

Mitochondrial Dysfunction and Ion Imbalance in a Rat Model of Hemodialysis-Induced Myocardial Stunning

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Establishment of Animal Model
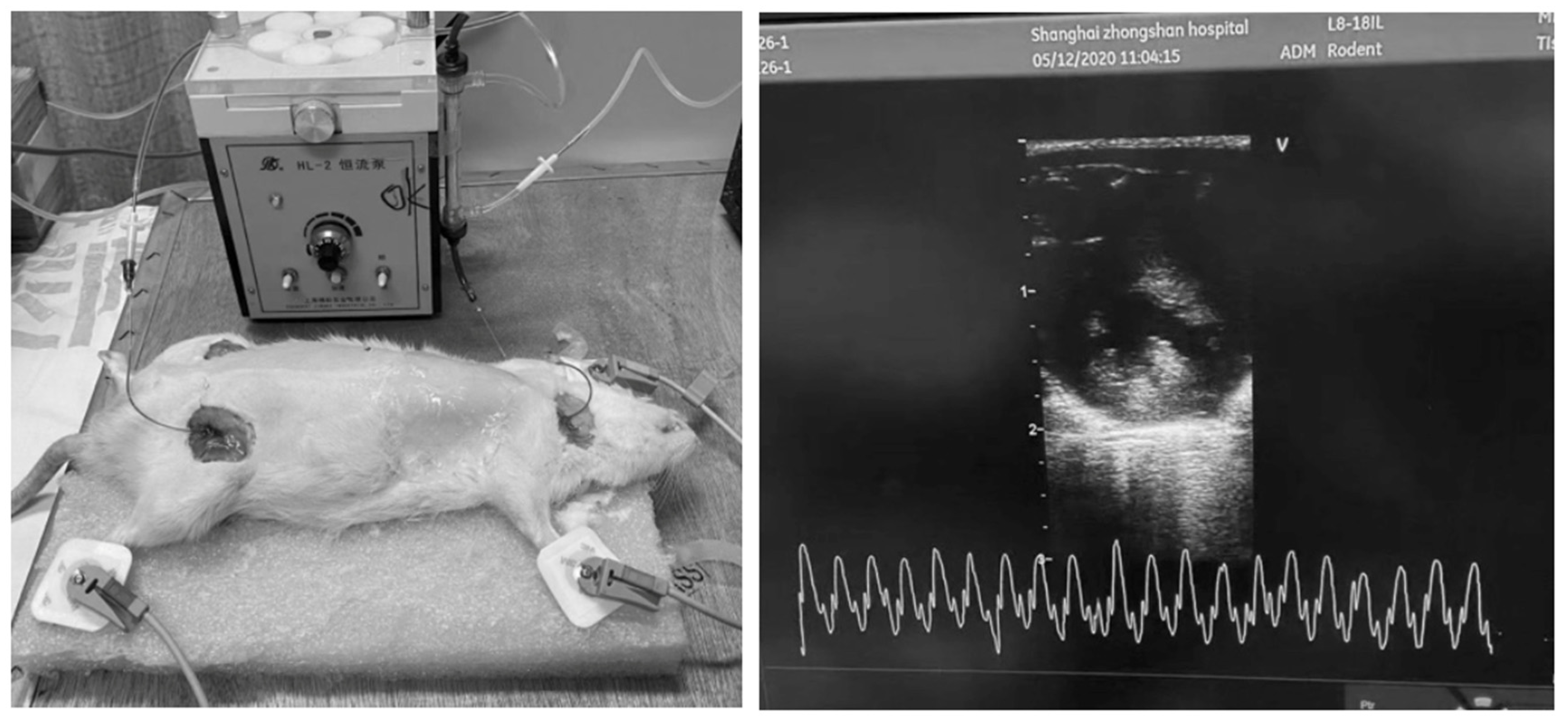
2.2. Vascular Access Creation, Extracorporeal Circulation, and Hemodialysis
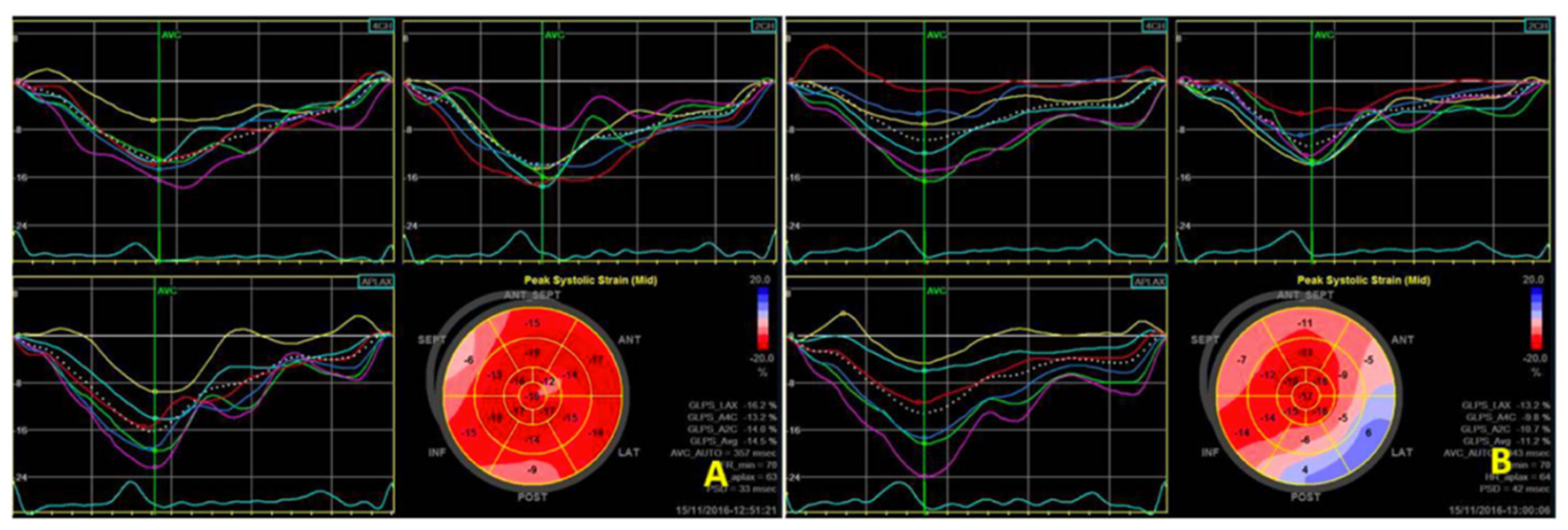
2.3. Echocardiography
2.4. Mitochondrial ATP Channel Intervention
2.5. Sampling and Processing of Experimental Animals
2.6. Grouping of Experimental Animals
2.7. Statistical Analyses
3. Results
3.1. Echocardiography
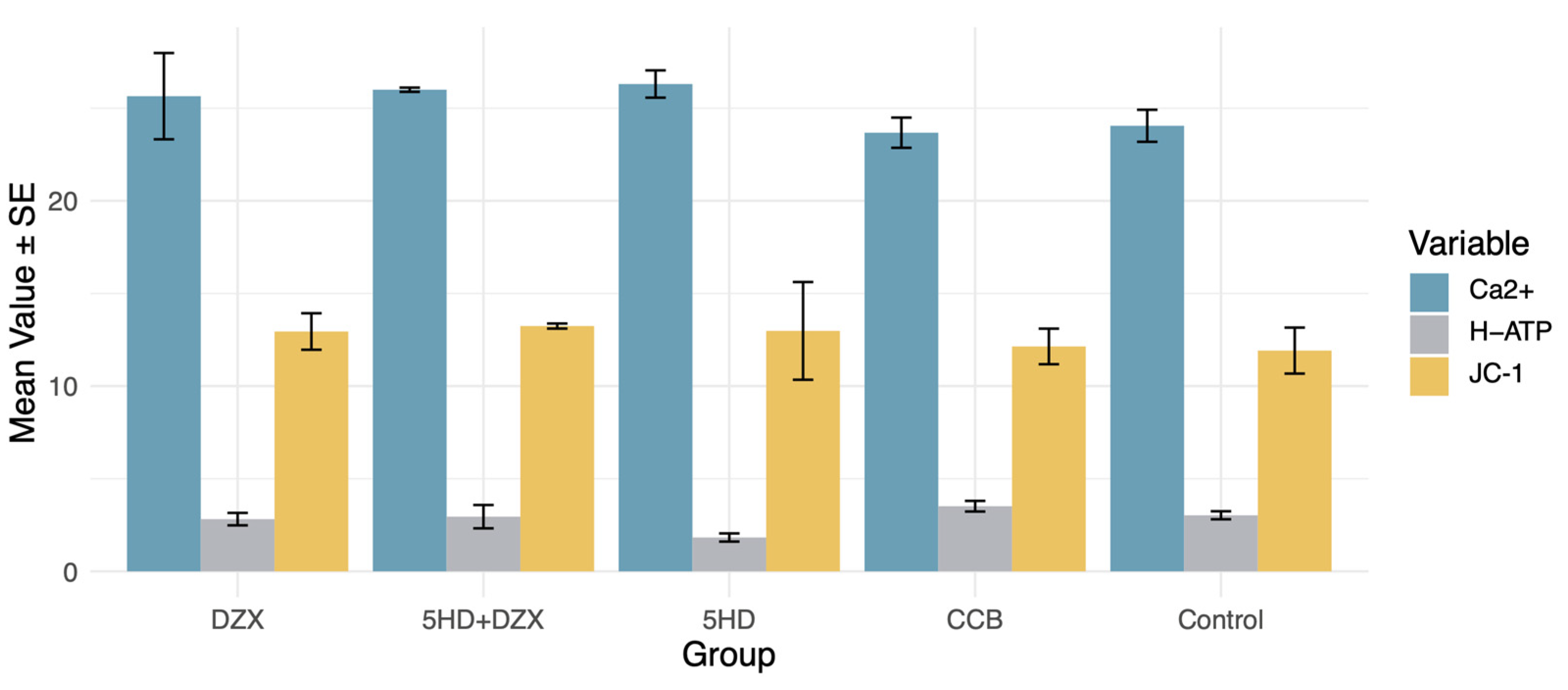
3.2. Effects of K+ and Ca2+ Concentrations on Mitochondrial Energy Metabolism and Myocardial Contraction
3.3. Effects of Mitochondrial ATP Channel Modulators and Calcium Channel Blockers on Mitochondrial Energy Metabolism and Myocardial Stunning
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Chronic Kidney Disease Collaboration. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed]
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wang, Y. Management of Cardiovascular Diseases in Chronic Hemodialysis Patients. Rev. Cardiovasc. Med. 2023, 24, 185. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Zou, X.; Sun, X.; Zhang, C. Coronary Artery Disease in CKD-G5D Patients: An Update. Rev. Cardiovasc. Med. 2023, 24, 227. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Amann, K.; Shoji, T. The Heart and Vascular System in Dialysis. Lancet 2016, 388, 276–284. [Google Scholar] [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The Effects of Lowering LDL Cholesterol with Simvastatin plus Ezetimibe in Patients with Chronic Kidney Disease (Study of Heart and Renal Protection): A Randomised Placebo-Controlled Trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef]
- Ferro, C.J.; Mark, P.B.; Kanbay, M.; Sarafidis, P.; Heine, G.H.; Rossignol, P.; Massy, Z.A.; Mallamaci, F.; Valdivielso, J.M.; Malyszko, J.; et al. Lipid Management in Patients with Chronic Kidney Disease. Nat. Rev. Nephrol. 2018, 14, 727–749. [Google Scholar] [CrossRef]
- Ethier, J.; Bragg-Gresham, J.L.; Piera, L.; Akizawa, T.; Asano, Y.; Mason, N.; Gillespie, B.W.; Young, E.W. Aspirin Prescription and Outcomes in Hemodialysis Patients: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2007, 50, 602–611. [Google Scholar] [CrossRef]
- Calice-Silva, V.; Muenz, D.; Wong, M.M.Y.; McCullough, K.; Charytan, D.; Reichel, H.; Robinson, B.; Stengel, B.; Massy, Z.A.; Pecoits-Filho, R.; et al. International Practice Patterns of Dyslipidemia Management in Patients with Chronic Kidney Disease under Nephrology Care: Is It Time to Review Guideline Recommendations? Lipids Health Dis. 2023, 22, 67. [Google Scholar] [CrossRef]
- Li, H.; Chen, W.; Lin, X.; Chen, W.; Xie, T.; Chen, K.; Hou, S.; Li, H. Influence of Renal Function on the Ability of TyG Index to Predict All-Cause Mortality. Lipids Health Dis. 2023, 22, 193. [Google Scholar] [CrossRef]
- Wang, B.; Jiang, C.; Qu, Y.; Wang, J.; Yan, C.; Zhang, X. Nonlinear Association between Atherogenic Index of Plasma and Chronic Kidney Disease: A Nationwide Cross-Sectional Study. Lipids Health Dis. 2024, 23, 312. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Cao, X.; Zou, J.; Shen, B.; Zhang, X.; Liu, Z.; Lv, W.; Teng, J.; Ding, X. Indoxyl Sulfate, a Valuable Biomarker in Chronic Kidney Disease and Dialysis. Hemodial. Int. 2017, 21, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zou, J.-Z.; Chen, J.; Tan, X.; Xiang, F.-F.; Shen, B.; Hu, J.-C.; Wang, J.-L.; Wang, Y.-Q.; Yu, J.-B.; et al. Association of Trimethylamine N-Oxide with Cardiovascular and All-Cause Mortality in Hemodialysis Patients. Ren. Fail. 2020, 42, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, G.; Yu, X.; Yang, J.; Jiang, A.; Cheng, H.; Fu, J.; Liang, X.; Liu, J.; Lou, J.; et al. Progression of Vascular Calcification and Clinical Outcomes in Patients Receiving Maintenance Dialysis. JAMA Netw. Open 2023, 6, e2310909. [Google Scholar] [CrossRef]
- Assimon, M.M.; Wenger, J.B.; Wang, L.; Flythe, J.E. Ultrafiltration Rate and Mortality in Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2016, 68, 911–922. [Google Scholar] [CrossRef]
- Burton, J.O.; Jefferies, H.J.; Selby, N.M.; McIntyre, C.W. Hemodialysis-Induced Cardiac Injury: Determinants and Associated Outcomes. Clin. J. Am. Soc. Nephrol. 2009, 4, 914–920. [Google Scholar] [CrossRef]
- Assa, S.; Hummel, Y.M.; Voors, A.A.; Kuipers, J.; Westerhuis, R.; de Jong, P.E.; Franssen, C.F.M. Hemodialysis-Induced Regional Left Ventricular Systolic Dysfunction: Prevalence, Patient and Dialysis Treatment-Related Factors, and Prognostic Significance. Clin. J. Am. Soc. Nephrol. 2012, 7, 1615–1623. [Google Scholar] [CrossRef]
- Nie, Y.; Zhang, Z.; Zou, J.; Liang, Y.; Cao, X.; Liu, Z.; Shen, B.; Chen, X.; Ding, X. Hemodialysis-Induced Regional Left Ventricular Systolic Dysfunction: HD-Induced LV Systolic Dysfunction. Hemodial. Int. 2016, 20, 564–572. [Google Scholar] [CrossRef]
- Jefferies, H.J.; Virk, B.; Schiller, B.; Moran, J.; McIntyre, C.W. Frequent Hemodialysis Schedules Are Associated with Reduced Levels of Dialysis-Induced Cardiac Injury (Myocardial Stunning). Clin. J. Am. Soc. Nephrol. 2011, 6, 1326–1332. [Google Scholar] [CrossRef]
- Zuidema, M.Y.; Dellsperger, K.C. Myocardial Stunning with Hemodialysis: Clinical Challenges of the Cardiorenal Patient. Cardiorenal Med. 2012, 2, 125–133. [Google Scholar] [CrossRef]
- Ünlü, S.; Şahinarslan, A.; Sezenöz, B.; Uludağ, O.M.; Gökalp, G.; Seçkin, Ö.; Arınsoy, S.T.; Gülbahar, Ö.; Boyacı, N.B. High-Sensitive Troponin T Increase after Hemodialysis Is Associated with Left Ventricular Global Longitudinal Strain and Ultrafiltration Rate. Cardiol. J. 2020, 27, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Rocha, S.; Nascimento, H.; Valente, M.J.; Catarino, C.; Rocha-Pereira, P.; Sameiro-Faria, M.; Oliveira, J.G.; Madureira, J.; Fernandes, J.C.; et al. Cell-Free DNA as a Marker for the Outcome of End-Stage Renal Disease Patients on Haemodialysis. Clin. Kidney J. 2021, 14, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Tovbin, D.; Novack, V.; Wiessman, M.P.; Abd Elkadir, A.; Zlotnik, M.; Douvdevani, A. Circulating Cell-Free DNA in Hemodialysis Patients Predicts Mortality. Nephrol. Dial. Transpl. 2012, 27, 3929–3935. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, J.; Zheng, Y.; Wang, J.; Wang, Z.; Gu, S.; Tan, J.; Jing, Q.; Yang, H. Uncoupling Protein 3 Mediates H2O2 Preconditioning-Afforded Cardioprotection through the Inhibition of MPTP Opening. Cardiovasc. Res. 2015, 105, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Inoue, I.; Nagase, H.; Kishi, K.; Higuti, T. ATP-Sensitive K+ Channel in the Mitochondrial Inner Membrane. Nature 1991, 352, 244–247. [Google Scholar] [CrossRef]
- O’Rourke, B. Mitochondrial Ion Channels. Annu. Rev. Physiol. 2007, 69, 19–49. [Google Scholar] [CrossRef]
- Schwartz, L.M.; Reimer, K.A.; Crago, M.S.; Jennings, R.B. Pharmacological Preconditioning with Diazoxide Slows Energy Metabolism during Sustained Ischemia. Exp. Clin. Cardiol. 2007, 12, 139–147. [Google Scholar]
- Maffit, S.K.; Sellitto, A.D.; Al-Dadah, A.S.; Schuessler, R.B.; Damiano, R.J.; Lawton, J.S. Diazoxide Maintains Human Myocyte Volume Homeostasis during Stress. J. Am. Heart Assoc. 2012, 1, jah3-e000778. [Google Scholar] [CrossRef]
- Coetzee, W.A. Multiplicity of Effectors of the Cardioprotective Agent, Diazoxide. Pharmacol. Ther. 2013, 140, 167–175. [Google Scholar] [CrossRef]
- Ishida, H.; Hirota, Y.; Genka, C.; Nakazawa, H.; Nakaya, H.; Sato, T. Opening of Mitochondrial K(ATP) Channels Attenuates the Ouabain-Induced Calcium Overload in Mitochondria. Circ. Res. 2001, 89, 856–858. [Google Scholar] [CrossRef]
- Garlid, K.D.; Paucek, P.; Yarov-Yarovoy, V.; Murray, H.N.; Darbenzio, R.B.; D’Alonzo, A.J.; Lodge, N.J.; Smith, M.A.; Grover, G.J. Cardioprotective Effect of Diazoxide and Its Interaction with Mitochondrial ATP-Sensitive K+ Channels. Possible Mechanism of Cardioprotection. Circ. Res. 1997, 81, 1072–1082. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, S.; Prasad, S.M.; Sellitto, A.D.; Schuessler, R.B.; Damiano, R.J.; Lawton, J.S. Myocyte Volume and Function in Response to Osmotic Stress: Observations in the Presence of an Adenosine Triphosphate-Sensitive Potassium Channel Opener. Circulation 2005, 112, I219–I223. [Google Scholar] [CrossRef] [PubMed]
- Dasselaar, J.J.; Slart, R.H.J.A.; Knip, M.; Pruim, J.; Tio, R.A.; McIntyre, C.W.; de Jong, P.E.; Franssen, C.F.M. Haemodialysis Is Associated with a Pronounced Fall in Myocardial Perfusion. Nephrol. Dial. Transpl. 2009, 24, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Burton, J.O.; Jefferies, H.J.; Selby, N.M.; McIntyre, C.W. Hemodialysis-Induced Repetitive Myocardial Injury Results in Global and Segmental Reduction in Systolic Cardiac Function. Clin. J. Am. Soc. Nephrol. 2009, 4, 1925–1931. [Google Scholar] [CrossRef]
- Selby, N.M.; McIntyre, C.W. Peritoneal Dialysis Is Not Associated with Myocardial Stunning. Perit. Dial. Int. 2011, 31, 27–33. [Google Scholar] [CrossRef]
- Canaud, B.; Kooman, J.P.; Selby, N.M.; Taal, M.W.; Francis, S.; Maierhofer, A.; Kopperschmidt, P.; Collins, A.; Kotanko, P. Dialysis-Induced Cardiovascular and Multiorgan Morbidity. Kidney Int. Rep. 2020, 5, 1856–1869. [Google Scholar] [CrossRef]
- Nie, Y.; Zou, J.; Liang, Y.; Shen, B.; Liu, Z.; Cao, X.; Chen, X.; Ding, X. Electrocardiographic Abnormalities and QTc Interval in Patients Undergoing Hemodialysis. PLoS ONE 2016, 11, e0155445. [Google Scholar] [CrossRef]
- Brunelli, S.M.; Du Mond, C.; Oestreicher, N.; Rakov, V.; Spiegel, D.M. Serum Potassium and Short-Term Clinical Outcomes Among Hemodialysis Patients: Impact of the Long Interdialytic Interval. Am. J. Kidney Dis. 2017, 70, 21–29. [Google Scholar] [CrossRef]
- Yusuf, A.A.; Hu, Y.; Singh, B.; Menoyo, J.A.; Wetmore, J.B. Serum Potassium Levels and Mortality in Hemodialysis Patients: A Retrospective Cohort Study. Am. J. Nephrol. 2016, 44, 179–186. [Google Scholar] [CrossRef]
- Sacher, F.; Jesel, L.; Borni-Duval, C.; De Precigout, V.; Lavainne, F.; Bourdenx, J.-P.; Haddj-Elmrabet, A.; Seigneuric, B.; Keller, A.; Ott, J.; et al. Cardiac Rhythm Disturbances in Hemodialysis Patients: Early Detection Using an Implantable Loop Recorder and Correlation With Biological and Dialysis Parameters. JACC Clin. Electrophysiol. 2018, 4, 397–408. [Google Scholar] [CrossRef]
- Ohnishi, T.; Kimachi, M.; Fukuma, S.; Akizawa, T.; Fukuhara, S. Postdialysis Hypokalemia and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis. Clin. J. Am. Soc. Nephrol. 2019, 14, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Ferrey, A.; You, A.S.; Kovesdy, C.P.; Nakata, T.; Veliz, M.; Nguyen, D.V.; Kalantar-Zadeh, K.; Rhee, C.M. Dialysate Potassium and Mortality in a Prospective Hemodialysis Cohort. Am. J. Nephrol. 2018, 47, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Mancini, E.; London, G.; Mercadal, L.; Fessy, H.; Perrone, B.; Cagnoli, L.; Grandi, E.; Severi, S.; Cavalcanti, S. Patients with Complex Arrhythmias during and after Haemodialysis Suffer from Different Regimens of Potassium Removal. Nephrol. Dial. Transpl. 2008, 23, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Redaelli, B.; Locatelli, F.; Limido, D.; Andrulli, S.; Signorini, M.G.; Sforzini, S.; Bonoldi, L.; Vincenti, A.; Cerutti, S.; Orlandini, G. Effect of a New Model of Hemodialysis Potassium Removal on the Control of Ventricular Arrhythmias. Kidney Int. 1996, 50, 609–617. [Google Scholar] [CrossRef]
- Sasaki, N.; Sato, T.; Ohler, A.; O’Rourke, B.; Marbán, E. Activation of Mitochondrial ATP-Dependent Potassium Channels by Nitric Oxide. Circulation 2000, 101, 439–445. [Google Scholar] [CrossRef]
- Xu, W.; Liu, Y.; Wang, S.; McDonald, T.; Van Eyk, J.E.; Sidor, A.; O’Rourke, B. Cytoprotective Role of Ca2+- Activated K+ Channels in the Cardiac Inner Mitochondrial Membrane. Science 2002, 298, 1029–1033. [Google Scholar] [CrossRef]
- Endoh, M. Cardiac Ca2+ Signaling and Ca2+ Sensitizers. Circ. J. 2008, 72, 1915–1925. [Google Scholar] [CrossRef]
- Williams, G.S.B.; Smith, G.D.; Sobie, E.A.; Jafri, M.S. Models of Cardiac Excitation–Contraction Coupling in Ventricular Myocytes. Math. Biosci. 2010, 226, 1–15. [Google Scholar] [CrossRef]
- Santulli, G.; Pagano, G.; Sardu, C.; Xie, W.; Reiken, S.; D’Ascia, S.L.; Cannone, M.; Marziliano, N.; Trimarco, B.; Guise, T.A.; et al. Calcium Release Channel RyR2 Regulates Insulin Release and Glucose Homeostasis. J. Clin. Investig. 2015, 125, 1968–1978. [Google Scholar] [CrossRef]
- Sardu, C.; Santulli, G.; Guerra, G.; Trotta, M.C.; Santamaria, M.; Sacra, C.; Testa, N.; Ducceschi, V.; Gatta, G.; Amico, M.D.; et al. Modulation of SERCA in Patients with Persistent Atrial Fibrillation Treated by Epicardial Thoracoscopic Ablation: The CAMAF Study. J. Clin. Med. 2020, 9, 544. [Google Scholar] [CrossRef]
- Langote, A.; Ahearn, M.; Zimmerman, D. Dialysate Calcium Concentration, Mineral Metabolism Disorders, and Cardiovascular Disease: Deciding the Hemodialysis Bath. Am. J. Kidney Dis. 2015, 66, 348–358. [Google Scholar] [CrossRef] [PubMed]
- van der Sande, F.M.; ter Meulen, K.J.A.; Kotanko, P.; Kooman, J.P. Dialysate Calcium Levels: Do They Matter? Blood Purif. 2019, 47, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Jennings, R.B. Historical Perspective on the Pathology of Myocardial Ischemia/Reperfusion Injury. Circ. Res. 2013, 113, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Ji, Q.; Zou, Z.; Zeng, Q.; Ren, T.; Chen, W.; Yan, Z.; Shen, D.; Li, Y.; Peng, F.; et al. Effect of Delayed Remote Ischemic Preconditioning on Acute Kidney Injury and Outcomes in Patients Undergoing Cardiac Surgery: A Randomized Clinical Trial. Circulation 2024. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Pre-Dialysis | 30 Min | 60 Min | 90 Min | Post-Dialysis | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| CS | LS | CS | LS | CS | LS | CS | LS | CS | LS | |
| DZX | −13.8 | −14 | −14 | −8.8 | −19.4 | −15.1 | −17.9 | −12.8 | −14.2 | −7.8 |
| DZX + 5HD | −20.4 | −16.9 | −18.5 | −14.4 | −18.4 | −12.7 | −21.7 | −14.3 | −17 | −13.5 |
| 5HD | −16.1 | −12.3 | −7.6 | 0 | −4.3 | −4.5 | −15.1 | −12.8 | −14.6 | −5.9 |
| CCB | −18.3 | −17.1 | −26.6 | −18.1 | −17.5 | −19 | −19.5 | −18 | −22.7 | −13.7 |
| Control | −18.6 | −20.6 | −25.1 | −23.8 | −25 | −18.4 | −21.7 | −8.9 | −20.1 | −14.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nie, Y.; Lin, L.; Yang, Q.; Hu, J.; Sun, M.; Xiang, F.; Cao, X.; Yu, J.; Wang, Y.; Teng, J.; et al. Mitochondrial Dysfunction and Ion Imbalance in a Rat Model of Hemodialysis-Induced Myocardial Stunning. Biomedicines 2024, 12, 2402. https://doi.org/10.3390/biomedicines12102402
Nie Y, Lin L, Yang Q, Hu J, Sun M, Xiang F, Cao X, Yu J, Wang Y, Teng J, et al. Mitochondrial Dysfunction and Ion Imbalance in a Rat Model of Hemodialysis-Induced Myocardial Stunning. Biomedicines. 2024; 12(10):2402. https://doi.org/10.3390/biomedicines12102402
Chicago/Turabian StyleNie, Yuxin, Liyu Lin, Qiang Yang, Jiachang Hu, Minmin Sun, Fangfang Xiang, Xuesen Cao, Jinbo Yu, Yaqiong Wang, Jie Teng, and et al. 2024. "Mitochondrial Dysfunction and Ion Imbalance in a Rat Model of Hemodialysis-Induced Myocardial Stunning" Biomedicines 12, no. 10: 2402. https://doi.org/10.3390/biomedicines12102402
APA StyleNie, Y., Lin, L., Yang, Q., Hu, J., Sun, M., Xiang, F., Cao, X., Yu, J., Wang, Y., Teng, J., Ding, X., Shen, B., & Zhang, Z. (2024). Mitochondrial Dysfunction and Ion Imbalance in a Rat Model of Hemodialysis-Induced Myocardial Stunning. Biomedicines, 12(10), 2402. https://doi.org/10.3390/biomedicines12102402