

Efficacy and Safety of OROSOL Spray for Oral Mucositis in Children: A Randomized, Double-Blind, Placebo-Controlled Trial

Abstract
1. Introduction
2. Methods
2.1. Study Design and Ethics
2.2. Study Population
2.3. Interventions and Randomization
2.4. Investigational Device
2.5. Study Procedures and Assessments
2.6. Blinding and Unblinding
2.7. Statistical Analysis
3. Results
3.1. Demographic Outcomes
3.2. Primary Endpoint
Symptom Scores
- a
- Mucositis Severity Score
- b
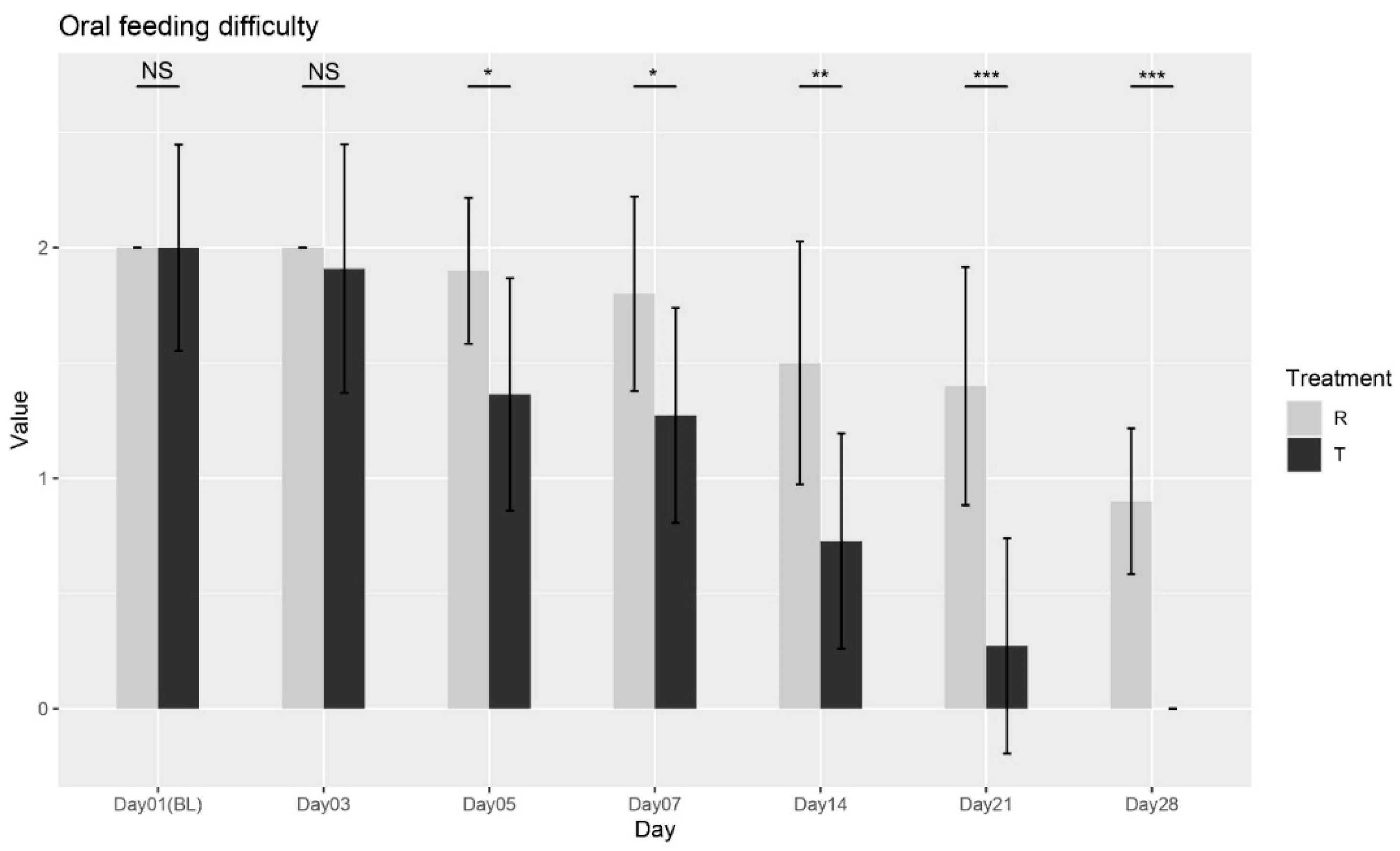
- Oral Feeding Difficulty
- c
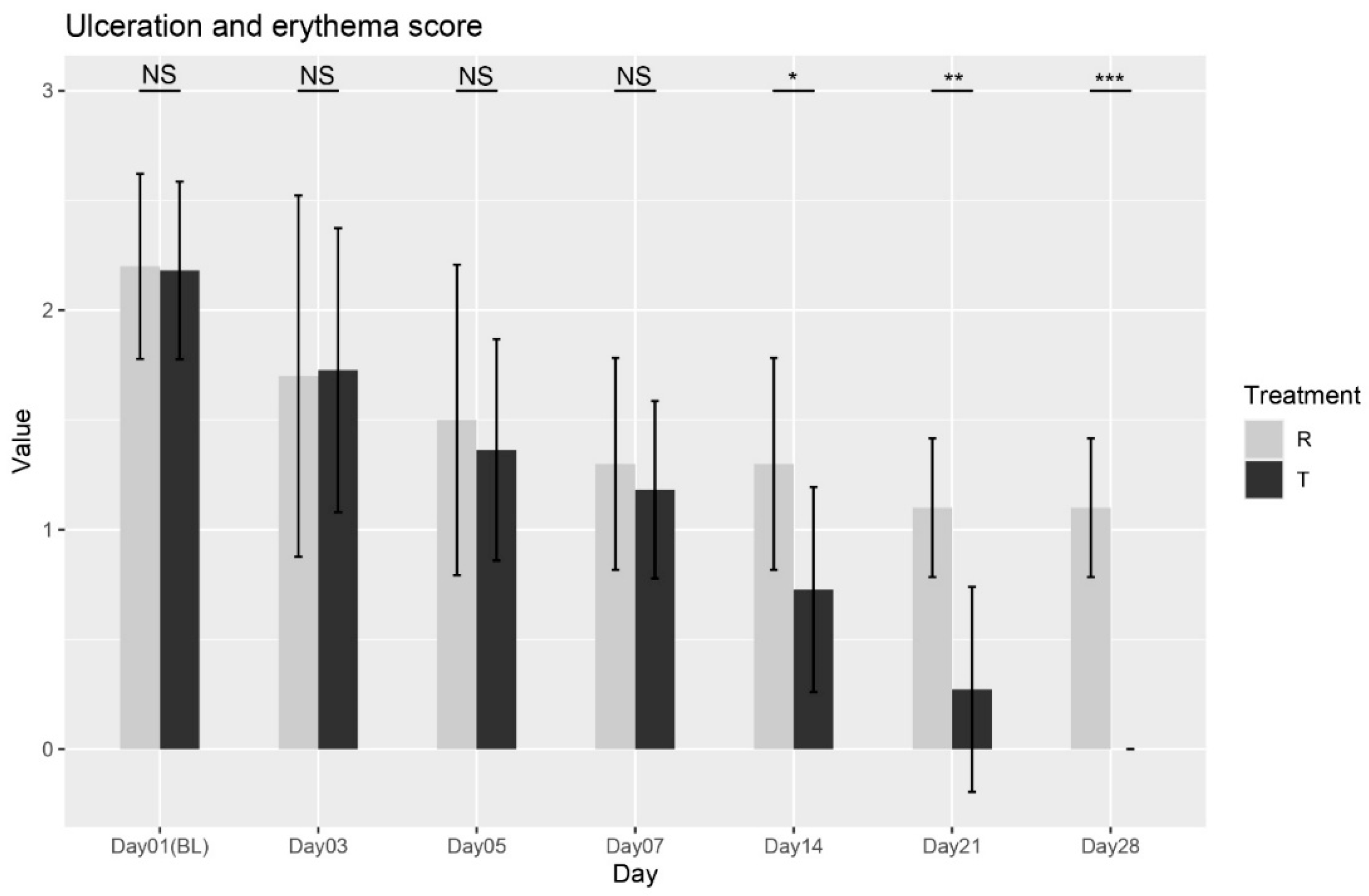
- Ulceration and Erythema Score
- d
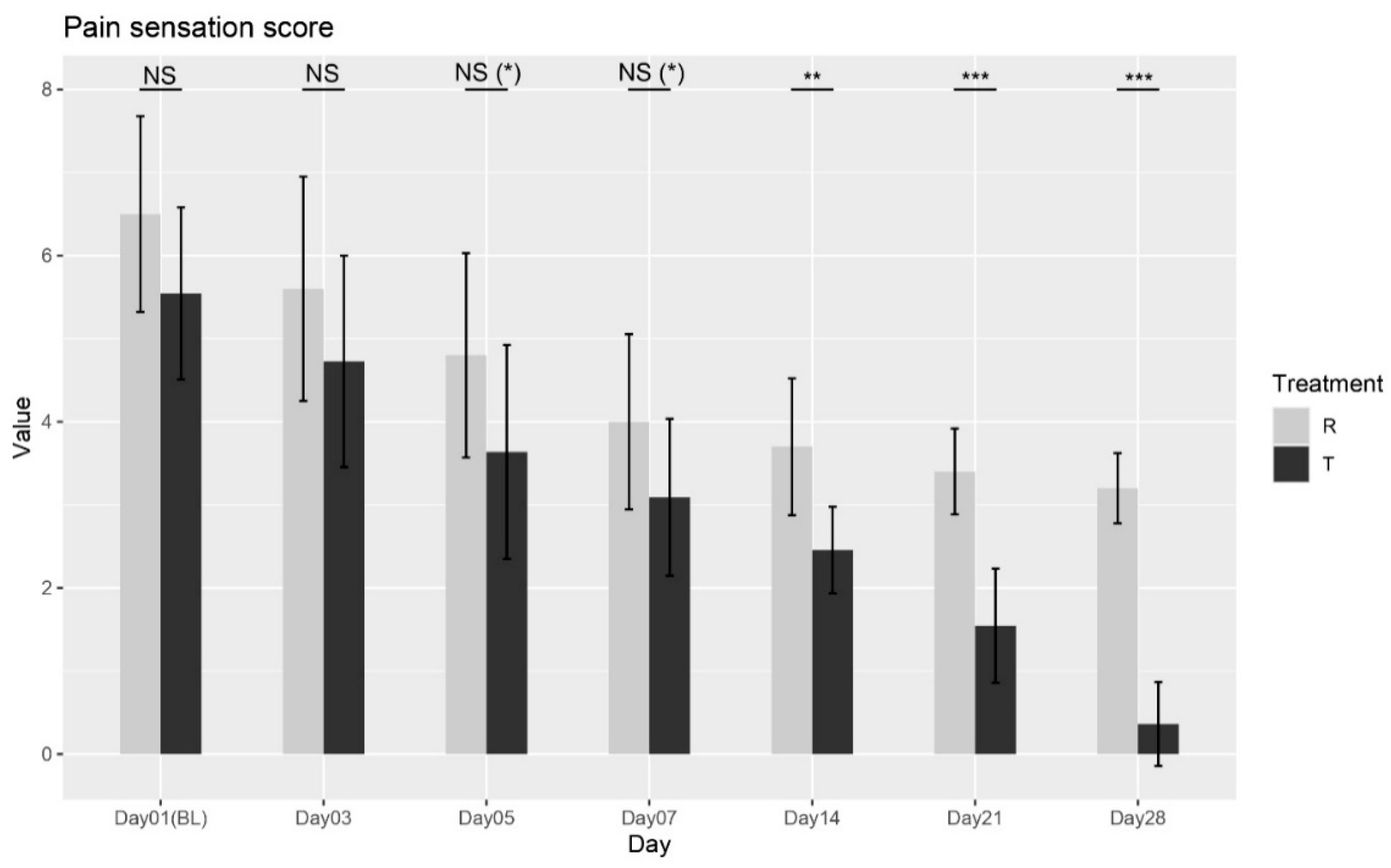
- Pain Sensation Score
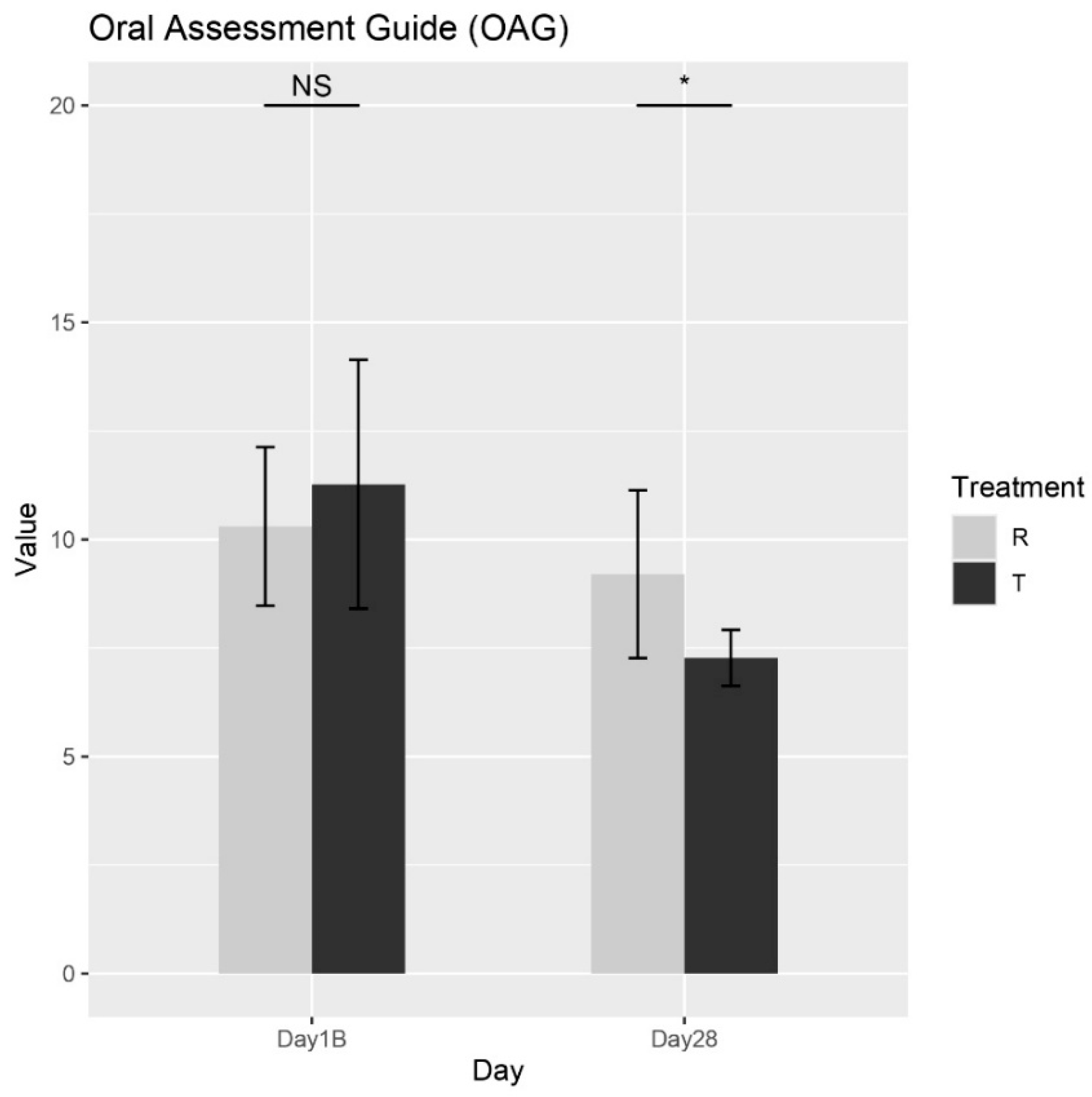
3.3. Secondary Endpoint
Oral Assessment Guide (OAG)
3.4. Safety and Tolerability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sonis, S.T. The pathobiology of mucositis. Nat. Rev. Cancer 2004, 4, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Elting, L.S.; Cooksley, C.D.; Chambers, M.S.; Garden, A.S. Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Sonis, S.T. Mucositis: The impact, biology and therapeutic opportunities of oral mucositis. Oral Oncol. 2009, 45, 1015–1020. [Google Scholar] [PubMed]
- Singh, V.; Singh, A.K. Oral mucositis. Natl. J. Maxillofac. Surg. 2020, 11, 159–168. [Google Scholar] [PubMed]
- Villa, A.; Sonis, S.T. Pharmacotherapy for the management of cancer regimen-related oral mucositis. Expert Opin. Pharmacother. 2016, 17, 1801–1807. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Sonis, S.T. Mucositis: Pathobiology and management. Curr. Opin. Oncol. 2015, 27, 159. [Google Scholar] [CrossRef] [PubMed]
- Lalla, R.V.; Sonis, S.T.; Peterson, D.E. Management of Oral Mucositis in Patients with Cancer. Dent. Clin. N. Am. 2008, 52, 61-viii. [Google Scholar] [CrossRef] [PubMed]
- Lalla, R.V.; Bowen, J.; Barasch, A.; Elting, L.; Epstein, J.; Keefe, D.M.; McGuire, D.B.; Migliorati, C.; Nicolatou-Galitis, O.; Peterson, D.E.; et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2014, 120, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Riley, P.; Glenny, A.M.; Worthington, H.V.; Littlewood, A.; Clarkson, J.E.; McCabe, M.G. Interventions for preventing oral mucositis in patients with cancer receiving treatment: Oral cryotherapy. Cochrane Database Syst. Rev. 2015, CD011552. [Google Scholar] [CrossRef]
- Peterson, D.E.; Bensadoun, R.J.; Roila, F. Management of oral and gastrointestinal mucositis: ESMO Clinical Practice Guidelines. Ann. Oncol. 2011, 22, vi78–vi84. [Google Scholar] [PubMed]
- Worthington, H.V.; Clarkson, J.E.; Bryan, G.; Furness, S.; Glenny, A.M.; Littlewood, A.; McCabe, M.G.; Meyer, S.; Khalid, T.; Riley, P. Interventions for preventing oral mucositis for patients with cancer receiving treatment. Cochrane Database Syst. Rev. 2011, CD000978. [Google Scholar] [CrossRef]
- Svanberg, A.; Öhrn, K.; Birgegård, G. Oral cryotherapy reduces mucositis and improves nutrition—A randomised controlled trial. J. Clin. Nurs. 2010, 19, 2146–2151. [Google Scholar] [CrossRef] [PubMed]
- Oton-Leite, A.F.; Silva, G.B.L.; Morais, M.O.; Silva, T.A.; Leles, C.R.; Valadares, M.C.; Pinezi, J.C.D.; Batista, A.C.; Mendonça, E.F. Effect of low-level laser therapy on chemoradiotherapy-induced oral mucositis and salivary inflammatory mediators in head and neck cancer patients. Lasers Surg. Med. 2015, 47, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Zadik, Y.; Arany, P.R.; Fregnani, E.R.; Bossi, P.; Antunes, H.S.; Bensadoun, R.J.; Gueiros, L.A.; Majorana, A.; Nair, R.G.; Ranna, V.; et al. Systematic review of photobiomodulation for the management of oral mucositis in cancer patients and clinical practice guidelines. Support. Care Cancer 2019, 27, 3969–3983. [Google Scholar] [CrossRef] [PubMed]
- McGuire, D.B.; Correa, M.E.P.; Johnson, J.; Wienandts, P. The role of basic oral care and good clinical practice principles in the management of oral mucositis. Support. Care Cancer 2006, 14, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, R.; Shrivastava, L.; Shrivastava, R. Composition for Topical Application Comprising Glycerol and Tannins. U.S. Patent US9597298B2, 21 March 2017. Available online: https://patents.google.com/patent/US9597298B2/en (accessed on 16 April 2025).
- Spielberger, R.; Stiff, P.; Bensinger, W.; Gentile, T.; Weisdorf, D.; Kewalramani, T.; Shea, T.; Yanovich, S.; Hansen, K.; Noga, S.; et al. Palifermin for Oral Mucositis after Intensive Therapy for Hematologic Cancers. N. Engl. J. Med. 2004, 351, 2590–2598. [Google Scholar] [CrossRef] [PubMed]
- Antunes, H.S.; Herchenhorn, D.; Small, I.A.; Araújo, C.M.; Viégas, C.M.P.; Cabral, E.; Rampini, M.P.; Rodrigues, P.C.; Silva, T.G.; Ferreira, E.M.; et al. Phase III trial of low-level laser therapy to prevent oral mucositis in head and neck cancer patients treated with concurrent chemoradiation. Radiother. Oncol. 2013, 109, 297–302. [Google Scholar] [PubMed]
- El Barche, F.Z.; D’almeida, M.; Dameron, S.; Shrivastava, R. Clinical Evaluation of NESOSPRAY HE-C, a Nasal Spray, for Rhinopharyngitis and Rhinosinusitis: A Randomized, Double-Blind, Placebo-Controlled Trial. Medicina 2025, 61, 1071. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | Group-R | Group-T | p-Value |
|---|---|---|---|---|
| Number of patients | 21 | 10 | 11 | X |
| Male (M) | M = 7 (33%) | M = 4 (19%) | M = 3 (14%) | 0.88 |
| Female (F) | F = 14 (67%) | F = 6 (29%) | F = 8 (38%) | 0.88 |
| Age (mean ± SD, [min, max]) | 9 ± 4 [3,16] | 9.9 ± 4.5 [3,16] | 8.2 ± 3.6 [3,14] | 0.35 |
| Height (mean ± SD, [min, max]) | 132.7 ± 22.3 [92,171] | 137.8 ± 23.8 [95,171] | 128.1 ± 21 [92,155] | 0.34 |
| Weight (mean ± SD, [min, max]) | 32.7 ± 14.1 [12.5,63.4] | 36.3 ± 16.3 [14.7,63.4] | 29.4 ± 11.7 [12.5,48.6] | 0.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Barche, F.-Z.; D’Almeida, M.; Dameron, S.; Shrivastava, R. Efficacy and Safety of OROSOL Spray for Oral Mucositis in Children: A Randomized, Double-Blind, Placebo-Controlled Trial. Biomedicines 2025, 13, 1677. https://doi.org/10.3390/biomedicines13071677
El Barche F-Z, D’Almeida M, Dameron S, Shrivastava R. Efficacy and Safety of OROSOL Spray for Oral Mucositis in Children: A Randomized, Double-Blind, Placebo-Controlled Trial. Biomedicines. 2025; 13(7):1677. https://doi.org/10.3390/biomedicines13071677
Chicago/Turabian StyleEl Barche, Fatima-Zahra, Manon D’Almeida, Séverine Dameron, and Rémi Shrivastava. 2025. "Efficacy and Safety of OROSOL Spray for Oral Mucositis in Children: A Randomized, Double-Blind, Placebo-Controlled Trial" Biomedicines 13, no. 7: 1677. https://doi.org/10.3390/biomedicines13071677
APA StyleEl Barche, F.-Z., D’Almeida, M., Dameron, S., & Shrivastava, R. (2025). Efficacy and Safety of OROSOL Spray for Oral Mucositis in Children: A Randomized, Double-Blind, Placebo-Controlled Trial. Biomedicines, 13(7), 1677. https://doi.org/10.3390/biomedicines13071677