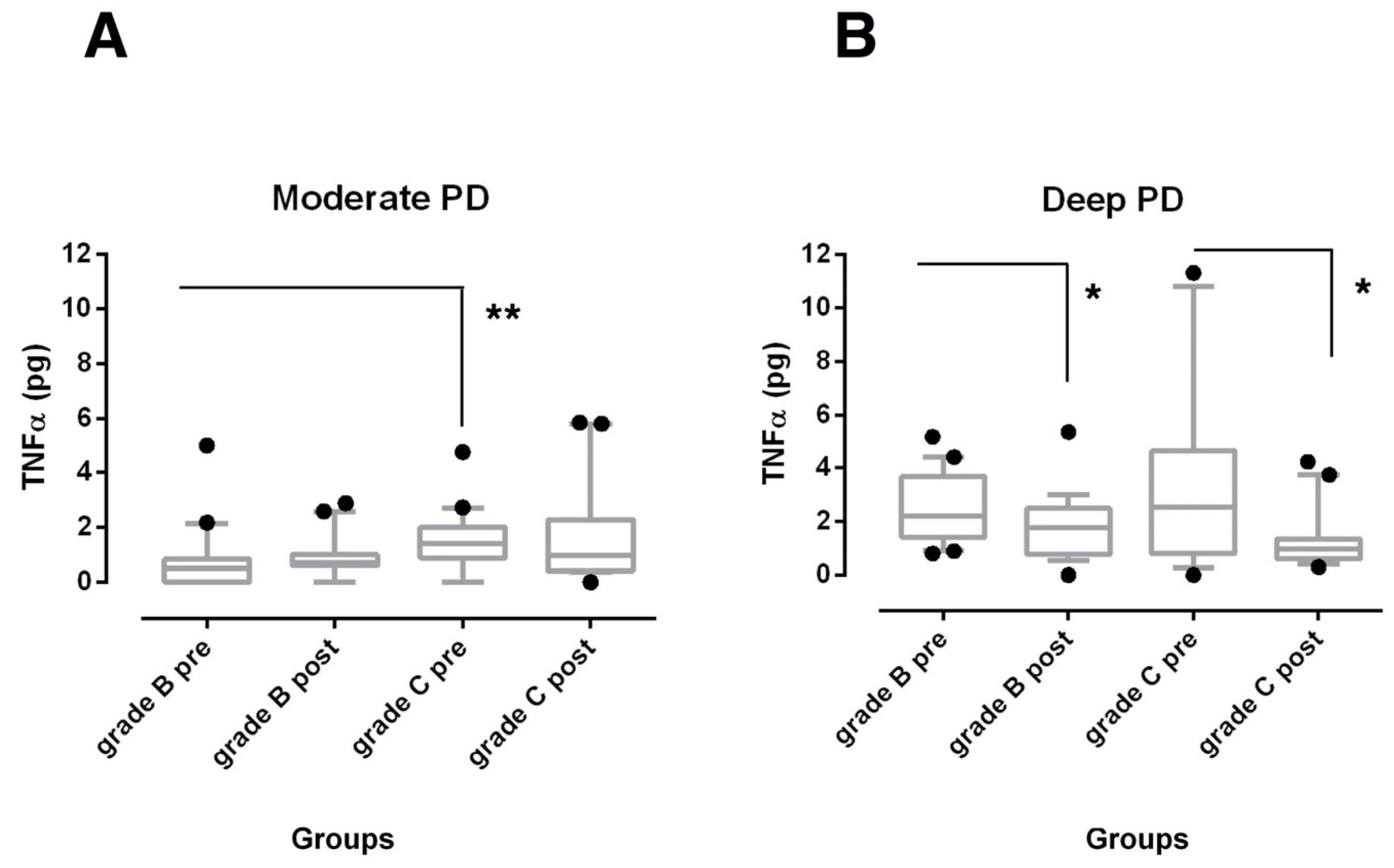
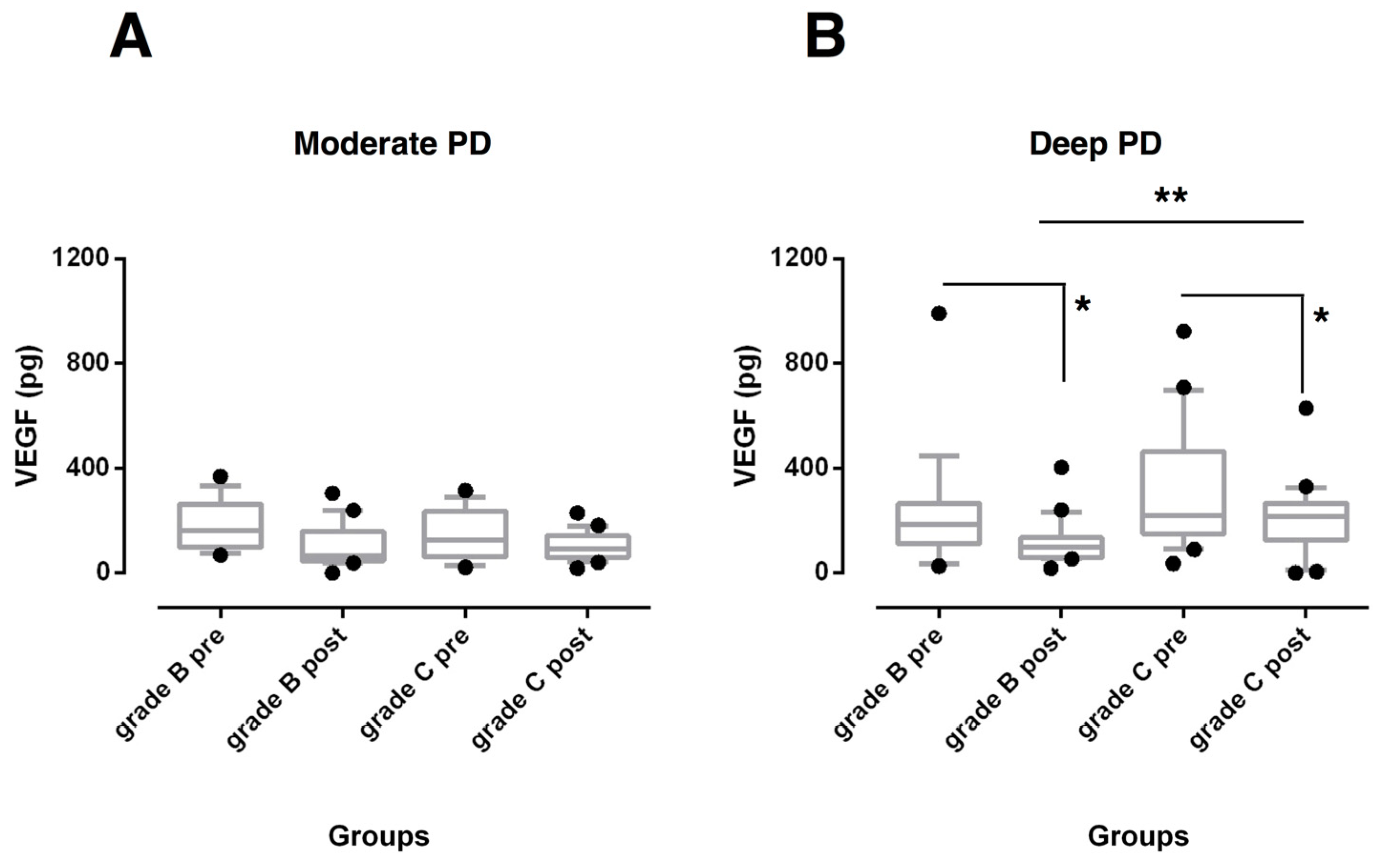
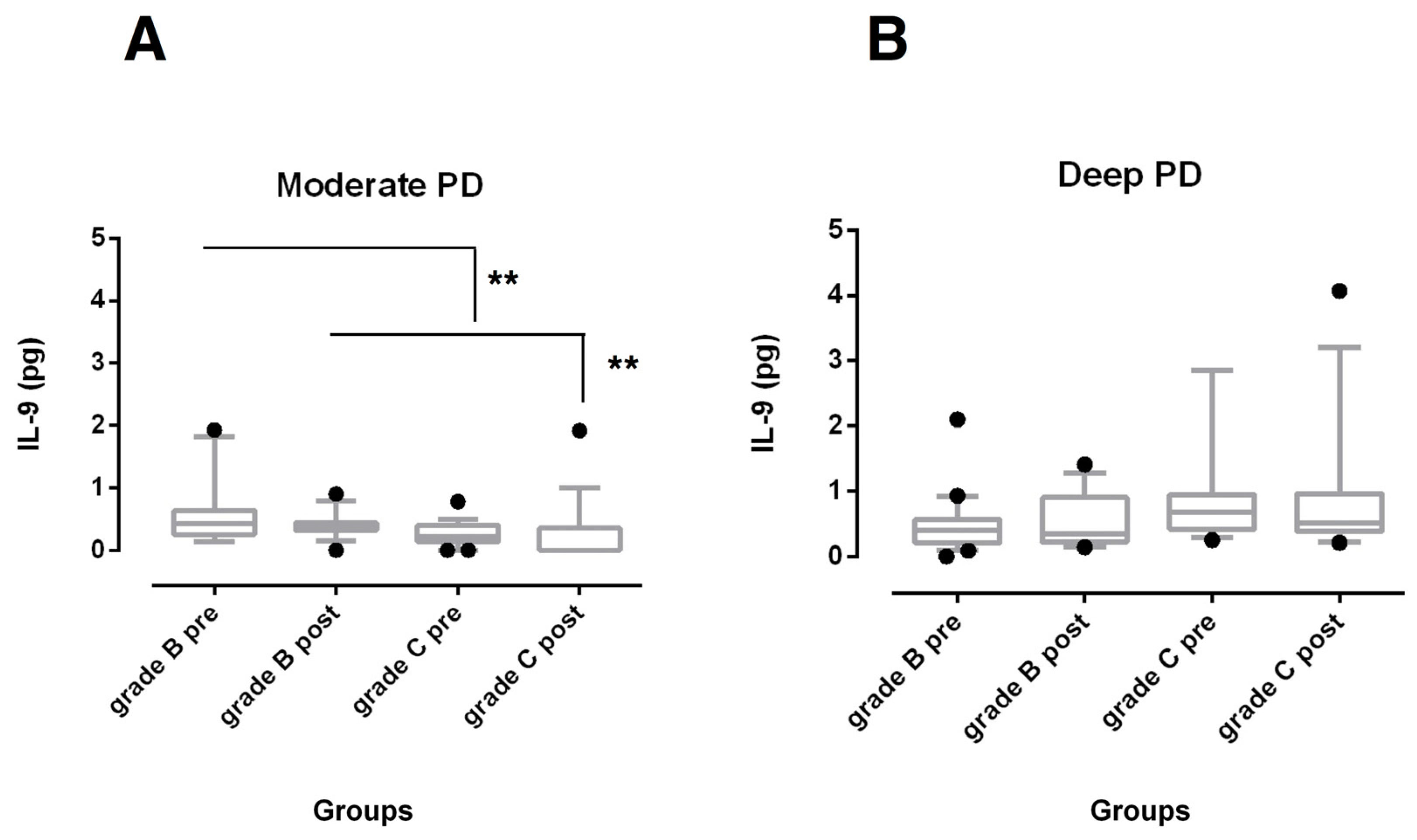
3.2. Biochemical Findings
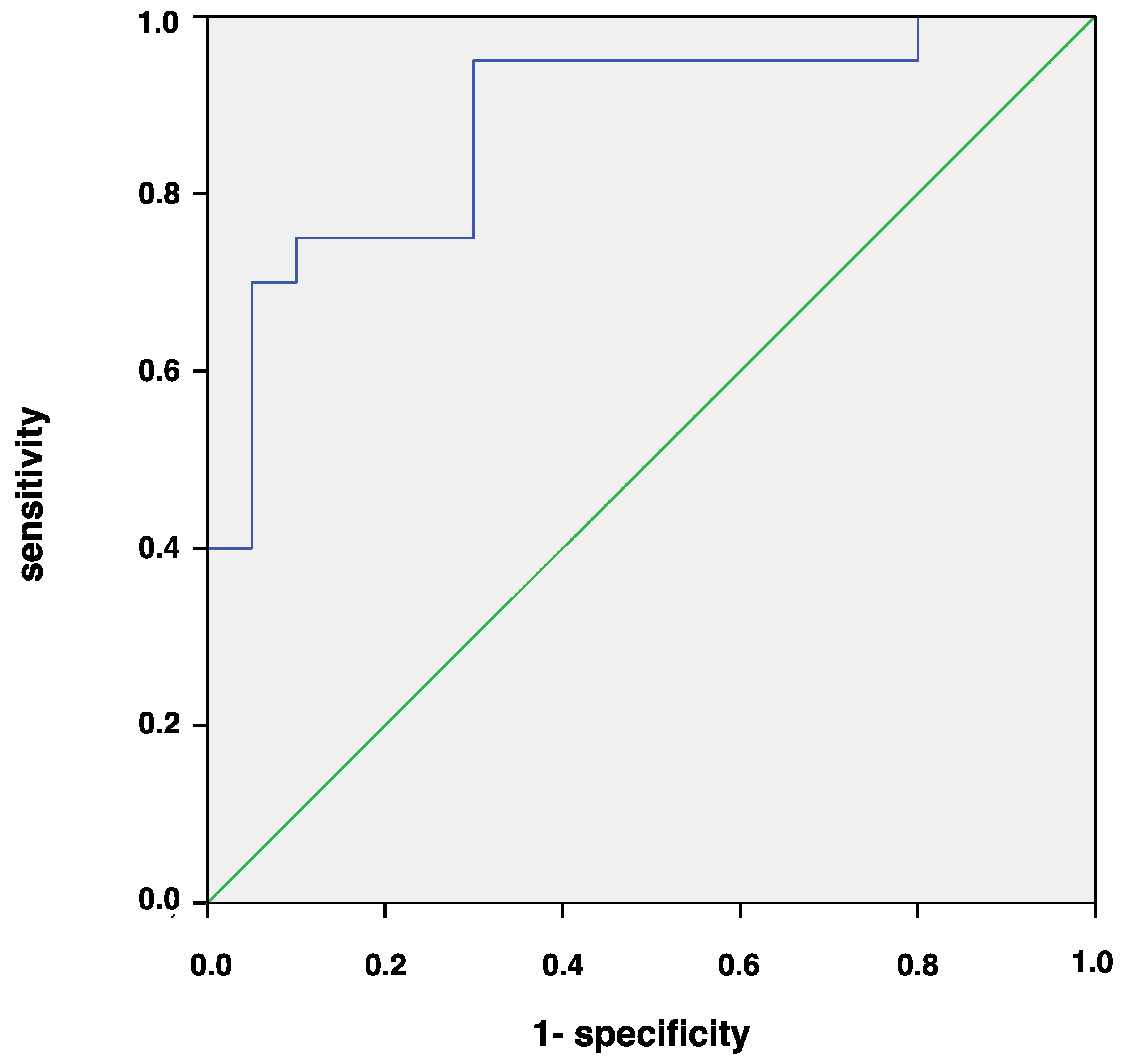
3.3. Correlation and ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hajishengallis, G.; Korostoff, J.M. Revisiting the Page & Schroeder model: The good, the bad and the unknowns in the periodontal host response 40 years later. Periodontology 2000 2017, 75, 116–151. [Google Scholar] [PubMed]
- Preshaw, P.M.; Taylor, J.J. How has research into cytokine interactions and their role in driving immune responses impacted our understanding of periodontitis? J. Clin. Periodontol. 2011, 38 (Suppl. 11), 60–84. [Google Scholar] [CrossRef]
- Loe, H.; Theilade, E.; Jensen, S.B. Experimental gingivitis in man. J. Periodontol. 1965, 36, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Tatakis, D.N.; Scapoli, C.; Bottega, S.; Orlandini, E.; Tosi, M. Modulation of clinical expression of plaque-induced gingivitis. II. Identification of “high-responder” and “low-responder” subjects. J. Clin. Periodontol. 2004, 31, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Danielsen, B.; Baelum, V.; Lopez, R. Identification of inflammatory response patterns in experimental gingivitis studies. Eur. J. Oral Sci. 2019, 127, 33–39. [Google Scholar] [CrossRef]
- Bostanci, N.; Silbereisen, A.; Bao, K.; Grossmann, J.; Nanni, P.; Fernandez, C.; Nascimento, G.G. Salivary proteotypes of gingivitis tolerance and resilience. J. Clin. Periodontol. 2020, 47, 1304–1316. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- Van Dyke, T.E. Inflammation and periodontal diseases: A reappraisal. J. Periodontol. 2008, 79, 1501–1502. [Google Scholar] [CrossRef]
- Barros, S.P.; Williams, R.; Offenbacher, S.; Morelli, T. Gingival crevicular fluid as a source of biomarkers for periodontitis. Periodontology 2000 2016, 70, 53–64. [Google Scholar] [CrossRef]
- Buduneli, N.; Kinane, D.F. Host-derived diagnostic markers related to soft tissue destruction and bone degradation in periodontitis. J. Clin. Periodontol. 2011, 38 (Suppl. 11), 85–105. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Oh, M.; Braun, T.M.; Ramseier, C.A.; Sugai, J.V.; Giannobile, W.V. Crevicular fluid biomarkers and periodontal disease progression. J. Clin. Periodontol. 2014, 41, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Thunell, D.H.; Tymkiw, K.D.; Johnson, G.K.; Joly, S.; Burnell, K.K.; Cavanaugh, J.E.; Brogden, K.A.; Guthmiller, J.M. A multiplex immunoassay demonstrates reductions in gingival crevicular fluid cytokines following initial periodontal therapy. J. Periodontal Res. 2010, 45, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Türer, C.C.; Durmus, D.; Balli, U.; Güven, B. Effect of non-surgical periodontal treatment on gingival crevicular fluid and serum endocan, vascular endhotelial growth factor-A, and tumor necrosis factor-alpha levels. J. Periodontol. 2017, 88, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.P.L.; Faveri, M.; Gursky, L.C.; Mestnik, M.J.; Haffajee, A.D.; Socransky, S.S.; Teles, R.P. Effects of periodontal therapy on GCF cytokines in generalized aggressive periodontitis subjects. J. Clin. Periodontol. 2012, 39, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Zekeridou, A.; Giannopoulou, C.; Cancela, J.; Courvoisier, D.; Mombelli, A. Effect of initial periodontal therapy on gingival crevicular fluid cytokine profile in subjects with chronic periodontitis. Clin. Exp. Dent. Res. 2017, 3, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Development of a classification system for periodontal diseases and conditions. Ann. Periodontol. 1999, 4, 1–6. [Google Scholar] [CrossRef]
- Risau, W.; Flamme, I. Vasculogenesis. Annu. Rev. Cell. Dev. Biol. 1995, 11, 73–91. [Google Scholar] [CrossRef]
- Shibuya, M. Vascular endothelial growth factor and its receptor system: Physiological functions in angiogenesis and pathological roles in various diseases. J. Biochem. 2013, 153, 13–19. [Google Scholar] [CrossRef]
- Prapulla, D.V.; Sujatha, P.B.; Pradeep, A.R. Gingival crevicular fluid VEGF levels in periodontal health and disease. J. Periodontol. 2007, 78, 1783–1787. [Google Scholar] [CrossRef]
- Afacan, B.; Öztürk, V.Ö.; Paşalı, Ç.; Bozkurt, E.; Köse, T.; Emingil, G. Gingival crevicular fluid and salivary HIF-1α, VEGF, and TNF-α levels in periodontal health and disease. J. Periodontol. 2019, 90, 788–797. [Google Scholar]
- Pradeep, A.; Prapulla, D.; Sharma, A.; Sujatha, P. Gingival crevicular fluid and serum vascular endothelial growth factor: Their relationship in periodontal health, disease and after treatment. Cytokine 2011, 54, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Romano, F.; Bongiovanni, L.; Bianco, L.; Di Scipio, F.; Yang, Z.; Sprio, A.E.; Berta, G.N.; Aimetti, M. Biomarker levels in gingival crevicular fluid of generalized aggressive periodontitis patients after non-surgical periodontal treatment. Clin. Oral. Investig. 2018, 22, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.; Hübner, G.; Breier, G.; Longaker, M.T.; Greenhalgh, D.G.; Werner, S. Regulation of vascular endothelial growth factor expression in cultured keratinocytes. Implications for normal and impaired wound healing. J. Biol. Chem. 1995, 270, 12607–12613. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Cappelli, D. Acute-phase reactants in infections and inflammatory diseases. Periodontology 2000 2000, 23, 19–49. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Cochran, D. The contribution of interleukin-1 and tumor necrosis factor to periodontal tissue destruction. J. Periodontol. 2003, 74, 391–401. [Google Scholar] [CrossRef]
- Gemmell, E.; Seymour, G.J. Immunoregulatory control of Th1/Th2 cytokine profiles in periodontal disease. Periodontology 2000 2004, 35, 21–24. [Google Scholar] [CrossRef]
- Jager, A.; Kuchroo, V.K. Effector and regulatory T-cell subsets in autoimmunity and tissue inflammation. Scand. J. Immunol. 2010, 72, 173–184. [Google Scholar] [CrossRef]
- Aranha, A.M.; Repeke, C.E.; Garlet, T.P.; Vieira, A.E.; Campanelli, A.P.; Trombone, A.P.; Letra, A.; Silva, R.M.; Garlet, G. P Evidence supporting a protective role for Th9 and Th22 cytokines in human and experimental periapical lesions. J. Endod. 2013, 39, 83–87. [Google Scholar] [CrossRef]
- Araujo-Pires, A.C.; Francisconi, C.F.; Biguetti, C.C.; Cavalla, F.; Aranha, A.M.; Letra, A.; Trombone, A.P.; Faveri, M.; Silva, R.M.; Garlet, G.P. Simultaneous analysis of T helper subsets (Th1, Th2, Th9, Th17, Th22 Tfh, Tr1 and Tregs) markers expression in periapical lesions reveals multiple cytokine clusters accountable for lesions activity and inactivity status. J. Appl. Oral Sci. 2014, 22, 336–346. [Google Scholar] [CrossRef]
- Tözüm, T.F.; Hatipoğlu, H.; Yamalik, N.; Gürsel, M.; Alptekin, N.O.; Ataoğlu, T.; Marakoğlu, I.; Gürsoy, U.K.; Eratalay, K. Critical steps in electronic volume quantification of gingival crevicular fluid: The potential impact of evaporation, fluid retention, local conditions and repeated measurements. J. Periodontal Res. 2004, 39, 344–357. [Google Scholar] [CrossRef]
- Swet, J.A. Measuring the accuracy of diagnostic systems. Science 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Duarte, P.M.; Bastos, M.F.; Fermiano, D.; Rabelo, C.C.; Perez-Chaparro, P.J.; Figueiredo, L.C.; Faveri, M.; Feres, M. Do subjects with aggressive and chronic periodontitis exhibit a different cytokine chemokine profile in the gingival crevicular fluid? A systematic review. J. Periodontal Res. 2015, 50, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Ghallab, N.A. Diagnostic potential and future directions of biomarkers in gingival crevicular fluid and saliva of periodontal diseases: Review of the current evidence. Arch. Oral. Biol. 2018, 87, 115–124. [Google Scholar] [CrossRef]
- Bostanci, N.; Belibasakis, G.N. Gingival crevicular fluid and immune mediators. Periodontology 2000 2017, 76, 68–84. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.J.; Chen, Y.L.; Kuo, M.Y.; Li, C.L.; Lu, H.K. Measurement of gp130 cytokines oncostatin M and IL-6 in gingival crevicular fluid of patients with chronic periodontitis. Cytokine 2005, 30, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.C.; Douglass, C.W. Meta-analysis of the effect of scaling and root planing, surgical treatment and antibiotic therapies on periodontal probing depth and attachment loss. J. Clin. Periodontol. 2002, 29, 975–986. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.B.; Serio, F.G.; Dai, X. Vascular endothelial growth factors and progression of periodontal diseases. J. Periodontol. 1999, 70, 848–852. [Google Scholar] [CrossRef]
- Keles, G.C.; Cetinkaya, B.O.; Eroglu, C.; Simsek, S.B.; Kahraman, H. Vascular endothelial growth factor expression levels of gingiva in gingivitis and periodontitis patients with/without diabetes mellitus. Inflamm. Res. 2010, 59, 543–549. [Google Scholar] [CrossRef]
- Cetinkaya, B.O.; Keles, G.C.; Ayas, B.; Sakallioglu, E.E.; Acikgoz, G. The expression of vascular endothelial growth factor in a rat model at destruction and healing stages of periodontal disease. J. Periodontol. 2007, 78, 1129–1135. [Google Scholar] [CrossRef]
- Booth, V.; Young, S.; Cruchley, A.; Taichman, N.S.; Paleolog, E. Vascular endothelial growth factor in human periodontal disease. J. Periodontal Res. 1998, 33, 491–499. [Google Scholar] [CrossRef]
- Engebretson, S.P.; Lamster, I.B.; Herrera-Abreu, M.; Celenti, R.S.; Timms, J.M.; Chaudhary, A.G.; di Giovine, F.S.; Kornman, K.S. The influence of interleukin gene polymorphism on expression of interleukin-1beta and tumor necrosis factor-alpha in periodontal tissue and gingival crevicular fluid. J. Periodontol. 1999, 70, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Konopka, L.; Pietrzak, A.; Brzezinska-Blaszczyk, E. Effect of scaling and root planing on interleukin-1beta, interleukin-8 and MMP-8 levels in gingival crevicular fluid from chronic periodontitis patients. J. Periodontal Res. 2012, 47, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Chaves, E.S.; Wood, R.C.; Jones, A.A.; Newbold, D.A.; Manwell, M.A.; Kornman, K.S. Relationship of “bleeding on probing” and “gingival index bleeding” as clinical parameters of gingival inflammation. J. Clin. Periodontol. 1993, 20, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Villa, S.; Sanz-Martín, I.; Maldonado, E.; Virto, L.; Sanz-Esporrín, J.; Sanz, M. Immunohistochemical, histomorphometric, and gingival crevicular fluid analysis of residual and shallow periodontal pockets in patients with periodontitis stages III and IV. J. Periodontol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Reiss, C.; Da Costa, A.V.; Guimarães, J.T.; Tuna, D.; Braga, A.C.; Pacheco, J.J.; Arosa, F.A.; Salazar, F.; Cardoso, E.M. Clinical improvement following therapy for periodontitis: Association with a decrease in IL-1 and IL-6. Exp. Ther. Med. 2014, 8, 323–327. [Google Scholar] [CrossRef]
- Madureira, D.F.; De Abreu Lima, I.L.; Costa, G.C.; Bastos Lages, E.M.; Martins, C.C.; Da Silva, T.A. Tumour necrosis factor-alpha in gingival crevicular fluid as a diagnostic marker for periodontal diseases: A systematic review. J. Evid. Base Dent. Pract. 2018, 18, 315–331. [Google Scholar] [CrossRef]
- Bastos, M.F.; Lima, J.A.; Vieira, P.M.; Mestnik, M.J.; Faveri, M.; Duarte, P.M. TNF-α and IL-4 levels in generalized aggressive periodontitis subjects. Oral Dis. 2009, 15, 82–87. [Google Scholar] [CrossRef]
- Khan, I.H.; Krishnan, V.V.; Ziman, M.; Janatpour, K.; Wun, T.; Luciw, P.A.; Tuscano, J. A comparison of multiplex suspension array large-panel kits for profiling cytokines and chemokines in rheumatoid arthritis patients. Cytom. B Clin. Cytom. 2009, 76, 159–168. [Google Scholar] [CrossRef]
- Díaz-Zúñiga, J.; Melgar-Rodríguez, S.; Rojas, L.; Alvarez, C.; Monasterio, G.; Carvajal, P.; Vernal, R. Increased levels of the T-helper 22-associated cytokine (interleukin-22) and transcription factor (aryl hydrocarbon receptor) in patients with periodontitis are associated with osteoclast resorptive activity and severity of the disease. J. Periodontal Res. 2017, 52, 893–902. [Google Scholar] [CrossRef]
- Tan, C.; Aziz, M.K.; Lovaas, J.D.; Vistica, V.P.; Shi, G.; Wawrousek, E.F.; Gery, I. Antigen-specific Th9 cells exhibit uniqueness in their kinetics of cytokine production and short retention at the inflammatory site. J. Immunol. 2010, 185, 6795–6801. [Google Scholar] [CrossRef]
- Arias-Bujanda, N.; Regueira-Iglesias, A.; Alonso-Sampedo, M.; González-Peteiro, M.M.; Mira, A.; Balsa-Castro, C.; Tomás, I. Cytokine thresholds in gingival crevicular fluid with potential diagnosis of chronic periodontitis differentiating by smoking status. Sci. Rep. 2018, 8, 18003. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Thurnheer, T.; Bostanci, N. Interleukin-8 responses of multi-layer gingival epithelia to subgingival biofilms: Role of the ‘red complex’ species. PLoS ONE 2013, 8, e81581. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Yao, Y.; Jiao, K.; Zhang, J.; Zheng, X.; Wu, F.; Hu, X.; Li, J.; Yu, Z.; Zhang, G.; et al. Relationship between gingival crevicular fluid microbiota and cytokine profile in periodontal host homeostasis. Front. Microbiol. 2017, 8, 2144. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Braun, T.; Ramseier, C.A.; Herr, A.E.; Sugai, J.V.; Shelburne, C.E.; Rayburn, L.A.; Singh, A.K.; Giannobile, W.V. Saliva/pathogen biomarker signatures and periodontal disease progression. J. Dent. Res. 2011, 90, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Tymkiw, K.D.; Thunell, D.H.; Johnson, G.K.; Joly, S.; Burnell, K.K.; Cavanaugh, J.E.; Brodgen, K.A.; Guthmiller, J.M. Influence of smoking on gingival crevicular fluid cytokines in severe chronic periodontitis. J. Clin. Periodontol. 2011, 38, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Eickholz, P.; Siegelin, Y.; Scharf, S.; Schacher, B.; Oremek, G.M.; Sauer-Eppel, H.; Schubert, R.; Wohlfeil, M. Non-surgical periodontal therapy decreases serum elastase levels in aggressive but not in chronic periodontitis. J. Clin. Periodontol. 2013, 40, 327–333. [Google Scholar] [CrossRef]
- Stowe, R.P.; Peek, M.K.; Cutchin, M.P.; Goodwin, J.S. Plasma cytokine levels in a population-based study: Relation to age and ethnicity. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 65, 429–433. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group | Baseline | 6 Months | Δ0–6 months |
|---|---|---|---|---|
| FMPS (%) | Stage B | 71.7 ± 15.9 | 14.6 ± 4.9 *** | 57.1 ± 17.7 |
| Stage C | 74.5 ± 25.6 | 13.3 ± 4.6 *** | 61.2 ± 24.8 | |
| Difference between groups | NS | NS | ||
| FMBS (%) | Stage B | 56.0 ± 20.7 | 13.6 ± 4.8 *** | 42.4 ± 19.6 |
| Stage C | 63.8 ± 23.0 | 16.1 ± 4.4 *** | 47.7 ± 22.7 | |
| Difference between groups | NS | NS | ||
| PD (mm) | Stage B | 4.6 ± 0.7 | 3.4 ± 0.4 *** | 1.2 ± 0.5 |
| Stage C | 4.9 ± 0.5 | 3.6 ± 0.6 *** | 1.3 ± 0.4 | |
| Difference between groups | NS | NS | ||
| CAL (mm) | Stage B | 5.3 ± 1.0 | 4.4 ± 0.8 *** | 0.9 ± 0.4 |
| Stage C | 5.6 ± 0.9 | 4.5 ± 0.7 *** | 1.2 ± 0.6 | |
| Difference between groups | NS | NS |
| Variables | Group | Moderate Pocket Sites (4–5 mm) | Deep Pocket Sites (≥6 mm) | ||
|---|---|---|---|---|---|
| Baseline | 6 Months | Baseline | 6 Months | ||
| PI | Stage B | 85.0 ± 23.5 | 10.0 ± 20.5 *** | 92.5 ± 18.3 | 25.0 ± 30.3 *** |
| Stage C | 77.5 ± 25.5 ¶ | 15.0 ± 28.6 *** | 95.0 ± 15.4 | 20.0 ± 29.9 *** | |
| Difference between groups | NS | NS | NS | NS | |
| GI | Stage B | 2.0 ± 0.5 ¶ | 0.6 ± 0.5 *** | 2.6 ± 0.5 | 0.9 ± 0.8 *** |
| Stage C | 1.8 ± 0.4 ¶ | 0.4 ± 0.6 *** | 2.4 ± 0.4 | 0.8 ± 0.7 *** | |
| Difference between groups | NS | NS | NS | NS | |
| PD (mm) | Stage B | 4.7 ± 0.5 | 3.0 ± 1.0 *** | 8.2 ± 1.4 | 4.5 ± 0.9 ***,§ |
| Stage C | 4.8 ± 0.4 | 3.2 ± 0.6 *** | 8.9 ± 1.7 | 4.9 ± 1.0 ***,§ | |
| Difference between groups | NS | NS | NS | NS | |
| CAL (mm) | Stage B | 5.8 ± 1.4 | 4.5 ± 1.8 ** | 9.3 ± 2.1 | 6.4 ± 2.1 **,§ |
| Stage C | 5.3 ± 0.7 | 4.1 ± 1.1 *** | 9.6 ± 1.9 | 6.6 ± 1.4 ***,§ | |
| Difference between groups | NS | NS | NS | NS | |
| GCF (µL) | Stage B | 0.56 ± 0.36 | 0.22 ± 0.15 ** | 1.09 ± 0.25 § | 0.45 ± 0.21 ***,§ |
| Stage C | 0.59 ± 0.39 | 0.27 ± 0.20 * | 1.13 ± 0.33 § | 0.54 ± 0.31 **,¶ | |
| Difference between groups | NS | NS | NS | NS | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, F.; Del Buono, W.; Bianco, L.; Arena, M.; Mariani, G.M.; Di Scipio, F.; Berta, G.N.; Aimetti, M. Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression. Biomedicines 2020, 8, 515. https://doi.org/10.3390/biomedicines8110515
Romano F, Del Buono W, Bianco L, Arena M, Mariani GM, Di Scipio F, Berta GN, Aimetti M. Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression. Biomedicines. 2020; 8(11):515. https://doi.org/10.3390/biomedicines8110515
Chicago/Turabian StyleRomano, Federica, Wilma Del Buono, Laura Bianco, Martina Arena, Giulia Maria Mariani, Federica Di Scipio, Giovanni Nicolao Berta, and Mario Aimetti. 2020. "Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression" Biomedicines 8, no. 11: 515. https://doi.org/10.3390/biomedicines8110515
APA StyleRomano, F., Del Buono, W., Bianco, L., Arena, M., Mariani, G. M., Di Scipio, F., Berta, G. N., & Aimetti, M. (2020). Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression. Biomedicines, 8(11), 515. https://doi.org/10.3390/biomedicines8110515