

Mitral Valve Transcatheter Edge-to-Edge Repair (MV-TEER) in Patients with Secondary Mitral Regurgitation Improves Hemodynamics, Enhances Renal Function, and Optimizes Quality of Life in Patients with Advanced Renal Insufficiency
 , , and
, , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. NICaS® Device and Procedure
2.3. Impact of MV-TEER on Quality of Life (EQ-5D-3L Questionnaire)
2.4. Study Objectives
2.5. Statistical Analysis
3. Results
3.1. Overall Cohort
3.1.1. Baseline Characteristics
3.1.2. Hemodynamics, Tissue Perfusion, and Renal Function
3.2. Impact of MV-TEER in Relation to Renal Function
3.2.1. Baseline Characteristics in eGFR Subgroups
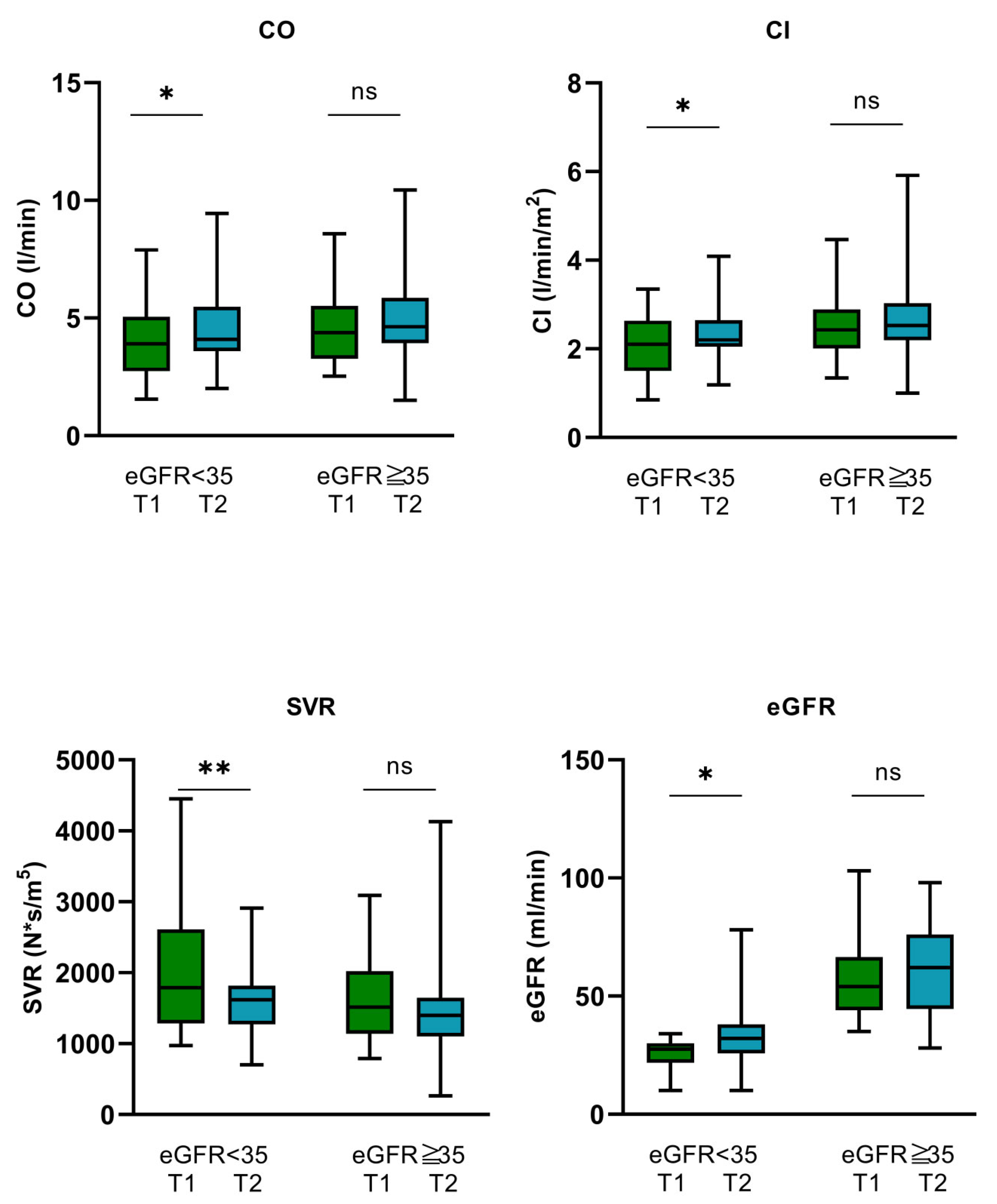
3.2.2. Hemodynamics, Tissue Perfusion, and Renal Function
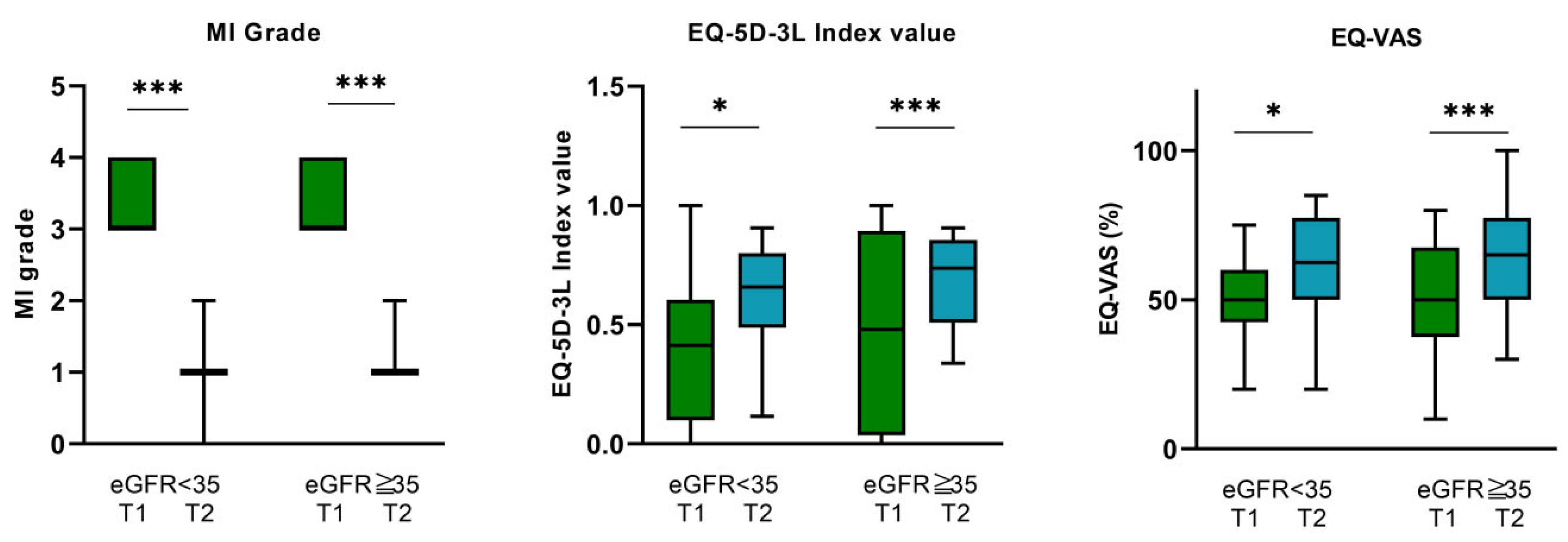
3.3. Impact of MV-TEER on Quality of Life—EQ-5D-3L and EQ-VAS Questionnaire
3.3.1. Overall Cohort
3.3.2. eGFR < 35 mL/min Subgroup
3.3.3. eGFR ≥ 35 mL/min Subgroup
4. Discussion
5. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aluru, J.S.; Barsouk, A.; Saginala, K.; Rawla, P.; Barsouk, A. Valvular Heart Disease Epidemiology. Med. Sci. 2022, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S. Mitral valve prolapse. Nihon Rinsho Jpn. J. Clin. Med. 2005, 63, 1195–1200. [Google Scholar]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, S.S.; Chokkalingam Mani, B. Mitral Valve Insufficiency; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Coffey, S.; Cairns, B.J.; Iung, B. The modern epidemiology of heart valve disease. Heart 2016, 102, 75–85. [Google Scholar] [CrossRef]
- Trichon, B.H.; Felker, G.M.; Shaw, L.K.; Cabell, C.H.; O’Connor, C.M. Relation of frequency and severity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure. Am. J. Cardiol. 2003, 91, 538–543. [Google Scholar] [CrossRef]
- Lurz, P.; Besler, C. Mitral Regurgitation in Cardiogenic Shock: A Novel Target for Transcatheter Therapy? JACC Cardiovasc. Interv. 2021, 14, 12–14. [Google Scholar] [CrossRef]
- Chehab, O.; Roberts-Thomson, R.; Ling, C.N.Y.; Marber, M.; Prendergast, B.D.; Rajani, R.; Redwood, S.R. Secondary mitral regurgitation: Pathophysiology, proportionality and prognosis. Heart 2020, 106, 716–723. [Google Scholar] [CrossRef]
- Payen, D.; de Pont, A.C.; Sakr, Y.; Spies, C.; Reinhart, K.; Vincent, J.L. Sepsis Occurrence in Acutely Ill Patients (SOAP) Investigators: A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit. Care 2008, 12, R74. [Google Scholar] [CrossRef]
- Sheikh, O.; Nguyen, T.; Bansal, S.; Prasad, A. Acute kidney injury in cardiogenic shock: A comprehensive review. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2021, 98, E91–E105. [Google Scholar] [CrossRef]
- van den Akker, J.P.C.; Bakker, J.; Groeneveld, A.B.J.; den Uil, C.A. Risk indicators for acute kidney injury in cardiogenic shock. J. Crit. Care 2019, 50, 11–16. [Google Scholar] [CrossRef]
- 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Valvular-Heart-Disease-Guidelines (accessed on 28 August 2021).
- Tarvasmäki, T.; Haapio, M.; Mebazaa, A.; Sionis, A.; Silva-Cardoso, J.; Tolppanen, H.; Lindholm, M.G.; Pulkki, K.; Parissis, J.; Harjola, V.-P.; et al. Acute kidney injury in cardiogenic shock: Definitions, incidence, haemodynamic alterations, and mortality. Eur. J. Heart Fail. 2018, 20, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, N.; Resta, M.L.; Somaschini, A.; Campodonico, J.; Lucci, C.; Moltrasio, M.; Bonomi, A.; Cornara, S.; Camporotondo, R.; Demarchi, A.; et al. Acute kidney injury and in-hospital mortality in patients with ST-elevation myocardial infarction of different age groups. Int. J. Cardiol. 2021, 344, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosyula, S.; Dunlay, S.M.; Barsness, G.W.; Vallabhajosyula, S.; Vallabhajosyula, S.; Sundaragiri, P.R.; Gersh, B.J.; Jaffe, A.S.; Kashani, K. Temporal trends, predictors, and outcomes of acute kidney injury and hemodialysis use in acute myocardial infarction-related cardiogenic shock. PLoS ONE 2019, 14, e0222894. [Google Scholar] [CrossRef] [PubMed]
- Mezhonov, E.M.; Vialkina, I.A.; Vakulchik, K.A.; Shalaev, S.V. Acute kidney injury in patients with ST-segment elevation acute myocardial infarction: Predictors and outcomes. Saudi J. Kidney Dis. Transplant. 2021, 32, 318–327. [Google Scholar] [CrossRef]
- Writing Committee Members; Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Thorac. Cardiovasc. Surg. 2021, 162, e183–e353. [Google Scholar] [CrossRef]
- Al Younis, S.M.; Hadjileontiadis, L.J.; Stefanini, C.; Khandoker, A.H. Non-invasive technologies for heart failure, systolic and diastolic dysfunction modeling: A scoping review. Front. Bioeng. Biotechnol. 2023, 11, 1261022. [Google Scholar] [CrossRef]
- Torre-Amione, G.; Milo, O.; Kaluski, E.; Vered, Z.; Cotter, G. Whole-body electrical bio-impendance is accurate in non invasive determination of cardiac output: A thermodilution controlled, prospective, double blind evaluation. J. Card. Fail. 2004, 10, 38–39. [Google Scholar] [CrossRef]
- Paredes, O.L.; Shite, J.; Shinke, T.; Watanabe, S.; Otake, H.; Matsumoto, D.; Imuro, Y.; Ogasawara, D.; Sawada, T.; Yokoyama, M. Impedance cardiography for cardiac output estimation: Reliability of wrist-to-ankle electrode configuration. Circ. J. 2006, 70, 1164–1168. [Google Scholar] [CrossRef]
- Tanino, Y.; Shite, J.; Paredes, O.L.; Shinke, T.; Ogasawara, D.; Sawada, T.; Kawamori, H.; Miyoshi, N.; Kato, H.; Yoshino, N.; et al. Whole body bioimpedance monitoring for outpatient chronic heart failure follow up. Circ. J. 2009, 73, 1074–1079. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Emoto, N.; Miyagawa, K.; Nakayama, K.; Kinutani, H.; Tanaka, H.; Shinke, T.; Hirata, K. Noninvasive and simple assessment of cardiac output and pulmonary vascular resistance with whole-body impedance cardiography is useful for monitoring patients with pulmonary hypertension. Circ. J. Off. J. Jpn. Circ. Soc. 2013, 77, 2383–2389. [Google Scholar] [CrossRef]
- Buchholz, I.; Marten, O.; Janssen, M.F. Feasibility and validity of the EQ-5D-3L in the elderly Europeans: A secondary data analysis using SHARE(d) data. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2022, 31, 3267–3282. [Google Scholar] [CrossRef] [PubMed]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2012, 78, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, S117–S314. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Friede, T.; von Bardeleben, R.-S.; Butler, J.; Khan, M.-S.; Diek, M.; Heinrich, J.; Geyer, M.; Placzek, M.; Ferrari, R.; et al. Transcatheter Valve Repair in Heart Failure with Moderate to Severe Mitral Regurgitation. N. Engl. J. Med. 2024. [Google Scholar] [CrossRef]
- Baldus, S.; Doenst, T.; Pfister, R.; Gummert, J.; Kessler, M.; Boekstegers, P.; Lubos, E.; Schröder, J.; Thiele, H.; Walther, T.; et al. Transcatheter Repair versus Mitral-Valve Surgery for Secondary Mitral Regurgitation. N. Engl. J. Med. 2024. [Google Scholar] [CrossRef]
- Anker, M.S.; Porthun, J.; Schulze, P.C.; Rassaf, T.; Landmesser, U. Percutaneous Transcatheter Edge-To-Edge Repair for Functional Mitral Regurgitation in Heart Failure: A Meta-Analysis of 3 Randomized Controlled Trials. J. Am. Coll. Cardiol. 2024. [Google Scholar] [CrossRef]
- Enriquez-Sarano, M.; Akins, C.W.; Vahanian, A. Mitral regurgitation. Lancet 2009, 373, 1382–1394. [Google Scholar] [CrossRef]
- Patsalis, N.; Kreutz, J.; Chatzis, G.; Syntila, S.; Choukeir, M.; Schieffer, B.; Markus, B. Early risk predictors of acute kidney injury and short-term survival during Impella support in cardiogenic shock. Sci. Rep. 2024, 14, 17484. [Google Scholar] [CrossRef]
- McCallum, W.; Sarnak, M.J. Cardiorenal Syndrome in the Hospital. Clin. J. Am. Soc. Nephrol. 2023, 18, 933–945. [Google Scholar] [CrossRef]
- D’ Marco, L. Congestive Nephropathy. Int. J. Environ. Res. Public Health 2022, 19, 2499. [Google Scholar] [CrossRef]
- Palazzuoli, A.; Lombardi, C.; Ruocco, G.; Padeletti, M.; Nuti, R.; Metra, M.; Ronco, C. Chronic kidney disease and worsening renal function in acute heart failure: Different phenotypes with similar prognostic impact? Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 534–548. [Google Scholar] [CrossRef]
- Legrand, M.; Mebazaa, A.; Ronco, C.; Januzzi, J.L. When cardiac failure, kidney dysfunction, and kidney injury intersect in acute conditions: The case of cardiorenal syndrome. Crit. Care Med. 2014, 42, 2109–2117. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Demographics, Characteristics, and Comorbidities | ||||
| Total (n = 45) | eGFR < 35 mL/min (n = 16) | eGFR ≥ 35 mL/min (n = 29) | p Value | |
| Age (years) | 78.7 ± 6.7 | 78.3 ± 7 | 78.9 ± 6.1 | 0.776 |
| Female n (%) | 18 (40) | 7 (43.8) | 18 (72) | 0.237 |
| Male n (%) | 27 (60) | 9 (56.3) | 11 (37.9) | 0.237 |
| BMI | 26.5 ± 5 | 26.1 ± 4.4 | 26.8 ± 5.3 | 0.041 |
| History of aHTN n (%) | 32 (71.1) | 11 (68.8) | 21 (72.4) | 0.654 |
| History of dyslipidemia n (%) | 22 (48.9) | 9 (56.3) | 13 (44.8) | 0.463 |
| History of DM n (%) | 15 (33.3) | 4 (25) | 11 (37.9) | 0.378 |
| Known history of CKD n (%) | 29 (64.4) | 13 (81.3) | 16 (55.2) | 0.080 |
| Atrial fibrillation n (%) | 35 (77.8) | 11 (68.8) | 24 (82.8) | 0.279 |
| CRT n (%) | 10 (22.2) | 4 (25) | 6 (20.7) | 0.739 |
| ICD n (%) | 5 (11.1) | 4 (25) | 1 (3.4) | 0.028 |
| CHD n (%) | 33 (73.3) | 12 (75) | 21 (72.4) | 0.851 |
| COPD n (%) | 12 (26.7) | 7 (43.8) | 5 (17.2) | 0.054 |
| LVEF (%) median [IQR] mean (SD) | 55 [39–56] 47.5 ± 11.2 | 52 [35–56] 47.5 ± 11.5 | 55 [39–56] 47.4 ± 11.1 | 0.6 |
| MR grade 3 n (%) 4 n (%) | 25 (55.6) 20 (44.4) | 9 (56.3) 7 (43.8) | 16 (55.2) 13 (44.8) | 0.095 |
| MR regurgitation volume (mL) | 59.5 [40–72.5] | 53.5 [40.25–77.5] | 59 [38–71.5] | 0.924 |
| MR EROA (cm2) | 0.36 [0.23–0.59] | 0,40 [0.22–0.68] | 0.33 [0.24–0.54] | 0.553 |
| TAPSE (cm) | 21 [19–22.5] | 22 [20–23] | 21 [18.5–22] | 0.443 |
| TKS’ lateral (cm/s) | 12 [10.2–13] | 12 [11.14.5] | 11 [10–12.3] | 0.184 |
| Hemoglobin (g/L) | 115.4 ± 191 | 111.9 ± 18.5 | 117.7 ± 18.1 | 0.007 |
| Hematocrit (L/L) | 0.36 [0.32–0.38] | 0.35 [0.32–0.38] | 0.36 [0.32–0.39] | 0.537 |
| Sodium (mmol/L) | 139.3 ± 3.2 | 139.4 ± 3.03 | 139 ± 3.3 | 0.543 |
| Potassium (mmol/L) | 4.05 [3.65–4.35] | 4.3 [3.8–4.9] | 4.0 [3.6–4.1] | 0.063 |
| NT-proBNP (pg/mL) | 3782 [1725–8513] | 8513 [3859–15,356] | 2046 [1378–4805] | <0.001 |
| Medication | ||||
| Torasemide (mg/d) n = 45 | 15 [10–15] | 15 [10–15] | 15 [10–15] | 1.0 |
| Eplerenone (mg/d) n = 38 | 25 [25–25] | 25 [25–25] | 25 [25–25] | 1.0 |
| Bisoprolol (mg/d) n = 38 | 5 [2.5–5] | 5 [2.5–5] | 5 [2.5–5] | 0.81 |
| Ramipril (mg/d) n = 22 | 5 [5–10] | 5 [5–10] | 5 [5–10] | 0.868 |
| Candesartan (mg/d) n = 23 | 16 [16–24] | 16 [16–22] | 16 [16–32] | 0.506 |
| Dapagliflozine (mg/d) n = 36 | 10 [10–10] | 10 [10–10] | 10 [10–10] | 1.0 |
| Amlodipine (mg/L) n = 37 | 10 [5–10] | 10 [5–10] | 10 [5–10] | 0.15 |
| Hemodynamics | ||||
| CO (L/min) | 4.38 ± 1.58 | 3.94 ± 1.6 | 4.63 ± 1.5 | 0.165 |
| CI (L/min/m2) | 2.36 ± 2.36 | 2.52 ± 0.82 | 2.07 ± 0.69 | 0.055 |
| SVR (N × s/m5) | 1596 [1177–2132] | 1791 [1285–2612] | 1514 [1138–2022] | 0.129 |
| T1 (Pre-Procedure) (n = 45) | T2 (3–5 d Post-Procedure) (n = 45) | p Value | |
|---|---|---|---|
| SAP (mmHg) | 118.89 ± 18.86 | 114.02 ± 18.79 | 0.135 |
| DAP (mmHg) | 67.2 ± 11.65 | 66.09 ± 11.54 | 0.601 |
| MAP (mmHg) | 84.07 ± 12.59 | 81.84 ± 10.81 | 0.284 |
| HR (bpm) | 77.1 ± 26.8 | 80.1 ± 24.1 | 0.549 |
| CO (L/min) | 4.13 [3.09–5.38] | 4.3 [3.86–5.69] | 0.025 |
| CI (L/min/m2) | 2.31 [1.82–2.78] | 2.44 [2.11–2.82] | 0.032 |
| SVR (N × s/m5) | 1765 [1177–2132] | 1427 [2226–3876] | 0.003 |
| eGFR (mL/min) | 46.26 ± 21.56 | 50.38 ± 21.34 | 0.03 |
| MR Grade | 3 [3–4] | 1 [1–1] | <0.001 |
| eGFR < 35 (T1) n = 16 | eGFR < 35 (T2) n = 16 | p Value | eGFR ≥ 35 (T1) n = 29 | eGFR ≥ 35 (T2) n = 29 | p Value | |
|---|---|---|---|---|---|---|
| SAP (mmHg) | 119.56 ± 14.36 | 117.13 ± 16.5 | 0.599 | 118.52 ± 21.18 | 112.21 ± 20.01 | 0.161 |
| DAP (mmHg) | 68.89 ± 7.53 | 67.44 ± 9.85 | 0.579 | 66.28 ± 13.43 | 65.34 ± 12.47 | 0.758 |
| MAP (mmHg) | 85.5 ± 6.82 | 84 ± 8.85 | 0.551 | 83.28 ± 14.92 | 80.66 ± 11.73 | 0.375 |
| HR (bpm) | 74.6 ± 18 | 74.7 ± 13.3 | 0.972 | 78.48 ± 30.77 | 83.07 ± 28.19 | 0.546 |
| CO (L/min) | 3.94 ± 1.6 | 4.47 ± 1.72 | 0.035 | 4.38 [3.27–5.52] | 4.63 [3.93–5.86] | 0.247 |
| CI (L/min/m2) | 2.07 ± 0.69 | 2.34 ± 0.68 | 0.031 | 2.43 [2.01–2.89] | 2.53 [2.2–3.039] | 0.294 |
| SVR (N × s/m5) | 1791 [1285–2612] | 1618 [2205–5654] | 0.007 | 1514 [1138–2022] | 1397 [2233–3793] | 0.061 |
| eGFR (mL/min) | 25.63 ± 6.54 | 33.81 ± 16.05 | 0.018 | 57.66 ± 18.15 | 59.51 ± 18.38 | 0.408 |
| MR Grade | 3 [3–4] | 1 [1–1] | <0.001 | 3 [3–4] | 1 [1–1] | <0.001 |
| Overall Cohort | |||
|---|---|---|---|
| T1 | 3M-FU | p Value | |
| EQ-VAS (%) | 51.7 ± 0.18 | 62.9 ± 0.17 | p < 0.001 |
| EQ-5D-3L index value | 0.44 ± 0.39 | 0.66 ± 0.20 | p < 0.001 |
| eGFR < 35 mL/min | |||
| EQ-VAS (%) | 51.6 ± 0.14 | 60.6 ± 0.18 | 0.015 |
| EQ-5D-3L index value | 0.527 ± 0.13 | 0.61 ± 0.19 | 0.034 |
| eGFR ≥ 35 mL/min | |||
| EQ-VAS (%) | 51.8 ± 0.17 | 64 ± 0.17 | <0.001 |
| EQ-5D-3L index value | 0.475 ± 0.4 | 0.68 ± 0.19 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markus, B.; Kreutz, J.; Chatzis, G.; Syntila, S.; Kuchenbuch, J.; Mueller, C.; Choukeir, M.; Schieffer, B.; Patsalis, N. Mitral Valve Transcatheter Edge-to-Edge Repair (MV-TEER) in Patients with Secondary Mitral Regurgitation Improves Hemodynamics, Enhances Renal Function, and Optimizes Quality of Life in Patients with Advanced Renal Insufficiency. Biomedicines 2024, 12, 2648. https://doi.org/10.3390/biomedicines12112648
Markus B, Kreutz J, Chatzis G, Syntila S, Kuchenbuch J, Mueller C, Choukeir M, Schieffer B, Patsalis N. Mitral Valve Transcatheter Edge-to-Edge Repair (MV-TEER) in Patients with Secondary Mitral Regurgitation Improves Hemodynamics, Enhances Renal Function, and Optimizes Quality of Life in Patients with Advanced Renal Insufficiency. Biomedicines. 2024; 12(11):2648. https://doi.org/10.3390/biomedicines12112648
Chicago/Turabian StyleMarkus, Birgit, Julian Kreutz, Giorgios Chatzis, Styliani Syntila, Jannis Kuchenbuch, Charlotte Mueller, Maryana Choukeir, Bernhard Schieffer, and Nikolaos Patsalis. 2024. "Mitral Valve Transcatheter Edge-to-Edge Repair (MV-TEER) in Patients with Secondary Mitral Regurgitation Improves Hemodynamics, Enhances Renal Function, and Optimizes Quality of Life in Patients with Advanced Renal Insufficiency" Biomedicines 12, no. 11: 2648. https://doi.org/10.3390/biomedicines12112648
APA StyleMarkus, B., Kreutz, J., Chatzis, G., Syntila, S., Kuchenbuch, J., Mueller, C., Choukeir, M., Schieffer, B., & Patsalis, N. (2024). Mitral Valve Transcatheter Edge-to-Edge Repair (MV-TEER) in Patients with Secondary Mitral Regurgitation Improves Hemodynamics, Enhances Renal Function, and Optimizes Quality of Life in Patients with Advanced Renal Insufficiency. Biomedicines, 12(11), 2648. https://doi.org/10.3390/biomedicines12112648