

Comparison of Intact Fish Skin Graft and Allograft as Temporary Coverage for Full-Thickness Burns: A Non-Inferiority Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Allograft Preparation
2.3. Anesthesia
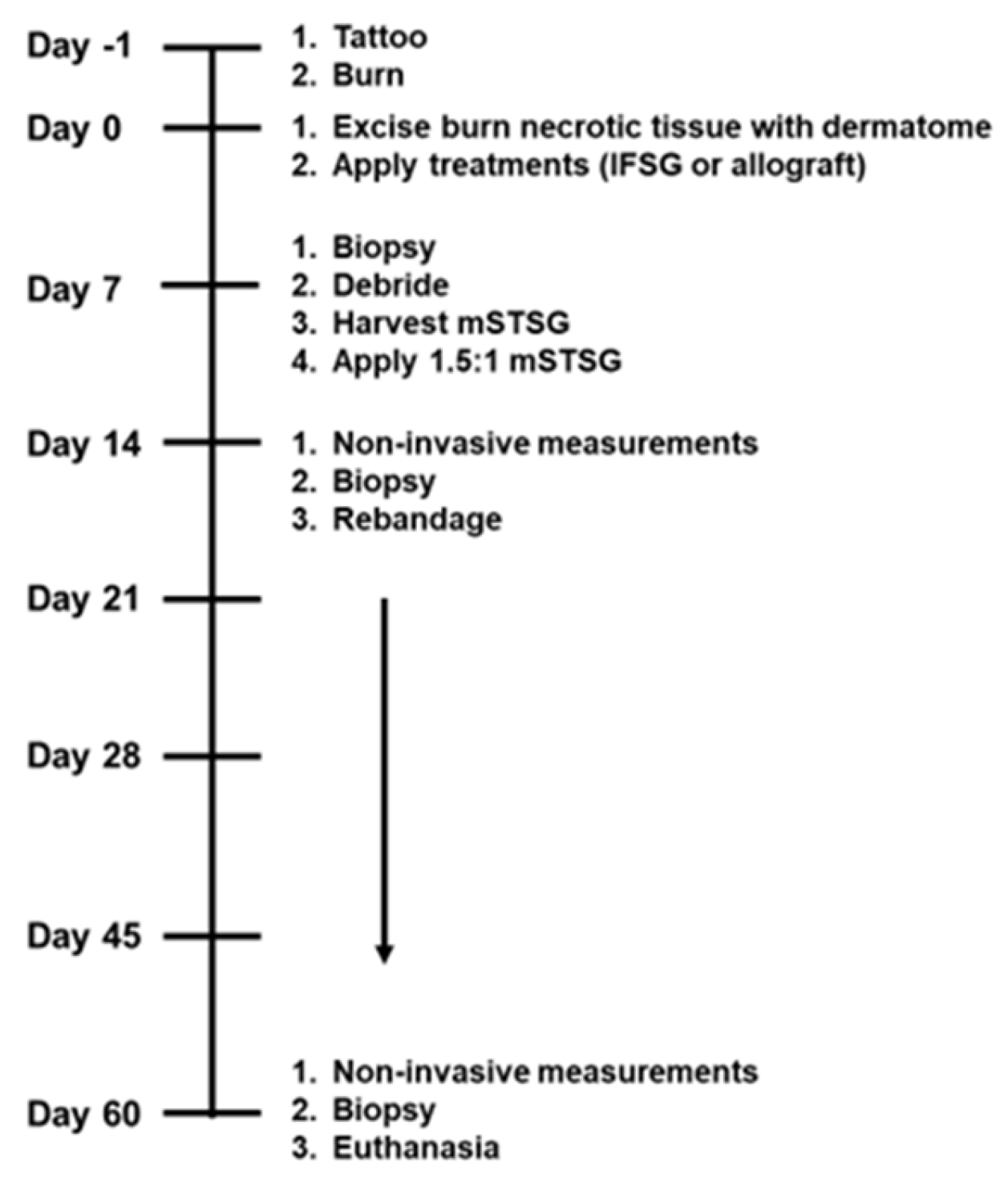
2.4. Porcine Burn Wounds
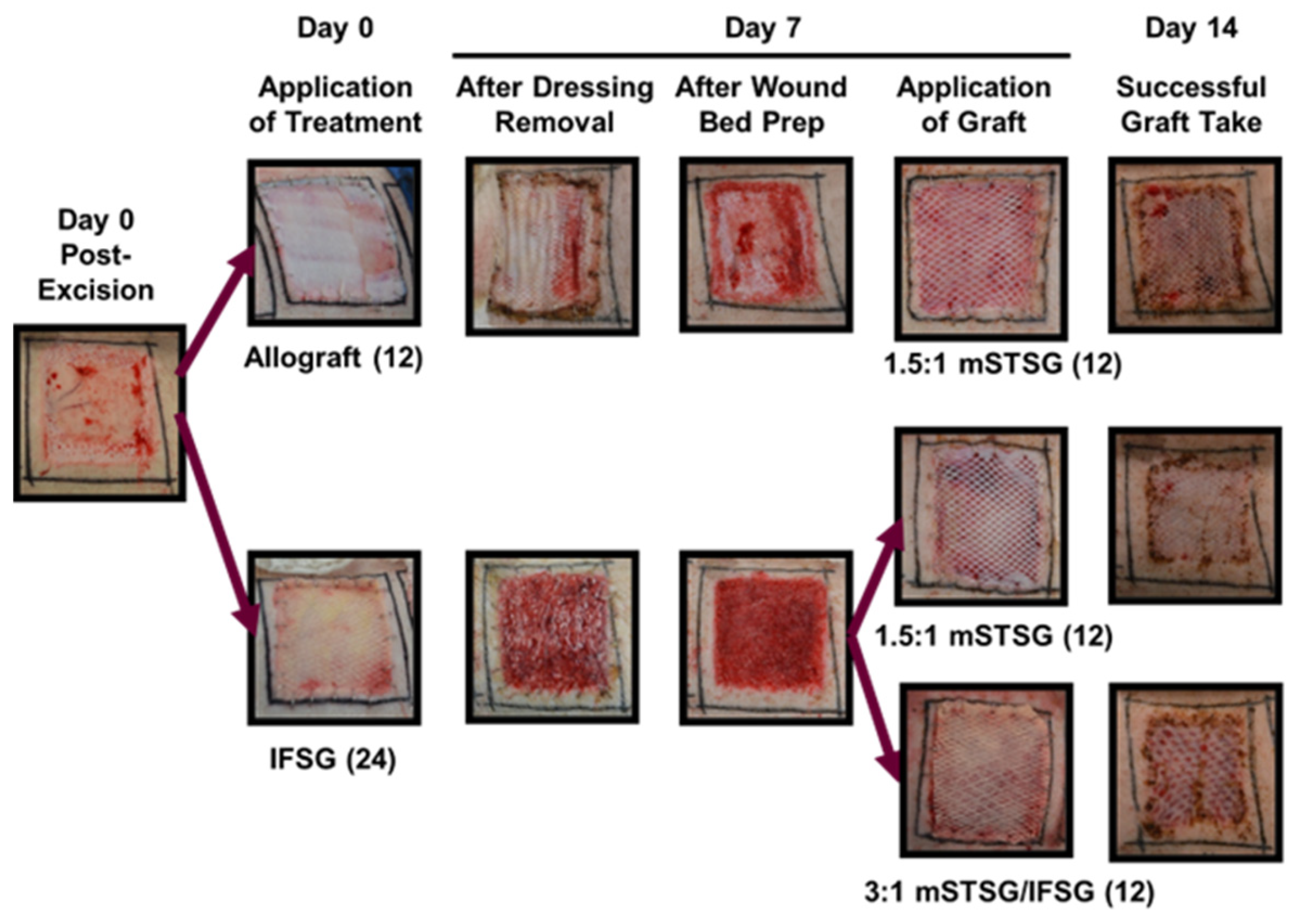
2.5. Surgical Debridement and Temporary Coverage Treatment
2.6. Autograft Harvesting and Application
2.7. Wound Care
2.8. Contraction Calculations
2.9. Skin Function Measurements
2.10. Laser Speckle
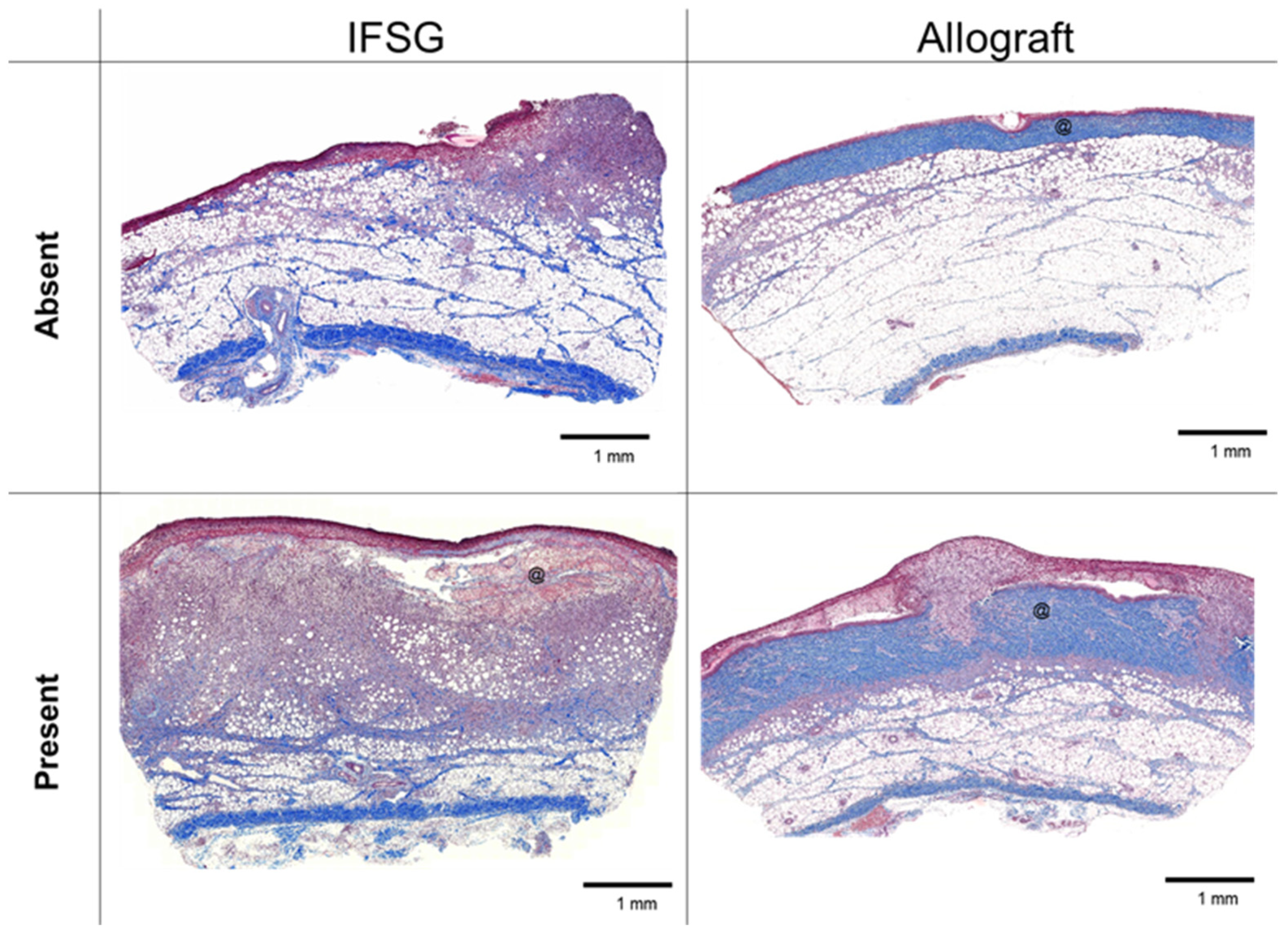
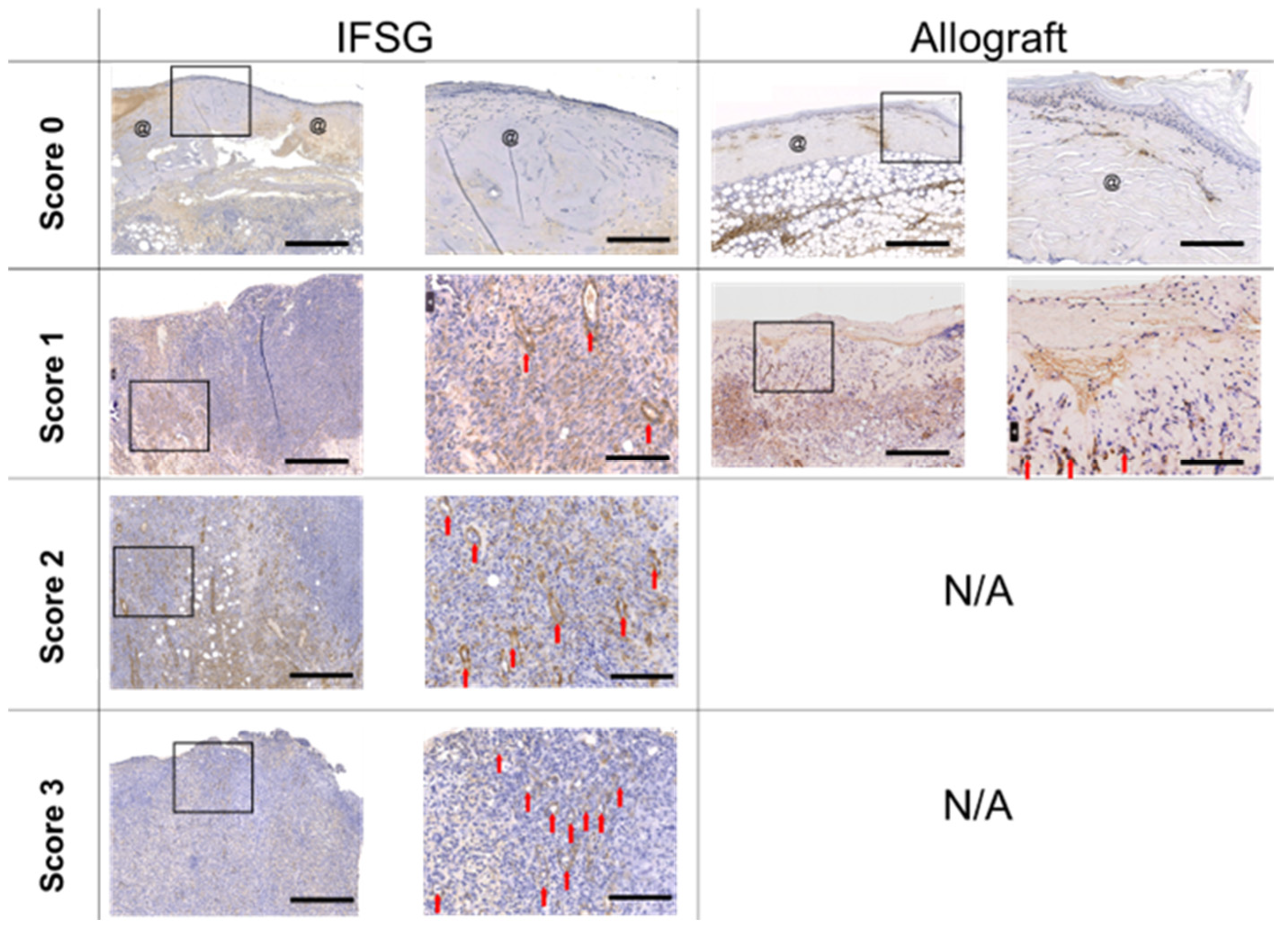
2.11. Histology and Pathological Analysis
2.12. Statistical Analysis
3. Results
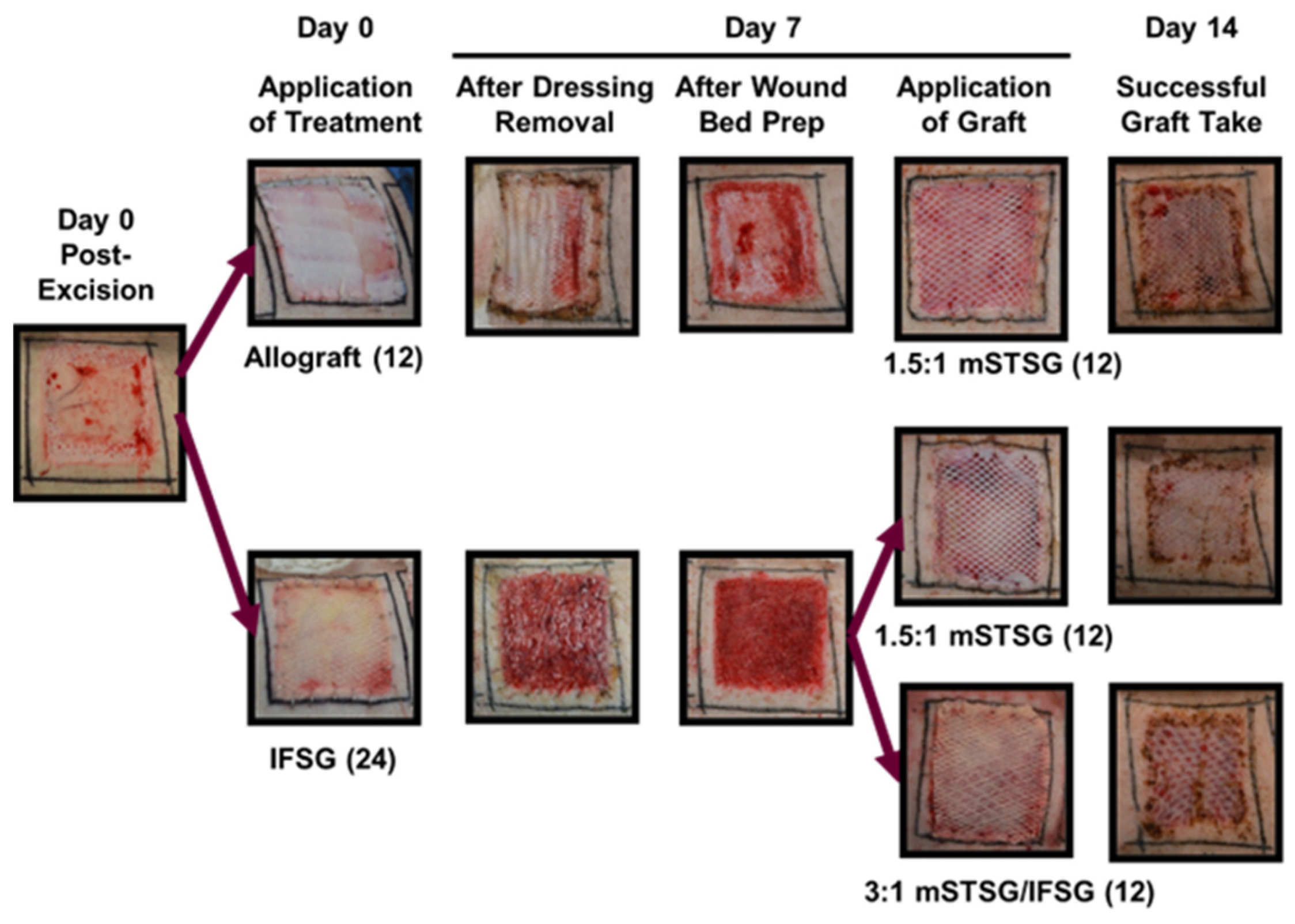
3.1. Porcine Burn Wound Model
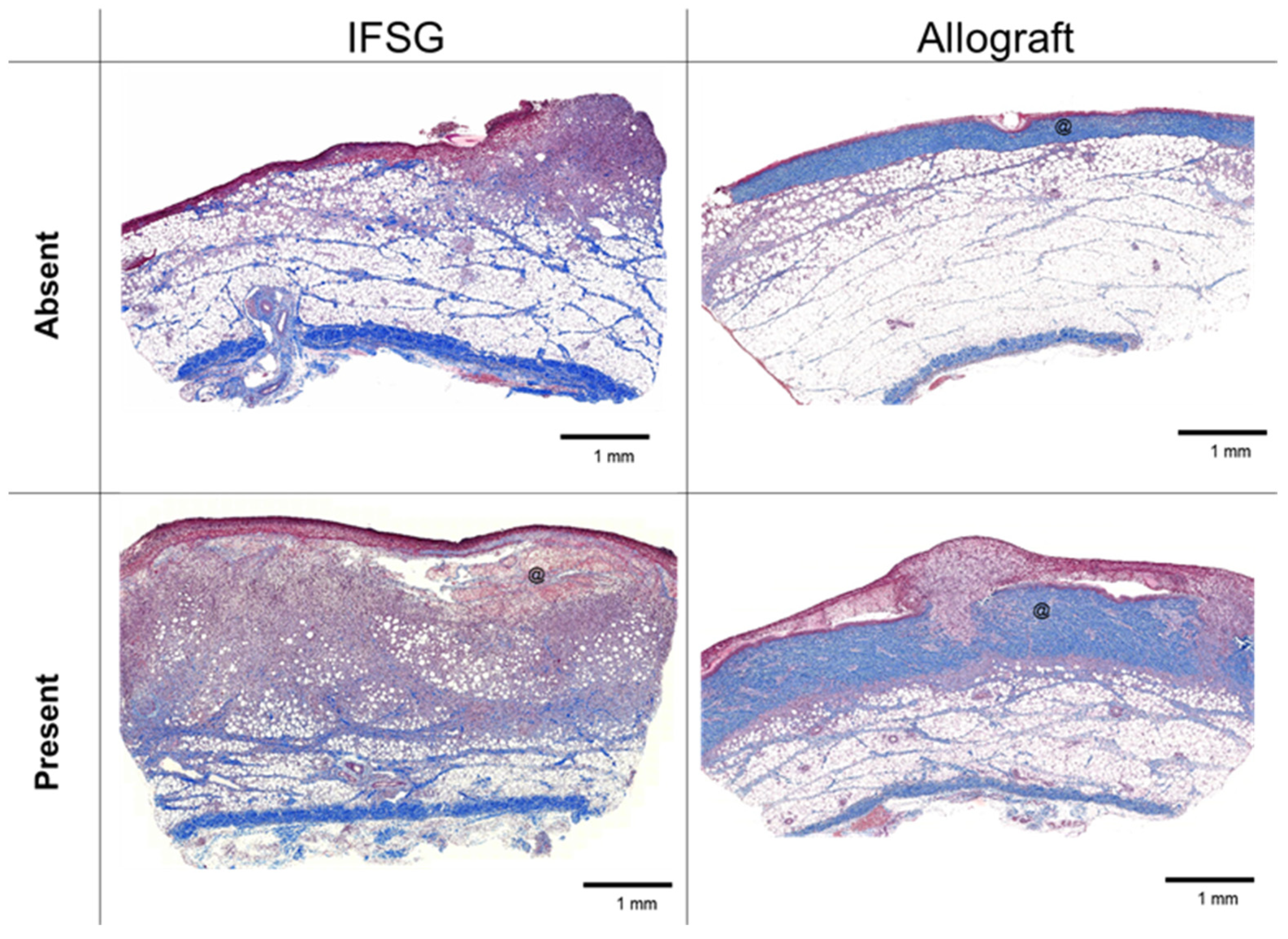
3.2. Histological Analysis of Wound Bed after 7 Days of Temporary Coverage of IFSG or Allograft
3.3. FSG Stimulated a Granulated Wound Bed
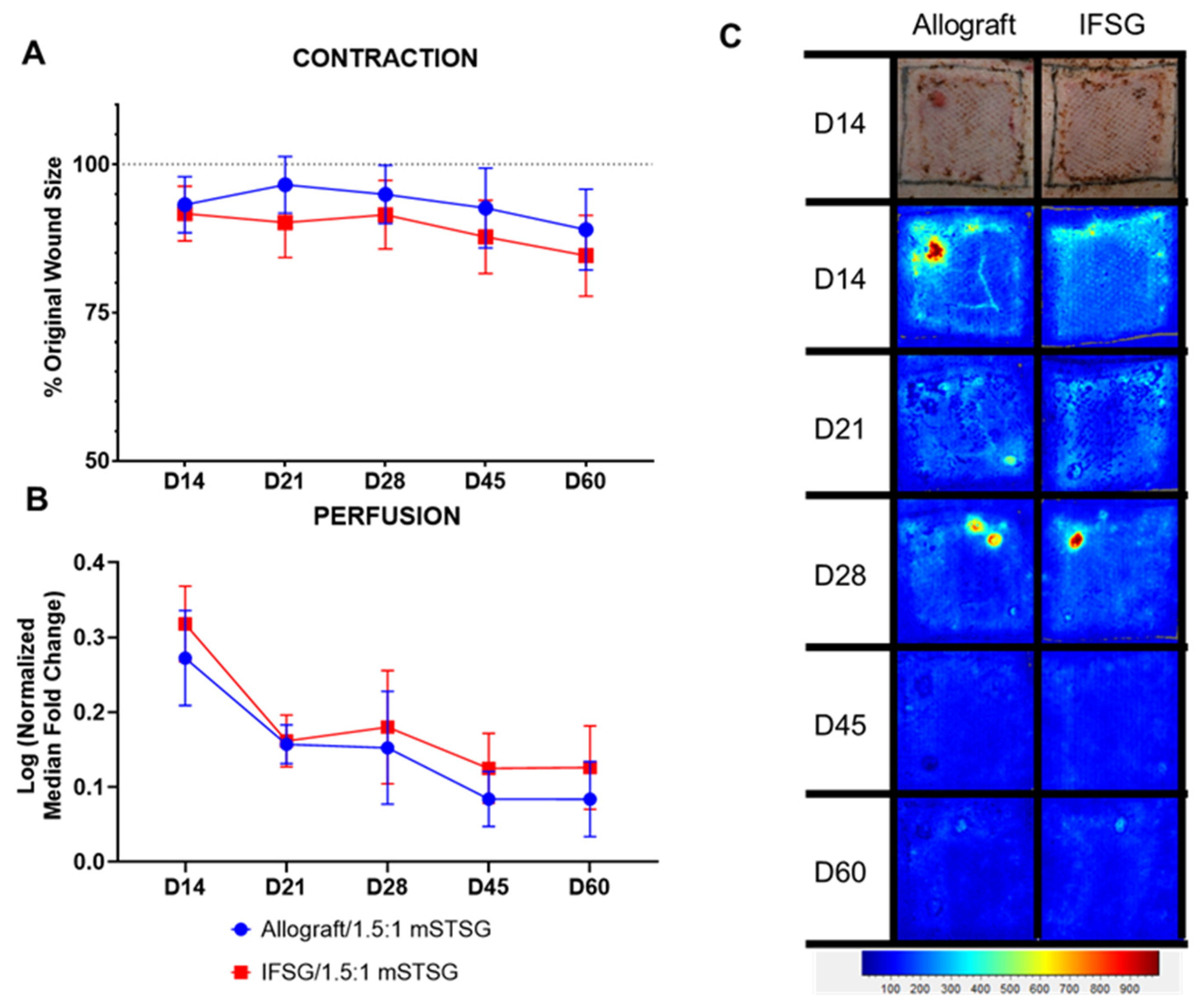
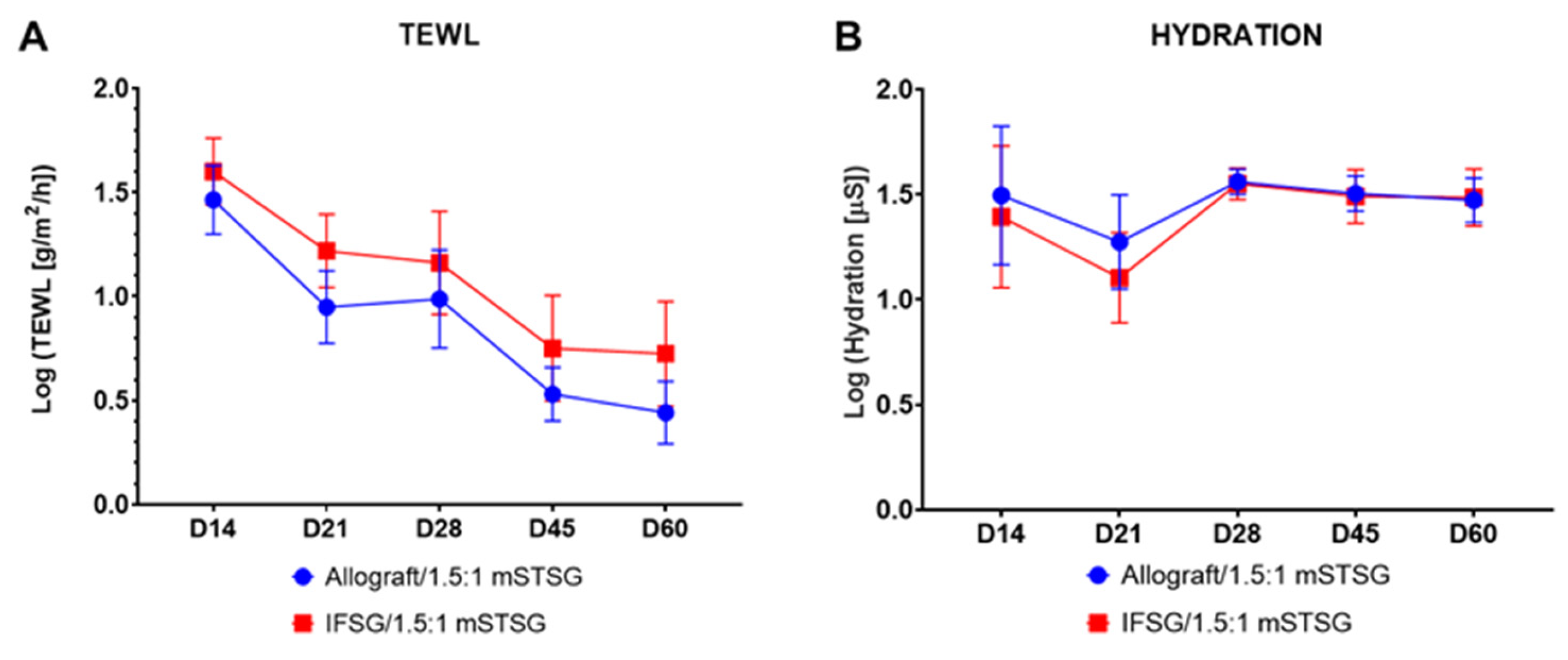
3.4. Wounds Treated with IFSG Showed No Differences in Contraction, Perfusion, TEWL, or Hydration Compared to Allograft after Grafting
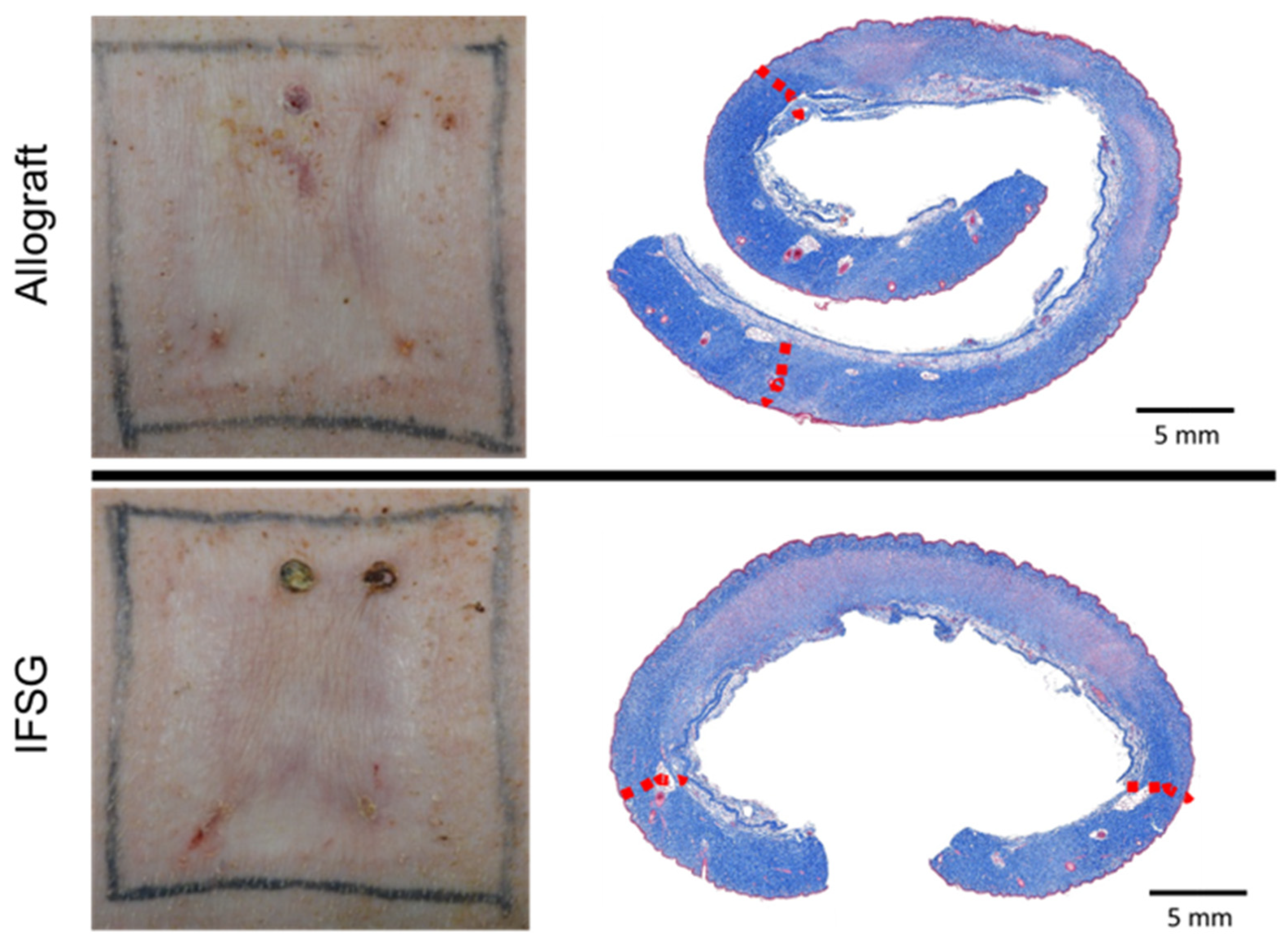
3.5. Histological Analysis after Grafting

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathologist Scoring Rubric | Allograft/1.5:1 mSTSG (N = 12) | IFSG/1.5:1 mSTSG (N = 10) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Epidermal Status | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = No epidermis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1 = Partial epidermis | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 2 = Regenerating or hyperplastic with 100% coverage | 10 | 4 | 0 | 1 | 0 | 6 | 3 | 1 | 0 | 1 |
| 3 = Normal epidermis across entire wound bed | 2 | 8 | 12 | 11 | 12 | 3 | 7 | 9 | 10 | 9 |
| p value | 0.801 | >0.999 | 0.455 | >0.999 | 0.455 | |||||
| Fibroplasia | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1 = Minimal | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2 = Mild | 6 | 5 | 7 | 9 | 5 | 2 | 2 | 5 | 7 | 3 |
| 3 = Moderate | 6 | 6 | 4 | 3 | 7 | 8 | 7 | 4 | 3 | 6 |
| 4 = Marked | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| p value | 0.204 | 0.126 | 0.348 | >0.999 | 0.526 | |||||
| Foreign Material | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = Absent | 7 | 12 | 12 | 12 | 12 | 9 | 10 | 10 | 10 | 10 |
| 1 = Present | 5 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| p value | 0.162 | >0.999 | >0.999 | >0.999 | >0.999 | |||||
| Angiogenesis | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 8 | 9 | 10 | 12 | 12 | 4 | 7 | 8 | 9 | 10 |
| 1 = ≤ 50 Vessels | 4 | 3 | 2 | 0 | 0 | 6 | 3 | 2 | 1 | 0 |
| p value | 0.391 | >0.999 | >0.999 | 0.455 | >0.999 | |||||
| Hemorrhage | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = Absent | 8 | 8 | 9 | 10 | 8 | 7 | 5 | 8 | 7 | 6 |
| 1 = Present | 4 | 4 | 3 | 2 | 4 | 3 | 5 | 2 | 3 | 4 |
| p value | >0.999 | 0.666 | >0.999 | 0.624 | >0.999 | |||||
| Hemorrhage Severity | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = Absent | 8 | 8 | 9 | 10 | 8 | 7 | 5 | 8 | 7 | 6 |
| 1 = Mild | 4 | 4 | 3 | 2 | 3 | 3 | 5 | 2 | 3 | 4 |
| 2 = Moderate | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| p value | >0.999 | 0.666 | >0.999 | 0.624 | >0.999 | |||||
| Neutrophils | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 10 | 11 | 12 | 12 | 12 | 7 | 10 | 9 | 10 | 10 |
| 1 = Minimal number of ICs | 2 | 1 | 0 | 0 | 0 | 3 | 0 | 1 | 0 | 0 |
| 2 = Mild number of ICs | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| p value | 0.624 | >0.999 | 0.455 | >0.999 | >0.999 | |||||
| Eosinophils | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 8 | 11 | 10 | 12 | 12 | 6 | 8 | 10 | 10 | 9 |
| 1 = Minimal number of ICs | 4 | 1 | 2 | 0 | 0 | 2 | 2 | 0 | 0 | 1 |
| 2 = Mild number of ICs | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 |
| p value | 0.554 | 0.571 | 0.481 | >0.999 | 0.455 | |||||
| Lymphocytes | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 7 | 8 | 7 | 11 | 8 | 4 | 3 | 8 | 8 | 5 |
| 1 = Minimal number of ICs | 4 | 3 | 4 | 1 | 3 | 5 | 6 | 1 | 2 | 3 |
| 2 = Mild number of ICs | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 2 |
| p value | 0.481 | 0.148 | 0.448 | 0.571 | 0.513 | |||||
| Macrophages | D14 | D21 | D28 | D45 | D60 | D14 | D21 | D28 | D45 | D60 |
| 0 = None | 7 | 10 | 8 | 9 | 7 | 5 | 9 | 8 | 8 | 5 |
| 1 = Minimal number of ICs | 4 | 2 | 4 | 3 | 5 | 5 | 1 | 2 | 2 | 4 |
| 2 = Mild number of ICs | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| p value | >0.999 | >0.999 | 0.646 | >0.999 | 0.726 | |||||
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ABA. Burn Incidence and Treatment in the United States: 2016 Fact Sheet; American Burn Association: Chicago, IL, USA, 2016; Available online: http://www.ameriburn.org/resources_factsheet.php (accessed on 15 October 2020).
- Stone, R., II; Natesan, S.; Kowalczewski, C.J.; Mangum, L.H.; Clay, N.E.; Clohessy, R.M.; Carlsson, A.H.; Tassin, D.H.; Chan, R.K.; Rizzo, J.A.; et al. Advancements in Regenerative Strategies through the Continuum of Burn Care. Front. Pharmacol. 2018, 9, 672. [Google Scholar] [CrossRef]
- Magnusson, S.; Baldursson, B.T.; Kjartansson, H.; Rolfsson, O.; Sigurjonsson, G.F. Regenerative and Antibacterial Properties of Acellular Fish Skin Grafts and Human Amnion/Chorion Membrane: Implications for Tissue Preservation in Combat Casualty Care. Mil. Med. 2017, 182, 383–388. [Google Scholar] [CrossRef]
- Winters, C.; Kirsner, R.S.; Margolis, D.J.; Lantis, J.C. Cost Effectiveness of Fish Skin Grafts versus Standard of Care on Wound Healing of Chronic Diabetic Foot Ulcers: A Retrospective Comparative Cohort Study. Wounds 2020, 32, 283–290. [Google Scholar]
- Zehnder, T.; Blatti, M. Faster than Projected Healing in Chronic Venous and Diabetic Foot Ulcers When Treated with Intact Fish Skin Grafts Compared to Expected Healing Times for Standard of Care: An Outcome-Based Model from a Swiss Hospital. Int. J. Low. Extrem. Wounds 2022, 15347346221096205. [Google Scholar] [CrossRef]
- Alam, K.; Jeffery, S.L.A. Acellular Fish Skin Grafts for Management of Split Thickness Donor Sites and Partial Thickness Burns: A Case Series. Mil. Med. 2019, 184, 16–20. [Google Scholar] [CrossRef]
- Kirsner, R.S.; Margolis, D.J.; Baldursson, B.T.; Petursdottir, K.; Davidsson, O.B.; Weir, D.; Lantis, J.C., 2nd. Fish skin grafts compared to human amnion/chorion membrane allografts: A double-blind, prospective, randomized clinical trial of acute wound healing. Wound Repair Regen. 2020, 28, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Lullove, E.J.; Liden, B.; Winters, C.; McEneaney, P.; Raphael, A.; Lantis, J.C., II. A Multicenter, Blinded, Randomized Controlled Clinical Trial Evaluating the Effect of Omega-3-Rich Fish Skin in the Treatment of Chronic, Nonresponsive Diabetic Foot Ulcers. Wounds 2021, 33, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Luze, H.; Nischwitz, S.P.; Smolle, C.; Zrim, R.; Kamolz, L.P. The Use of Acellular Fish Skin Grafts in Burn Wound Management-A Systematic Review. Medicina 2022, 58, 912. [Google Scholar] [CrossRef] [PubMed]
- Michael, S.; Winters, C.; Khan, M. Acellular Fish Skin Graft Use for Diabetic Lower Extremity Wound Healing: A Retrospective Study of 58 Ulcerations and a Literature Review. Wounds 2019, 31, 262–268. [Google Scholar]
- Seth, N.; Chopra, D.; Lev-Tov, H. Fish Skin Grafts with Omega-3 for Treatment of Chronic Wounds: Exploring the Role of Omega-3 Fatty Acids in Wound Healing and a Review of Clinical Healing Outcomes. Surg. Technol. Int. 2022, 40, 38–46. [Google Scholar] [CrossRef]
- Woodrow, T.; Chant, T.; Chant, H. Treatment of diabetic foot wounds with acellular fish skin graft rich in Omega-3: A prospective evaluation. J. Wound Care 2019, 28, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.K.; Polanco, T.O.; Lantis, J.C., 2nd. A Prospective, Postmarket, Compassionate Clinical Evaluation of a Novel Acellular Fish-skin Graft Which Contains Omega-3 Fatty Acids for the Closure of Hard-to-heal Lower Extremity Chronic Ulcers. Wounds 2016, 28, 112–118. [Google Scholar] [PubMed]
- Stone, R., 2nd; Saathoff, E.C.; Larson, D.A.; Wall, J.T.; Wienandt, N.A.; Magnusson, S.; Kjartansson, H.; Natesan, S.; Christy, R.J. Accelerated Wound Closure of Deep Partial Thickness Burns with Acellular Fish Skin Graft. Int. J. Mol. Sci. 2021, 22, 1590. [Google Scholar] [CrossRef] [PubMed]
- Kearney, J.N. Guidelines on processing and clinical use of skin allografts. Clin. Dermatol. 2005, 23, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.; Burd, A. “Xenograft” dressing in the treatment of burns. Clin. Dermatol. 2005, 23, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.; Jockheck-Clark, A.R.; Natesan, S.; Rizzo, J.A.; Wienandt, N.A.; Scott, L.L.; Larson, D.A.; Wall, J.T.; Holik, M.A.; Shaffer, L.J.; et al. Enzymatic Debridement of Porcine Burn Wounds via a Novel Protease, SN514. J. Burn Care Res. 2020, 41, 1015–1028. [Google Scholar] [CrossRef] [PubMed]
- White, C.E.; Renz, E.M. Advances in surgical care: Management of severe burn injury. Crit. Care Med. 2008, 36, S318–S324. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Blackbourne, L.H.; Wolf, S.E.; White, C.E.; Renz, E.M.; Cancio, L.C.; Holcomb, J.B.; Barillo, D.J. Evolution of burn resuscitation in operation Iraqi freedom. J. Burn Care Res. 2006, 27, 606–611. [Google Scholar] [CrossRef]
- Wolf, S.E.; Kauvar, D.S.; Wade, C.E.; Cancio, L.C.; Renz, E.P.; Horvath, E.E.; White, C.E.; Park, M.S.; Wanek, S.; Albrecht, M.A.; et al. Comparison between civilian burns and combat burns from Operation Iraqi Freedom and Operation Enduring Freedom. Ann. Surg. 2006, 243, 786–792; discussion 792–795. [Google Scholar] [CrossRef]
- Owens, B.D.; Kragh, J.F., Jr.; Wenke, J.C.; Macaitis, J.; Wade, C.E.; Holcomb, J.B. Combat wounds in operation Iraqi Freedom and operation Enduring Freedom. J. Trauma 2008, 64, 295–299. [Google Scholar] [CrossRef]
- Cancio, L.C.; Barillo, D.J.; Kearns, R.D.; Holmes, J.H.t.; Conlon, K.M.; Matherly, A.F.; Cairns, B.A.; Hickerson, W.L.; Palmieri, T. Guidelines for Burn Care under Austere Conditions: Surgical and Nonsurgical Wound Management. J. Burn Care Res. 2017, 38, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Blackstone, B.N.; Kim, J.Y.; McFarland, K.L.; Sen, C.K.; Supp, D.M.; Bailey, J.K.; Powell, H.M. Scar formation following excisional and burn injuries in a red Duroc pig model. Wound Repair Regen. 2017, 25, 618–631. [Google Scholar] [CrossRef] [PubMed]
- Harunari, N.; Zhu, K.Q.; Armendariz, R.T.; Deubner, H.; Muangman, P.; Carrougher, G.J.; Isik, F.F.; Gibran, N.S.; Engrav, L.H. Histology of the thick scar on the female, red Duroc pig: Final similarities to human hypertrophic scar. Burns 2006, 32, 669–677. [Google Scholar] [CrossRef] [PubMed]





| DAY 7 ANALYSIS | Allograft (N =12) | IFSG (N = 24) | p Value | |||
|---|---|---|---|---|---|---|
| Parameter | Pathologist Scoring Rubric | N | % | N | % | |
| Angiogenesis | 0—None | 6 | 50 | 3 | 12.5 | <0.0001 * |
| 1—≤50 Vessels | 6 | 50 | 3 | 12.5 | ||
| 2—51–100 Vessels | 0 | 0 | 12 | 50 | ||
| 3—101–150 Vessels | 0 | 0 | 6 | 25 | ||
| Foreign Material | 0—Absent | 6 | 50 | 5 | 20.8 | 0.1245 |
| 1—Present | 6 | 50 | 19 | 79.2 | ||
| Hemorrhage | 0—Absent | 6 | 50 | 4 | 16.7 | 0.0532 |
| 1—Present | 6 | 50 | 20 | 83.3 | ||
| Hemorrhage Severity | 0—Absent | 6 | 50 | 4 | 16.7 | 0.2493 |
| 1—Mild | 2 | 16.7 | 12 | 50 | ||
| 2—Moderate | 4 | 33.3 | 7 | 29.2 | ||
| 3—Severe | 0 | 0 | 1 | 4.2 | ||
| Granulation Tissue | 0—Absent | 10 | 83.3 | 4 | 16.7 | 0.0002 * |
| 1—Present | 2 | 16.7 | 20 | 83.3 | ||
| Fibroplasia | 0—None | 1 | 8.3 | 0 | 0 | 0.0006 * |
| 1—Minimal | 2 | 16.7 | 1 | 4.2 | ||
| 2—Mild | 6 | 50 | 4 | 16.7 | ||
| 3—Moderate | 3 | 25 | 11 | 45.7 | ||
| 4—Marked | 0 | 0 | 7 | 29.2 | ||
| 5—Severe | 0 | 0 | 1 | 4.2 | ||
| Neutrophils | 0—None | 4 | 33.3 | 0 | 0 | <0.0001 * |
| 1—Minimal number of ICs | 7 | 58.3 | 2 | 8.3 | ||
| 2—Mild number of ICs | 0 | 0 | 13 | 54.2 | ||
| 3—Moderate number of ICs | 0 | 0 | 2 | 8.3 | ||
| 4—Marked number of ICs | 0 | 0 | 3 | 12.5 | ||
| 5—Severe number of ICs | 1 | 8.4 | 4 | 16.7 | ||
| Eosinophils | 0—None | 7 | 58.3 | 1 | 4.2 | <0.0001 |
| 1—Minimal number of ICs | 4 | 33.3 | 2 | 8.3 | ||
| 2—Mild number of ICs | 1 | 8.3 | 12 | 50 | ||
| 3—Moderate number of ICs | 0 | 0 | 9 | 37.5 | ||
| Lymphocytes | 0—None | 4 | 33.3 | 1 | 4.2 | <0.0001 * |
| 1—Minimal number of ICs | 5 | 41.7 | 0 | 0 | ||
| 2—Mild number of ICs | 3 | 25 | 17 | 70.8 | ||
| 3—Moderate number of ICs | 0 | 0 | 6 | 25 | ||
| Macrophages | 0—None | 6 | 50 | 1 | 4.2 | 0.0048 * |
| 1—Minimal number of ICs | 5 | 41.7 | 16 | 66.7 | ||
| 2—Mild number of ICs | 1 | 8.3 | 7 | 29.2 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stone, R., II; Saathoff, E.C.; Larson, D.A.; Wall, J.T.; Wienandt, N.A.; Magnusson, S.; Kjartansson, H.; Christy, R.J.; Natesan, S. Comparison of Intact Fish Skin Graft and Allograft as Temporary Coverage for Full-Thickness Burns: A Non-Inferiority Study. Biomedicines 2024, 12, 680. https://doi.org/10.3390/biomedicines12030680
Stone R II, Saathoff EC, Larson DA, Wall JT, Wienandt NA, Magnusson S, Kjartansson H, Christy RJ, Natesan S. Comparison of Intact Fish Skin Graft and Allograft as Temporary Coverage for Full-Thickness Burns: A Non-Inferiority Study. Biomedicines. 2024; 12(3):680. https://doi.org/10.3390/biomedicines12030680
Chicago/Turabian StyleStone, Randolph, II, Emily C. Saathoff, David A. Larson, John T. Wall, Nathan A. Wienandt, Skuli Magnusson, Hilmar Kjartansson, Robert J. Christy, and Shanmugasundaram Natesan. 2024. "Comparison of Intact Fish Skin Graft and Allograft as Temporary Coverage for Full-Thickness Burns: A Non-Inferiority Study" Biomedicines 12, no. 3: 680. https://doi.org/10.3390/biomedicines12030680
APA StyleStone, R., II, Saathoff, E. C., Larson, D. A., Wall, J. T., Wienandt, N. A., Magnusson, S., Kjartansson, H., Christy, R. J., & Natesan, S. (2024). Comparison of Intact Fish Skin Graft and Allograft as Temporary Coverage for Full-Thickness Burns: A Non-Inferiority Study. Biomedicines, 12(3), 680. https://doi.org/10.3390/biomedicines12030680