
An Interpretable Machine Learning Model Based on Inflammatory–Nutritional Biomarkers for Predicting Metachronous Liver Metastases After Colorectal Cancer Surgery

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Research Methods
2.4. Data Analysis
3. Results
3.1. Patient Characteristics
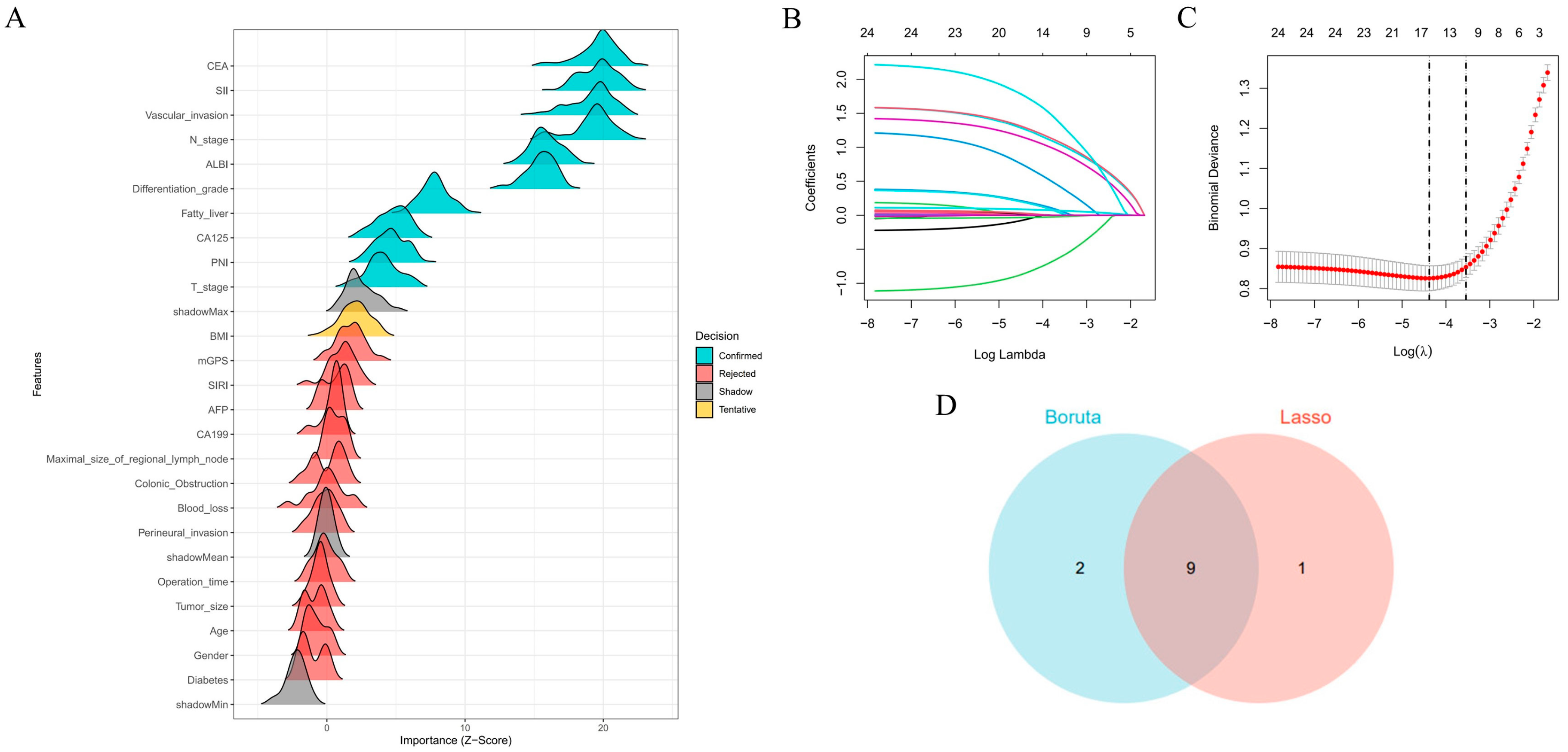
3.2. Feature Selection
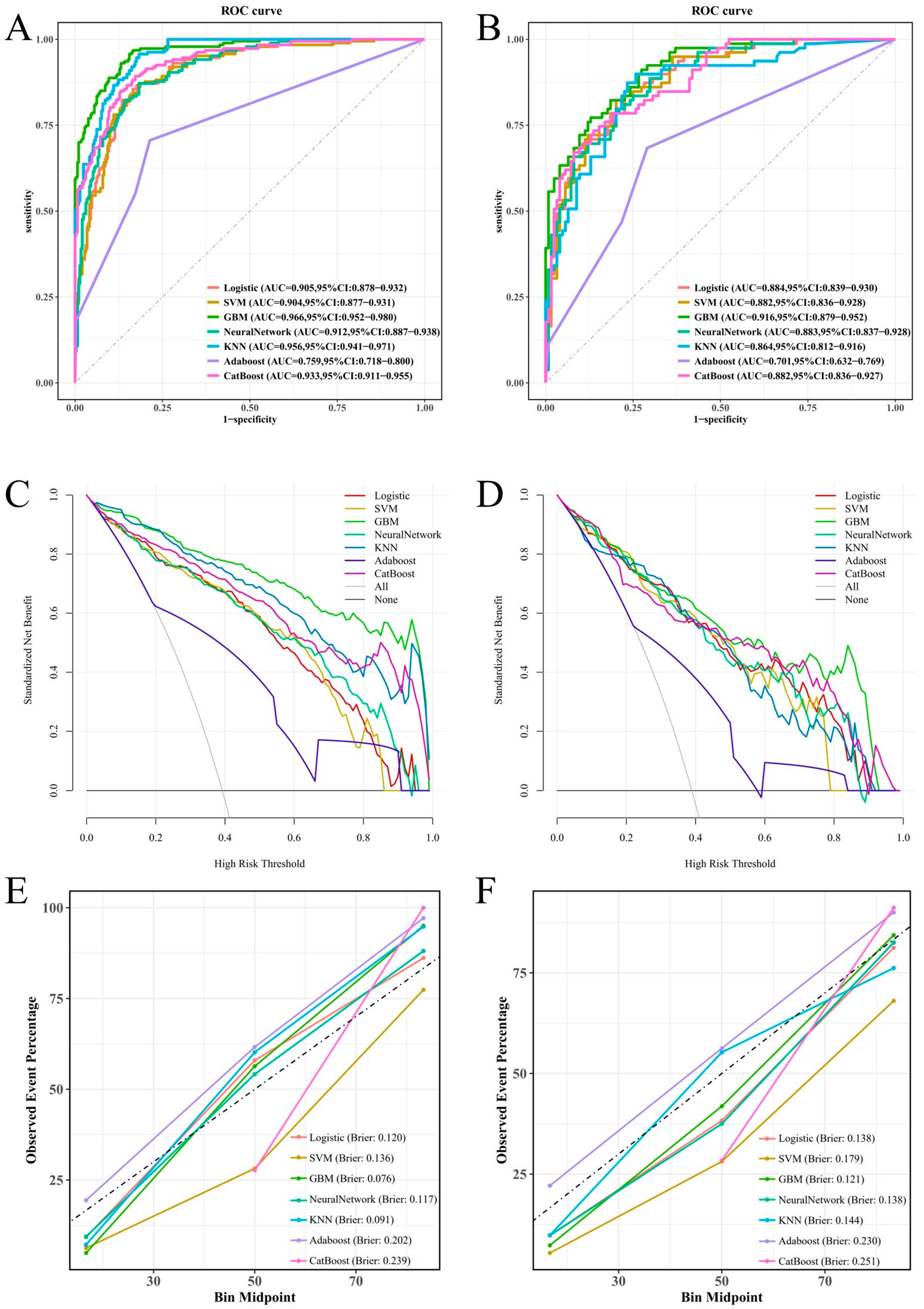
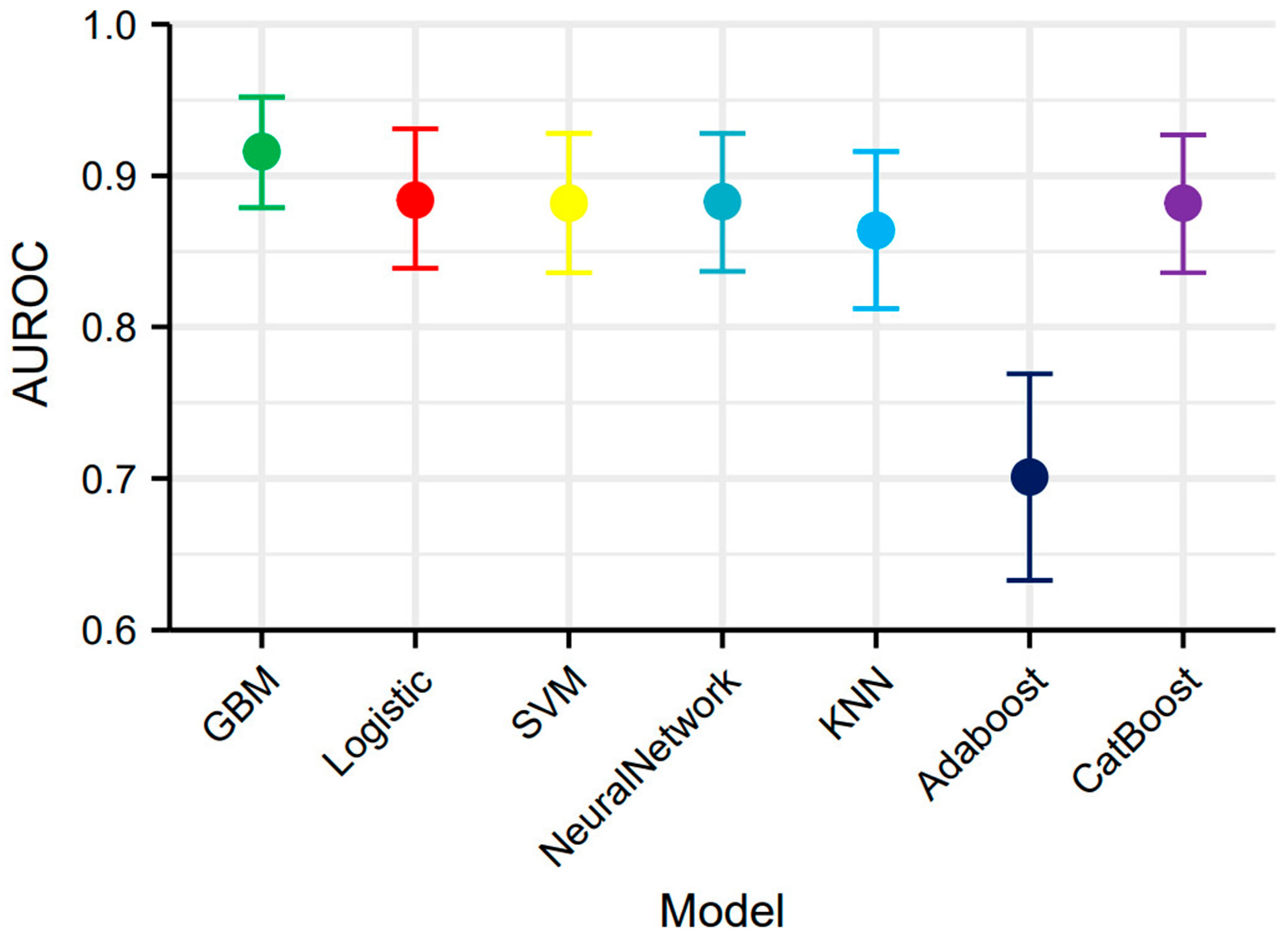
3.3. Constructing and Validating Models
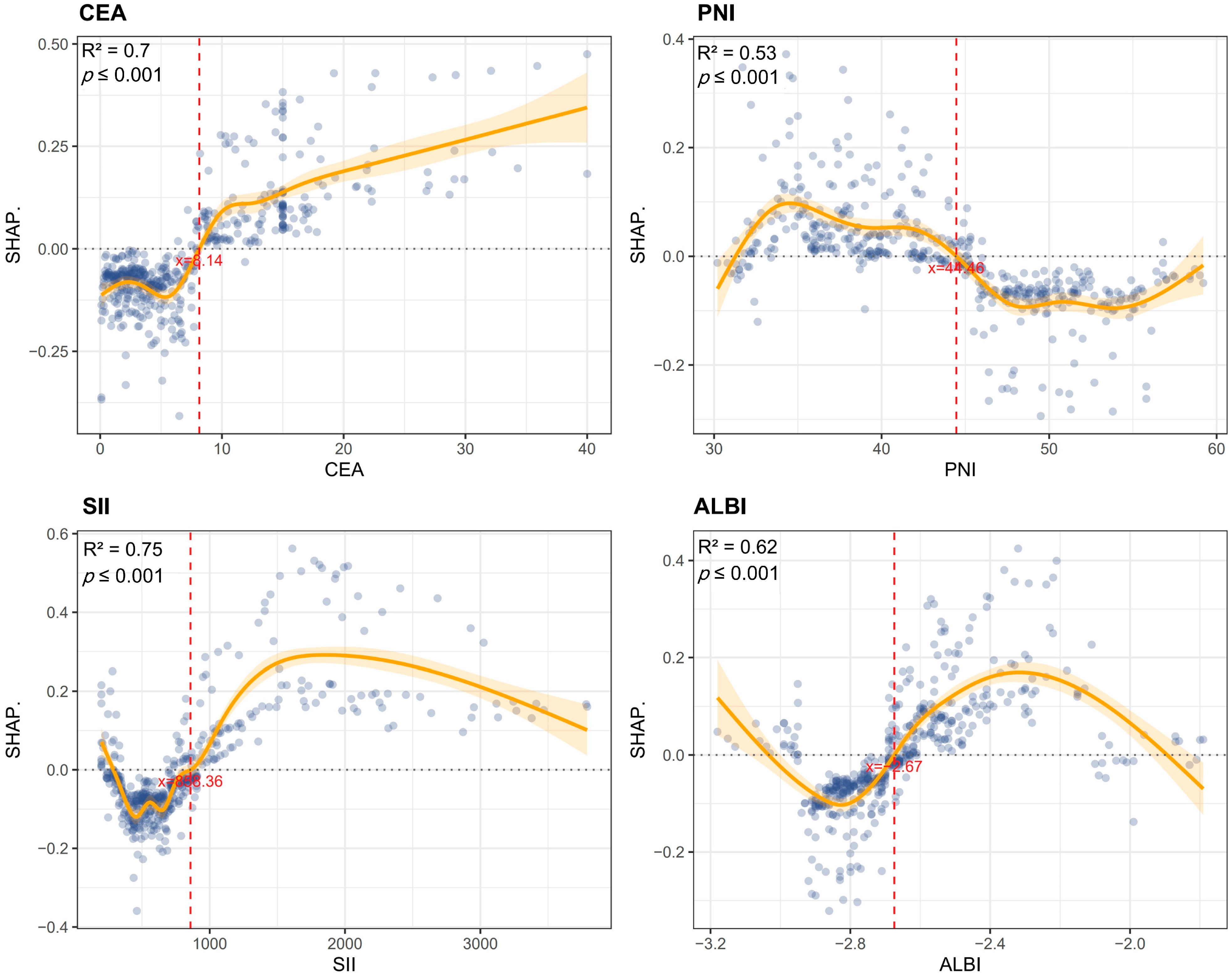
3.4. Feature Contribution Analysis via SHAP Values
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cao, W.; Chen, H.-D.; Yu, Y.-W.; Li, N.; Chen, W.-Q. Changing profiles of cancer burden worldwide and in China: A secondary analysis of the global cancer statistics 2020. Chin. Med. J. 2021, 134, 783–791. [Google Scholar] [CrossRef]
- Wu, K.; Zhang, G.; Shen, C.; Zhu, L.; Yu, C.; Sartorius, K.; Ding, W.; Jiang, Y.; Lu, Y. Role of T cells in liver metastasis. Cell Death Dis. 2024, 15, 341. [Google Scholar] [CrossRef]
- Wang, J.-C.; Liu, Y.-H.; Jiang, B.-B.; Shao, L.-J.; Wang, S.; Yang, W.; Wu, W.; Yan, K.; Zhang, Z.-Y. Prospective analysis of the effects of RAS mutation on local tumor progression and overall survival after radiofrequency ablation for colorectal liver metastases. Int. J. Hyperth. 2024, 41, 2438852. [Google Scholar] [CrossRef]
- Lupinacci, R.M.; Andraus, W.; Haddad, L.B.D.P.; D′Albuquerque, L.A.C.; Herman, P. Simultaneous laparoscopic resection of primary colorectal cancer and associated liver metastases: A systematic review. Tech. Coloproctol. 2014, 18, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Bhullar, D.S.; Barriuso, J.; Mullamitha, S.; Saunders, M.P.; O’Dwyer, S.T.; Aziz, O. Biomarker concordance between primary colorectal cancer and its metastases. eBioMedicine 2019, 40, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Pietrocola, F.; Kroemer, G. Nutrition, inflammation and cancer. Nat. Immunol. 2017, 18, 843–850. [Google Scholar] [CrossRef]
- Maiorino, L.; Daßler-Plenker, J.; Sun, L.; Egeblad, M. Innate Immunity and Cancer Pathophysiology. Annu. Rev. Pathol. 2022, 17, 425–457. [Google Scholar] [CrossRef]
- Ho, C.-T.; Tan, E.C.-H.; Lee, P.-C.; Chu, C.-J.; Huang, Y.-H.; Huo, T.-I.; Hou, M.-C.; Wu, J.-C.; Su, C.-W. Prognostic Nutritional Index as a Prognostic Factor for Very Early-Stage Hepatocellular Carcinoma. Clin. Transl. Gastroenterol. 2024, 15, e00678. [Google Scholar] [CrossRef]
- Jing, Y.; Ren, M.; Li, X.; Sun, X.; Xiao, Y.; Xue, J.; Liu, Z. The Effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Early Gastric Cancer. J. Inflamm. Res. 2024, 17, 10273–10287. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Li, J.; Zhu, N.; Wang, C.; You, L.; Guo, W.; Yuan, Z.; Qi, S.; Zhao, H.; Yu, J.; Huang, Y. Preoperative albumin-to-globulin ratio and prognostic nutritional index predict the prognosis of colorectal cancer: A retrospective study. Sci. Rep. 2023, 13, 17272. [Google Scholar] [CrossRef]
- Lu, Z.; Sun, J.; Wang, M.; Jiang, H.; Chen, G.; Zhang, W. A nomogram prediction model based on clinicopathological combined radiological features for metachronous liver metastasis of colorectal cancer. J. Cancer 2024, 15, 916–925. [Google Scholar] [CrossRef] [PubMed]
- Bertsimas, D.; Wiberg, H. Machine Learning in Oncology: Methods, Applications, and Challenges. JCO Clin. Cancer Inform. 2020, 4, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhang, Z.; Liu, L.; Zhao, Y.; Liu, Z.; Zhang, C.; Qi, H.; Feng, J.; Yang, C.; Tai, W.; et al. Machine learning for predicting liver and/or lung metastasis in colorectal cancer: A retrospective study based on the SEER database. Eur. J. Surg. Oncol. 2024, 50, 108362. [Google Scholar] [CrossRef]
- Xing, Y.; Yu, G.; Jiang, Z.; Wang, Z. Development of prediction models for liver metastasis in colorectal cancer based on machine learning: A population-level study. Transl. Cancer Res. 2024, 13, 5943–5952. [Google Scholar] [CrossRef] [PubMed]
- Cabitza, F.; Rasoini, R.; Gensini, G.F. Unintended Consequences of Machine Learning in Medicine. JAMA 2017, 318, 517–518. [Google Scholar] [CrossRef]
- Loh, H.W.; Ooi, C.P.; Seoni, S.; Barua, P.D.; Molinari, F.; Acharya, U.R. Application of explainable artificial intelligence for healthcare: A systematic review of the last decade (2011–2022). Comput. Methods Programs Biomed. 2022, 226, 107161. [Google Scholar] [CrossRef]
- Wang, X.; Ren, J.; Ren, H.; Song, W.; Qiao, Y.; Zhao, Y.; Linghu, L.; Cui, Y.; Zhao, Z.; Chen, L.; et al. Diabetes mellitus early warning and factor analysis using ensemble Bayesian networks with SMOTE-ENN and Boruta. Sci. Rep. 2023, 13, 12718. [Google Scholar] [CrossRef]
- Emmanuel, T.; Maupong, T.; Mpoeleng, D.; Semong, T.; Mphago, B.; Tabona, O. A survey on missing data in machine learning. J. Big Data 2021, 8, 140. [Google Scholar] [CrossRef]
- Yin, X.; Ma, X.; Sun, P.; Shen, D.; Tang, Z. A novel nomogram based on inflammatory-nutritional biomarkers for gallbladder cancer after surgical resection. BMC Gastroenterol. 2024, 24, 289. [Google Scholar] [CrossRef]
- Zhu, J.; Wang, D.; Liu, C.; Huang, R.; Gao, F.; Feng, X.; Lan, T.; Li, H.; Wu, H. Development and validation of a new prognostic immune-inflammatory-nutritional score for predicting outcomes after curative resection for intrahepatic cholangiocarcinoma: A multicenter study. Front. Immunol. 2023, 14, 1165510. [Google Scholar] [CrossRef]
- Liu, Z.; Yuan, H.; Suo, C.; Zhao, R.; Jin, L.; Zhang, X.; Zhang, T.; Chen, X. Point-based risk score for the risk stratification and prediction of hepatocellular carcinoma: A population-based random survival forest modeling study. eClinicalMedicine 2024, 75, 102796. [Google Scholar] [CrossRef] [PubMed]
- Spinella, R.; Sawhney, R.; Jalan, R. Albumin in chronic liver disease: Structure, functions and therapeutic implications. Hepatol. Int. 2016, 10, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Thurnham, D.I. Interactions between nutrition and immune function: Using inflammation biomarkers to interpret micronutrient status. Proc. Nutr. Soc. 2014, 73, 1–8. [Google Scholar] [CrossRef]
- Karin, M. Nuclear factor-κB in cancer development and progression. Nature 2006, 441, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef]
- Shrihari, T.G. Innate and adaptive immune cells in Tumor microenvironment. Gulf J. Oncol. 2021, 1, 77–81. [Google Scholar]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef]
- Stotz, M.; Pichler, M.; Absenger, G.; Szkandera, J.; Arminger, F.; Schaberl-Moser, R.; Samonigg, H.; Stojakovic, T.; Gerger, A. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br. J. Cancer 2014, 110, 435–440. [Google Scholar] [CrossRef]
- Beyer, M.; Schultze, J.L. Regulatory T cells in cancer. Blood 2006, 108, 804–811. [Google Scholar] [CrossRef]
- Quigley, D.A.; Kristensen, V. Predicting prognosis and therapeutic response from interactions between lymphocytes and tumor cells. Mol. Oncol. 2015, 9, 2054–2062. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.C.; Chou, J.F.; Strong, V.E.; Brennan, M.F.; Capanu, M.; Coit, D.G. Pretreatment Neutrophil to Lymphocyte Ratio Independently Predicts Disease-specific Survival in Resectable Gastroesophageal Junction and Gastric Adenocarcinoma. Ann. Surg. 2016, 263, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Wang, X.; Yao, W.; Shi, D.; Shao, X.; Lu, Z.; Chai, Y.; Song, J.; Tang, W.; Wang, X. Mechanism insights and therapeutic intervention of tumor metastasis: Latest developments and perspectives. Signal Transduct. Target. Ther. 2024, 9, 192. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Matsukane, R.; Watanabe, H.; Hata, K.; Suetsugu, K.; Tsuji, T.; Egashira, N.; Nakanishi, Y.; Okamoto, I.; Ieiri, I. Prognostic significance of pre-treatment ALBI grade in advanced non-small cell lung cancer receiving immune checkpoint therapy. Sci. Rep. 2021, 11, 15057. [Google Scholar] [CrossRef]
- Yagyu, T.; Saito, H.; Sakamoto, T.; Uchinaka, E.; Morimoto, M.; Amisaki, M.; Watanabe, J.; Tokuyasu, N.; Honjo, S.; Ashida, K.; et al. Preoperative Albumin-Bilirubin Grade as a Useful Prognostic Indicator in Patients with Pancreatic Cancer. Anticancer Res. 2019, 39, 1441–1446. [Google Scholar] [CrossRef]
- Liu, Y.; Li, P.; Lu, J.; Xiong, W.; Oger, J.; Tetzlaff, W.; Cynader, M. Bilirubin possesses powerful immunomodulatory activity and suppresses experimental autoimmune encephalomyelitis. J. Immunol. 2008, 181, 1887–1897. [Google Scholar] [CrossRef]
- He, M.; Fang, Z.; Hang, D.; Wang, F.; Polychronidis, G.; Wang, L.; Lo, C.; Wang, K.; Zhong, R.; Knudsen, M.D.; et al. Circulating liver function markers and colorectal cancer risk: A prospective cohort study in the UK Biobank. Int. J. Cancer 2021, 148, 1867–1878. [Google Scholar] [CrossRef]
- Yuan, N.; Li, X.; Wang, M.; Zhang, Z.; Qiao, L.; Gao, Y.; Xu, X.; Zhi, J.; Li, Y.; Li, Z.; et al. Gut Microbiota Alteration Influences Colorectal Cancer Metastasis to the Liver by Remodeling the Liver Immune Microenvironment. Gut Liver 2022, 16, 575–588. [Google Scholar] [CrossRef]
- Lee, H.G.; Lim, S.-B.; Lee, J.L.; Kim, C.W.; Yoon, Y.S.; Park, I.J.; Kim, J.C. Preoperative albumin–bilirubin score as a prognostic indicator in patients with stage III colon cancer. Sci. Rep. 2022, 12, 14910. [Google Scholar] [CrossRef]
- Wang, Q.; Tan, X.; Deng, G.; Fu, S.; Li, J.; Li, Z. Dynamic changes in the systemic immune-inflammation index predict the prognosis of EGFR-mutant lung adenocarcinoma patients receiving brain metastasis radiotherapy. BMC Pulm. Med. 2022, 22, 75. [Google Scholar] [CrossRef]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.-J.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef]
- Polk, N.; Budai, B.; Hitre, E.; Patócs, A.; Mersich, T. High Neutrophil-To-Lymphocyte Ratio (NLR) and Systemic Immune-Inflammation Index (SII) Are Markers of Longer Survival After Metastasectomy of Patients with Liver-Only Metastasis of Rectal Cancer. Pathol. Oncol. Res. 2022, 28, 1610315. [Google Scholar] [CrossRef]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis. Cancer Cell 2011, 20, 576–590. [Google Scholar] [CrossRef]
- Coffelt, S.B.; Wellenstein, M.D.; De Visser, K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.-S.; Ma, X.-F.; Zhao, J.; Du, S.-X.; Zhang, J.; Dong, M.-Z.; Xin, Y.-N. Association between nonalcoholic fatty liver disease and extrahepatic cancers: A systematic review and meta-analysis. Lipids Health Dis. 2020, 19, 118. [Google Scholar] [CrossRef]
- Miyata, T.; Shinden, Y.; Motoyama, S.; Sannomiya, Y.; Tamezawa, H.; Nagayama, T.; Nishiki, H.; Hashimoto, A.; Kaida, D.; Fujita, H.; et al. Non-Alcoholic Fatty Liver Disease May Be a Risk Factor for Liver Metastasis After Radical Surgery for Colorectal Cancer: A Retrospective Study. J. Gastrointest. Cancer 2024, 55, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhang, Y.; Dong, Y.; Zi, R.; Wang, Y.; Chen, Y.; Liu, C.; Wang, J.; Wang, X.; Li, J.; et al. Non-alcoholic fatty liver disease promotes liver metastasis of colorectal cancer via fatty acid synthase dependent EGFR palmitoylation. Cell Death Discov. 2024, 10, 41. [Google Scholar] [CrossRef]
- Murono, K.; Kitayama, J.; Tsuno, N.H.; Nozawa, H.; Kawai, K.; Sunami, E.; Akahane, M.; Watanabe, T. Hepatic steatosis is associated with lower incidence of liver metastasis from colorectal cancer. Int. J. Color. Dis. 2013, 28, 1065–1072. [Google Scholar] [CrossRef]
- Wu, W.; Chen, J.; Ye, W.; Li, X.; Zhang, J. Fatty liver decreases the risk of liver metastasis in patients with breast cancer: A two-center cohort study. Breast Cancer Res. Treat. 2017, 166, 289–297. [Google Scholar] [CrossRef]
- Muzurović, E.; Mikhailidis, D.P.; Mantzoros, C. Non-alcoholic fatty liver disease, insulin resistance, metabolic syndrome and their association with vascular risk. Metabolism 2021, 119, 154770. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.F.; Groom, A.C.; MacDonald, I.C. Dissemination and growth of cancer cells in metastatic sites. Nat. Rev. Cancer 2002, 2, 563–572. [Google Scholar] [CrossRef]
- Karube, H.; Masuda, H.; Hayashi, S.; Ishii, Y.; Nemoto, N. Fatty liver suppressed the angiogenesis in liver metastatic lesions. Hepatogastroenterology 2000, 47, 1541–1545. [Google Scholar] [PubMed]
- Rizeq, B.; Zakaria, Z.; Ouhtit, A. Towards understanding the mechanisms of actions of carcinoembryonic antigen-related cell adhesion molecule 6 in cancer progression. Cancer Sci. 2018, 109, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Bolocan, A.; Ion, D.; Ciocan, D.N.; Paduraru, D.N. Prognostic and predictive factors in colorectal cancer. Chirurgia (Bucur) 2012, 107, 555–563. [Google Scholar]
- Seeberg, L.T.; Brunborg, C.; Waage, A.; Hugenschmidt, H.; Renolen, A.; Stav, I.; Bjørnbeth, B.A.; Borgen, E.; Naume, B.; Brudvik, K.W.; et al. Survival Impact of Primary Tumor Lymph Node Status and Circulating Tumor Cells in Patients with Colorectal Liver Metastases. Ann. Surg. Oncol. 2017, 24, 2113–2121. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort | Training Cohort | Testing Cohort |
|---|---|---|---|
| n = 680 | n = 477 | n = 203 | |
| Gender | |||
| Male | 322 (47.4) | 235 (49.3) | 87 (42.9) |
| Female | 358 (52.6) | 242 (50.7) | 116 (57.1) |
| Diabetes | |||
| Yes | 116 (17.1) | 85 (17.8) | 31 (15.3) |
| No | 564 (82.9) | 392 (82.2) | 172 (84.7) |
| Fatty liver | |||
| Yes | 183 (26.9) | 137 (28.7) | 46 (22.7) |
| No | 497 (73.1) | 340 (71.3) | 157 (77.3) |
| T stage | |||
| T1–2 | 197 (29.0) | 145 (30.4) | 52 (25.6) |
| T3–4 | 483 (71.0) | 332 (69.6) | 151 (74.4) |
| N stage | |||
| N0 | 344 (50.6) | 253 (53.0) | 91 (44.8) |
| N1–2 | 336 (49.4) | 224 (47.0) | 112 (55.2) |
| Differentiation grade | |||
| G1–2 | 521 (76.6) | 366 (76.7) | 155 (76.4) |
| G3–4 | 159 (23.4) | 111 (23.3) | 48 (23.6) |
| Colonic obstruction | |||
| Yes | 106 (15.6) | 76 (15.9) | 30 (14.8) |
| No | 574 (84.4) | 401 (84.1) | 173 (85.2) |
| Vascular invasion | |||
| Yes | 291 (42.8) | 202 (42.3) | 89 (43.8) |
| No | 389 (57.2) | 275 (57.7) | 114 (56.2) |
| Perineural invasion | |||
| Yes | 166 (24.4) | 119 (24.9) | 47 (23.2) |
| No | 514 (75.6) | 358 (75.1) | 156 (76.8) |
| Maximal size of regional lymph node (%) | |||
| <5 mm | 274 (40.3) | 195 (40.9) | 79 (38.9) |
| 5–10 mm | 301 (44.3) | 216 (45.3) | 85 (41.9) |
| >10 mm | 105 (15.4) | 66 (13.8) | 39 (19.2) |
| mGPS (%) | |||
| 0 | 275 (40.4) | 184 (38.6) | 91 (44.8) |
| 1 | 269 (39.6) | 192 (40.3) | 77 (37.9) |
| 2 | 136 (20.0) | 101 (21.2) | 35 (17.2) |
| Age | 66.53 (9.59) | 66.51 (9.13) | 66.60 (10.61) |
| BMI | 22.53 (3.39) | 22.47 (3.35) | 22.68 (3.48) |
| AFP | 3.09 (1.92) | 3.16 (1.97) | 2.92 (1.78) |
| CA125 | 44.39 (104.96) | 41.89 (99.86) | 50.27 (116.13) |
| CA199 | 34.96 (93.03) | 36.79 (95.70) | 30.66 (86.51) |
| CEA | 7.85 (7.18) | 7.67 (6.90) | 8.26 (7.80) |
| Operation time | 208.98 (88.98) | 210.39 (88.76) | 205.65 (89.62) |
| Blood loss | 267.01 (294.69) | 265.53 (291.84) | 270.50 (302.00) |
| SIRI | 1.55 (1.75) | 1.57 (1.76) | 1.50 (1.72) |
| PNI | 43.61 (6.97) | 43.44 (6.98) | 44.03 (6.94) |
| SII | 825.19 (630.17) | 840.36 (639.21) | 789.55 (608.47) |
| ALBI | −2.65 (0.24) | −2.65 (0.23) | −2.63 (0.26) |
| Tumor size | 3.62 (2.03) | 3.66 (2.00) | 3.52 (2.11) |
| Characteristics | Training Cohort | p Overall | ||
|---|---|---|---|---|
| Overall n = 477 | CRC n = 290 | MLM n = 187 | ||
| Gender | 0.39 | |||
| Male | 235 (49.3) | 148 (51.0) | 87 (46.5) | |
| Female | 242 (50.7) | 142 (49.0) | 100 (53.5) | |
| Diabetes | 0.59 | |||
| Yes | 85 (17.8) | 49 (16.9) | 36 (19.3) | |
| No | 392 (82.2) | 241 (83.1) | 151 (80.7) | |
| Fatty liver | <0.001 | |||
| Yes | 137 (28.7) | 107 (36.9) | 30 (16.0) | |
| No | 340 (71.3) | 183 (63.1) | 157 (84.0) | |
| T stage | <0.001 | |||
| T1–2 | 145 (30.4) | 107 (36.9) | 38 (20.3) | |
| T3–4 | 332 (69.6) | 183 (63.1) | 149 (79.7) | |
| N stage | <0.001 | |||
| N0 | 253 (53.0) | 198 (68.3) | 55 (29.4) | |
| N1–2 | 224 (47.0) | 92 (31.7) | 132 (70.6) | |
| Differentiation grade | <0.001 | |||
| G1–2 | 366 (76.7) | 256 (88.3) | 110 (58.8) | |
| G3–4 | 111 (23.3) | 34 (11.7) | 77 (41.2) | |
| Colonic obstruction | 0.23 | |||
| Yes | 76 (15.9) | 41 (14.1) | 35 (18.7) | |
| No | 401 (84.1) | 249 (85.9) | 152 (81.3) | |
| Vascular invasion | <0.001 | |||
| Yes | 202 (42.3) | 79 (27.2) | 123 (65.8) | |
| No | 275 (57.7) | 211 (72.8) | 64 (34.2) | |
| Perineural invasion | 0.4 | |||
| Yes | 119 (24.9) | 68 (23.4) | 51 (27.3) | |
| No | 358 (75.1) | 222 (76.6) | 136 (72.7) | |
| Maximal size of regional lymph node (%) | 0.11 | |||
| <5 mm | 195 (40.9) | 126 (43.4) | 69 (36.9) | |
| 5–10 mm | 216 (45.3) | 131 (45.2) | 85 (45.5) | |
| >10 mm | 66 (13.8) | 33 (11.4) | 33 (17.6) | |
| mGPS (%) | 0.01 | |||
| 0 | 184 (38.6) | 112 (38.6) | 72 (38.5) | |
| 1 | 192 (40.3) | 129 (44.5) | 63 (33.7) | |
| 2 | 101 (21.2) | 49 (16.9) | 52 (27.8) | |
| Age | 66.51 (9.13) | 66.16 (9.14) | 67.04 (9.12) | 0.31 |
| BMI | 22.47 (3.35) | 22.22 (3.21) | 22.87 (3.54) | 0.04 |
| AFP | 3.16 (1.97) | 3.13 (1.89) | 3.20 (2.09) | 0.67 |
| CA125 | 41.89 (99.86) | 48.70 (108.94) | 31.33 (83.03) | 0.06 |
| CA199 | 36.79 (95.70) | 39.41 (102.85) | 32.74 (83.51) | 0.46 |
| CEA | 7.67 (6.90) | 5.93 (5.60) | 10.37 (7.83) | <0.001 |
| Operation time | 210.39 (88.76) | 211.82 (89.63) | 208.18 (87.57) | 0.66 |
| Blood loss | 265.53 (291.84) | 274.03 (312.51) | 252.34 (256.76) | 0.43 |
| SIRI | 1.57 (1.76) | 1.54 (1.79) | 1.61 (1.70) | 0.68 |
| PNI | 43.44 (6.98) | 44.30 (7.18) | 42.09 (6.46) | 0.001 |
| SII | 840.36 (639.21) | 672.90 (433.92) | 1100.05 (800.97) | <0.001 |
| ALBI | −2.65 (0.23) | −2.71 (0.20) | −2.57 (0.25) | <0.001 |
| Tumor size | 3.66 (2.00) | 3.68 (2.05) | 3.62 (1.91) | 0.76 |
| Model | AUROC (95% CI) | Accuracy (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | Precision (95% CI) | F1 (95% CI) |
|---|---|---|---|---|---|---|
| GBM | 0.916 [0.879–0.952] | 0.833 [0.781–0.884] | 0.772 [0.680–0.865] | 0.871 [0.812–0.930] | 0.792 [0.703–0.882] | 0.782 [0.691–0.873] |
| Logistic | 0.884 [0.839–0.931] | 0.803 [0.748–0.858] | 0.861 [0.784–0.937] | 0.766 [0.692–0.841] | 0.701 [0.600–0.802] | 0.773 [0.680–0.865] |
| SVM | 0.882 [0.836–0.928] | 0.808 [0.754–0.862] | 0.823 [0.739–0.907] | 0.798 [0.728–0.869] | 0.722 [0.623–0.821] | 0.769 [0.676–0.862] |
| Neural Network | 0.883 [0.837–0.928] | 0.793 [0.737–0.849] | 0.797 [0.709–0.886] | 0.79 [0.719–0.862] | 0.708 [0.608–0.808] | 0.75 [0.655–0.845] |
| KNN | 0.864 [0.812–0.916] | 0.803 [0.748–0.858] | 0.899 [0.832–0.965] | 0.742 [0.665–0.819] | 0.689 [0.587–0.791] | 0.78 [0.689–0.872] |
| AdaBoost | 0.701 [0.632–0.769] | 0.7 [0.636–0.763] | 0.684 [0.581–0.786] | 0.71 [0.630–0.790] | 0.6 [0.492–0.708] | 0.639 [0.533–0.745] |
| CatBoost | 0.882 [0.836–0.927] | 0.813 [0.759–0.866] | 0.734 [0.637–0.832] | 0.863 [0.802–0.923] | 0.773 [0.681–0.866] | 0.753 [0.658–0.848] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H.; Shen, D.; Gan, X.; Sun, D. An Interpretable Machine Learning Model Based on Inflammatory–Nutritional Biomarkers for Predicting Metachronous Liver Metastases After Colorectal Cancer Surgery. Biomedicines 2025, 13, 1706. https://doi.org/10.3390/biomedicines13071706
Zhu H, Shen D, Gan X, Sun D. An Interpretable Machine Learning Model Based on Inflammatory–Nutritional Biomarkers for Predicting Metachronous Liver Metastases After Colorectal Cancer Surgery. Biomedicines. 2025; 13(7):1706. https://doi.org/10.3390/biomedicines13071706
Chicago/Turabian StyleZhu, Hao, Danyang Shen, Xiaojie Gan, and Ding Sun. 2025. "An Interpretable Machine Learning Model Based on Inflammatory–Nutritional Biomarkers for Predicting Metachronous Liver Metastases After Colorectal Cancer Surgery" Biomedicines 13, no. 7: 1706. https://doi.org/10.3390/biomedicines13071706
APA StyleZhu, H., Shen, D., Gan, X., & Sun, D. (2025). An Interpretable Machine Learning Model Based on Inflammatory–Nutritional Biomarkers for Predicting Metachronous Liver Metastases After Colorectal Cancer Surgery. Biomedicines, 13(7), 1706. https://doi.org/10.3390/biomedicines13071706