

Systemic Ozone Therapy Improves Oral Hard and Soft Tissue Healing in Medication-Related Osteonecrosis of the Jaw (MRONJ): A Study in Senescent Female Rats

 , ,
, ,  ,
,  ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Computed Microtomography (MicroCT)
2.3. Analysis and Processing of the Soft Tissues
2.4. Microscopic Analysis and Microscopic Area of Interest (AMI)
2.5. Histopathological and Histometric Analysis
2.6. Immunohistochemical Analysis
2.7. Statistical Analysis
3. Results
3.1. Analysis of the Volumetric Parameters (MicroCT)
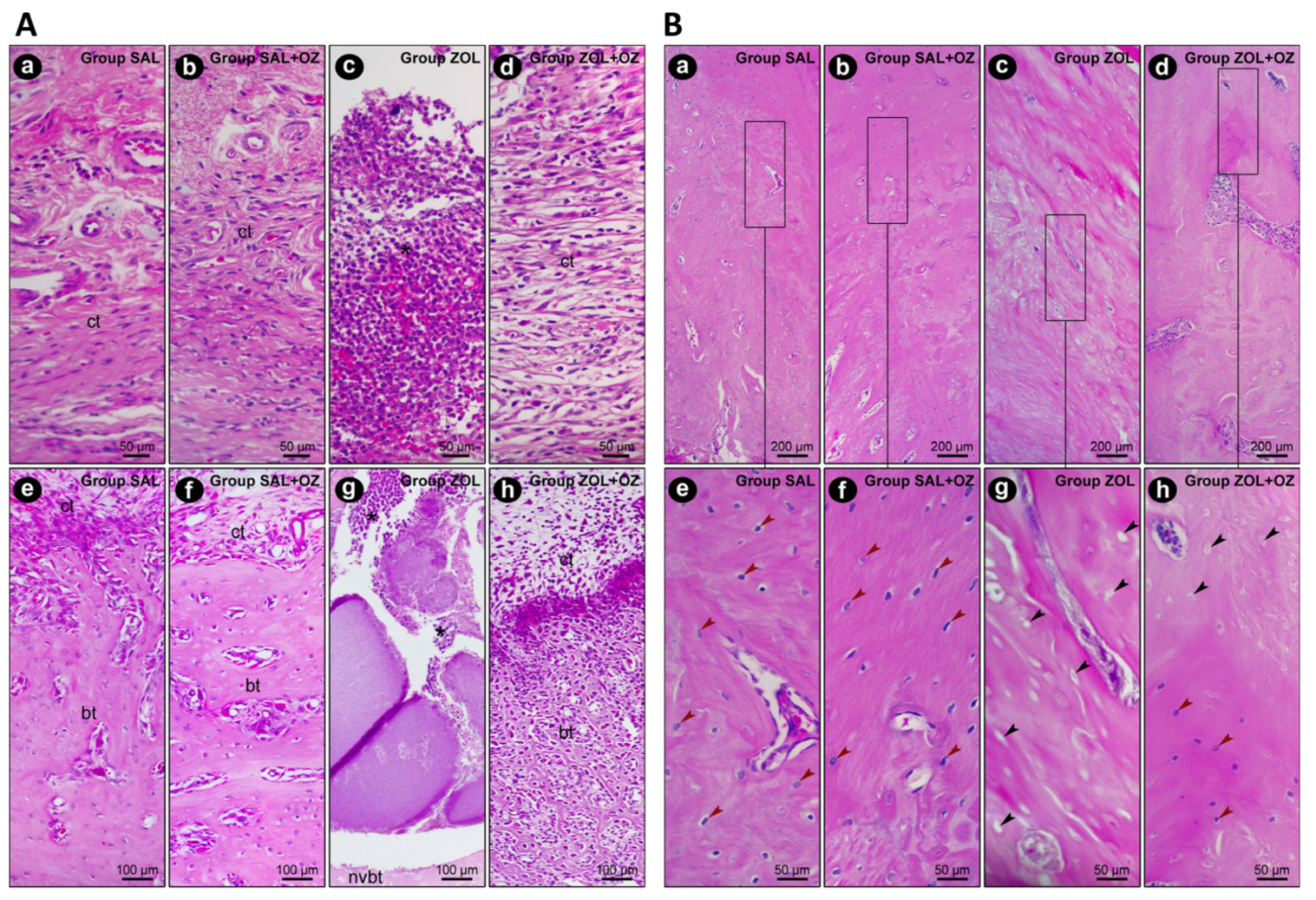
3.2. Histopathological and Histological Analysis
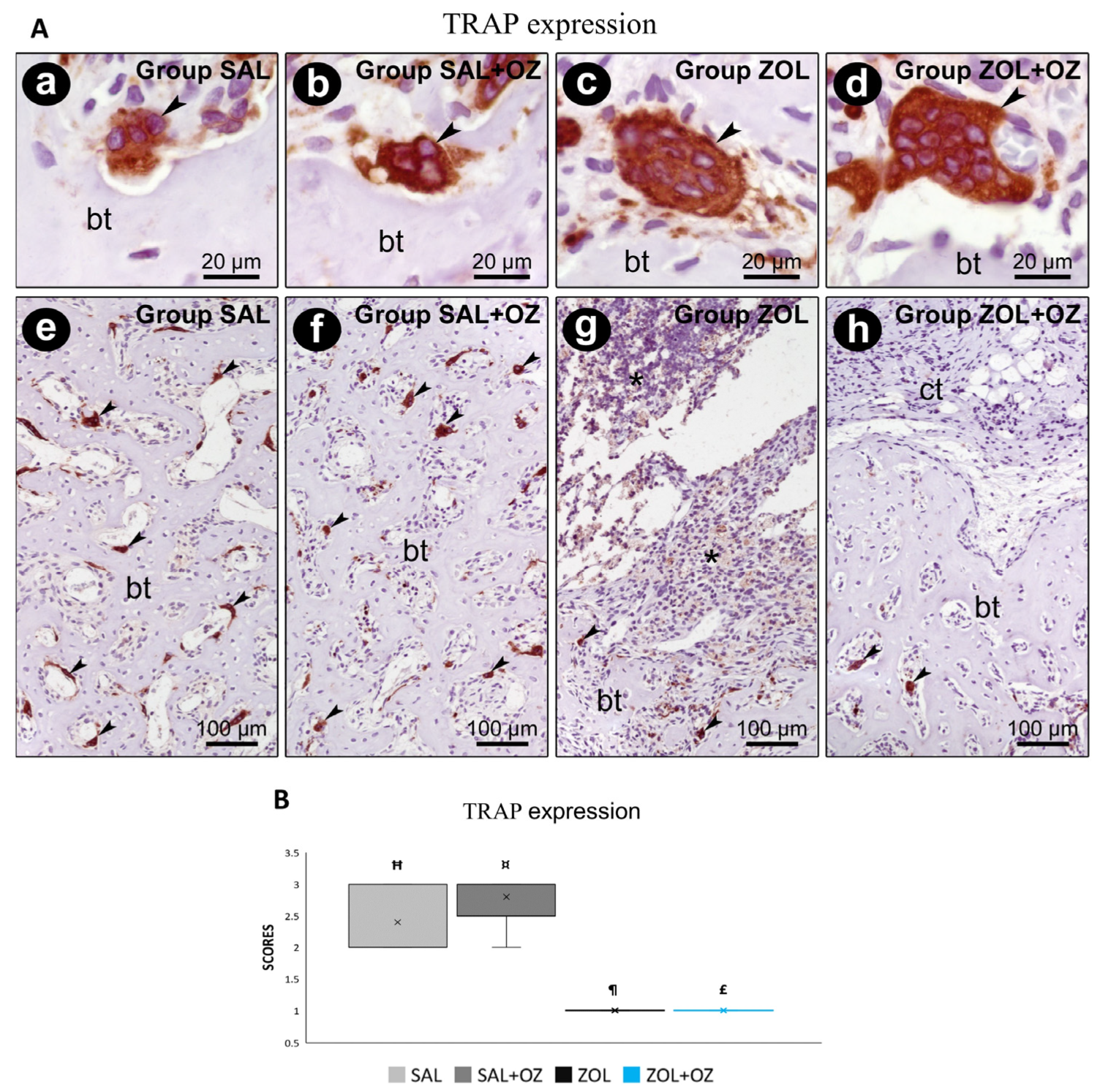
3.3. Immunohistochemistry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- McGowan, K.; McGowan, T.; Ivanovski, S. Risk Factors for Medication-Related Osteonecrosis of the Jaws: A Systematic Review. Oral Dis. 2018, 24, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Pautke, C.; Van den Wyngaert, T.; Niepel, D.; Schiødt, M. Bisphosphonate-Related Osteonecrosis of the Jaws—Characteristics, Risk Factors, Clinical Features, Localization and Impact on Oncological Treatment. J. Cranio-Maxillofac. Surg. 2012, 40, 303–309. [Google Scholar] [CrossRef]
- Marx, R.E. Pamidronate (Aredia) and Zoledronate (Zometa) Induced Avascular Necrosis of the Jaws: A Growing Epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Ripamonti, C.I.; Cislaghi, E.; Mariani, L.; Maniezzo, M. Efficacy and Safety of Medical Ozone (O3) Delivered in Oil Suspension Applications for the Treatment of Osteonecrosis of the Jaw in Patients with Bone Metastases Treated with Bisphosphonates: Preliminary Results of a Phase I-II Study. Oral Oncol. 2011, 47, 185–190. [Google Scholar] [CrossRef]
- Ozdemir, H.; Toker, H.; Balcı, H.; Ozer, H. Effect of Ozone Therapy on Autogenous Bone Graft Healing in Calvarial Defects: A Histologic and Histometric Study in Rats. J. Periodontal Res. 2013, 48, 722–726. [Google Scholar] [CrossRef]
- Toker, H.; Özdemir, H.; Kuzu, T.E.; Özer, H. The Effects of Allograft Combined with Ozone Therapy on Regeneration of Calvarial Defects in Rats. Cumhur. Dent. J. 2017, 20, 205–213. [Google Scholar] [CrossRef]
- Gonenci, R.; Tabur, M.; Ozsoy, S.Y. Preventive and Curative Effects of Medical Ozone in Rats Exposed to Experimental Osteomyelitis. Pak. Vet. J. 2017, 37, 355–359. [Google Scholar]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Statkievicz, C.; Toro, L.F.; Marcantonio, C.C.; Ervolino, E.; Garcia, V.G.; Marcantonio, E. Photomodulation Multiple Sessions as a Promising Preventive Therapy for Medication-Related Osteonecrosis of the Jaws after Tooth Extraction in Rats. J. Photochem. Photobiol. B Biol. 2018, 184, 7–19. [Google Scholar] [CrossRef]
- Ervolino, E.; Statkievicz, C.; Toro, L.F.; de Mello-Neto, J.M.; Cavazana, T.P.; Issa, J.P.M.; Dornelles, R.C.M.; de Almeida, J.M.; Garcia, V.G.; Marcantonio, E. Antimicrobial Photodynamic Therapy Improves the Alveolar Repair Process and Prevents the Occurrence of Osteonecrosis of the Jaws after Tooth Extraction in Senile Rats Treated with Zoledronate. Bone 2019, 120, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Alshaikh, A.; Kim, T.; Kim, S.; Dunlap, M.; Schricker, S.; Kim, R.H.; Kang, M.K.; Park, N.H.; Shin, K.H. Preexisting Periapical Inflammatory Condition Exacerbates Tooth Extraction-Induced Bisphosphonate-Related Osteonecrosis of the Jaw Lesions in Mice. J. Endod. 2016, 42, 1641–1646. [Google Scholar] [CrossRef] [PubMed]
- Garcia, V.G.; Longo, M.; Gualberto Júnior, E.C.; Bosco, A.F.; Nagata, M.J.H.; Ervolino, E.; Theodoro, L.H. Effect of the Concentration of Phenothiazine Photosensitizers in Antimicrobial Photodynamic Therapy on Bone Loss and the Immune Inflammatory Response of Induced Periodontitis in Rats. J. Periodontal Res. 2014, 49, 584–594. [Google Scholar] [CrossRef]
- Thumbigere-Math, V.; Michalowicz, B.S.; Hughes, P.J.; Basi, D.L.; Tsai, M.L.; Swenson, K.K.; Rockwell, L.; Gopalakrishnan, R. Periodontal Disease as a Risk Factor for Bisphosphonate-Related Osteonecrosis of the Jaw. J. Periodontol. 2014, 85, 226–233. [Google Scholar] [CrossRef]
- MacKay, J.W.; Murray, I.R.; Kasmai, B.; Dias, J.; McAlinden, M.G.; Goodall, J.; Drost, E.; Graves, M.J.; Gregson, R.; Toms, A.P. Subchondral Bone in Osteoarthritis: Association between MRI Texture Analysis and Histomorphometry. Osteoarthr. Cartil. 2017, 25, 700–707. [Google Scholar] [CrossRef]
- Endo, Y.; Kumamoto, H.; Nakamura, M.; Funayama, S.; Suzuki, T.; Hattori, T.; Miyamoto, I.; Takahashi, T.; Ueda, M.; Aoki, T. Mechanisms and Therapeutic Strategies for Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ). Biol. Pharm. Bull. 2017, 40, 739–750. [Google Scholar] [CrossRef]
- Diab, D.L.; Watts, N.B. Bisphosphonate Drug Holiday: Who, When and How Long. Ther. Adv. Musculoskelet. Dis. 2013, 5, 107–111. [Google Scholar] [CrossRef]
- Martelli, S.J.R.; Santos, P.L.; Santos, R.A.; Nogueira, R.D.; Domingues, R.R.; Fontes, K.B.F.C.; Rocha, A.L.; Arantes-Rodrigues, R.; Santos, R.P.; Santos, F.R. Comparison of Effects of Zoledronic Acid and Clodronate on the Bone Structure: Imaginological and Histomorphometrical Study In Vivo. J. Oral Pathol. Med. 2017, 46, 632–636. [Google Scholar] [CrossRef]
- Syed, F.A.; Ng, A.C. The Pathophysiology of the Aging Skeleton. Curr. Osteoporos. Rep. 2010, 8, 235–240. [Google Scholar] [CrossRef]
- Kim, J.W.; Cha, I.H.; Kim, S.J.; Kim, M.R. Biomarkers for Bisphosphonate-Related Osteonecrosis of the Jaw. Clin. Implant Dent. Relat. Res. 2016, 18, 281–291. [Google Scholar] [CrossRef]
- Huang, X.; Xu, X.; Zhang, Q.; Liu, Q.; Zhang, Y.; Li, J. A Dose-Dependent Inhibitory Effects of Zoledronic Acid on Osteoblast Viability and Function In Vitro. Mol. Med. Rep. 2016, 13, 613–622. [Google Scholar] [CrossRef]
- Kimmel, D.B. Mechanism of Action, Pharmacokinetic and Pharmacodynamic Profile, and Clinical Applications of Nitrogen-Containing Bisphosphonates. J. Dent. Res. 2007, 86, 1022–1033. [Google Scholar] [CrossRef]
- Erdemci, F.; Gunaydin, Y.; Ozkan, M.; Sener, I.; Tuncer, I.; Erturk, M. Histomorphometric Evaluation of the Effect of Systemic and Topical Ozone on Alveolar Bone Healing Following Tooth Extraction in Rats. Int. J. Oral Maxillofac. Surg. 2014, 43, 777–783. [Google Scholar] [CrossRef]
- Rosales, H.D.; Garcia Guevara, H.; Requejo, S.; Jensen, M.D.; Acero, J.; Olate, S. Medication-Related Osteonecrosis of the Jaws (MRONJ) in Children and Young Patients—A Systematic Review. J. Clin. Med. 2023, 12, 1416. [Google Scholar] [CrossRef]
- Pereira-Silva, M.; Hadad, H.; de Jesus, L.K.; de Almeida, J.F.A.; Ninima, H.H.; Okamoto, R. Ozone Therapy Effect in Medication-Related Osteonecrosis of the Jaw as Prevention or Treatment: Microtomographic, Confocal Laser Microscopy and Histomorphometric Analysis. Clin. Oral Investig. 2024, 28, 151. [Google Scholar] [CrossRef]
- Ripamonti, C.I.; Maniezzo, M.; Cislaghi, E.; Campa, T.; Fagnoni, M.; Mariani, L. Efficacy and Tolerability of Medical Ozone Gas Insufflations in Patients with Osteonecrosis of the Jaw Treated with Bisphosphonates—Preliminary Data: Medical Ozone Gas Insufflation in Treating ONJ Lesions. J. Bone Oncol. 2012, 1, 81–87. [Google Scholar] [CrossRef]
- da Silva, W.P.P.; Delanora, L.A.; Rios, B.R.; Barbosa, S.; Simon, M.E.S.; Sukotjo, C.; Faverani, L.P. Feasible Low Bone Density Condition for Assessing Bioactivity in Ex-In Vivo and In Vivo Studies. J. Appl. Oral Sci. 2023, 31, e20220411. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histological Analysis | ||||
|---|---|---|---|---|
| Parameters and Respective Scores | Percentage of Specimens | |||
| Experimental Groups | ||||
| SAL | SAL+OZ | ZOL | ZOL+OZ | |
| Intensity of local inflammatory response | ||||
| (1) absence of inflammation (presence of few inflammatory cells) | 100% | 100% | - | 60% |
| (2) mild quantity of inflammatory cells (less than 1/3 of cells are inflammatory cells) | - | - | - | 40% |
| (3) moderate quantity of inflammatory cells (1/3–2/3 of cells are inflammatory cells) | - | - | 40% | - |
| (4) severe quantity of inflammatory cells (more than 1/3 of cells are inflammatory cells) | - | - | 60% | - |
| median | 1 | 1 | 4*a,b | 1*c |
| Inflammation extension | ||||
| (1) absence of inflammation | 100% | 100% | - | 60% |
| (2) partial extension of connective tissue | - | - | - | 40% |
| (3) entire extension of connective tissue, without reaching bone tissue | - | - | 20% | - |
| (4) entire extension of connective tissue and bone tissue | - | - | 80% | - |
| median | 1 | 1 | 4*a,b | 1*c |
| Cellular pattern and epithelial tissue structure | ||||
| (1) epithelial tissue with moderate thickness (larger than half the surgical wound epithelium border thickness) and completely recovering extraction site | 60% | 80% | - | 20% |
| (2) epithelial tissue with thin thickness (smaller than half the surgical wound epithelium border thickness) and completely recovering extraction site | 40% | 20% | - | 80% |
| (3) thin layer of epithelial tissue (smaller than half the surgical wound epithelium border thickness) and only in edges of open surgical wound | - | - | 20% | - |
| (4) absence of epithelial tissue on open surgical wound | - | - | 80% | - |
| median | 1 | 1 | 4*a,b | 2*c |
| Cellular pattern and connective tissue structure | ||||
| (1) moderate quantity of fibroblasts and large quantity of collagen fibers (approximately 2/3 of area occupied by fibroblast/collagen fibers, where collagen fibers are prevalent over fibroblasts) | 60% | 80% | - | 20% |
| (2) moderate quantity of both fibroblasts and collagen fibers (approximately 2/3 of area occupied by fibroblast/collagen fibers, where collagen fibers and fibroblasts are equivalent) | 40% | 20% | - | 80% |
| (3) small quantity of both fibroblasts and collagen fibers (approximately 1/3 of area occupied by fibroblast/collagen fibers, where collagen fibers and fibroblasts are equivalent) | - | - | 40% | - |
| (4) severe tissue disorganization with necrosis areas (approximately 2/3 of area occupied by disorganized connective tissue) | - | - | 60% | - |
| median | 1 | 1 | 4*a,b | 2*c |
| Cellular pattern and bone tissue structure | ||||
| (1) absence of non-vital bone in adjacencies of extraction site and trabecular bone filling more than half of dental alveolus | 80% | 100% | - | - |
| (2) absence of non-vital bone in adjacencies of extraction site and trabecular bone filling less than half of dental alveolus | 20% | - | - | 60% |
| (3) presence of few areas with non-vital bone in adjacencies of extraction site and trabecular bone filling less than a third of dental alveolus | - | - | 20% | 40% |
| (4) presence of many areas with non-vital bone in adjacencies of extraction site and trabecular bone filling less than a third of dental alveolus | - | - | 80% | - |
| median | 1 | 1 | 4*a,b | 2*a,b,c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delanora, L.A.; de Lima Neto, T.J.; da Rocha, T.E.; Silveira, G.R.C.; Levin, L.; Shibli, J.A.; Ervolino, E.; Mourão, C.F.; Faverani, L.P. Systemic Ozone Therapy Improves Oral Hard and Soft Tissue Healing in Medication-Related Osteonecrosis of the Jaw (MRONJ): A Study in Senescent Female Rats. Biomedicines 2025, 13, 1248. https://doi.org/10.3390/biomedicines13051248
Delanora LA, de Lima Neto TJ, da Rocha TE, Silveira GRC, Levin L, Shibli JA, Ervolino E, Mourão CF, Faverani LP. Systemic Ozone Therapy Improves Oral Hard and Soft Tissue Healing in Medication-Related Osteonecrosis of the Jaw (MRONJ): A Study in Senescent Female Rats. Biomedicines. 2025; 13(5):1248. https://doi.org/10.3390/biomedicines13051248
Chicago/Turabian StyleDelanora, Leonardo Alan, Tiburtino José de Lima Neto, Tiago Esgalha da Rocha, Glauco Rodrigues Carmo Silveira, Liran Levin, Jamil Awad Shibli, Edilson Ervolino, Carlos Fernando Mourão, and Leonardo P. Faverani. 2025. "Systemic Ozone Therapy Improves Oral Hard and Soft Tissue Healing in Medication-Related Osteonecrosis of the Jaw (MRONJ): A Study in Senescent Female Rats" Biomedicines 13, no. 5: 1248. https://doi.org/10.3390/biomedicines13051248
APA StyleDelanora, L. A., de Lima Neto, T. J., da Rocha, T. E., Silveira, G. R. C., Levin, L., Shibli, J. A., Ervolino, E., Mourão, C. F., & Faverani, L. P. (2025). Systemic Ozone Therapy Improves Oral Hard and Soft Tissue Healing in Medication-Related Osteonecrosis of the Jaw (MRONJ): A Study in Senescent Female Rats. Biomedicines, 13(5), 1248. https://doi.org/10.3390/biomedicines13051248