
Influence of Obesity on Short-Term Surgical Outcomes in HFrEF Patients Undergoing CABG: A Retrospective Multicenter Study

 ,
, 
 , , , ,
, , , ,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Description of Surgical Procedures
2.3. Statistical Analysis
3. Results
3.1. Preoperative Demographic and Clinical Profile
3.2. Intraoperative Management
3.3. Postoperative Outcomes and Laboratory Insights
3.4. Complications and Morbidity
4. Discussion
4.1. Preoperative Demographic and Clinical Profile
4.2. Intraoperative Management
4.3. Postoperative Outcomes and Laboratory Insights
4.4. Complications and Morbidity
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Despres, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Riaz, H.; Khan, M.S.; Siddiqi, T.J.; Usman, M.S.; Shah, N.; Goyal, A.; Khan, S.S.; Mookadam, F.; Krasuski, R.A.; Ahmed, H. Association between Obesity and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Mendelian Randomization Studies. JAMA Netw. Open 2018, 1, e183788. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Arena, R.; Alpert, M.A.; Milani, R.V.; Ventura, H.O. Management of Cardiovascular Diseases in Patients with Obesity. Nat. Rev. Cardiol. 2018, 15, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Stefil, M.; Gaudino, M.; Benedetto, U.; Gerry, S.; Gray, A.; Lees, B.; Podesser, B.; Krzych, L.; Sajja, L.R.; Taggart, D.; et al. Influence of Diabetes and Obesity on Ten-Year Outcomes after Coronary Artery Bypass Grafting in the Arterial Revascularisation Trial. Clin. Res. Cardiol. 2023, 2023, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Krasivskyi, I.; Eghbalzadeh, K.; Ivanov, B.; Gerfer, S.; Grossmann, C.; Sabashnikov, A.; Kuhn, E.; Mader, N.; Djordjevic, I.; Wahlers, T. Impact of Obesity on Early in-Hospital Outcomes after Coronary Artery Bypass Grafting Surgery in Acute Coronary Syndrome: A Propensity Score Matching Analysis. J. Clin. Med. 2022, 11, 6805. [Google Scholar] [CrossRef]
- Chan, P.G.; Sultan, I.; Gleason, T.G.; Wang, Y.; Navid, F.; Thoma, F.; Kilic, A. Contemporary Outcomes of Coronary Artery Bypass Grafting in Obese Patients. J. Card. Surg. 2020, 35, 549–556. [Google Scholar] [CrossRef]
- Ruka, E.; Dagenais, F.; Mohammadi, S.; Chauvette, V.; Poirier, P.; Voisine, P. Bilateral Mammary Artery Grafting Increases Postoperative Mediastinitis without Survival Benefit in Obese Patients. Eur. J. Cardiothorac. Surg. 2016, 50, 1188–1195. [Google Scholar] [CrossRef]
- Grau, J.B.; Kuschner, C.E.; Johnson, C.K.; Ferrari, G.; Zapolanski, A.; Brizzio, M.E.; Shaw, R.E. The Effects of Using a Radial Artery in Patients Already Receiving Bilateral Internal Mammary Arteries During Coronary Bypass Grafting: 30-Day Outcomes and 14-Year Survival in a Propensity-Matched Cohort. Eur. J. Cardiothorac. Surg. 2016, 49, 203–210. [Google Scholar] [CrossRef]
- Rustenbach, C.J.; Reichert, S.; Radwan, M.; Doll, I.; Mustafi, M.; Nemeth, A.; Marinos, S.L.; Berger Baumbach, R.; Zdanyte, M.; Haeberle, H.; et al. On- vs. Off- Pump Cabg in Heart Failure Patients with Reduced Ejection Fraction (Hfref): A Multicenter Analysis. Biomedicines 2023, 11, 3043. [Google Scholar] [CrossRef] [PubMed]
- Engel, A.M.; McDonough, S.; Smith, J.M. Does an Obese Body Mass Index Affect Hospital Outcomes after Coronary Artery Bypass Graft Surgery? Ann. Thorac. Surg. 2009, 88, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.P.; Parlow, J.L.; Whitehead, M.; Xu, J.; Rohland, S.; Milne, B. Body Mass Index, Outcomes, and Mortality Following Cardiac Surgery in Ontario, Canada. J. Am. Heart Assoc. 2015, 4, e002140. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. Euroscore Ii. Eur. J. Cardiothorac. Surg. 2012, 41, 734–744, discussion 44–45. [Google Scholar] [CrossRef] [PubMed]
- Mariscalco, G.; Wozniak, M.J.; Dawson, A.G.; Serraino, G.F.; Porter, R.; Nath, M.; Klersy, C.; Kumar, T.; Murphy, G.J. Body Mass Index and Mortality among Adults Undergoing Cardiac Surgery: A Nationwide Study with a Systematic Review and Meta-Analysis. Circulation 2017, 135, 850–863. [Google Scholar] [CrossRef]
- Lavie, C.J.; Alpert, M.A.; Arena, R.; Mehra, M.R.; Milani, R.V.; Ventura, H.O. Impact of Obesity and the Obesity Paradox on Prevalence and Prognosis in Heart Failure. JACC Heart Fail. 2013, 1, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Ghoorah, K.; Campbell, P.; Kent, A.; Maznyczka, A.; Kunadian, V. Obesity and Cardiovascular Outcomes: A Review. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 77–85. [Google Scholar] [CrossRef]
- Bhavsar, R.; Tang, M.; Greisen, J.; Jakobsen, C.J. Increasing Obesity Is Associated with Lower Postoperative Bleeding in Coronary Bypass Patients. J. Cardiothorac. Vasc. Anesth. 2023, 37, 1129–1137. [Google Scholar] [CrossRef]
- Zhang, W.; Chen, S.; Liu, X.; Wang, L.; Wang, S.; Yu, Y.; Ao, H. Can Higher Body Mass Index Patients Save Blood Following on-Pump Coronary Artery Bypass Grafting? Heart Surg. Forum 2019, 22, E352–E356. [Google Scholar] [CrossRef]
- Braekkan, S.K.; van der Graaf, Y.; Visseren, F.L.; Algra, A. Obesity and Risk of Bleeding: The Smart Study. J. Thromb. Haemost. 2016, 14, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Bladbjerg, E.M.; Stolberg, C.R.; Juhl, C.B. Effects of Obesity Surgery on Blood Coagulation and Fibrinolysis: A Literature Review. Thromb. Haemost. 2020, 120, 579–591. [Google Scholar] [CrossRef]
- Lock, J.F.; Ungeheuer, L.; Borst, P.; Swol, J.; Lob, S.; Brede, E.M.; Roder, D.; Lengenfelder, B.; Sauer, K.; Germer, C.T. Markedly Increased Risk of Postoperative Bleeding Complications During Perioperative Bridging Anticoagulation in General and Visceral Surgery. Perioper. Med. 2020, 9, 39. [Google Scholar] [CrossRef]
- Gurm, H.S.; Whitlow, P.L.; Kip, K.E.; Bari Investigators. The Impact of Body Mass Index on Short- and Long-Term Outcomes Inpatients Undergoing Coronary Revascularization. Insights from the Bypass Angioplasty Revascularization Investigation (Bari). J. Am. Coll. Cardiol. 2002, 39, 834–840. [Google Scholar] [CrossRef]
- Aguiar, C.; MacLeod, J.; Yip, A.; Melville, S.; Legare, J.F.; Pulinilkunnil, T.; Kienesberger, P.; Brunt, K.; Hassan, A. Impact of Obesity on Postoperative Outcomes Following Cardiac Surgery (the Opos Study): Rationale and Design of an Investigator-Initiated Prospective Study. BMJ Open 2019, 9, e023418. [Google Scholar] [CrossRef]
- Alam, M.; Siddiqui, S.; Lee, V.V.; Elayda, M.A.; Nambi, V.; Yang, E.Y.; Jneid, H.M.; Wilson, J.M.; Ballantyne, C.M.; Virani, S.S. Isolated Coronary Artery Bypass Grafting in Obese Individuals: A Propensity Matched Analysis of Outcomes. Circ. J. 2011, 75, 1378–1385. [Google Scholar] [CrossRef]
- De Heredia, F.P.; Gomez-Martinez, S.; Marcos, A. Obesity, Inflammation and the Immune System. Proc. Nutr. Soc. 2012, 71, 332–338. [Google Scholar] [CrossRef]
- Vargo, P.R.; Steffen, R.J.; Bakaeen, F.G.; Navale, S.; Soltesz, E.G. The Impact of Obesity on Cardiac Surgery Outcomes. J. Card. Surg. 2018, 33, 588–594. [Google Scholar] [CrossRef]
- Ko, Y.; Kim, H.E.; Park, J.Y.; Kim, J.J.; Cho, J.; Oh, J. Relationship between Body Mass Index and Risk of Delirium in an Intensive Care Unit. Arch. Gerontol. Geriatr. 2023, 108, 104921. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Han, D.; Xu, F.; Zheng, S.; Zhang, L.; Wang, Z.; Yang, R.; Yin, H.; Lyu, J. Obesity Paradox of All-Cause Mortality in 4133 Patients Treated with Coronary Revascularization. J. Interv. Cardiol. 2021, 2021, 3867735. [Google Scholar] [CrossRef] [PubMed]
- Gruberg, L.; Mercado, N.; Milo, S.; Boersma, E.; Disco, C.; van Es, G.A.; Lemos, P.A.; Tzvi, M.B.; Wijns, W.; Unger, F.; et al. Impact of Body Mass Index on the Outcome of Patients with Multivessel Disease Randomized to Either Coronary Artery Bypass Grafting or Stenting in the Arts Trial: The Obesity Paradox Ii? Am. J. Cardiol. 2005, 95, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Amundson, D.E.; Djurkovic, S.; Matwiyoff, G.N. The Obesity Paradox. Crit. Care Clin. 2010, 26, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Horwich, T.B.; Fonarow, G.C.; Hamilton, M.A.; MacLellan, W.R.; Woo, M.A.; Tillisch, J.H. The Relationship between Obesity and Mortality in Patients with Heart Failure. J. Am. Coll. Cardiol. 2001, 38, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.I.; Gao, Y.; Anugu, P.; Anugu, A.; Correa, A. Obesity and Overall Mortality: Findings from the Jackson Heart Study. BMC Public Health 2021, 21, 50. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total Cohort | Normal Weight | Obesity | p Value |
|---|---|---|---|---|
| (n = 574) | (n = 163) 28.4% | (n = 158) 27.5% | ||
| Demographic Data | ||||
| Age, mean (±SD) | 67.82 (±9.89) | 69.15 (±9.85) | 65.84 (±10.00) | 0.003 ANOVA |
| Gender | ||||
| Male n (%) | 504 (87.80%) | 144 (88.34%) | 134 (84.81%) | 0.353 Chi² |
| Female n (%) | 70 (12.19%) | 19 (11.65%) | 24 (15.19%) | |
| BMI, mean (±SD) | 27.91 (±5.01) | 23.03 (±1.50) | 34.15 (±4.04) | <0.001 ANOVA |
| Clinical Measurements | ||||
| EuroScore II, mean (±SD) | 5.36 (±5.08) | 4.99 (±4.32) | 5.23 (±4.87) | 0.648 ANOVA |
| STS Score, mean (±SD) | 2.65 (±2.31) | 2.56 (±2.06) | 2.60 (±2.43) | 0.860 ANOVA |
| LVEF preop, mean (±SD) | 31.51 (±6.97) | 30.34 (±7.06) | 32.04 (±6.46) | 0.026 ANOVA |
| Health Status | ||||
| Diabetes | ||||
| OAD n (%) | 134 (23.3%) | 37 (22.69%) | 39 (24.68%) | 0.051 Chi² |
| Insulin dependent n (%) | 138 (24.0%) | 33 (19.64%) | 48 (27.22%) | |
| Smoking history | ||||
| Former n (%) | 157 (27.4%) | 38 (23.31%) | 52 (32.91%) | 0.131 Chi² |
| Active n (%) | 117 (20.4%) | 31 (19.13%) | 29 (17.94%) | |
| Hypertension, n (%) | 534 (93.03%) | 151 (92.6%) | 151 (95.56%) | 0.266 Chi2 |
| COPD, n (%) | 111 (19.3%) | 33 (20.25%) | 36 (22.78%) | 0.580 Chi2 |
| Hyperlipidemia, n (%) | 484 (84.6%) | 138 (84.66%) | 136 (86.08%) | 0.617 Chi² |
| Stroke preOP, n (%) | 59 (10.27%) | 15 (9.20%) | 16 (10.12%) | 0.779 Chi² |
| Carotid Stenosis, n (%) | 95 (10.27%) | 34 (9.20%) | 27 (17.09%) | 0.389 Chi² |
| PAD, n (%) | 131 (22.82%) | 33 (20.46%) | 35 (22.15%) | 0.676 Chi² |
| Renal insufficiency, n (%) | 172 (29.97%) | 44 (26.99%) | 45 (28.48%) | 0.845 Chi² |
| Cardiac History | ||||
| Rhythm, pre-operative | ||||
| SR, n (%) | 378 (65.85%) | 116 (71.17%) | 101 (63.92%) | 0.296 Chi² |
| Afib, n (%) | 192 (33.45%) | 47 (28.83%) | 55 (34.81%) | |
| NSTEMI, n (%) | 188 (32.75%) | 52 (31.90%) | 53 (33.54%) | 0.754 Chi2 |
| STEMI, n (%) | 86 (14.98%) | 25 (15.34%) | 19 (12.03%) | 0.388 Chi2 |
| Previous PCI, n (%) | 206 (35.89%) | 54 (33.13%) | 65 (41.14%) | 0.126 Chi2 |
| Classification of surgery | ||||
| Elective, n (%) | 314 (54.7%) | 86 (52.76%) | 90 (56.96%) | 0.695 Chi² |
| Urgent, n (%) | 173 (30.1%) | 50 (30.67%) | 42 (26.58%) | |
| Emergent, n (%) | 87 (15.2%) | 27 (16.56%) | 26 (16.46%) |
| BMI Category | Normal Weight | Obesity | Total (n, %) |
|---|---|---|---|
| OPCAB (n, %) | 56 (34.35%) | 69 (43.67%) | 125 (51.0%) |
| ONCAB (n, %) | 107 (65.64%) | 89 (56.33%) | 196 (48.9%) |
| Total, n (%) by BMI Cateory | 163 (50.78%) | 158 (49.22%) | 321 (100%) |
| Variable | Total Cohort | Normal Weight | Obesity | p Value |
|---|---|---|---|---|
| (n = 574) | (n = 163) | (n = 158) | ||
| 28.4% | 27.5% | |||
| Intraoperative Requirement for Transfusion | ||||
| PRB, mean (±SD) | 0.48 (±1.08) | 0.35 (±0.88) | 0.72 (±1.29) | 0.002 ANOVA |
| PLTP, mean (±SD) | 0.34 (±0.69) | 0.44 (±0.79) | 0.28 (±0.61) | 0.142 ANOVA |
| FFP, mean (±SD) | 0.27 (±1.07) | 0.34 (±1.22) | 0.30 (±1.15) | 0.602 ANOVA |
| Postoperative (after chest closure) Vasopressor and Inotropic requirements | ||||
| Epinephrine, median (IQR) | 0 (0–0.04) | 0 (0–0.05) | 0 (0–0.02) | 0.048 MW |
| Norepinephrine, median (IQR) | 0.10 (0.06–0.16) | 0.11 (0.06–0.17) | 0.1 (0–0.10) | 0.120 MW |
| Postoperative Parameters and Complications | ||||
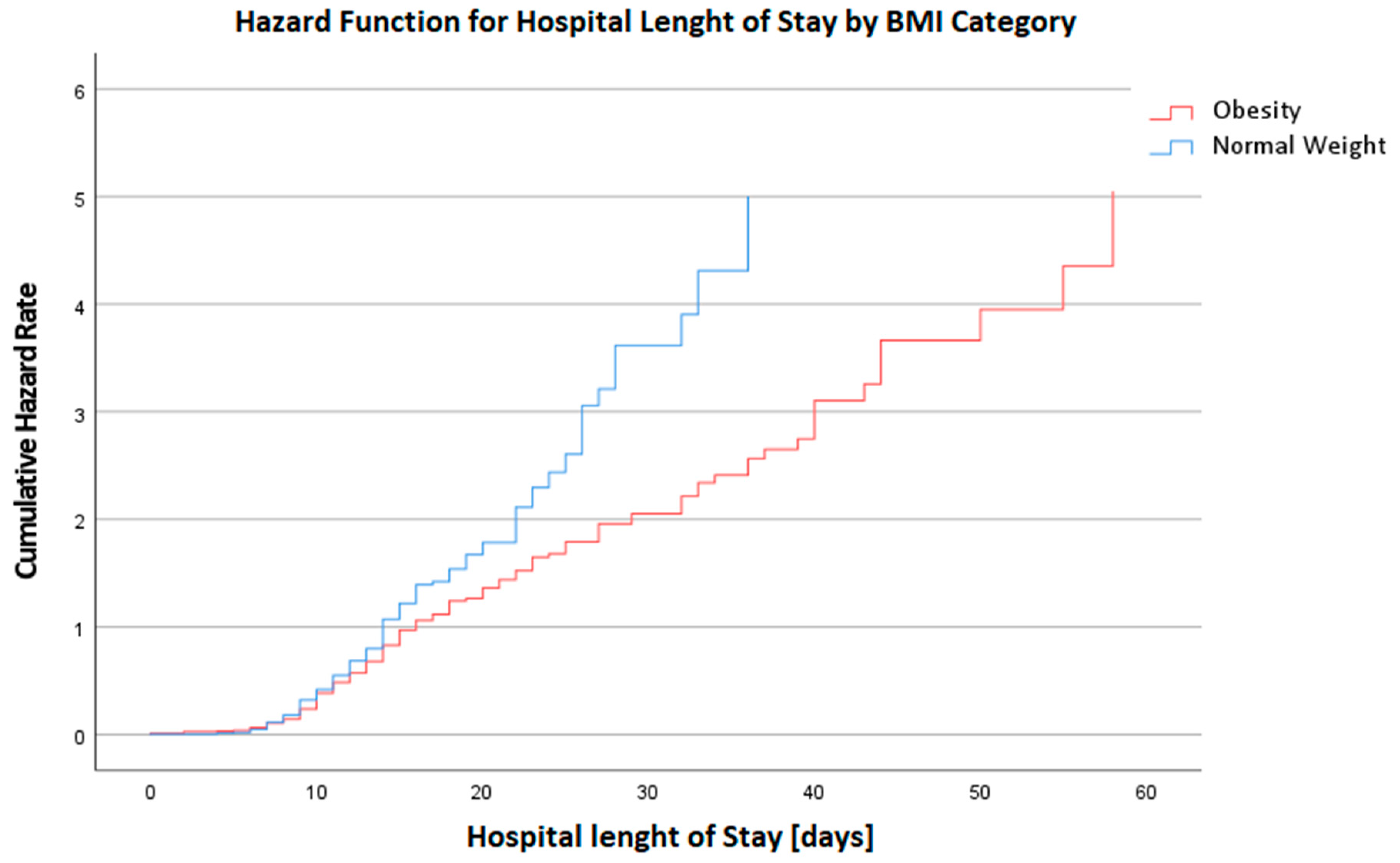
| LOS@Hospital (d), median (IQR) | 13 (9–18) | 13 (9–16.5) | 14 (10–21) | 0.041 MW |
| LOS@ICU (h), median (IQR) | 92 (42–144) | 87 (46–143) | 95 (42–165) | 0.163 MW |
| Vent (h), median (IQR) | 13 (8–23) | 13 (8–28) | 16 (8–31) | 0.049 MW |
| Laboratory values pre OP | ||||
| Hb (g/dl), mean (±SD) | 13.40 (±1.95) | 13.06 (±1.91) | 13.56 (±1.89) | 0.019 TT |
| Creatinine (mg/dl), mean (±SD) | 2.62 (±11.07) | 2.23 (±9.52) | 2.26 (±9.74) | 0.976 TT |
| GFR (ml/min/BSA), mean (±SD) | 76.35 (±25.68) | 77.37 (±27.11) | 75.77 (±24.29) | 0.580 TT |
| CK (U/L), mean (±SD) | 228.98 (±618.20) | 204.65 (±538.83) | 285.14 (±839.72) | 0.363 TT |
| CK-MB (U/L), mean (±SD) | 48.41 (±79.35) | 41.44 (±62.57) | 45.36 (±63.67) | 0.724 TT |
| Trop I (HS) (ng/L), mean (±SD) | 1033.61 (±3770.32) | 811.72 (±3171.76) | 1216.98 (±3799.54) | 0.416 TT |
| Lactate (mmol/L), mean (±SD) | 0.97 (±0.57) | 1.03 (±0.65) | 0.96 (±0.49) | 0.316 TT |
| Variable | Total Cohort | Normal Weight | Obesity | p Value | OR | 95% CI | p Value |
|---|---|---|---|---|---|---|---|
| (n = 574) | (n = 163) | (n = 158) | |||||
| 28.4% | 27.5% | ||||||
| Resuscitation, n (%) | 20 (3.48%) | 8 (4.91%) | 4 (2.53%) | 0.267 Chi² | 0.671 | 0.29–2.36 | 0.999 Wald |
| Resternotomy, n (%) | 36 (6.27%) | 12 (7.36%) | 11 (6.96%) | 0.902 Chi² | 0.956 | 0.22–4.15 | 0.952 Wald |
| ECLS, n (%) | 46 (85.18%) | 14 (8.58%) | 17 (10.75%) | 0.348 Chi² | 1.219 | 0.37–4.06 | 0.747 Wald |
| AKI, n (%) | 74 (12.89%) | 15 (9.20%) | 28 (17.72%) | 0.048 Chi² | 2.424 | 0.14–1.28 | 0.129 Wald |
| Dialysis, n (%) | 66 (11.49%) | 16 (9.82%) | 21 (13.29%) | 0.452 Chi² | 1.124 | 0.16–3.18 | 0.669 Wald |
| OPCAB, n (%) | 233 (40.59%) | 56 (34.36%) | 69 (43.67%) | 0.087 Chi² | |||
| ONCAB, n (%) | 339 (59.06%) | 107 (65.64%) | 89 (56.33%) | ||||
| Stroke, n (%) | 19 (3.31%) | 2 (1.23%) | 5 (3.29%) | 0.174 Fish | 0.902 | 0.12–2.19 | 0.399 Wald |
| Delirium, n (%) | 98 (17.07%) | 22 (13.49%) | 41 (26.58%) | 0.016 Chi² | 2.523 | 0.26–1.05 | 0.068 Wald |
| Mortality, n (%) | 30 (5.22%) | 6 (3.68%) | 11 (6.96%) | 0.049 Chi² | 2.672 | 0.10–4.45 | 0.681 Wald |
| Sepsis, n (%) | 40 (6.96%) | 11 (6.75%) | 10 (6.33%) | 0.837 Chi² | 4.591 | 0.99–21.12 | 0.050 Wald |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rustenbach, C.J.; Reichert, S.; Salewski, C.; Schano, J.; Berger, R.; Nemeth, A.; Zdanyte, M.; Häberle, H.; Caldonazo, T.; Saqer, I.; et al. Influence of Obesity on Short-Term Surgical Outcomes in HFrEF Patients Undergoing CABG: A Retrospective Multicenter Study. Biomedicines 2024, 12, 426. https://doi.org/10.3390/biomedicines12020426
Rustenbach CJ, Reichert S, Salewski C, Schano J, Berger R, Nemeth A, Zdanyte M, Häberle H, Caldonazo T, Saqer I, et al. Influence of Obesity on Short-Term Surgical Outcomes in HFrEF Patients Undergoing CABG: A Retrospective Multicenter Study. Biomedicines. 2024; 12(2):426. https://doi.org/10.3390/biomedicines12020426
Chicago/Turabian StyleRustenbach, Christian Jörg, Stefan Reichert, Christoph Salewski, Julia Schano, Rafal Berger, Attila Nemeth, Monika Zdanyte, Helene Häberle, Túlio Caldonazo, Ibrahim Saqer, and et al. 2024. "Influence of Obesity on Short-Term Surgical Outcomes in HFrEF Patients Undergoing CABG: A Retrospective Multicenter Study" Biomedicines 12, no. 2: 426. https://doi.org/10.3390/biomedicines12020426
APA StyleRustenbach, C. J., Reichert, S., Salewski, C., Schano, J., Berger, R., Nemeth, A., Zdanyte, M., Häberle, H., Caldonazo, T., Saqer, I., Saha, S., Schnackenburg, P., Djordjevic, I., Krasivskyi, I., Serna-Higuita, L. M., Doenst, T., Hagl, C., Wahlers, T., Schlensak, C., & Sandoval Boburg, R. (2024). Influence of Obesity on Short-Term Surgical Outcomes in HFrEF Patients Undergoing CABG: A Retrospective Multicenter Study. Biomedicines, 12(2), 426. https://doi.org/10.3390/biomedicines12020426