
Combination of Brentuximab Vedotin and Pembrolizumab as Salvage Treatment Before Autologous Stem Cell Transplantation and Maintenance in Patients with Relapsed/Refractory Hodgkin Lymphoma †


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
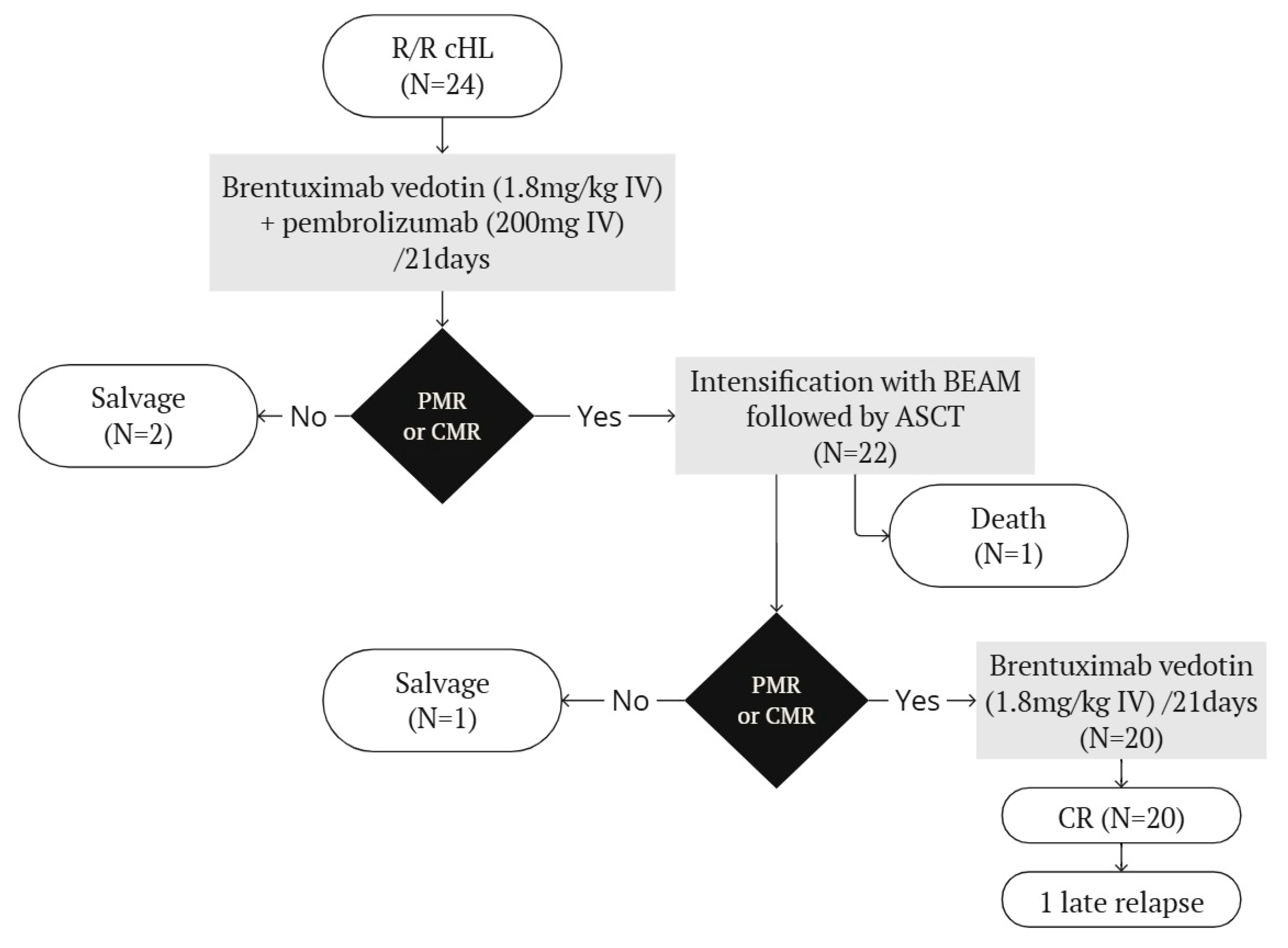
3.2. Treatment and Outcomes
3.3. Toxicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCT | Autologous stem cell transplantation |
| BV | Brentuximab Vedotin |
| cHL | Classical Hodgkin lymphoma |
| CMR | Complete metabolic response |
| CTCAE | Common Terminology Criteria for Adverse Events |
| DS | Deauville score |
| HDCT | High-dose chemotherapy |
| HLH | Hemophagocytic lymphohistiocytosis |
| OR | Overall response |
| OS | Overall survival |
| PET-CT | 18FDG PET-CT |
| PFS | Progression-free survival |
| R/R | Relapsed or refractory |
References
- Castagna, L.; Santoro, A.; Carlo-Stella, C. Salvage Therapy for Hodgkin’s Lymphoma: A Review of Current Regimens and Outcomes. J. Blood Med. 2020, 11, 389–403. [Google Scholar] [CrossRef] [PubMed]
- Eichenauer, D.A.; Aleman, B.M.P.; André, M.; Federico, M.; Hutchings, M.; Illidge, T.; Engert, A.; Ladetto, M.; ESMO Guidelines Committee. Hodgkin lymphoma: ESMO clinical practice guidelines for diagnosis, treatment, and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv19–iv29. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Hodgkin Lymphoma (Version 1.2023). National Comprehensive Cancer Network. Published 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/hodgkin.pdf (accessed on 20 July 2024).
- Ansell, S.M. Hodgkin lymphoma: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2022, 97, 1478–1488. [Google Scholar] [CrossRef] [PubMed]
- Bröckelmann, P.J.; Müller, H.; Gillessen, S.; Yang, X.; Koeppel, L.; Pilz, V.; Marinello, P.; Kaskel, P.; Raut, M.; Fuchs, M.; et al. Clinical outcomes of relapsed and refractory Hodgkin lymphoma patients after contemporary first-line treatment: A German Hodgkin Study Group analysis. Leukemia 2022, 36, 772–780. [Google Scholar] [CrossRef]
- Adams, H.J.; Kwee, T.C. Prognostic value of pretransplant FDG-PET in refractory/relapsed Hodgkin lymphoma treated with autologous stem cell transplantation: Systematic review and meta-analysis. Ann. Hematol. 2016, 95, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, C.H.; Walewski, J.; Nademanee, A.; Masszi, T.; Agura, E.; Holowiecki, J.; Abidi, M.H.; Chen, A.I.; Stiff, P.; Viviani, S.; et al. Five-year PFS from the AETHERA trial of brentuximab vedotin for Hodgkin lymphoma at high risk of progression or relapse. Blood 2018, 132, 2639–2642. [Google Scholar] [CrossRef] [PubMed]
- Bröckelmann, P.J.; Müller, H.; Kücüksarioglan, E.; Kaskel, P.; Metterlein, V.; Giezek, H.; Balakumaran, A.; Raut, M.; Engert, A.; von Tresckow, B. Outcomes of patients with the third or higher relapsed classical Hodgkin lymphoma: Results from the German Hodgkin Study Group. Ann. Oncol. 2019, 30, 490–491. [Google Scholar] [CrossRef] [PubMed]
- Harker-Murray, P.; Mauz-Körholz, C.; Leblanc, T.; Mascarin, M.; Michel, G.; Cooper, S.; Beishuizen, A.; Leger, K.J.; Amoroso, L.; Buffardi, S.; et al. Nivolumab and brentuximab vedotin with or without bendamustine for R/R Hodgkin lymphoma in children, adolescents, and young adults. Blood 2023, 141, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Advani, R.H.; Moskowitz, A.J.; Bartlett, N.L.; Vose, J.M.; Ramchandren, R.; Feldman, T.A.; LaCasce, A.S.; Christian, B.A.; Ansell, S.M.; Moskowitz, C.H.; et al. Brentuximab vedotin in combination with nivolumab in relapsed or refractory Hodgkin lymphoma: 3-year study results. Blood 2021, 138, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, J.; Ramchandren, R.; Santoro, A.; Paszkiewicz-Kozik, E.; Gasiorowski, R.; A Johnson, N.; Fogliatto, L.M.; Goncalves, I.; de Oliveira, J.S.R.; Buccheri, V.; et al. Pembrolizumab versus brentuximab vedotin in relapsed or refractory classical Hodgkin lymphoma (KEYNOTE-204): An interim analysis of a multicentre, randomised, open-label, phase 3 study. Lancet Oncol. 2021, 22, 512–524. [Google Scholar] [CrossRef]
- Massaro, F.; Meuleman, N.; Bron, D.; Vercruyssen, M.; Maerevoet, M. Brentuximab vedotin and pembrolizumab combination in patients with relapsed/refractory Hodgkin lymphoma: A single-centre retrospective analysis. Cancers 2022, 14, 982. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Published 2017. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 20 July 2024).
- Knauft, J.; Schenk, T.; Ernst, T.; Schnetzke, U.; Hochhaus, A.; La Rosée, P.; Birndt, S. Lymphoma-associated hemophagocytic lymphohistiocytosis (LA-HLH): A scoping review unveils clinical and diagnostic patterns of a lymphoma subgroup with poor prognosis. Leukemia 2024, 38, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Mosalem, O.; Pai, T.; Alqawasma, M.; Shaikh, M.; Li, K.D.; Moustafa, M.A. Severe cytokine release syndrome and hemophagocytic lymphohistiocytosis (HLH)-like syndrome following administration of combined brentuximab vedotin and nivolumab for recurrent classical Hodgkin lymphoma: A case report. J. Blood Med. 2024, 15, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Massa, H.; Massaro, F.; Maerevoet, M. Combination of brentuximab vedotin and pembrolizumab before intensification with autologous stem cell transplantation and maintenance in patients with relapsed/refractory Hodgkin lymphoma. Presented at the EHA2024 Hybrid Congress, Madrid, Spain, 13–16 June 2024. [Google Scholar]

{kind=link}
| Characteristics | |
|---|---|
| Sex, n (%) | |
| Male | 19 (79.2%) |
| Female | 5 (20.8%) |
| Median age at initial diagnosis, years (range) | 28.2 (7.6–49.3) |
| Median age at referral, years (range) | 30.2 (20.5–52.6) |
| Median time from diagnosis to referral, years (range) | 2.6 (0.8–16.2) |
| Ann Arbor stage at initial diagnosis, n (%) | |
| II | 5 (20.8%) |
| III | 4 (16.7%) |
| IV | 15 (62.5%) |
| Number of prior treatments, n (%) | |
| 2 | 4 (16.7%) |
| 3 | 14 (58.3%) |
| 4 | 5 (20.8%) |
| 5 | 1 (4.2%) |
| Types of prior treatments as first line, n (%) | |
| ABVD | 9 (37.5%) |
| ABVD → BEACOPP-like | 2 (8.3%) |
| BEACOPP-like | 7 (29.2%) |
| BEACOPP-like → ABVD | 3 (12.5%) |
| CHOP | 3 (12.5%) |
| In subsequent lines, n (%) | |
| ABVD | 2 (8.3%) |
| BEACOPP-like | 3 (12.5%) |
| DHAC-like | 20 (83.3%) |
| BeGeV-like | 15 (62.5%) |
| ICE | 3 (12.5%) |
| rituximab | 1 (4.2%) |
| radiotherapy | 5 (20.8%) |
| PD1-inhibitor | 0 (0.0%) |
| brentuximab vedotin | 2 (8.3%) |
| ASCT | 1 (4.2%) |
| Status after front-line therapy, n (%) | |
| Primary refractory | 14 (58.3%) |
| Early relapse (<12 months) | 3 (12.5%) |
| Late relapse (≥12 months) | 7 (29.2%) |
| Disease burden at referral, n (%) | |
| Stage III–IV | 21 (87.5%) |
| Extra nodal disease | 20 (83.3%) |
| None of the above | 3 (12.5%) |
| Median follow-up time, months (range) | 13.3 (6.4–39.9) |
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | Grade 5 | |
|---|---|---|---|---|---|
| Salvage with BV and pembrolizumab (N = 24) | |||||
| Total | 21 | 14 | 11 | 8 | 0 |
| Hematological | |||||
| Neutropenia | 0 | 1 | 1 | 3 | 0 |
| Anemia | 7 | 5 | 4 | 0 | 0 |
| Thrombocytopenia | 4 | 5 | 0 | 1 | 0 |
| Lymphopenia | 7 | 2 | 5 | 2 | 0 |
| Thyroid | |||||
| Hypothyroidism | 2 | 0 | 0 | 0 | 0 |
| Hyperthyroidism | 0 | 0 | 0 | 1 | 0 |
| Myalgia/arthralgia | 1 | 0 | 1 | 0 | 0 |
| Pancreatitis | 0 | 1 | 0 | 0 | 0 |
| Hemophagocytic lymphohistiocytosis | 0 | 0 | 0 | 1 | 0 |
| Intensification with BEAM and ASCT (N = 22) | |||||
| Total | 4 | 12 | 29 | 67 | 1 |
| Neurological | |||||
| Autonomous | 0 | 1 | 0 | 0 | 0 |
| Hematological | |||||
| Neutropenia | 0 | 0 | 2 | 20 | 0 |
| Anemia | 2 | 9 | 9 | 2 | 0 |
| Thrombopenia | 1 | 0 | 0 | 21 | 0 |
| Lymphopenia | 0 | 1 | 0 | 21 | 0 |
| Infectious | 0 | 0 | 18 | 1 | 1 |
| Thyroid | |||||
| Hypothyroidism | 1 | 1 | 0 | 0 | 0 |
| Pneumonitis | 0 | 0 | 0 | 1 | 0 |
| Hemophagocytic lymphohistiocytosis | 0 | 0 | 0 | 1 | 0 |
| BV maintenance (N = 20) | |||||
| Total | 34 | 17 | 5 | 1 | 0 |
| Neurological | |||||
| Autonomous | 1 | 3 | 0 | 0 | 0 |
| Peripheral | 6 | 3 | 1 | 0 | 0 |
| Hematological | |||||
| Neutropenia | 6 | 3 | 2 | 1 | 0 |
| Anemia | 3 | 5 | 0 | 0 | 0 |
| Thrombopenia | 7 | 1 | 1 | 0 | 0 |
| Lymphopenia | 9 | 0 | 1 | 0 | 0 |
| Thyroid | |||||
| Hypothyroidism | 0 | 1 | 0 | 0 | 0 |
| Myalgia/arthralgia | 2 | 1 | 0 | 0 | 0 |
| Reason | Number of Patients, n (%) |
|---|---|
| Peripheral neuropathy | 8 (40%) |
| Arthralgia/myalgia | 3 (15%) |
| Autonomous neuropathy | 3 (15%) |
| Grade 3 thrombopenia | 1 (5%) |
| Grade 4 neutropenia | 1 (5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massa, H.; Massaro, F.; Maerevoet, M. Combination of Brentuximab Vedotin and Pembrolizumab as Salvage Treatment Before Autologous Stem Cell Transplantation and Maintenance in Patients with Relapsed/Refractory Hodgkin Lymphoma. Biomedicines 2025, 13, 252. https://doi.org/10.3390/biomedicines13020252
Massa H, Massaro F, Maerevoet M. Combination of Brentuximab Vedotin and Pembrolizumab as Salvage Treatment Before Autologous Stem Cell Transplantation and Maintenance in Patients with Relapsed/Refractory Hodgkin Lymphoma. Biomedicines. 2025; 13(2):252. https://doi.org/10.3390/biomedicines13020252
Chicago/Turabian StyleMassa, Hanne, Fulvio Massaro, and Marie Maerevoet. 2025. "Combination of Brentuximab Vedotin and Pembrolizumab as Salvage Treatment Before Autologous Stem Cell Transplantation and Maintenance in Patients with Relapsed/Refractory Hodgkin Lymphoma" Biomedicines 13, no. 2: 252. https://doi.org/10.3390/biomedicines13020252
APA StyleMassa, H., Massaro, F., & Maerevoet, M. (2025). Combination of Brentuximab Vedotin and Pembrolizumab as Salvage Treatment Before Autologous Stem Cell Transplantation and Maintenance in Patients with Relapsed/Refractory Hodgkin Lymphoma. Biomedicines, 13(2), 252. https://doi.org/10.3390/biomedicines13020252