

Clinical Features and Survival Analysis of Lupus Nephritis among Patients with Systemic Lupus Erythematosus: A Three-Decade-Long Retrospective Cohort Study


 ,
, 
Abstract
1. Introduction
2. Methodology
2.1. Study Population
2.2. Clinical and Laboratory Evaluation
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Clinical Characteristics and Laboratory Findings of LN and Non-LN Patients
3.3. Treatment Modalities for LN and Non-LN Patients
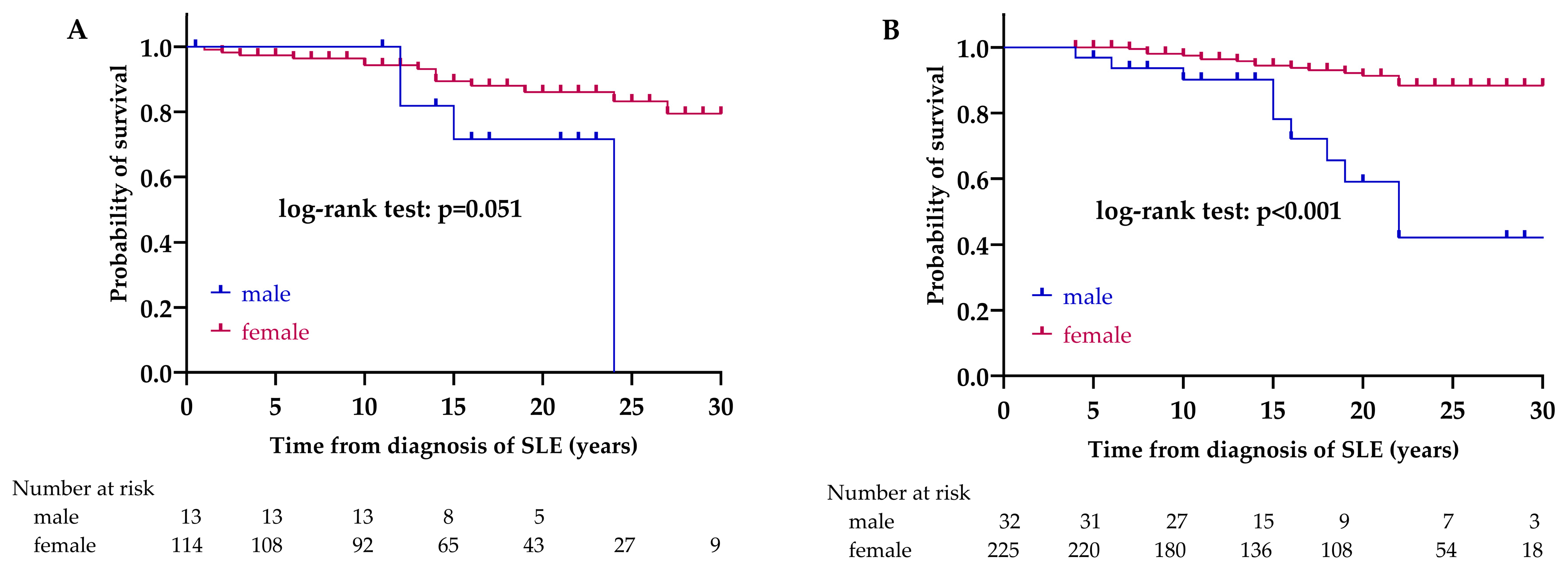
3.4. Survival Rates and Causes of Death
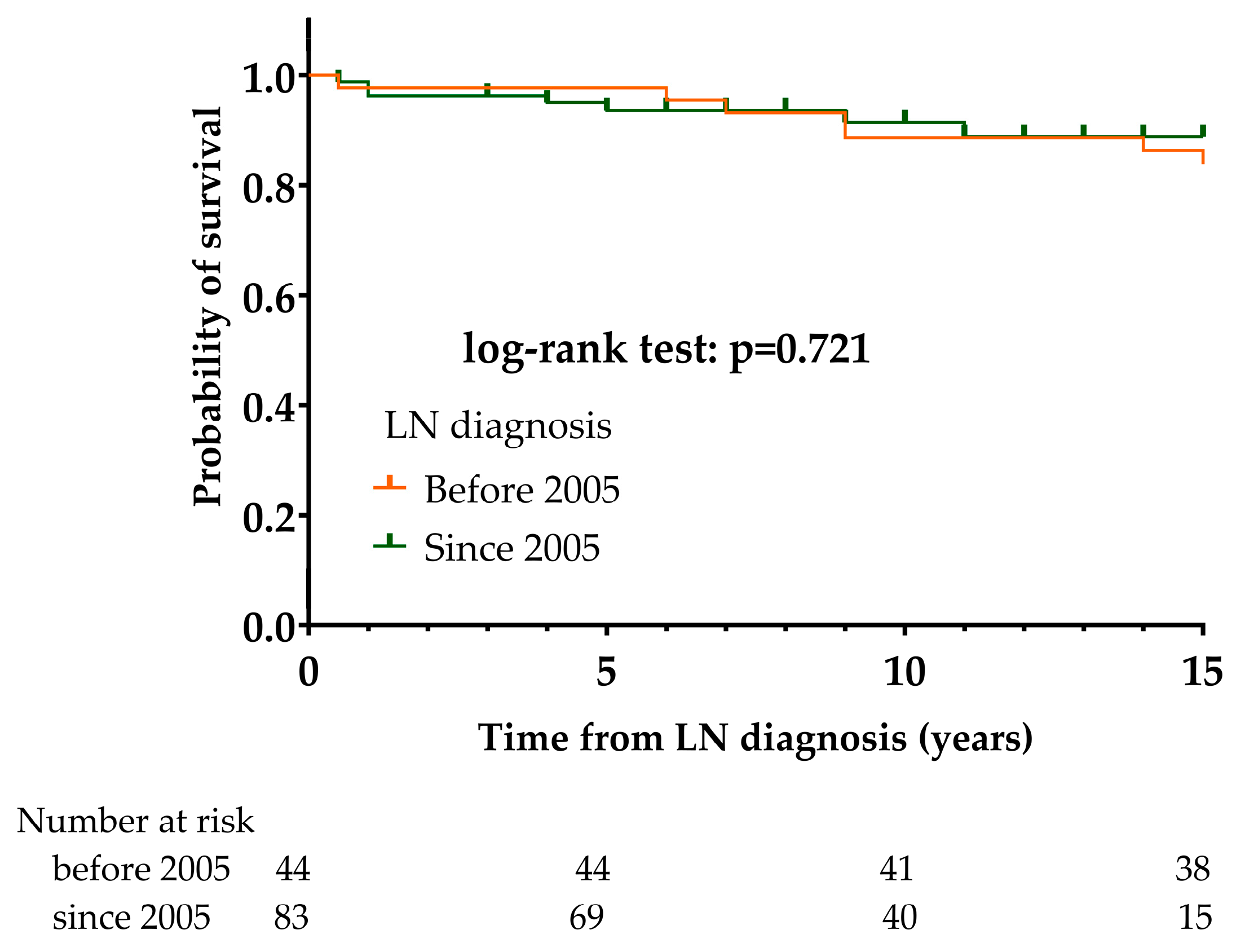
3.5. Differences between LN Patients Diagnosed before 2005 or since 2005
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anders, H.J.; Saxena, R.; Zhao, M.H.; Parodis, I.; Salmon, J.E.; Mohan, C. Lupus nephritis. Nat. Rev. Dis. Primers 2020, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Stillman, I.K. Systemic Lupus Erythematosus, 5th ed.; Lahita, R., Ed.; Academic Press: San Diego, CA, USA, 2011; pp. 769–814. [Google Scholar]
- Hanly, J.G.; O’Keeffe, A.G.; Su, L.; Urowitz, M.B.; Romero-Diaz, J.; Gordon, C.; Bae, S.C.; Bernatsky, S.; Clarke, A.E.; Wallace, D.J.; et al. The frequency and outcome of lupus nephritis: Results from an international inception cohort study. Rheumatology 2016, 55, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Yurkovich, M.; Vostretsova, K.; Chen, W.; Aviña-Zubieta, J.A. Overall and cause-specific mortality in patients with systemic lupus erythematosus: A meta-analysis of observational studies. Arthritis Care Res. 2014, 66, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Choi, S.J.; Ji, J.D.; Song, G.G. Overall and cause-specific mortality in systemic lupus erythematosus: An updated meta-analysis. Lupus 2016, 25, 727–734. [Google Scholar] [CrossRef]
- Garcia, M.A.; Marcos, J.C.; Marcos, A.I.; Pons-Estel, B.A.; Wojdyla, D.; Arturi, A.; Babini, J.C.; Catoggio, L.J.; Alarcon-Segovia, D. Male systemic lupus erythematosus in a Latin-American inception cohort of 1214 patients. Lupus 2005, 14, 938–946. [Google Scholar] [CrossRef]
- Andrade, R.M.; Alarcón, G.S.; Fernández, M.; Apte, M.; Vilá, L.M.; Reveille, J.D.; LUMINA Study Group. Accelerated damage accrual among men with systemic lupus erythematosus: XLIV. Results from a multiethnic US cohort. Arthritis Rheum. 2007, 56, 622–630. [Google Scholar] [CrossRef]
- Stefanidou, S.; Benos, A.; Galanopoulou, V.; Chatziyannis, I.; Kanakoudi, F.; Aslanidis, S.; Boura, P.; Sfetsios, T.; Settas, L.; Katsounaros, M.; et al. Clinical expression and morbidity of systemic lupus erythematosus during a post-diagnostic 5-year follow-up: A male:female comparison. Lupus 2011, 20, 1090–1094. [Google Scholar] [CrossRef]
- Ramírez Gómez, L.A.; Uribe Uribe, O.; Osio Uribe, O.; Grisales Romero, H.; Cardiel, M.H.; Wojdyla, D.; Pons-Estel, B.A.; Grupo Latinoamericano de Estudio del Lupus (GLADEL); Catoggio, L.J.; Soriano, E.R.; et al. Childhood systemic lupus erythematosus in Latin America. The GLADEL experience in 230 children. Lupus 2008, 17, 596–604. [Google Scholar] [CrossRef]
- Hoffman, I.E.; Lauwerys, B.R.; De Keyser, F.; Huizinga, T.W.; Isenberg, D.; Cebecauer, L.; Dehoorne, J.; Joos, R.; Hendrickx, G.; Houssiau, F.; et al. Juvenile-onset systemic lupus erythematosus: Different clinical and serological pattern than adult-onset systemic lupus erythematosus. Ann. Rheum. Dis. 2009, 68, 412–415. [Google Scholar] [CrossRef]
- Tarr, T.; Dérfalvi, B.; Győri, N.; Szántó, A.; Siminszky, Z.; Malik, A.; Szabó, A.J.; Szegedi, G.; Zeher, M. Similarities and differences between pediatric and adult patients with systemic lupus erythematosus. Lupus 2015, 24, 796–803. [Google Scholar] [CrossRef]
- Gordon, C.; Jayne, D.; Pusey, C.; Adu, D.; Amoura, Z.; Aringer, M.; Ballerin, J.; Cervera, R.; Calvo-Alén, J.; Chizzolini, C.; et al. European consensus statement on the terminology used in the management of lupus glomerulonephritis. Lupus 2009, 18, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Bertsias, G.K.; Tektonidou, M.; Amoura, Z.; Aringer, M.; Bajema, I.; Berden, J.H.; Boletis, J.; Cervera, R.; Dörner, T.; Doria, A.; et al. Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann. Rheum. Dis. 2012, 71, 1771–1782. [Google Scholar] [CrossRef] [PubMed]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. International Society of Nephrology Working Group on the Classification of Lupus Nephritis; Renal Pathology Society Working Group on the Classification of Lupus Nephritis. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004, 65, 521–530. [Google Scholar] [CrossRef]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Lupus Nephritis Work Group Collaborators. KDIGO 2024 Clinical Practice Guideline for the management of Lupus Nephritis. Kidney Int. 2024, 105, S1–S69. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Andersen, J.; Aringer, M.; Arnaud, L.; Bae, S.C.; Boletis, J.; Bruce, I.N.; Cervera, R.; Doria, A.; et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann. Rheum. Dis. 2024, 83, 15–29. [Google Scholar] [CrossRef]
- Furie, R.; Rovin, B.H.; Houssiau, F.; Malvar, A.; Teng, Y.K.O.; Contreras, G.; Amoura, Z.; Yu, X.; Mok, C.C.; Santiago, M.B.; et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N. Engl. J. Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef]
- Tanaka, Y.; Nakayamada, S.; Yamaoka, K.; Ohmura, K.; Yasuda, S. Rituximab in the real-world treatment of lupus nephritis: A retrospective cohort study in Japan. Mod. Rheumatol. 2023, 33, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Teng, Y.K.O.; Ginzler, E.M.; Arriens, C.; Caster, D.J.; Romero-Diaz, J.; Gibson, K.; Kaplan, J.; Lisk, L.; Navarra, S.; et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): A double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2021, 397, 2070–2080. [Google Scholar] [CrossRef]
- Furie, R.A.; Aroca, G.; Cascino, M.D.; Garg, J.P.; Rovin, B.H.; Alvarez, A.; Fragoso-Loyo, H.; Zuta-Santillan, E.; Schindler, T.; Brunetta, P.; et al. B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: A randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2022, 81, 100–107. [Google Scholar] [CrossRef]
- Jayne, D.; Rovin, B.; Mysler, E.F.; Furie, R.A.; Houssiau, F.A.; Trasieva, T.; Knagenhjelm, J.; Schwetje, E.; Chia, Y.L.; Tummala, R.; et al. Phase II randomised trial of type I interferon inhibitor anifrolumab in patients with active lupus nephritis. Ann. Rheum. Dis. 2022, 81, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Morand, E.F.; Furie, R.; Tanaka, Y.; Bruce, I.N.; Askanase, A.D.; Richez, C.; Bae, S.C.; Brohawn, P.Z.; Pineda, L.; Berglind, A.; et al. TULIP-2 Trial Investigators. Trial of Anifrolumab in Active Systemic Lupus Erythematosus. N. Engl. J. Med. 2020, 382, 211–221. [Google Scholar] [CrossRef]
- van Vollenhoven, R.; Voskuyl, A.; Bertsias, G.; Aranow, C.; Aringer, M.; Arnaud, L.; Askanase, A.; Balážová, P.; Bonfa, E.; Bootsma, H.; et al. A framework for remission in SLE: Consensus findings from a large international task force on definitions of remission in SLE (DORIS). Ann. Rheum. Dis. 2017, 76, 554–561. [Google Scholar] [CrossRef]
- Golder, V.; Tsang-A-Sjoe, M.W.P. Treatment targets in SLE: Remission and low disease activity state. Rheumatology 2020, 59 (Suppl. S5), v19–v28. [Google Scholar] [CrossRef]
- Petri, M.; Magder, L.S. Comparison of Remission and Lupus Low Disease Activity State in Damage Prevention in a United States Systemic Lupus Erythematosus Cohort. Arthritis Rheumatol. 2018, 70, 1790–1795. [Google Scholar] [CrossRef]
- Ugarte-Gil, M.F.; Wojdyla, D.; Pons-Estel, G.J.; Catoggio, L.J.; Drenkard, C.; Sarano, J.; Berbotto, G.A.; Borba, E.F.; Sato, E.I.; Tavares Brenol, J.C.; et al. GLADEL. Remission and Low Disease Activity Status (LDAS) protect lupus patients from damage occurrence: Data from a multiethnic, multinational Latin American Lupus Cohort (GLADEL). Ann. Rheum. Dis. 2017, 76, 2071–2074. [Google Scholar] [CrossRef]
- Tarr, T.; Papp, G.; Nagy, N.; Cserép, E.; Zeher, M. Chronic high-dose glucocorticoid therapy triggers the development of chronic organ damage and worsens disease outcome in systemic lupus erythematosus. Clin. Rheumatol. 2017, 36, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Kwok, R.C.; Yip, P.S. Effect of renal disease on the standardized mortality ratio and life expectancy of patients with systemic lupus erythematosus. Arthritis Rheum. 2013, 65, 2154–2160. [Google Scholar] [CrossRef]
- Tan, E.M.; Cohen, A.S.; Fries, J.F.; Masi, A.T.; McShane, D.J.; Rothfield, N.F.; Schaller, J.G.; Talal, N.; Winchester, R.J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982, 25, 1271–1277. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Orbai, A.M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the systemic lupus interna-tional collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.A.; Gharavi, A.E.; Koike, T.; Lockshin, M.D.; Branch, D.W.; Piette, J.C.; Brey, R.; Derksen, R.; Harris, E.N.; Hughes, G.R.; et al. International consensus statement on preliminaryclassification criteria for definite an-tiphospholipid syndrome: Reportof an international workshop. Arthritis Rheum. 1999, 42, 1309–1311. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; DE Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Barbhaiya, M.; Zuily, S.; Naden, R.; Hendry, A.; Manneville, F.; Amigo, M.C.; Amoura, Z.; Andrade, D.; Andreoli, L.; Artim-Esen, B.; et al. ACR/EULAR APS Classification Criteria Collaborators. The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria. Arthritis Rheumatol. 2023, 75, 1687–1702. [Google Scholar] [CrossRef]
- Churg, J.; Sobin, L. Renal Disease: Classification and Atlas of Glomerular Disease; Igaku-Shoin: Tokyo, Japan, 1982. [Google Scholar]
- Cattran, D.C.; Feehally, J.; Cook, H.T.; Liu, Z.H.; Fervenza, F.C.; Mezzano, S.A.; Floege, J.; Nachman, P.H.; Gipson, D.S.; Praga, M.; et al. Kidney disease: Improving global outcomes (KDIGO) glomerulonephritis work group. KDIGO clinical practice guideline for glomerulonephritis. Kidney Int. Suppl. 2012, 2, 139–274. [Google Scholar]
- Gladman, D.; Ginzler, E.; Goldsmith, C.; Fortin, P.; Liang, M.; Urowitz, M.; Bacon, P.; Bombardieri, S.; Hanly, J.; Hay, E.; et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996, 39, 363–369. [Google Scholar] [CrossRef]
- Nikolopoulos, D.; Kostopoulou, M.; Pieta, A.; Karageorgas, T.; Tseronis, D.; Chavatza, K.; Flouda, S.; Rapsomaniki, P.; Banos, A.; Kremasmenou, E.; et al. Evolving phenotype of systemic lupus erythematosus in Caucasians: Low incidence of lupus nephritis, high burden of neuropsychiatric disease and increased rates of late-onset lupus in the ‘Attikon’ cohort. Lupus 2020, 29, 514–522. [Google Scholar] [CrossRef]
- Galindo-Izquierdo, M.; Rodriguez-Almaraz, E.; Pego-Reigosa, J.M.; López-Longo, F.J.; Calvo-Alén, J.; Olivé, A.; Fernández-Nebro, A.; Martinez-Taboada, V.; Vela-Casasempere, P.; Freire, M.; et al. Characterization of Patients with Lupus Nephritis Included in a Large Cohort From the Spanish Society of Rheumatology Registry of Patients with Systemic Lupus Erythematosus (RELESSER). Medicine 2016, 95, e2891. [Google Scholar] [CrossRef]
- Faezi, S.T.; Almodarresi, M.H.; Paragomi, P.; Gharibdoost, F.; Akhlaghi, M.; Jamshidi, A.; Shafaie, N.; Akbarian, M. Clinical picture of lupus nephritis in patients with systemic lupus erythematosus (SLE): Results of a large survey. Rheum. Res. 2017, 2, 51–59. [Google Scholar] [CrossRef]
- Mok, C.C.; Ho, L.Y.; Chan, K.L.; Tse, S.M.; To, C.H. Trend of Survival of a Cohort of Chinese Patients With Systemic Lupus Erythematosus over 25 Years. Front. Med. 2020, 7, 552. [Google Scholar] [CrossRef]
- Anaya, J.M.; Cañas, C.; Mantilla, R.D.; Pineda-Tamayo, R.; Tobón, G.J.; Herrera-Diaz, C.; Rendón, D.M.; Rojas-Villarraga, A.; Uribe, M. Lupus nephritis in Colombians: Contrasts and comparisons with other populations. Clin. Rev. Allergy Immunol. 2011, 40, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Dema, B.; Charles, N. Autoantibodies in SLE: Specificities, Isotypes and Receptors. Antibodies 2016, 5, 2. [Google Scholar] [CrossRef]
- Korbet, S.M.; Lewis, E.J.; Schwartz, M.M.; Reichlin, M.; Evans, J.; Rohde, R.D. Factors predictive of outcome in severe lupus nephritis. Lupus Nephritis Collaborative Study Group. Am. J. Kidney Dis. 2000, 35, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.; Masson, P.; Craig, J.C.; Flanc, R.S.; Roberts, M.A.; Strippoli, G.F.; Webster, A.C. Treatment for lupus nephritis. Cochrane Database Syst. Rev. 2012, 12, CD002922. [Google Scholar] [CrossRef]
- Hahn, B.H.; McMahon, M.A.; Wilkinson, A.; Wallace, W.D.; Daikh, D.I.; Fitzgerald, J.D.; Karpouzas, G.A.; Merrill, J.T.; Wallace, D.J.; Yazdany, J.; et al. American College of Rheumatology. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 2012, 64, 797–808. [Google Scholar] [CrossRef]
- Moroni, G.; Vercelloni, P.G.; Quaglini, S.; Gatto, M.; Gianfreda, D.; Sacchi, L.; Raffiotta, F.; Zen, M.; Costantini, G.; Urban, M.L.; et al. Changing patterns in clinical-histological presentation and renal outcome over the last five decades in a cohort of 499 patients with lupus nephritis. Ann. Rheum. Dis. 2018, 77, 1318–1325. [Google Scholar] [CrossRef]
- Doria, A.; Iaccarino, L.; Ghirardello, A.; Zampieri, S.; Arienti, S.; Sarzi-Puttini, P.; Atzeni, F.; Piccoli, A.; Todesco, S. Long-term prognosis and causes of death in systemic lupus erythematosus. Am. J. Med. 2006, 119, 700–706. [Google Scholar] [CrossRef]
- Luo, W.; Farinha, F.; Isenberg, D.A.; Rahman, A. Survival analysis of mortality and development of lupus nephritis in patients with systemic lupus erythematosus up to 40 years of follow-up. Rheumatology 2022, 62, 200–208. [Google Scholar] [CrossRef]
- Kandane-Rathnayake, R.; Golder, V.; Louthrenoo, W.; Chen, Y.H.; Cho, J.; Lateef, A.; Hamijoyo, L.; Luo, S.F.; Wu, Y.J.; Navarra, S.V.; et al. Asia-Pacific Lupus Collaboration. Lupus low disease activity state and remission and risk of mortality in patients with systemic lupus erythematosus: A prospective, multinational, longitudinal cohort study. Lancet Rheumatol. 2022, 4, e822–e830. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LN (n = 127) | Non-LN (n = 257) | p-Value | |
|---|---|---|---|
| Sex (female) | 114 (89.8) | 225 (87.5) | 0.525 |
| Age, years | 45.3 ± 11.6 | 53.5 ± 13.4 | <0.001 |
| Age onset SLE, years | 28.4 ± 9.9 | 35.7 ± 12.1 | <0.001 |
| Duration of disease, years | 16.9 ± 8.1 | 17.8 ± 8 | 0.319 |
| LN (n = 127) | Non-LN (n = 257) | p-Value | |
|---|---|---|---|
| Clinical manifestations | |||
| Mucocutan | |||
| Livedo reticularis | 11 (8.7) | 19 (7.4) | 0.663 |
| Acute skin lesions | 53 (41.7) | 93 (36.2) | 0.292 |
| DLE | 6 (4.7) | 47 (18.3) | <0.001 |
| SCLE | 7 (5.5) | 37 (14.4) | 0.010 |
| Alopecia | 38 (29.9) | 59 (23) | 0.140 |
| Photosensitivity | 29 (22.8) | 79 (30.7) | 0.105 |
| Mucous ulcer | 16 (12.6) | 20 (7.8) | 0.128 |
| Serositis | |||
| Pleuritis | 32 (25.2) | 63 (24.5) | 0.884 |
| Pericarditis | 25 (19.7) | 43 (16.7) | 0.476 |
| Neuropsychiatric | |||
| CNS manifestations | 25 (19.7) | 67 (26.1) | 0.168 |
| PNS manifestations | 10 (7.9) | 30 (11.7) | 0.252 |
| Psychiatric manifestations | 25 (19.7) | 45 (17.5) | 0.603 |
| Cardiovascular | |||
| APS | 21 (16.5) | 66 (25.7) | 0.044 |
| DVT | 17 (13.4) | 56 (21.8) | 0.048 |
| PE | 4 (3.1) | 11 (4.3) | 0.781 |
| AMI | 3 (2.4) | 3 (1.2) | 0.402 |
| Stroke | 8 (6.3) | 24 (9.3) | 0.311 |
| Obliterative arteriopathy | 1 (0.8) | 1 (0.4) | 0.553 |
| Valvulopathy | 25 (19.7) | 56 (21.8) | 0.634 |
| Others | |||
| Polyarthritis | 111 (87.4) | 209 (81.3) | 0.133 |
| Spontaneous abortion (n = 339) | 20 (17.5) | 36 (16) | 0.718 |
| Associated autoimmune diseases | |||
| RA | 13 (10.2) | 54 (21) | 0.009 |
| SS | 5 (3.9) | 29 (11.3) | 0.017 |
| PSS | 2 (1.6) | 0 (0) | 0.109 |
| SDI | 1 (0–2) | 1 (0–2) | 0.782 |
| Laboratory findings | |||
| Thrombocytopenia | 58 (45.7) | 92 (35.8) | 0.062 |
| Leukopaenia | 97 (76.4) | 175 (68.1) | 0.093 |
| Anaemia | 110 (86.6) | 172 (66.9) | <0.001 |
| Anti ß2-GP-1 | 67 (52.8) | 127 (49.4) | 0.538 |
| Anti-CL | 83 (65.4) | 152 (59.1) | 0.240 |
| LA | 23 (18.1) | 54 (21) | 0.504 |
| ANA | 113 (89) | 212 (82.5) | 0.097 |
| Anti-dsDNA | 120 (94.5) | 228 (88.7) | 0.068 |
| Anti-Sm | 52 (40.9) | 85 (33.1) | 0.130 |
| Anti-RNP | 46 (36.2) | 68 (26.5) | 0.049 |
| Anti-SS-A (Ro) | 77 (60.6) | 168 (65.4) | 0.363 |
| Anti-SS-B (La) | 51 (40.2) | 119 (46.3) | 0.254 |
| ANCA | 17 (13.4) | 25 (9.7) | 0.280 |
| Cryoglobulin | 7 (5.5) | 6 (2.3) | 0.134 |
| Coombs test positivity | 20 (15.7) | 25 (9.7) | 0.084 |
| LN (n = 127) | Non-LN (n = 257) | p-Value | |
|---|---|---|---|
| Corticosteroid | 127 (100) | 239 (93) | 0.002 |
| Corticosteroid (currently) | 81 (63.8) | 148 (57.6) | 0.245 |
| CD of corticosteroid, mg/kg | 16,060 (7300–32,120) | 15,330 (5840–29,200) | 0.255 |
| Chloroquine | 60 (47.2) | 161 (62.6) | 0.004 |
| Azathioprine | 96 (75.6) | 107 (41.6) | <0.001 |
| Mycophenolate mofetil | 52 (40.9) | 7 (2.7) | <0.001 |
| Cyclophosphamide | 103 (81.1) | 53 (20.6) | <0.001 |
| Methotrexate | 12 (9.4) | 60 (23.3) | 0.001 |
| Cyclosporin A | 13 (10.2) | 35 (13.6) | 0.346 |
| Plasmapheresis | 26 (20.5) | 35 (13.6) | 0.084 |
| Rituximab | 18 (14.2) | 9 (3.5) | <0.001 |
| LLDAS | 23 (18.1) | 43 (16.7) | 0.736 |
| Remission | 22 (17.3) | 54 (21) | 0.393 |
| LN (n = 18) | Non-LN (n = 27) | p-Value | |
|---|---|---|---|
| CV | 5 (27.8) | 8 (29.6) | 0.893 |
| Infection | 3 (16.7) | 9 (33.3) | 0.308 |
| Sepsis | 5 (27.8) | 1 (3.7) | 0.031 |
| Tumor | 3 (16.7) | 8 (29.6) | 0.482 |
| Other a | 2 (11.1) | 1 (3.7) | 0.562 |
| LN (n = 127) | Before 2005 (n = 44) | Since 2005 (n = 83) | p-Value | |
|---|---|---|---|---|
| Class I-II | 7 (5.5) | 4 (9.1) | 3 (3.6) | 0.234 |
| Class III | 13 (10.2) | 4 (9.1) | 9 (10.8) | 1.000 |
| Class IV | 74 (58.3) | 26 (59.1) | 48 (57.8) | 0.891 |
| Class V | 20 (15.7) | 7 (15.9) | 13 (15.7) | 0.971 |
| Mixed class | 11 (8.7) | 2 (4.5) | 9 (10.8) | 0.327 |
| Class I–II + Class III | 1 (9.1) | 1 (50) | 0 (0) | |
| Class I–II + Class IV | 1 (9.1) | 0 (0) | 1 (11.1) | |
| Class I–II + Class V | 1 (9.1) | 0 (0) | 1 (11.1) | |
| Class III + Class IV | 2 (18.2) | 1 (50) | 1 (11.1) | |
| Class III + Class V | 5 (45.5) | 0 (0) | 5 (55.6) | |
| Class IV + Class V | 1 (9.1) | 0 (0) | 1 (11.1) | |
| Not classified | 2 (1.6) | 1 (2.3) | 1 (1.2) | 1.000 |
| Before 2005 (n = 44) | Since 2005 (n = 83) | p-Value | |
|---|---|---|---|
| Clinical manifestations | |||
| Mucocutan | |||
| Livedo reticularis | 4 (9.1) | 7 (8.4) | 1.000 |
| Acute skin lesions | 21 (47.7) | 32 (38.6) | 0.319 |
| DLE | 5 (11.4) | 1 (1.2) | 0.019 |
| SCLE | 3 (6.8) | 4 (4.8) | 0.693 |
| Alopecia | 14 (31.8) | 24 (28.9) | 0.734 |
| Photosensitivity | 10 (22.7) | 19 (22.9) | 0.983 |
| Mucous ulcer | 4 (9.1) | 12 (14.5) | 0.386 |
| Serositis | |||
| Pleuritis | 17 (38.6) | 15 (18.1) | 0.011 |
| Pericarditis | 15 (34.1) | 10 (12) | 0.003 |
| Neuropsychiatric | |||
| CNS manifestations | 14 (31.8) | 11 (13.3) | 0.012 |
| PNS manifestations | 4 (9.1) | 6 (7.2) | 0.737 |
| Psychiatric manifestations | 13 (29.5) | 12 (14.5) | 0.042 |
| Cardiovascular | |||
| APS | 9 (20.5) | 12 (14.5) | 0.387 |
| DVT | 5 (11.4) | 12 (14.5) | 0.626 |
| PE | 1 (2.3) | 3 (3.6) | 1.000 |
| AMI | 2 (4.5) | 1 (1.2) | 0.275 |
| Stroke | 6 (13.6) | 2 (2.4) | 0.020 |
| Obliterative arteriopathy | 0 (0) | 1 (1.2) | 1.000 |
| Valvulopathy | 9 (20.5) | 16 (19.3) | 0.874 |
| Renal | |||
| CKD | 15 (34.1) | 20 (24.1) | 0.230 |
| ESRD | 6 (13.6) | 6 (7.2) | 0.339 |
| Others | |||
| Raynaud-syndrome | 21 (47.7) | 24 (28.9) | 0.035 |
| Polyarthritis | 41 (93.2) | 70 (84.3) | 0.153 |
| Spontaneous abortion (n = 114) | 7 (17.9) | 13 (17.3) | 0.935 |
| Associated autoimmune diseases | |||
| RA | 4 (9.1) | 9 (16.9) | 1.000 |
| SS | 0 (0) | 5 (6) | 0.163 |
| PSS | 0 (0) | 2 (2.4) | 0.544 |
| SDI | 1 (0–3) | 0 (0–1) | 0.001 |
| Treatments | |||
| Corticosteroid (currently) | 26 (59.1) | 55 (66.3) | 0.423 |
| CD of corticosteroid, mg/kg | 26,280 (18,250–42,340) | 11,680 (5840–24,090) | <0.001 |
| Chloroquine | 12 (27.3) | 48 (57.8) | 0.001 |
| Azathioprine | 36 (81.8) | 60 (72.3) | 0.234 |
| Maintenance Therapy | 33 (75) | 48 (57.8) | 0.055 |
| Mycophenolate mofetil | |||
| Induction Therapy | 5 (11.4) | 47 (56.6) | <0.001 |
| Maintenance Therapy | 2 (4.5) | 33 (39.8) | <0.001 |
| Cyclophosphamide | 40 (90.9) | 63 (75.9) | 0.040 |
| Methotrexate | 5 (11.4) | 7 (8.4) | 0.751 |
| Cyclosporin A | 6 (13.6) | 7 (8.4) | 0.751 |
| Plasmapheresis | 10 (22.7) | 16 (19.3) | 0.647 |
| Rituximab | 1 (2.3) | 17 (20.5) | 0.005 |
| Belimumab | 2 (4.5) | 6 (7.2) | 0.713 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perge, B.; Papp, G.; Bói, B.; Nagy, N.; Gáspár-Kiss, E.; Tarr, T. Clinical Features and Survival Analysis of Lupus Nephritis among Patients with Systemic Lupus Erythematosus: A Three-Decade-Long Retrospective Cohort Study. Biomedicines 2024, 12, 2117. https://doi.org/10.3390/biomedicines12092117
Perge B, Papp G, Bói B, Nagy N, Gáspár-Kiss E, Tarr T. Clinical Features and Survival Analysis of Lupus Nephritis among Patients with Systemic Lupus Erythematosus: A Three-Decade-Long Retrospective Cohort Study. Biomedicines. 2024; 12(9):2117. https://doi.org/10.3390/biomedicines12092117
Chicago/Turabian StylePerge, Bianka, Gábor Papp, Bernadett Bói, Nikolett Nagy, Eszter Gáspár-Kiss, and Tünde Tarr. 2024. "Clinical Features and Survival Analysis of Lupus Nephritis among Patients with Systemic Lupus Erythematosus: A Three-Decade-Long Retrospective Cohort Study" Biomedicines 12, no. 9: 2117. https://doi.org/10.3390/biomedicines12092117
APA StylePerge, B., Papp, G., Bói, B., Nagy, N., Gáspár-Kiss, E., & Tarr, T. (2024). Clinical Features and Survival Analysis of Lupus Nephritis among Patients with Systemic Lupus Erythematosus: A Three-Decade-Long Retrospective Cohort Study. Biomedicines, 12(9), 2117. https://doi.org/10.3390/biomedicines12092117