

Brain Structural Alterations Underlying Mood-Related Deficits in Schizophrenia



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. MRI Data Acquisition
2.3. Whole-Brain VBM Analysis
2.4. Regression Analysis Focused on VBM-GMV and Symptom Severity
3. Results
3.1. Demographics and Clinical Data
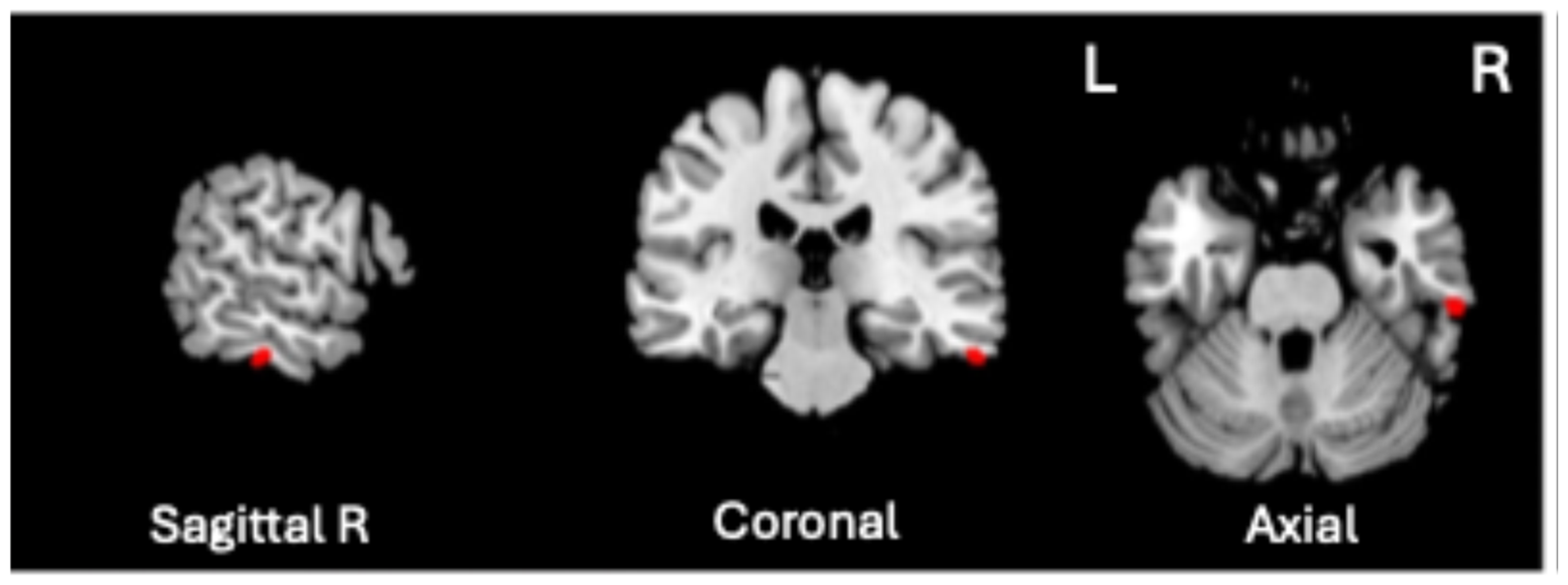
3.2. Whole-Brain VBM Analysis
3.3. Regression Analysis Focused on VBM-GMV and Symptom Severity
3.4. Post Hoc Analysis of PANSS Scores: Generalized Psychopathology (GP) Items
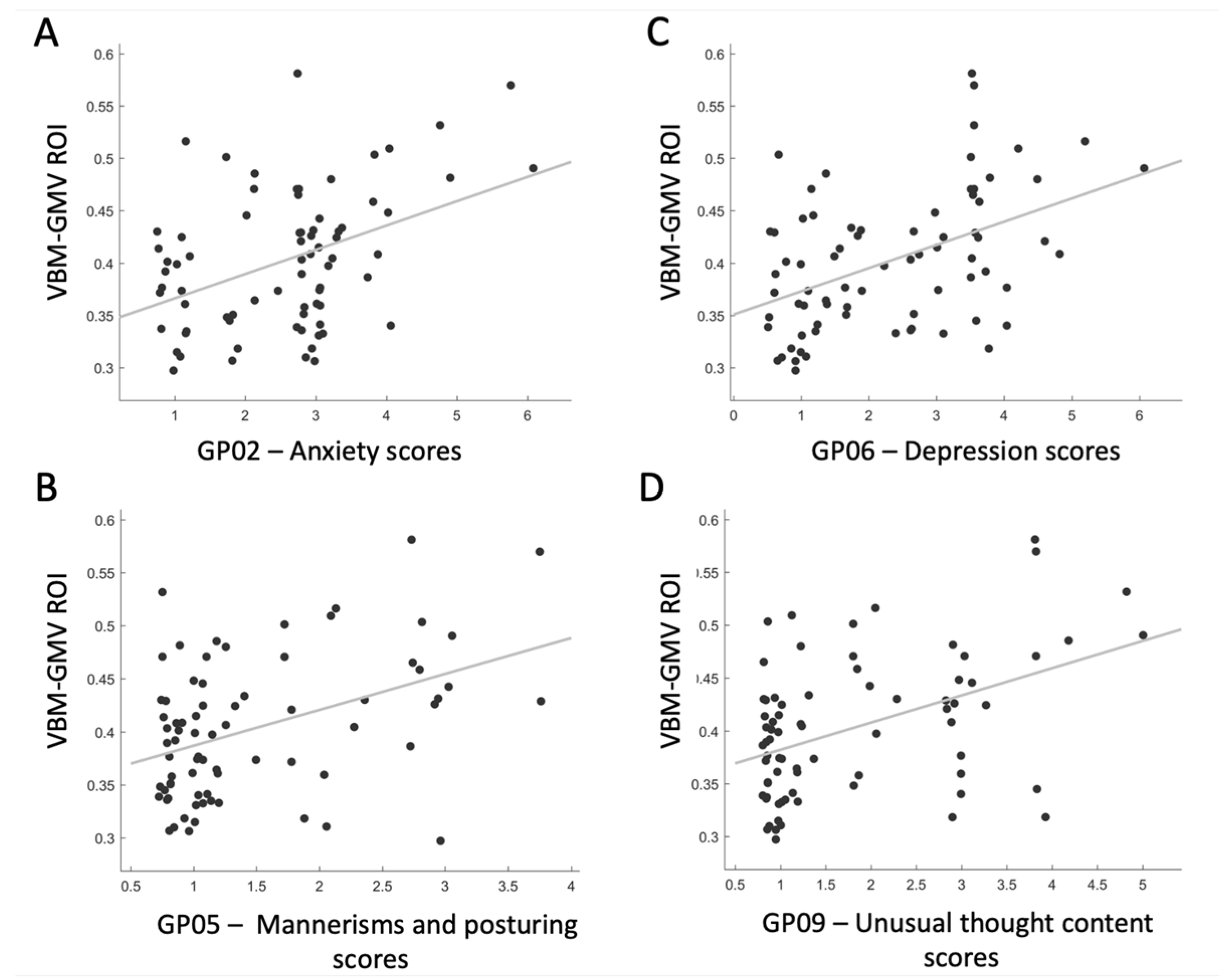
3.5. Post Hoc Analysis of ROI-GMV and Selected GP Items
4. Discussion
4.1. GMV Reductions in SZ Patients
4.2. Correlation Between GMV Alteration and Generalized Psychopathology Scores in SZ Patients
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization, “Schizophrenia”. Available online: https://www.who.int/news-room/fact-sheets/detail/schizophrenia (accessed on 16 July 2024).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013; p. 99. [Google Scholar]
- Tandon, R.; Nasrallah, H.; Akbarian, S.; Carpenter, W.T.; DeLisi, L.E.; Gaebel, W.; Green, M.F.; Gur, R.E.; Heckers, S.; Kane, J.M.; et al. The schizophrenia syndrome, circa 2024: What we know and how that informs its nature. Schizophr. Res. 2024, 264, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Marenco, S.; Weinberger, D.R. The neurodevelopmental hypothesis of schizophrenia: Following a trail of evidence from cradle to grave. Dev. Psychopathol. 2000, 12, 501–527. [Google Scholar] [CrossRef]
- Rapoport, J.L.; Giedd, J.N.; Gogtay, N. Neurodevelopmental model of schizophrenia: Update 2012. Mol. Psychiatry 2012, 17, 1228–1238. [Google Scholar] [CrossRef]
- Stone, W.S.; Phillips, M.R.; Yang, L.H.; Kegeles, L.S.; Susser, E.S.; Lieberman, J.A. Neurodegenerative model of schizophrenia: Growing evidence to support a revisit. Schizophr. Res. 2022, 243, 154–162. [Google Scholar] [CrossRef]
- Przedborski, S.; Vila, M.; Jackson-Lewis, V. Series Introduction: Neurodegeneration: What is it and where are we? J. Clin. Investig. 2003, 111, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Neri, I.; Ramírez-Bermúdez, J.; Montes, S.; Ríos, C. Possible mechanisms of neurodegeneration in schizophrenia. Neurochem. Res. 2006, 31, 1279–1294. [Google Scholar] [CrossRef]
- Iliuta, F.P.; Manea, M.C.; Budisteanu, M.; Ciobanu, A.M.; Manea, M. Magnetic resonance imaging in schizophrenia: Luxury or necessity? (Review). Exp Ther. Med. 2021, 22, 765. [Google Scholar] [CrossRef] [PubMed]
- Picó-Pérez, M.; Vieira, R.; Fernández-Rodríguez, M.; De Barros, M.A.P.; Radua, J.; Morgado, P. Multimodal meta-analysis of structural gray matter, neurocognitive and social cognitive fMRI findings in schizophrenia patients. Psychol. Med. 2022, 52, 614–624. [Google Scholar] [CrossRef]
- Howes, O.D.; Cummings, C.; Chapman, G.E.; Shatalina, E. Neuroimaging in schizophrenia: An overview of findings and their implications for synaptic changes. Neuropsychopharmacology 2023, 48, 151–167. [Google Scholar] [CrossRef]
- Olabi, B.; Ellison-Wright, I.; McIntosh, A.M.; Wood, S.J.; Bullmore, E.; Lawrie, S.M. Are there progressive brain changes in schizophrenia? A meta-analysis of structural magnetic resonance imaging studies. Biol. Psychiatry 2011, 70, 88–96. [Google Scholar] [CrossRef]
- Vita, A.; De Peri, L.; Deste, G.; Sacchetti, E. Progressive loss of cortical gray matter in schizophrenia: A meta-analysis and meta-regression of longitudinal MRI studies. Transl. Psychiatry 2012, 2, e190. [Google Scholar] [CrossRef]
- Dietsche, B.; Kircher, T.; Falkenberg, I. Structural brain changes in schizophrenia at different stages of the illness: A selective review of longitudinal magnetic resonance imaging studies. Aust. N. Z. J. Psychiatry 2017, 51, 500–508. [Google Scholar] [CrossRef]
- Andreasen, N.C.; Nopoulos, P.; Magnotta, V.; Pierson, R.; Ziebell, S.; Ho, B.C. Progressive brain change in schizophrenia: A prospective longitudinal study of first-episode schizophrenia. Biol. Psychiatry 2011, 70, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Ashe, P.C.; Berry, M.D.; Boulton, A.A. Schizophrenia, a neurodegenerative disorder with neurodevelopmental antecedents. Prog. Neuropsychopharmacol. Biol. Psychiatry 2001, 25, 691–707. [Google Scholar] [CrossRef]
- De Haan, L.; Bakker, J.M. Overview of neuropathological theories of schizophrenia: From degeneration to progressive developmental disorder. Psychopathology 2004, 37, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pino, O.; Guilera, G.; Gómez-Benito, J.; Najas-García, A.; Rufián, S.; Rojo, E. Neurodevelopment or neurodegeneration: Review of theories of schizophrenia. Actas. Esp. Psiquiatr. 2014, 42, 185–195. [Google Scholar]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry—The methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef]
- Fornito, A.; Yücel, M.; Patti, J.; Wood, S.J.; Pantelis, C. Mapping grey matter reductions in schizophrenia: An anatomical likelihood estimation analysis of voxel-based morphometry studies. Schizophr. Res. 2009, 108, 104–113. [Google Scholar] [CrossRef]
- Gupta, C.N.; Calhoun, V.D.; Rachakonda, S.; Chen, J.; Patel, V.; Liu, J.; Segall, J.; Franke, B.; Zwiers, M.P.; Arias-Vasquez, A.; et al. Patterns of gray matter abnormalities in schizophrenia based on an international mega-analysis. Schizophr. Bull. 2015, 41, 1133–1142. [Google Scholar] [CrossRef]
- Liloia, D.; Brasso, C.; Cauda, F.; Mancuso, L.; Nani, A.; Manuello, J.; Costa, T.; Duca, S.; Rocca, P. Updating and characterizing neuroanatomical markers in high-risk subjects, recently diagnosed and chronic patients with schizophrenia: A revised coordinate-based meta-analysis. Neurosci. Biobehav. Rev. 2021, 123, 83–103. [Google Scholar] [CrossRef]
- Glahn, D.C.; Laird, A.R.; Ellison-Wright, I.; Thelen, S.M.; Robinson, J.L.; Lancaster, J.L.; Bullmore, E.; Fox, P.T. Meta-analysis of gray matter anomalies in schizophrenia: Application of anatomic likelihood estimation and network analysis. Biol. Psychiatry 2008, 64, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.C.; Di, X.; McAlonan, G.M.; Gong, Q.Y. Brain anatomical abnormalities in high-risk individuals, first-episode, and chronic schizophrenia: An activation likelihood estimation meta-analysis of illness progression. Schizophr. Bull. 2011, 37, 177–188. [Google Scholar] [CrossRef]
- Bora, E.; Fornito, A.; Radua, J.; Walterfang, M.; Seal, M.; Wood, S.J.; Yücel, M.; Velakoulis, D.; Pantelis, C. Neuroanatomical abnormalities in schizophrenia: A multimodal voxelwise meta-analysis and meta-regression analysis. Schizophr. Res. 2011, 127, 46–57. [Google Scholar] [CrossRef]
- Bora, E.; Fornito, A.; Yücel, M.; Pantelis, C. The effects of gender on grey matter abnormalities in major psychoses: A comparative voxelwise meta-analysis of schizophrenia and bipolar disorder. Psychol. Med. 2012, 42, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Torres, U.S.; Portela-Oliveira, E.; Borgwardt, S.; Busatto, G.F. Structural brain changes associated with antipsychotic treatment in schizophrenia as revealed by voxel-based morphometric MRI: An activation likelihood estimation meta-analysis. BMC Psychiatry 2013, 13, 342. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Zhang, W.; Yao, L.; Xiao, Y.; Liu, L.; Liu, J.; Li, S.; Tao, B.; Shah, C.; Gong, Q.; et al. Association between structural and functional brain alterations in drug-free patients with schizophrenia: A multimodal meta-analysis. J. Psychiatry Neurosci. 2018, 43, 131–142. [Google Scholar] [CrossRef]
- Qi, Z.; Wang, J.; Gong, J.; Su, T.; Fu, S.; Huang, L.; Wang, Y. Common and specific patterns of functional and structural brain alterations in schizophrenia and bipolar disorder: A multimodal voxel-based meta-analysis. J. Psychiatry Neurosci. 2022, 47, E32–E47. [Google Scholar] [CrossRef]
- Wang, L.; Liu, R.; Liao, J.; Xiong, X.; Xia, L.; Wang, W.; Liu, J.; Zhao, F.; Zhuo, L.; Li, H. Meta-analysis of structural and functional brain abnormalities in early-onset schizophrenia. Front. Psychiatry 2024, 15, 1465758. [Google Scholar] [CrossRef]
- Zhu, J.; Zhuo, C.; Liu, F.; Xu, L.; Yu, C. Neural substrates underlying delusions in schizophrenia. Sci. Rep. 2016, 6, 33857. [Google Scholar] [CrossRef]
- Romeo, Z.; Spironelli, C. Hearing voices in the head: Two meta-analyses on structural correlates of auditory hallucinations in schizophrenia. NeuroImage. Clin. 2022, 36, 103241. [Google Scholar] [CrossRef]
- Rotarska-Jagiela, A.; van de Ven, V.; Oertel-Knöchel, V.; Uhlhaas, P.J.; Vogeley, K.; Linden, D.E. Resting-state functional network correlates of psychotic symptoms in schizophrenia. Schizophr. Res. 2010, 117, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Bora, E. Neurodevelopmental origin of cognitive impairment in schizophrenia. Psychol. Med. 2015, 45, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Melle, I. Cognition in schizophrenia: A marker of underlying neurodevelopmental problems? World Psychiatry 2019, 18, 164. [Google Scholar] [CrossRef]
- Mäkinen, J.; Miettunen, J.; Isohanni, M.; Koponen, H. Negative symptoms in schizophrenia—A review. Nord. J. Psychiatry 2008, 62, 334–341. [Google Scholar] [CrossRef]
- Zhao, M.; Ma, J.; Wu, Y.; Zhang, Y.; Wang, L.; Song, H.; Sun, X. Depressive and anxiety symptoms among schizophrenia patients. J. Affect. Disord. 2024, 362, 749–754. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T. regulation and schizophrenia. Int. J. Cogn. Ther. 2012, 5, 67–76. [Google Scholar] [CrossRef]
- ten Donkelaar, H.J.; Insausti, R.; van Domburg, P.; Küsters, B.; Hashizume, Y.; Hori, A. The limbic system. In Clinical Neuroanatomy: Brain Circuitry and Its Disorders; Springer: Cham, Switzerland, 2020; pp. 745–830. [Google Scholar]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Gibbon, M. The structured clinical interview for DSM-IV axis I disorders (SCID-I) and the structured clinical interview for DSM-IV axis II disorders (SCID-II). In Comprehensive Handbook of Psychological Assessment; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004; Volume 2, pp. 134–143. [Google Scholar]
- Ashburner, J.; Friston, K.J. Unified segmentation. NeuroImage 2005, 26, 839–851. [Google Scholar] [CrossRef]
- Gaser, C.; Dahnke, R.; Thompson, P.M.; Kurth, F.; Luders, E. The Alzheimer’s Disease Neuroimaging Initiative. CAT: A computational anatomy toolbox for the analysis of structural MRI data. GigaScience 2024, 13, giae049. [Google Scholar] [CrossRef]
- Adler, C.M.; Levine, A.D.; DelBello, M.P.; Strakowski, S.M. Changes in gray matter volume in patients with bipolar disorder. Biol. Psychiatry 2005, 58, 151–157. [Google Scholar] [CrossRef]
- Cano, M.; Lee, E.; Cardoner, N.; Martínez-Zalacaín, I.; Pujol, J.; Makris, N.; Henry, M.; Via, E.; Hernández-Ribas, R.; Contreras-Rodríguez, O. Brain Volumetric Correlates of Right Unilateral Versus Bitemporal Electroconvulsive Therapy for Treatment-Resistant Depression. J. Neuropsychiatry Clin. Neurosci. 2019, 31, 152–158. [Google Scholar] [CrossRef]
- Mubarik, A.; Tohid, H. Frontal lobe alterations in schizophrenia: A review. Trends Psychiatry Psychother. 2016, 38, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Zhou, Y.; Liu, B.; Liu, Y.; Song, M. Brainnetome-wide association studies in schizophrenia: The advances and future. Neurosci. Biobehav. Rev. 2013, 37, 2818–2835. [Google Scholar] [CrossRef] [PubMed]
- Smucny, J.; Dienel, S.J.; Lewis, D.A.; Carter, C.S. Mechanisms underlying dorsolateral prefrontal cortex contributions to cognitive dysfunction in schizophrenia. Neuropsychopharmacology 2022, 47, 292–308. [Google Scholar] [CrossRef] [PubMed]
- Bunney, W.E.; Bunney, B.G. Evidence for a compromised dorsolateral prefrontal cortical parallel circuit in schizophrenia. Brain Res. Rev. 2000, 31, 138–146. [Google Scholar] [CrossRef]
- Hughes, H.; Brady, L.J.; Schoonover, K.E. GABAergic dysfunction in postmortem dorsolateral prefrontal cortex: Implications for cognitive deficits in schizophrenia and affective disorders. Front. Cell. Neurosci. 2024, 18, 1440834. [Google Scholar] [CrossRef]
- Barch, D.M.; Carter, C.S.; Braver, T.S.; Sabb, F.W.; MacDonald, A.; Noll, D.C.; Cohen, J.D. Selective deficits in prefrontal cortex function in medication-naive patients with schizophrenia. Arch. Gen. Psychiatry 2001, 58, 280–288. [Google Scholar] [CrossRef]
- Yoon, J.H.; Minzenberg, M.J.; Ursu, S.; Walters, R.; Wendelken, C.; Ragland, J.D.; Carter, C.S. Association of dorsolateral prefrontal cortex dysfunction with disrupted coordinated brain activity in schizophrenia: Relationship with impaired cognition, behavioral disorganization, and global function. Am. J. Psychiatry 2008, 165, 1006–1014. [Google Scholar] [CrossRef]
- Lesh, T.A.; Westphal, A.J.; Niendam, T.A.; Yoon, J.H.; Minzenberg, M.J.; Ragland, J.D.; Carter, C.S. Proactive and reactive cognitive control and dorsolateral prefrontal cortex dysfunction in first episode schizophrenia. NeuroImage Clin. 2013, 2, 590–599. [Google Scholar] [CrossRef]
- Miller, E.K. The prefontral cortex and cognitive control. Nat. Rev. Neurosci. 2000, 1, 59–65. [Google Scholar] [CrossRef]
- Weissman, D.H.; Perkins, A.S.; Woldorff, M.G. Cognitive control in social situations: A role for the dorsolateral prefrontal cortex. Neuroimage 2008, 40, 955–962. [Google Scholar] [CrossRef]
- Levy, R.; Goldman-Rakic, P.S. Segregation of working memory functions within the dorsolateral prefrontal cortex. Exp. Brain Res. 2000, 133, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Robbins, T.W. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Mihaljević-Peleš, A.; Bajs Janović, M.; Šagud, M.; Živković, M.; Janović, Š.; Jevtović, S. Cognitive deficit in schizophrenia: An overview. Psychiatr. Danub. 2019, 31 (Suppl. S2), 139–142. [Google Scholar]
- Biondi, M.; Marino, M.; Mantini, D.; Spironelli, C. Unveiling altered connectivity between cognitive networks and cerebellum in schizophrenia. Schizophr. Res. 2024, 271, 47–58. [Google Scholar] [CrossRef] [PubMed]
- García-León, M.Á.; Fuentes-Claramonte, P.; Soler-Vidal, J.; Ramiro-Sousa, N.; Salgado-Pineda, P.; Salavert, J.; Pomarol-Clotet, E. Cortical volume abnormalities in schizophrenia: Correlations with symptoms and cognitive impairment. Schizophr. Res. 2024, 266, 50–57. [Google Scholar] [CrossRef]
- Glahn, D.C.; Ragland, J.D.; Abramoff, A.; Barrett, J.; Laird, A.R.; Bearden, C.E.; Velligan, D.I. Beyond hypofrontality: A quantitative meta-analysis of functional neuroimaging studies of working memory in schizophrenia. Hum. Brain Mapp. 2005, 25, 60–69. [Google Scholar] [CrossRef]
- Gong, Q.; Lui, S.; Sweeney, J.A. A selective review of cerebral abnormalities in patients with first-episode schizophrenia before and after treatment. Am. J. Psychiatry 2016, 173, 232–243. [Google Scholar] [CrossRef]
- Lopez-Garcia, P.; Aizenstein, H.J.; Snitz, B.E.; Walter, R.P.; Carter, C.S. Automated ROI-based brain parcellation analysis of frontal and temporal brain volumes in schizophrenia. Psychiatry Res. 2006, 147, 153–161. [Google Scholar] [CrossRef]
- Andreou, C.; Borgwardt, S. Structural and functional imaging markers for susceptibility to psychosis. Mol. Psychiatry 2020, 25, 2773–2785. [Google Scholar] [CrossRef]
- Picado, M.; Carmona, S.; Hoekzema, E.; Pailhez, G.; Bergé, D.; Mané, A.; Fauquet, J.; Hilferty, J.; Moreno, A.; Cortizo, R. The neuroanatomical basis of panic disorder and social phobia in schizophrenia: A voxel based morphometric study. PLoS ONE 2015, 10, e0119847. [Google Scholar] [CrossRef]
- Ellison-Wright, I.; Glahn, D.C.; Laird, A.R.; Thelen, S.M.; Bullmore, E. The anatomy of first-episode and chronic schizophrenia: An anatomical likelihood estimation meta-analysis. Am. J. Psychiatry 2008, 165, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Gur, R.E.; Turetsky, B.I.; Cowell, P.E.; Finkelman, C.; Maany, V.; Grossman, R.I.; Arnold, S.E.; Bilker, W.B.; Gur, R.C. Temporolimbic volume reductions in schizophrenia. Arch. Gen. Psychiatry 2000, 57, 769–775. [Google Scholar] [CrossRef]
- Yang, Y.; Li, X.; Cui, Y.; Liu, K.; Qu, H.; Lu, Y.; Li, W.; Zhang, L.; Zhang, Y.; Song, J.; et al. Reduced gray matter volume in orbitofrontal cortex across schizophrenia, major depressive disorder, and bipolar disorder: A comparative imaging study. Front. Neurosci. 2022, 16, 919272. [Google Scholar] [CrossRef]
- Kasai, K.; Shenton, M.E.; Salisbury, D.F.; Onitsuka, T.; Toner, S.K.; Yurgelun-Todd, D.; Kikinis, R.; Jolesz, F.A.; McCarley, R.W. Differences and similarities in insular and temporal pole MRI gray matter volume abnormalities in first-episode schizophrenia and affective psychosis. Arch. Gen. Psychiatry 2003, 60, 1069–1077. [Google Scholar] [CrossRef]
- Lee, S.H.; Niznikiewicz, M.; Asami, T.; Otsuka, T.; Salisbury, D.F.; Shenton, M.E.; McCarley, R.W. Initial and progressive gray matter abnormalities in insular gyrus and temporal pole in first-episode schizophrenia contrasted with first-episode affective psychosis. Schizophr. Bull. 2016, 42, 790–801. [Google Scholar] [CrossRef] [PubMed]
- Bhojraj, T.S.; Sweeney, J.A.; Prasad, K.M.; Eack, S.M.; Francis, A.N.; Miewald, J.M.; Montrose, D.M.; Keshavan, M.S. Gray matter loss in young relatives at risk for schizophrenia: Relation with prodromal psychopathology. Neuroimage 2011, 54, S272–S279. [Google Scholar] [CrossRef]
- Van Erp, T.G.; Walton, E.; Hibar, D.P.; Schmaal, L.; Jiang, W.; Glahn, D.C.; Pearlson, G.D.; Yao, N.; Fukunaga, M.; Hashimoto, R.; et al. Cortical brain abnormalities in 4474 individuals with schizophrenia and 5098 control subjects via the enhancing neuro imaging genetics through meta analysis (ENIGMA) consortium. Biol. Psychiatry 2018, 84, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Herold, R.; Feldmann, A.; Simon, M.; Tenyi, T.; Kövér, F.; Nagy, F.; Varga, E.; Fekete, S. Regional gray matter reduction and theory of mind deficit in the early phase of schizophrenia: A voxel-based morphometric study. Acta Psychiatr. Scand. 2009, 119, 199–208. [Google Scholar] [CrossRef]
- Horn, H.; Federspiel, A.; Wirth, M.; Müller, T.J.; Wiest, R.; Walther, S.; Strik, W. Gray matter volume differences specific to formal thought disorder in schizophrenia. Psychiatry Res. 2010, 182, 183–186. [Google Scholar] [CrossRef]
- Herlin, B.; Navarro, V.; Dupont, S. The temporal pole: From anatomy to function—A literature appraisal. J. Chem. Neuroanat. 2021, 113, 101925. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.G.; Thompson, W.K. Functional brain imaging in schizophrenia: Selected results and methods. Curr. Top. Behav. Neurosci. 2010, 4, 181–214. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.M.; Mathalon, D.H.; Whitfield, S.; Faustman, W.O.; Roth, W.T. Reduced communication between frontal and temporal lobes during talking in schizophrenia. Biol. Psychiatry 2002, 51, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Barredo, J.; Öztekin, I.; Badre, D. Ventral fronto-temporal pathway supporting cognitive control of episodic memory retrieval. Cereb. Cortex 2015, 25, 1004–1019. [Google Scholar] [CrossRef]
- McCutcheon, R.A.; Keefe, R.S.; McGuire, P.K. Cognitive impairment in schizophrenia: Aetiology, pathophysiology, and treatment. Mol. Psychiatry 2023, 28, 1902–1918. [Google Scholar] [CrossRef]
- Alkan, E.; Davies, G.; Evans, S.L. Cognitive impairment in schizophrenia: Relationships with cortical thickness in fronto-temporal regions, and dissociability from symptom severity. NPJ Schizophr. 2021, 7, 20. [Google Scholar] [CrossRef]
- Nickl-Jockschat, T.; Schneider, F.; Pagel, A.D.; Laird, A.R.; Fox, P.T.; Eickhoff, S.B. Progressive pathology is functionally linked to the domains of language and emotion: Meta-analysis of brain structure changes in schizophrenia patients. Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261, 166–171. [Google Scholar] [CrossRef]
- Cipriani, G.; Danti, S.; Nuti, A.; Di Fiorino, M.; Cammisuli, D.M. Is that schizophrenia or frontotemporal dementia? Supporting clinicians in making the right diagnosis. Acta Neurol. Belg. 2020, 120, 799–804. [Google Scholar] [CrossRef]
- Tanaka, M.; Battaglia, S.; Giménez-Llort, L.; Chen, C.; Hepsomali, P.; Avenanti, A.; Vécsei, L. Innovation at the intersection: Emerging translational research in neurology and psychiatry. Cells 2024, 13, 790. [Google Scholar] [CrossRef]
- Harciarek, M.; Malaspina, D.; Sun, T.; Goldberg, E. Schizophrenia and frontotemporal dementia: Shared causation? Int. Rev. Psychiatry 2013, 25, 168–177. [Google Scholar] [CrossRef]
- Zheng, F.; Li, C.; Zhang, D.; Cui, D.; Wang, Z.; Qiu, J. Study on the sub-regions volume of hippocampus and amygdala in schizophrenia. Quant. Imaging Med. Surg. 2019, 9, 1025. [Google Scholar] [CrossRef] [PubMed]
- Di Gregorio, F.; Battaglia, S. The intricate brain–body interaction in psychiatric and neurological diseases. Adv. Clin. Exp. Med. 2024, 33, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Port, J.D.; Bazzocchi, M.; Renshaw, P.F. Update on the use of MR for assessment and diagnosis of psychiatric diseases. Radiology 2010, 255, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Sokolowski, K.; Corbin, J.G. Wired for behaviors: From development to function of innate limbic system circuitry. Front. Mol. Neurosci. 2012, 5, 55. [Google Scholar] [CrossRef]
- Torrico, T.J.; Abdijadid, S. Neuroanatomy, Limbic System; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Phelps, E.A. Emotion and cognition: Insights from studies of the human amygdala. Annu. Rev. Psychol. 2006, 57, 27–53. [Google Scholar] [CrossRef]
- Šimić, G.; Tkalčić, M.; Vukić, V.; Mulc, D.; Španić, E.; Šagud, M.; Olucha-Bordonau, F.E.; Vukšić, M.R.; Hof, P. Understanding Emotions: Origins and Roles of the Amygdala. Biomolecules 2021, 11, 823. [Google Scholar] [CrossRef]
- LeDoux, J. The amygdala. Curr. Biol. 2007, 17, R868–R874. [Google Scholar] [CrossRef]
- Aminoff, E.M.; Kveraga, K.; Bar, M. The role of the parahippocampal cortex in cognition. Trends Cogn. Sci. 2013, 17, 379–390. [Google Scholar] [CrossRef]
- Romeo, Z.; Biondi, M.; Oltedal, L.; Spironelli, C. The Dark and Gloomy Brain: Grey Matter Volume Alterations in Major Depressive Disorder–Fine-Grained Meta-Analyses. Depress. Anxiety 2024, 2024, 6673522. [Google Scholar] [CrossRef]
- Price, J.L.; Drevets, W.C. Neurocircuitry of mood disorders. Neuropsychopharmacology 2010, 35, 192–216. [Google Scholar] [CrossRef]
- Dugré, J.R.; Bitar, N.; Dumais, A.; Potvin, S. Limbic hyperactivity in response to emotionally neutral stimuli in schizophrenia: A neuroimaging meta-analysis of the hypervigilant mind. Am. J. Psychiatry 2019, 176, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Pantelis, C.; Velakoulis, D.; McGorry, P.D.; Wood, S.J.; Suckling, J.; Phillips, L.J.; Yung, A.R.; Bullmore, E.T.; Brewer, W.; Soulsby, B.; et al. Neuroanatomical abnormalities before and after onset of psychosis: A cross-sectional and longitudinal MRI comparison. Lancet 2003, 361, 281–288. [Google Scholar] [CrossRef]
- Pol, H.E.H.; Schnack, H.G.; Mandl, R.C.; van Haren, N.E.; Koning, H.; Collins, D.L.; Evans, A.C.; Kahn, R.S. Focal gray matter density changes in schizophrenia. Arch. Gen. Psychiatry 2001, 58, 1118–1125. [Google Scholar] [CrossRef]
- Lieberman, J.A. Is schizophrenia a neurodegenerative disorder? A clinical and neurobiological perspective. Biol. Psychiatry 1999, 46, 729–739. [Google Scholar] [CrossRef]
- Lin, Y.; Li, M.; Zhou, Y.; Deng, W.; Ma, X.; Wang, Q.; Wang, G.; Li, Y.; Jiang, L.; Hu, X.; et al. Age-related reduction in cortical thickness in first-episode treatment-naïve patients with schizophrenia. Neurosci. Bull. 2019, 35, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Kochunov, P.; Hong, L.E. Neurodevelopmental and neurodegenerative models of schizophrenia: White matter at the center stage. Schizophr. Bull. 2014, 40, 721–728. [Google Scholar] [CrossRef]
- Lin, Y.H.; Young, I.M.; Conner, A.K.; Glenn, C.A.; Chakraborty, A.R.; Nix, C.E.; Bai, M.Y.; Dhanaraj, V.; Fonseka, R.D.; Hormovas, J.; et al. Anatomy and white matter connections of the inferior temporal gyrus. World Neurosurg. 2020, 143, e656–e666. [Google Scholar] [CrossRef]
- APA Dictionary of Psychology, “Somatic Symptom Disorder”. Available online: https://dictionary.apa.org/somatic-symptom-disorder. (accessed on 14 November 2024).
- Su, Q.; Yao, D.; Jiang, M.; Liu, F.; Jiang, J.; Xu, C.; Dai, Y.; Yu, M.; Long, L.; Li, H.; et al. Increased functional connectivity strength of right inferior temporal gyrus in first-episode, drug-naive somatization disorder. Aust. N. Z. J. Psychiatry 2015, 49, 74–81. [Google Scholar] [CrossRef]
- Du, L.; Wang, J.; Meng, B.; Yong, N.; Yang, X.; Huang, Q.; Zhang, Y.; Yang, L.; Qu, Y.; Chen, Z.; et al. Early life stress affects limited regional brain activity in depression. Sci. Rep. 2016, 6, 25338. [Google Scholar] [CrossRef]
- APA Dictionary of Psychology, “Alexithymia”. Available online: https://dictionary.apa.org/alexithymia (accessed on 14 November 2024).
- Deng, Y.; Ma, X.; Tang, Q. Brain response during visual emotional processing: An fMRI study of alexithymia. Psychiatry Res. 2013, 213, 225–229. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, B.; Luo, Q.; Qiu, L.; Wang, S. Gray matter structural alterations in social anxiety disorder: A voxel-based meta-analysis. Front. Psychiatry 2018, 9, 449. [Google Scholar] [CrossRef] [PubMed]
- Honea, R.; Crow, T.J.; Passingham, D.; Mackay, C.E. Regional deficits in brain volume in schizophrenia: A meta-analysis of voxel-based morphometry studies. Am. J. Psychiatry 2005, 162, 2233–2245. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Suzuki, M.; Zhou, S.Y.; Tanino, R.; Hagino, H.; Niu, L.; Kawasaki, Y.; Seto, H.; Kurachi, M. Temporal lobe gray matter in schizophrenia spectrum: A volumetric MRI study of the fusiform gyrus, parahippocampal gyrus, and middle and inferior temporal gyri. Schizophr. Res. 2006, 87, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, N.; Shenton, M.E.; Salisbury, D.F.; Hirayasu, Y.; Onitsuka, T.; Ersner, H.; Yurgelun-Todd, D.; Kikinis, R.; Jolesz, F.A.; McCarley, R.W. Middle and inferior temporal gyrus gray matter volume abnormalities in first-episode schizophrenia: An MRI study. Am. J. Psychiatry 2006, 163, 2103–2110. [Google Scholar] [CrossRef]
- Onitsuka, T.; Shenton, M.E.; Salisbury, D.F.; Dickey, C.C.; Kasai, K.; Toner, S.K.; Frumin, M.; Kikinis, R.; Jolesz, F.A.; McCarley, R.W. Middle and inferior temporal gyrus gray matter volume abnormalities in chronic schizophrenia: An MRI study. Am. J. Psychiatry 2004, 161, 1603–1611. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| SZ (n = 74) | HC (n = 91) | Statistics | ||
|---|---|---|---|---|
| Age | 37.43 ± 14.02 | 38.54 ± 11.67 | t163 = −0.55, n.s. | |
| Sex (M/F) | 60/14 | 65/26 | χ2 = 1.51, n.s. | |
| Age of onset | 22.61 ± 8.85 | - | ||
| SZ-m | SZ-f | |||
| 22.38 ± 9.07 | 23.57 ± 8.04 | t72 = −0.45, n.s. | ||
| Illness duration (years) | 14.82 ± 12.33 | - | ||
| SZ-m | SZ-f | |||
| 14.78 ± 12.73 | 15 ± 10.86 | t72 = −0.06, n.s | ||
| Total olanzapine equivalent dose (mg) | 14.72 ± 10.46 | - | ||
| SZ-m | SZ-f | |||
| 13.7 ± 8.7 | 18.95 ± 15.57 | t72 = 0.66, n.s | ||
| Total chlorpromazine equivalent dose (mg) | 379.06 ± 300.78 | - | ||
| SZ-m | SZ-f | |||
| 355.97 ± 240.41 | 476.36 ± 480.19 | t72 = −1.27, n.s | ||
| MNI Coordinates | Volume (mm3) | t-Score | Cohen’s d Value | BA | Anatomical Label |
|---|---|---|---|---|---|
| 42, 19, −22 | 1015 | 6.57 | 1.029 | 38 | Right-Temporalpole |
| 39, 19, −26 | 834 | 6.33 | 0.992 | 38 | Right-Temporalpole |
| −41, 13, −20 | 313 | 5.34 | 0.836 | 38 | Left-Temporalpole |
| −37, 19, −27 | 148 | 5.12 | 0.802 | 38 | Left-Temporalpole |
| −24, 4, −28 | 246 | 5.43 | 0.851 | 36 | Left-Parahipp |
| 39, 40, −10 | 150 | 5.38 | 0.843 | 47 | Right-ParsOrbitalis |
| −39, 36, 14 | 142 | 5.20 | 0.814 | 46 | Left-dlPFC |
| 20, −1, −20 | 130 | 5.65 | 0.885 | n/a | Right-Amygdala |
| 23, −1, −18 | 115 | 5.85 | 0.916 | n/a | Right-Amygdala |
| 48, −8, 15 | 45 | 5.26 | 0.824 | 1 | Right-PrimSensory |
| GP Items | GP Scores | Exact q-Value | Cohen’s d Value |
|---|---|---|---|
| GP01—Somatic concern | r = 0.37 | 0.001314 | 0.797 |
| GP02—Anxiety | r = 0.70 | 0.000000 (*) | 1.960 |
| GP03—Guilt feeling | r = 0.55 | 0.000000 (*) | 1.317 |
| GP04—Tension | r = 0.69 | 0.000000 (*) | 1.907 |
| GP05—Mannerisms and posturing | r = 0.58 | 0.000000 (*) | 1.424 |
| GP06—Depression | r = 0.72 | 0.000000 (*) | 2.075 |
| GP07—Motor retardation | r = 0.38 | 0.001132 | 0.822 |
| GP08—Uncooperativeness | r = 0.29 | 0.01270 | 0.606 |
| GP09—Unusual thought content | r = 0.64 | 0.000000 (*) | 1.666 |
| GP10—Disorientation | r = 0.35 | 0.002432 | 0.747 |
| GP11—Poor attention | r = 0.37 | 0.001314 | 0.797 |
| GP12—Lack of judgment and insight | r = 0.38 | 0.001132 | 0.822 |
| GP13—Disturbance of volition | r = 0.66 | 0.000000 (*) | 1.759 |
| GP14—Poor impulse control | r = 0.41 | 0.000448 | 0.899 |
| GP15—Preoccupation | r = 0.54 | 0.000001 (*) | 1.283 |
| GP16—Active social avoidance | r = 0.54 | 0.000001 (*) | 1.283 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biondi, M.; Marino, M.; Mantini, D.; Spironelli, C. Brain Structural Alterations Underlying Mood-Related Deficits in Schizophrenia. Biomedicines 2025, 13, 736. https://doi.org/10.3390/biomedicines13030736
Biondi M, Marino M, Mantini D, Spironelli C. Brain Structural Alterations Underlying Mood-Related Deficits in Schizophrenia. Biomedicines. 2025; 13(3):736. https://doi.org/10.3390/biomedicines13030736
Chicago/Turabian StyleBiondi, Margherita, Marco Marino, Dante Mantini, and Chiara Spironelli. 2025. "Brain Structural Alterations Underlying Mood-Related Deficits in Schizophrenia" Biomedicines 13, no. 3: 736. https://doi.org/10.3390/biomedicines13030736
APA StyleBiondi, M., Marino, M., Mantini, D., & Spironelli, C. (2025). Brain Structural Alterations Underlying Mood-Related Deficits in Schizophrenia. Biomedicines, 13(3), 736. https://doi.org/10.3390/biomedicines13030736