
Influence of NUCB/Nesfatin-1 Polymorphism on Treatment Response to Naltrexone/Bupropion SR in Binge Eating Disorder and Obesity

 ,
,  ,
,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures and Assessment
2.3. General and Eating Psychopathological Measures
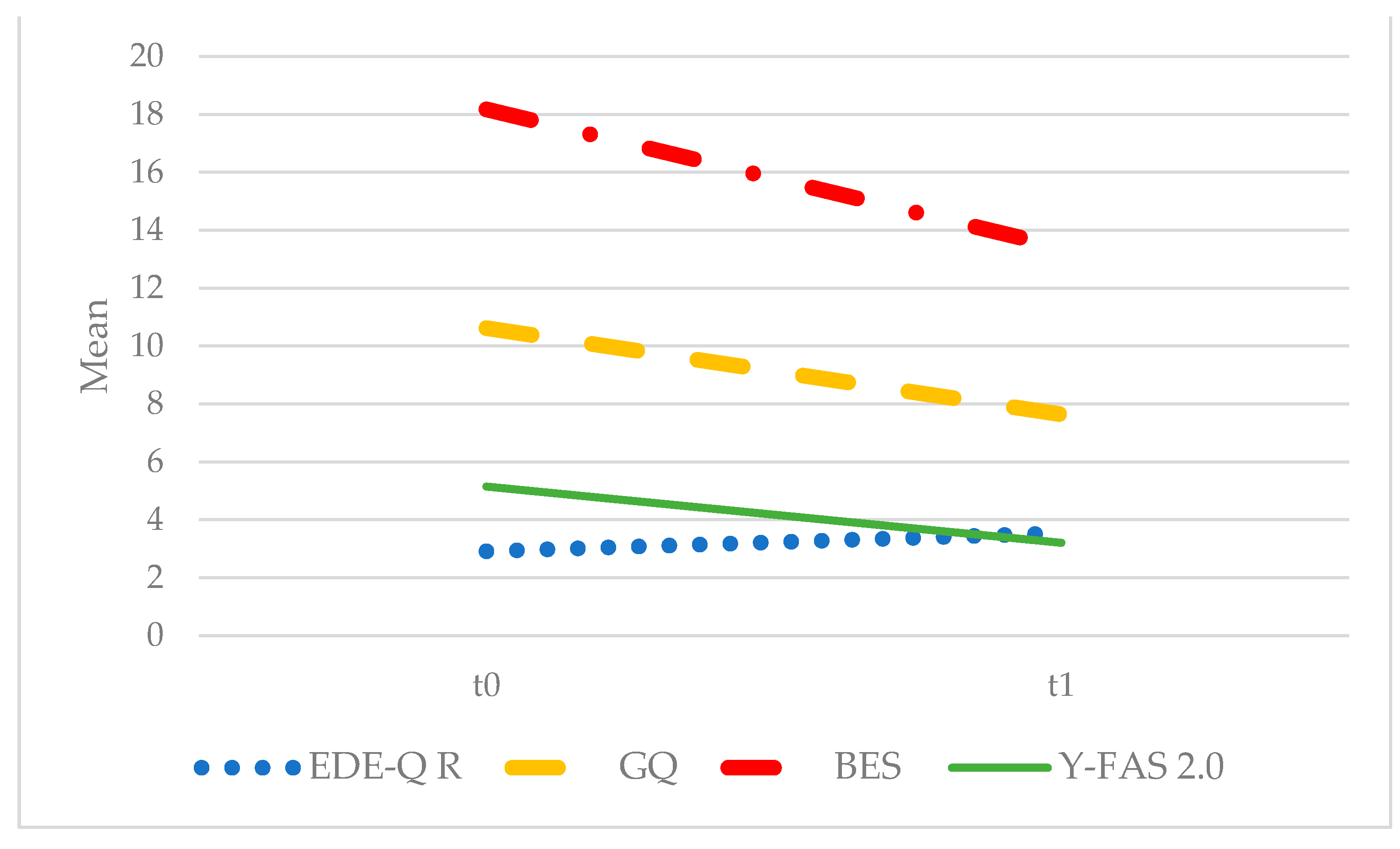
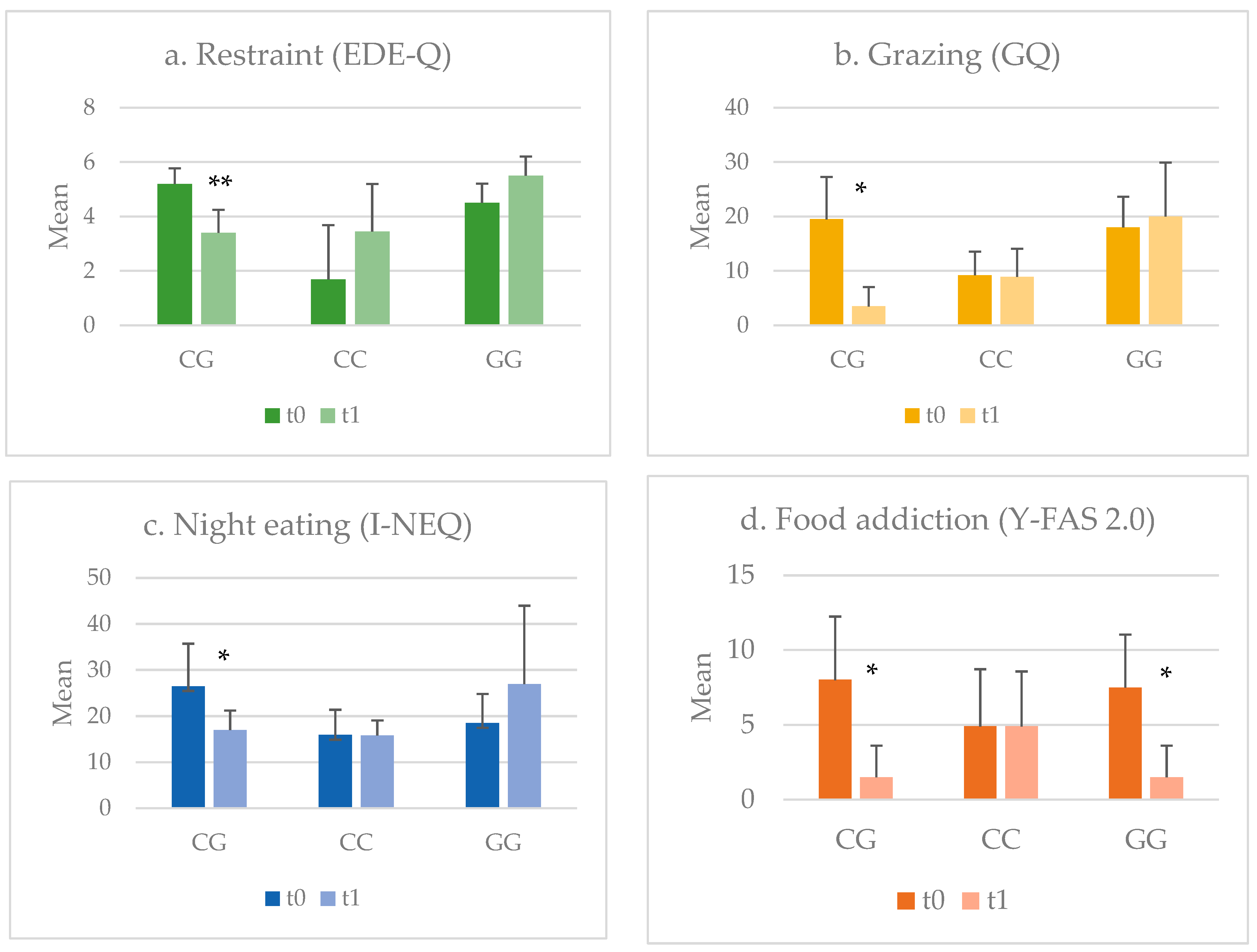
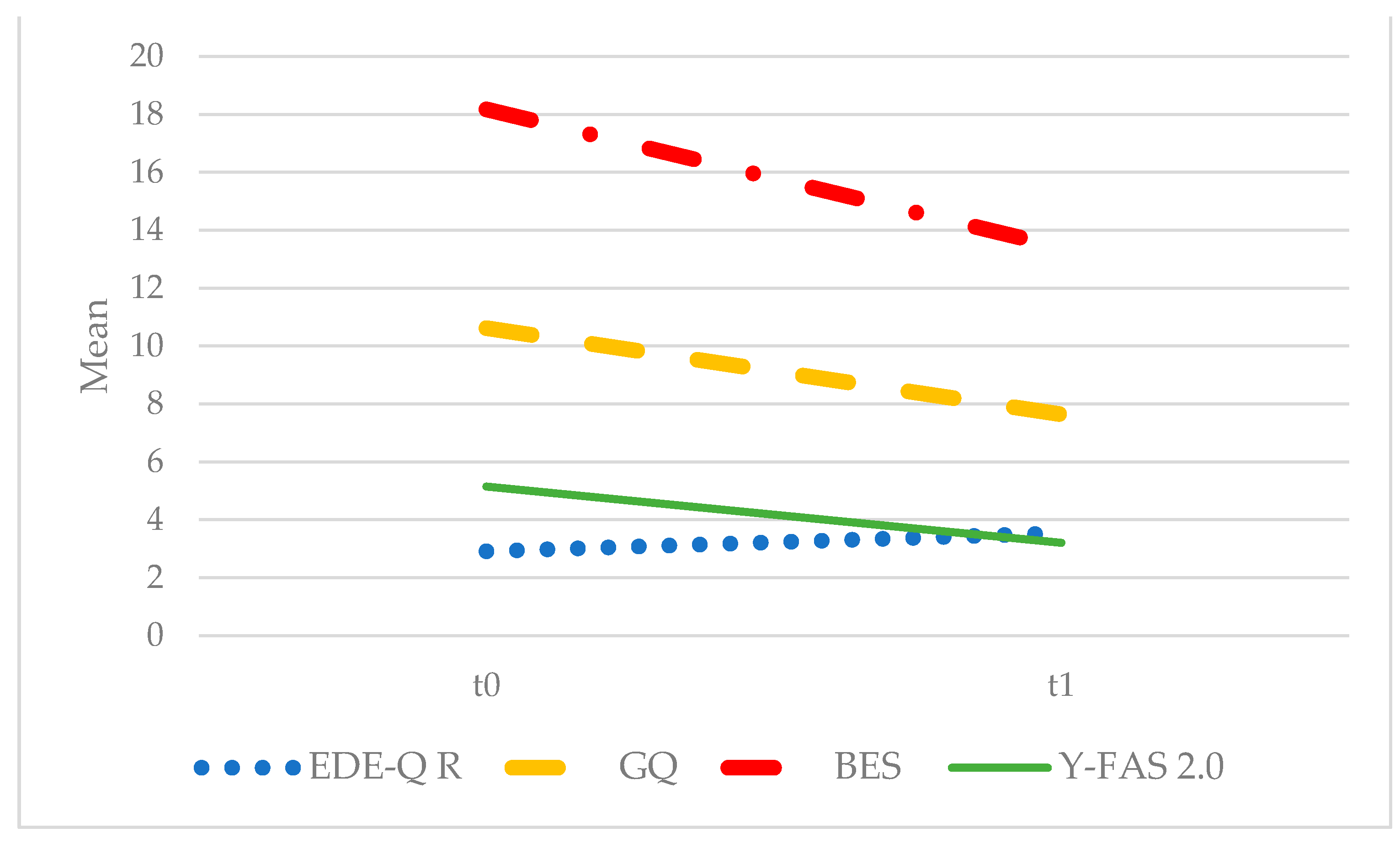
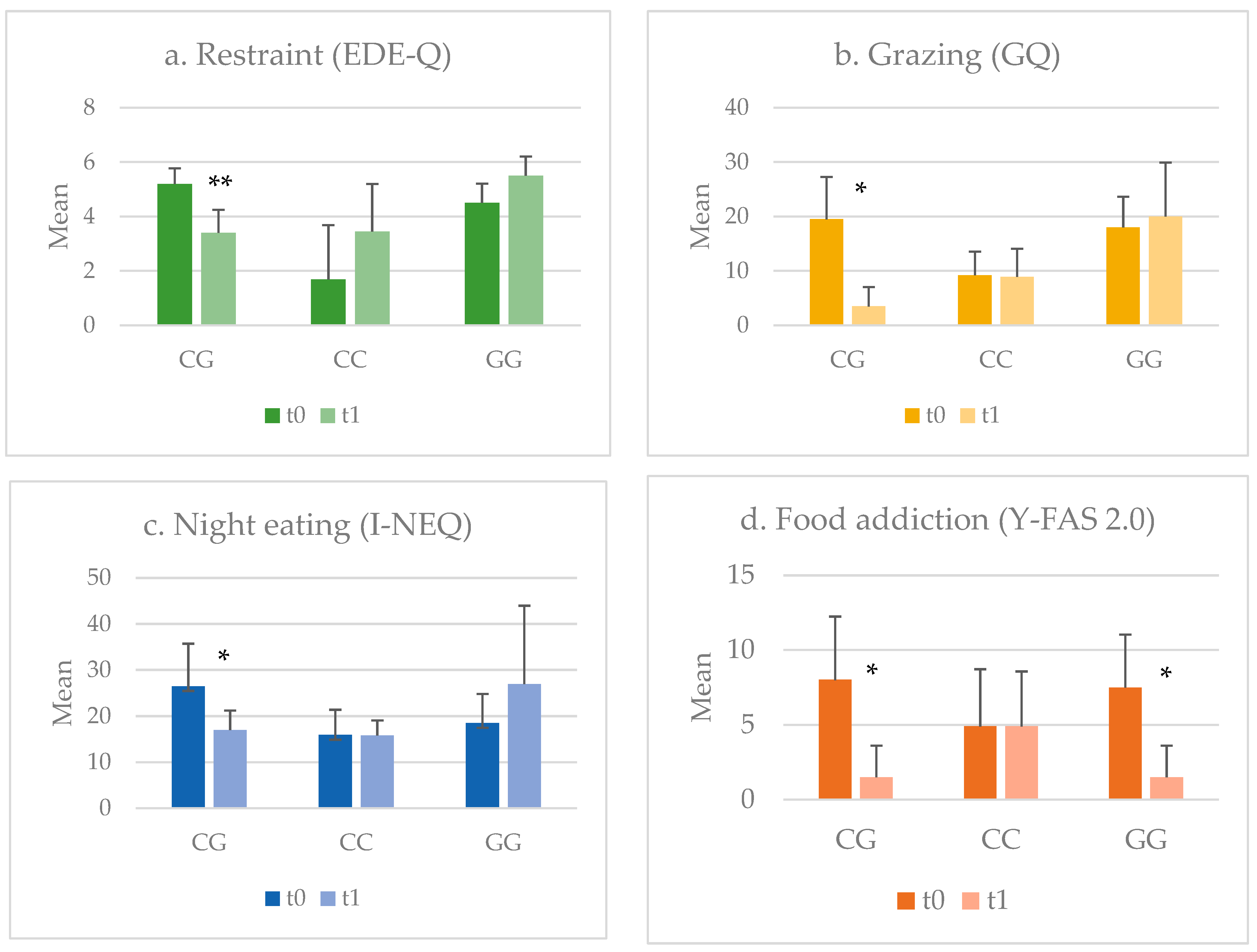
- Eating Disorder Examination Questionnaire (EDE-Q 6.0) [34] to evaluate the psychopathology and symptomatology of eating disorders; we consider the Restraint subscale of EDE-Q as a measure of the reduction in food intake;
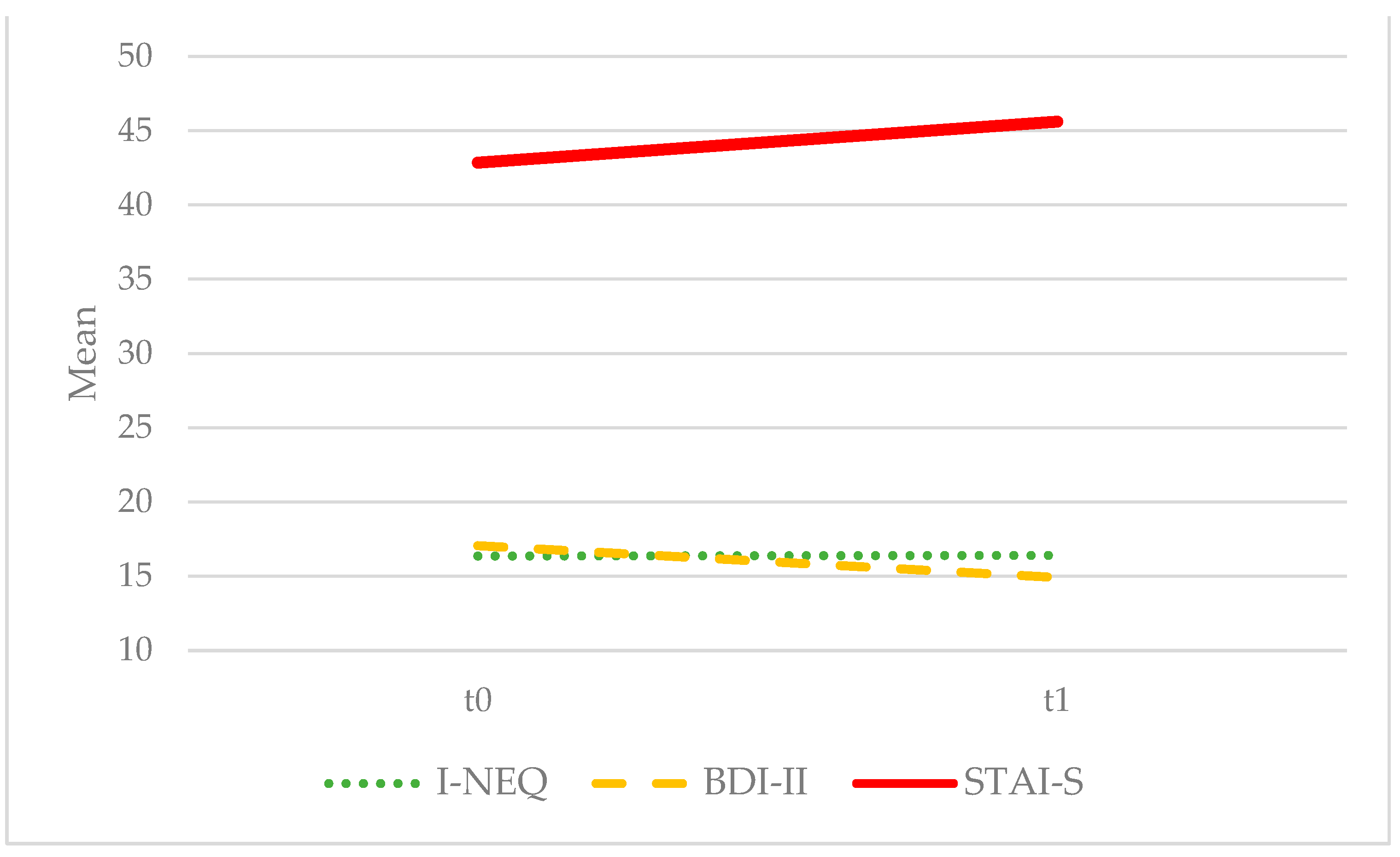
- Beck Depression Inventory (BDI-II) to assess depression severity [35];
- State–Trait Anxiety Inventory (STAI-S) to assess state anxiety [36];
- Binge Eating Scale (BES) [37] to measure the severity of behaviours, feelings and cognitions associated with binge eating;
- Night eating questionnaire (NEQ) [38], Italian version, to measure the night eating symptoms;
- Grazing Questionnaire (GQ) [39], Italian version, to evaluate the grazing behaviour;
- Yale Food Addiction Scale 2.0 (Y-FAS 2.0) [40], Italian version, to assess addiction-like eating behavior over the past 12 months; for this study, the total criteria were used.
2.4. Patient Genotyping Analysis
2.5. Treatment Program
2.6. Data Analysis
3. Results
3.1. Sample Description
3.2. Treatment Response
3.3. Influence of rs757081 NUCB2 Polymorphism on Treatment Response
4. Discussion
Practical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morton, G.J.; Meek, T.H.; Schwartz, M.W. Neurobiology of Food Intake in Health and Disease. Nat. Rev. Neurosci. 2014, 15, 367–378. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.-J.; Baler, R.D. Reward, Dopamine and the Control of Food Intake: Implications for Obesity. Trends Cogn. Sci. 2011, 15, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Lutter, M.; Nestler, E.J. Homeostatic and Hedonic Signals Interact in the Regulation of Food Intake. J. Nutr. 2009, 139, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, M.M.I. Central and Peripheral Control of Food Intake. Endocr. Regul. 2017, 51, 52–70. [Google Scholar] [CrossRef] [PubMed]
- Oh-I, S.; Shimizu, H.; Satoh, T.; Okada, S.; Adachi, S.; Inoue, K.; Eguchi, H.; Yamamoto, M.; Imaki, T.; Hashimoto, K.; et al. Identification of Nesfatin-1 as a Satiety Molecule in the Hypothalamus. Nature 2006, 443, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Dore, R.; Levata, L.; Lehnert, H.; Schulz, C. Nesfatin-1: Functions and Physiology of a Novel Regulatory Peptide. J. Endocrinol. 2017, 232, R45–R65. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Zhang, J.; Tang, Y.; Bi, F.; Liu, J.N. The Novel Function of Nesfatin-1: Anti-Hyperglycemia. Biochem. Biophys. Res. Commun. 2010, 391, 1039–1042. [Google Scholar] [CrossRef]
- Könczöl, K.; Pintér, O.; Ferenczi, S.; Varga, J.; Kovács, K.; Palkovits, M.; Zelena, D.; Tóth, Z.E. Nesfatin-1 Exerts Long-Term Effect on Food Intake and Body Temperature. Int. J. Obes. 2012, 36, 1514–1521. [Google Scholar] [CrossRef]
- Dore, R.; Levata, L.; Gachkar, S.; Jöhren, O.; Mittag, J.; Lehnert, H.; Schulz, C. The Thermogenic Effect of Nesfatin-1 Requires Recruitment of the Melanocortin System. J. Endocrinol. 2017, 235, 111–122. [Google Scholar] [CrossRef]
- Dore, R.; Krotenko, R.; Reising, J.P.; Murru, L.; Sundaram, S.M.; Di Spiezio, A.; Müller-Fielitz, H.; Schwaninger, M.; Jöhren, O.; Mittag, J.; et al. Nesfatin-1 Decreases the Motivational and Rewarding Value of Food. Neuropsychopharmacology 2020, 45, 1645–1655. [Google Scholar] [CrossRef]
- Lefner, M.J.; Wanat, M.J. Nesfatin-1 Puts the Brakes on Reward-Based Feeding. Neuropsychopharmacology 2020, 45, 1591–1592. [Google Scholar] [CrossRef]
- Price, T.O.; Samson, W.K.; Niehoff, M.L.; Banks, W.A. Permeability of the Blood-Brain Barrier to a Novel Satiety Molecule Nesfatin-1. Peptides 2007, 28, 2372–2381. [Google Scholar] [CrossRef]
- Goebel-Stengel, M.; Wang, L.; Stengel, A.; Taché, Y. Localization of Nesfatin-1 Neurons in the Mouse Brain and Functional Implication. Brain Res. 2011, 1396, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Erlanson-Albertsson, C. How Palatable Food Disrupts Appetite Regulation. Basic Clin. Pharmacol. Toxicol. 2005, 97, 61–73. [Google Scholar] [CrossRef]
- Zegers, D.; Beckers, S.; de Freitas, F.; Jennes, K.; Van Camp, J.K.; Mertens, I.L.; Van Hoorenbeeck, K.; Rooman, R.P.; Desager, K.N.; Massa, G.; et al. Identification of Mutations in the NUCB2/Nesfatin Gene in Children with Severe Obesity. Mol. Genet. Metab. 2012, 107, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Zegers, D.; Beckers, S.; Mertens, I.L.; Van Gaal, L.F.; Van Hul, W. Association between Polymorphisms of the Nesfatin Gene, NUCB2, and Obesity in Men. Mol. Genet. Metab. 2011, 103, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Chan, R.M.E.; Tan, K.M.L.; Poh, L.K.S.; Loke, K.Y.; Wang, J.P.; Li, H.; Hu, Y.H.; Wang, L.; Lee, K.O.; et al. The Association of a Nucleobindin 2 Gene (NUCB2) Variant with Childhood Adiposity. Gene 2013, 516, 48–52. [Google Scholar] [CrossRef]
- Agüera, Z.; Lozano-Madrid, M.; Mallorquí-Bagué, N.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. A Review of Binge Eating Disorder and Obesity. Neuropsychiatrie 2021, 35, 57–67. [Google Scholar] [CrossRef]
- Mehler, P.S.; Frank, G.K.W.; Mitchell, J.E. Medical Comorbidity and Medical Complications Associated with Binge-Eating Disorder. Int. J. Eat. Disord. 2016, 49, 319–323. [Google Scholar] [CrossRef]
- Caroleo, M.; Carbone, E.A.; Arcidiacono, B.; Greco, M.; Primerano, A.; Mirabelli, M.; Fazia, G.; Rania, M.; Hribal, M.L.; Gallelli, L.; et al. Does NUCB2/Nesfatin-1 Influence Eating Behaviors in Obese Patients with Binge Eating Disorder? Toward a Neurobiological Pathway. Nutrients 2023, 15, 348. [Google Scholar] [CrossRef]
- Iwasa, T.; Matsuzaki, T.; Tungalagsuvd, A.; Munkhzaya, M.; Yiliyasi, M.; Kuwahara, A.; Irahara, M. Developmental Changes in the Hypothalamic mRNA Levels of Nucleobindin-2 (NUCB2) and Their Sensitivity to Fasting in Male and Female Rats. Int. J. Dev. Neurosci. 2016, 49, 46–49. [Google Scholar] [CrossRef]
- Nasri, A.; Unniappan, S. Nucleobindin-Derived Nesfatin-1 and Nesfatin-1-like Peptide Stimulate pro-Opiomelanocortin Synthesis in Murine AtT-20 Corticotrophs through the CAMP/PKA/CREB Signaling Pathway. Mol. Cell. Endocrinol. 2021, 536, 111401. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wang, M.; Liu, L.; He, B.; Hu, J.; Wang, Y. Hypothalamic Nesfatin-1 Mediates Feeding Behavior via MC3/4R-ERK Signaling Pathway after Weight Loss in Obese Sprague-Dawley Rats. Peptides 2019, 119, 170080. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shu, X.; Cong, Z.K.; Jiang, Z.Y.; Jiang, H. Nesfatin-1 Acts on the Dopaminergic Reward Pathway to Inhibit Food Intake. Neuropeptides 2015, 53, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Ari, M.; Ozturk, O.H.; Bez, Y.; Oktar, S.; Erduran, D. High Plasma Nesfatin-1 Level in Patients with Major Depressive Disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, T.; Weibert, E.; Ahnis, A.; Obbarius, A.; Elbelt, U.; Rose, M.; Klapp, B.F.; Stengel, A. Alterations of Circulating NUCB2/Nesfatin-1 during Short Term Therapeutic Improvement of Anxiety in Obese Inpatients. Psychoneuroendocrinology 2017, 79, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Greenway, F.L.; Fujioka, K.; Plodkowski, R.A.; Mudaliar, S.; Guttadauria, M.; Erickson, J.; Kim, D.D.; Dunayevich, E. Effect of Naltrexone plus Bupropion on Weight Loss in Overweight and Obese Adults (COR-I): A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet 2010, 376, 595–605. [Google Scholar] [CrossRef]
- Apovian, C.M.; Aronne, L.; Rubino, D.; Still, C.; Wyatt, H.; Burns, C.; Kim, D.; Dunayevich, E.; COR-II Study Group. A Randomized, Phase 3 Trial of Naltrexone SR/Bupropion SR on Weight and Obesity-Related Risk Factors (COR-II). Obesity 2013, 21, 935–943. [Google Scholar] [CrossRef]
- Hollander, P.; Gupta, A.K.; Plodkowski, R.; Greenway, F.; Bays, H.; Burns, C.; Klassen, P.; Fujioka, K.; COR-Diabetes Study Group. Effects of Naltrexone Sustained-Release/Bupropion Sustained-Release Combination Therapy on Body Weight and Glycemic Parameters in Overweight and Obese Patients with Type 2 Diabetes. Diabetes Care 2013, 36, 4022–4029. [Google Scholar] [CrossRef]
- Carbone, E.A.; Caroleo, M.; Rania, M.; Calabrò, G.; Staltari, F.A.; de Filippis, R.; Aloi, M.; Condoleo, F.; Arturi, F.; Segura-Garcia, C. An Open-Label Trial on the Efficacy and Tolerability of Naltrexone/Bupropion SR for Treating Altered Eating Behaviours and Weight Loss in Binge Eating Disorder. Eat. Weight Disord. 2021, 26, 779–788. [Google Scholar] [CrossRef]
- Gadde, K.M.; Allison, D.B.; Ryan, D.H.; Peterson, C.A.; Troupin, B.; Schwiers, M.L.; Day, W.W. Effects of Low-Dose, Controlled-Release, Phentermine plus Topiramate Combination on Weight and Associated Comorbidities in Overweight and Obese Adults (CONQUER): A Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2011, 377, 1341–1352. [Google Scholar] [CrossRef]
- World Medical Association, W. Wma Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 8 January 2024).
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders—Clinician Version (SCID-5-CV); American Psychiatric Association: Washington, DC, USA, 2016. [Google Scholar]
- Fairburn, C.G.; Beglin, S.J. Assessment of Eating Disorder Psychopathology: Interview or Self-Report Questionnaire. Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.; Lushene, R. STAI Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The Assessment of Binge Eating Severity among Obese Persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Aloi, M.; Rania, M.; De Fazio, P.; Vinai, P.; Tagliabue, A.; Allison, K.C.; Segura-Garcia, C.; Segura-García, C. Validation of the Italian Version of the Night Eating Questionnaire (I-NEQ). J. Psychopathol. 2017, 23, 137–144. [Google Scholar]
- Aloi, M.; Rania, M.; De Fazio, P.; Segura-Garcia, C. Italian Validation of the Grazing Questionnaire: Analysis of Psychometric Properties. Minerva Psichiatr. 2017, 58, 196–202. [Google Scholar] [CrossRef]
- Aloi, M.; Rania, M.; Rodríguez Muñoz, R.C.; Jiménez Murcia, S.; Fernández-Aranda, F.; De Fazio, P.; Segura-Garcia, C. Validation of the Italian Version of the Yale Food Addiction Scale 2.0 (I-YFAS 2.0) in a Sample of Undergraduate Students. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Valbrun, L.P.; Zvonarev, V. The Opioid System and Food Intake: Use of Opiate Antagonists in Treatment of Binge Eating Disorder and Abnormal Eating Behavior. J. Clin. Med. Res. 2020, 12, 41–63. [Google Scholar] [CrossRef] [PubMed]
- Billes, S.K.; Sinnayah, P.; Cowley, M.A. Naltrexone/Bupropion for Obesity: An Investigational Combination Pharmacotherapy for Weight Loss. Pharmacol. Res. 2014, 84, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Wang, J.; Wan, X. Association of the Polymorphism in Nucleobindin 2 Gene and the Risk of Metabolic Syndrome. Genet. Test. Mol. Biomark. 2016, 20, 49–52. [Google Scholar] [CrossRef]
- Schalla, M.A.; Unniappan, S.; Lambrecht, N.W.G.; Mori, M.; Taché, Y.; Stengel, A. NUCB2/Nesfatin-1—Inhibitory Effects on Food Intake, Body Weight and Metabolism. Peptides 2020, 128, 170308. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Maejima, Y.; Sedbazar, U.; Ando, A.; Kurita, H.; Damdindorj, B.; Takano, E.; Gantulga, D.; Iwasaki, Y.; Kurashina, T.; et al. Stressor-Responsive Central Nesfatin-1 Activates Corticotropin-Releasing Hormone, Noradrenaline and Serotonin Neurons and Evokes Hypothalamic-Pituitary-Adrenal Axis. Aging 2010, 2, 775–784. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Group 1 (Ob-BED) N = 22 | Group 2 (Ob-noBED) N = 20 | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | p | ||
| Age | (Years) | 42 | (12.5) | 43.4 | (14.7) | 1.380 | 0.744 |
| BMI | (kg/m2) | 38.4 | (6.7) | 45.4 | (10.4) | 2.617 | 0.012 |
| Fr | % | Fr | % | χ² | p | ||
| Sex | Female | 18 | (81.8) | 8 | (40) | 6.010 | 0.013 |
| Male | 4 | (18.2) | 12 | (60) | |||
| Education | Elementary school | 2 | (9.1) | 3 | (15) | 1.552 | 0.670 |
| Middle school I | 5 | (22.7) | 5 | (25) | |||
| High school II | 11 | (50) | 12 | (60) | |||
| University degree | 4 | (18.2) | 0 | (0) | |||
| Employment | Unpaid activity | 5 | (22.7) | 2 | (10) | 2.387 | 0.496 |
| Employed | 13 | (59.1) | 11 | (55) | |||
| Unemployed | 3 | (13.6) | 6 | (30) | |||
| Student | 1 | (4.5) | 1 | (5) | |||
| Civil status | Single | 9 | (40.9) | 7 | (35) | 0.155 | 0.925 |
| Married | 11 | (50) | 11 | (55) | |||
| Divorced | 2 | (9.1) | 2 | (10) | |||
| rs757081 NUCB2 genotype | CG | 3 | (13.6) | 7 | (35) | 2.637 | 0.680 |
| CC | 16 | (72.7) | 11 | (55) | |||
| GG | 3 | (13.6) | 2 | (10) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbone, E.A.; Caroleo, M.; Rania, M.; de Filippis, R.; Condoleo, F.; Catalano, F.; Aloi, M.; De Fazio, P.; Arturi, F.; Hribal, M.L.; et al. Influence of NUCB/Nesfatin-1 Polymorphism on Treatment Response to Naltrexone/Bupropion SR in Binge Eating Disorder and Obesity. Biomedicines 2024, 12, 451. https://doi.org/10.3390/biomedicines12020451
Carbone EA, Caroleo M, Rania M, de Filippis R, Condoleo F, Catalano F, Aloi M, De Fazio P, Arturi F, Hribal ML, et al. Influence of NUCB/Nesfatin-1 Polymorphism on Treatment Response to Naltrexone/Bupropion SR in Binge Eating Disorder and Obesity. Biomedicines. 2024; 12(2):451. https://doi.org/10.3390/biomedicines12020451
Chicago/Turabian StyleCarbone, Elvira Anna, Mariarita Caroleo, Marianna Rania, Renato de Filippis, Francesca Condoleo, Federica Catalano, Matteo Aloi, Pasquale De Fazio, Franco Arturi, Marta Letizia Hribal, and et al. 2024. "Influence of NUCB/Nesfatin-1 Polymorphism on Treatment Response to Naltrexone/Bupropion SR in Binge Eating Disorder and Obesity" Biomedicines 12, no. 2: 451. https://doi.org/10.3390/biomedicines12020451
APA StyleCarbone, E. A., Caroleo, M., Rania, M., de Filippis, R., Condoleo, F., Catalano, F., Aloi, M., De Fazio, P., Arturi, F., Hribal, M. L., Fiorentino, T. V., & Segura-Garcia, C. (2024). Influence of NUCB/Nesfatin-1 Polymorphism on Treatment Response to Naltrexone/Bupropion SR in Binge Eating Disorder and Obesity. Biomedicines, 12(2), 451. https://doi.org/10.3390/biomedicines12020451