
Hemoadsorption Therapy for Critically Ill Patients with Acute Liver Dysfunction: A Meta-Analysis and Systematic Review
 , , , ,
, , , , 
Abstract
:1. Introduction
Objectives
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Collection Process
2.5. Study Risk of Bias and Certainty of Evidence Assessment
2.6. Statistical Analysis
3. Results
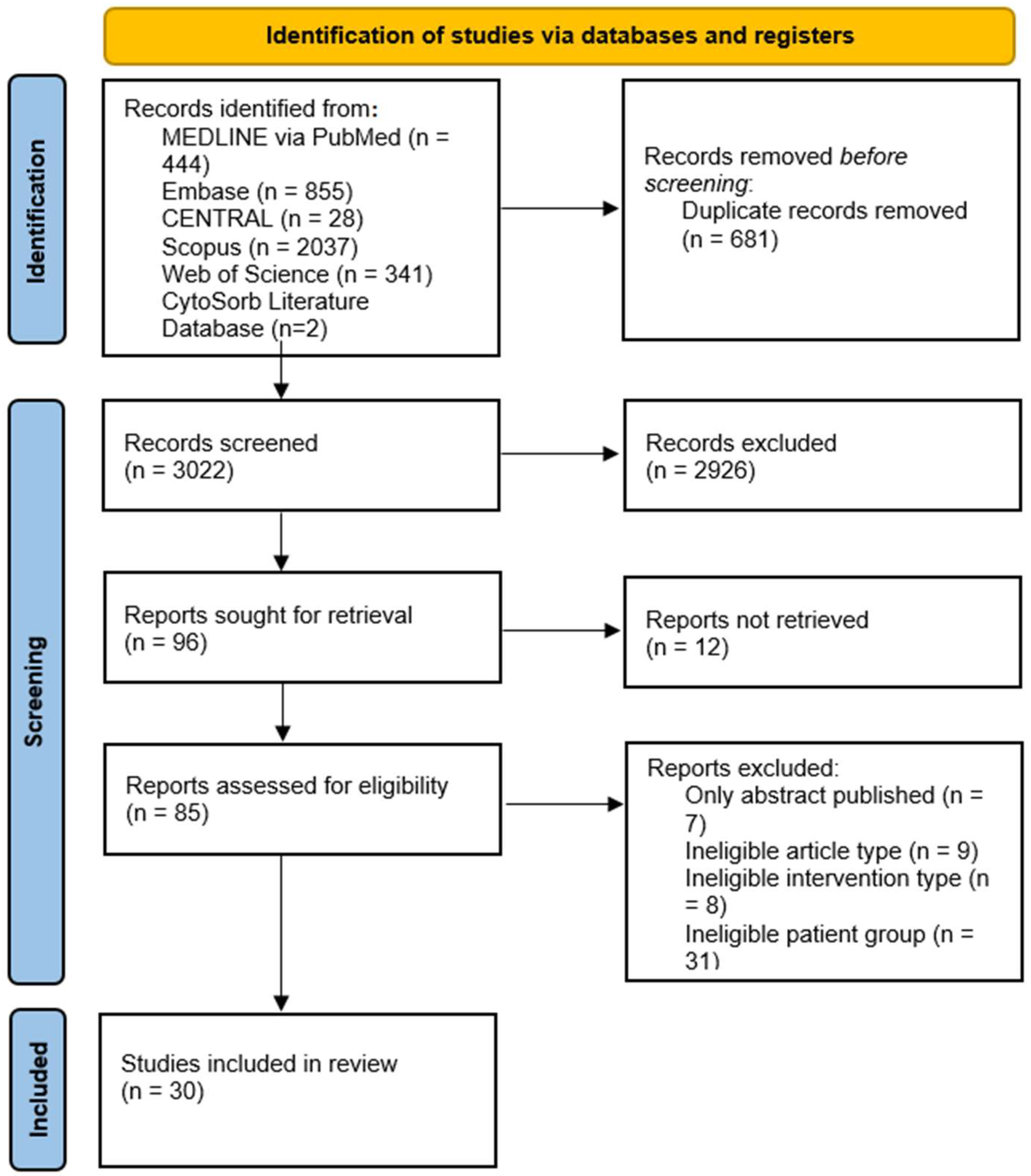
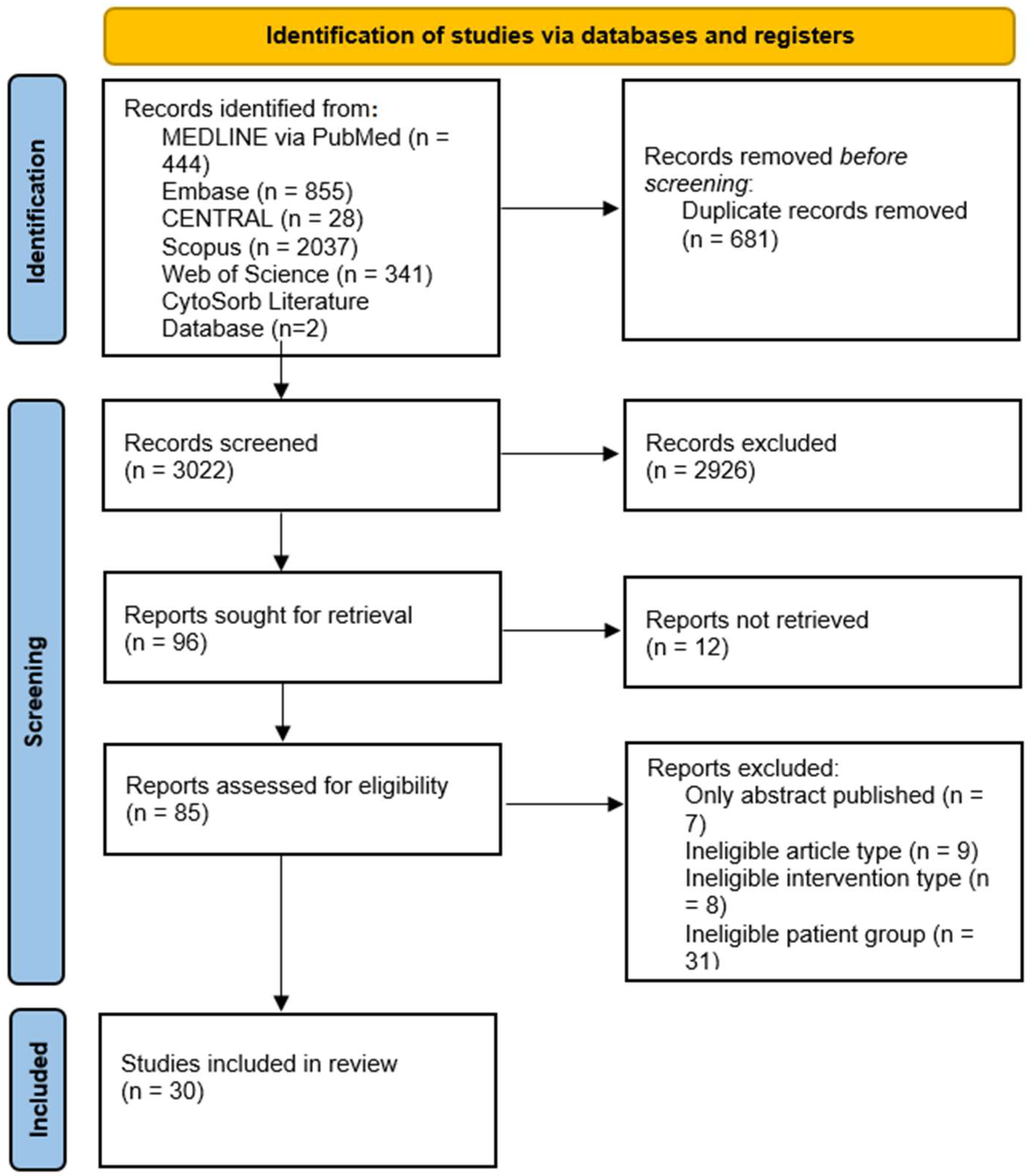
3.1. Study Selection and Characteristics
3.2. Main Characteristics of the Included Studies
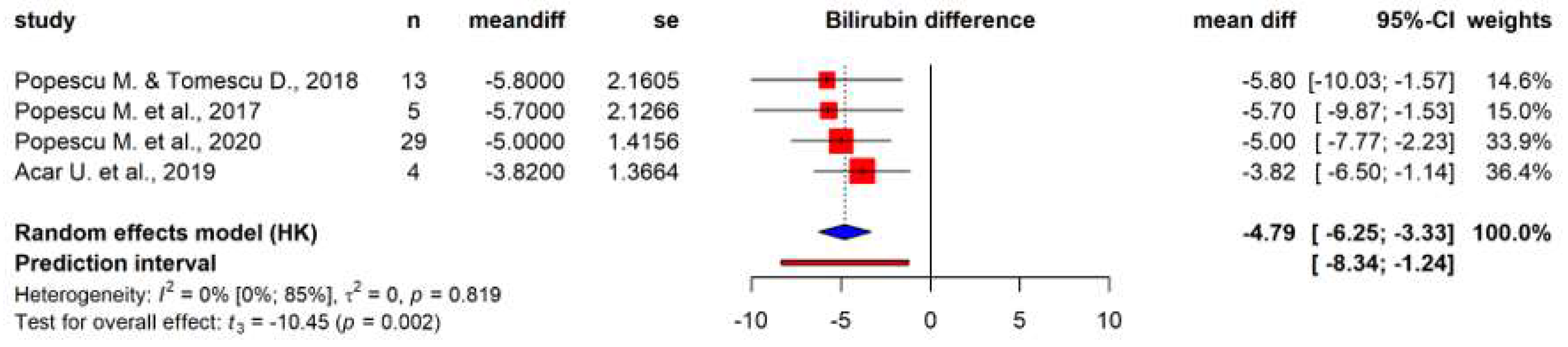
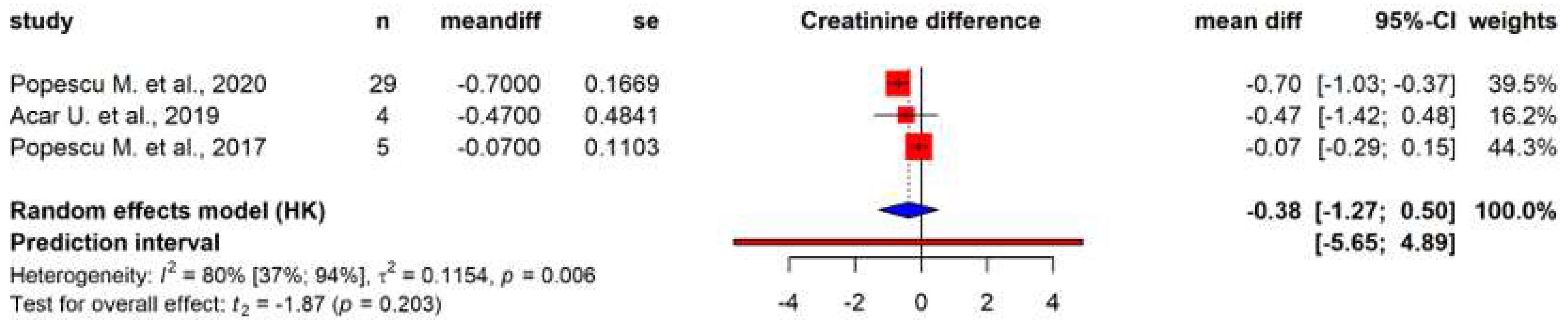
3.3. Primary Outcomes
3.4. Other Outcomes
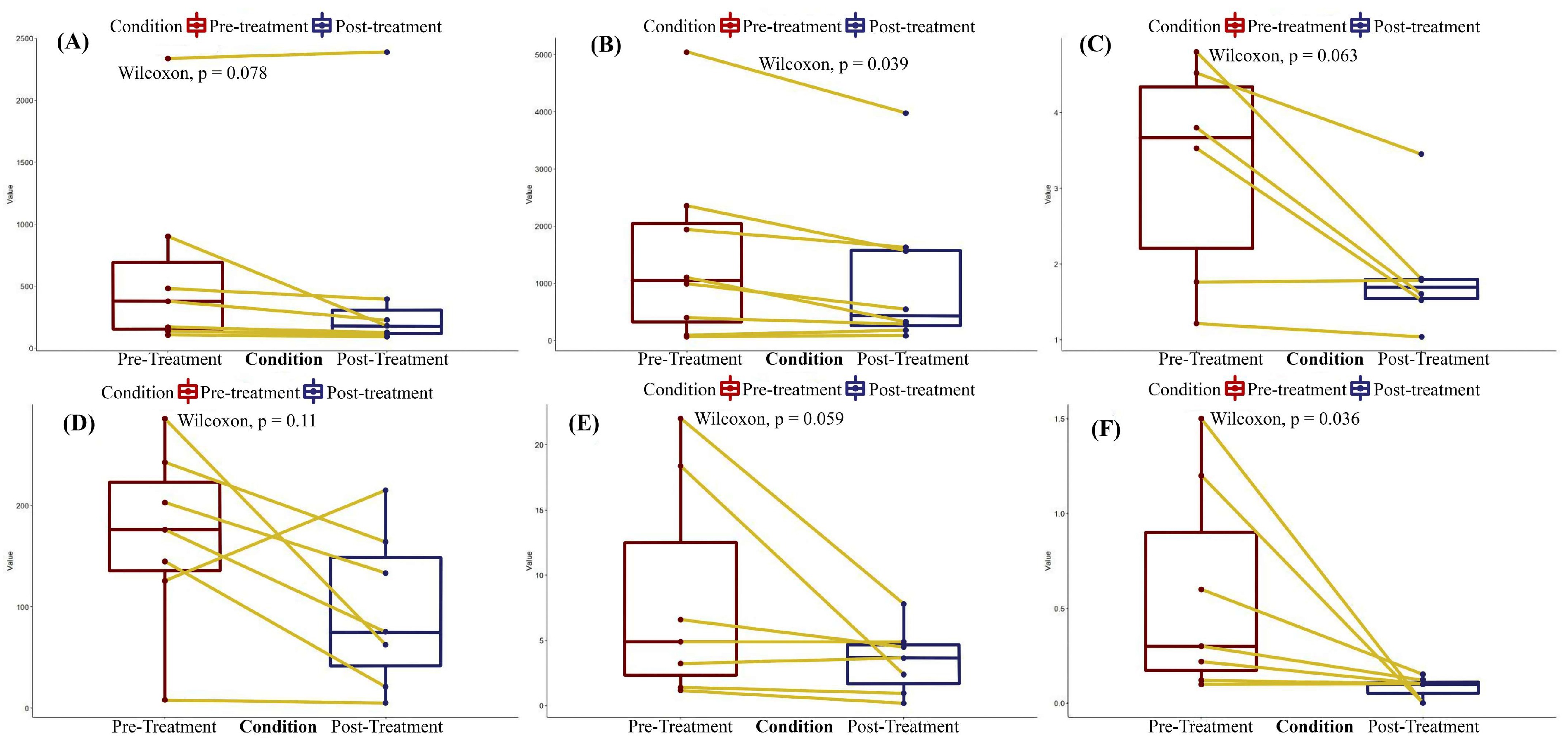
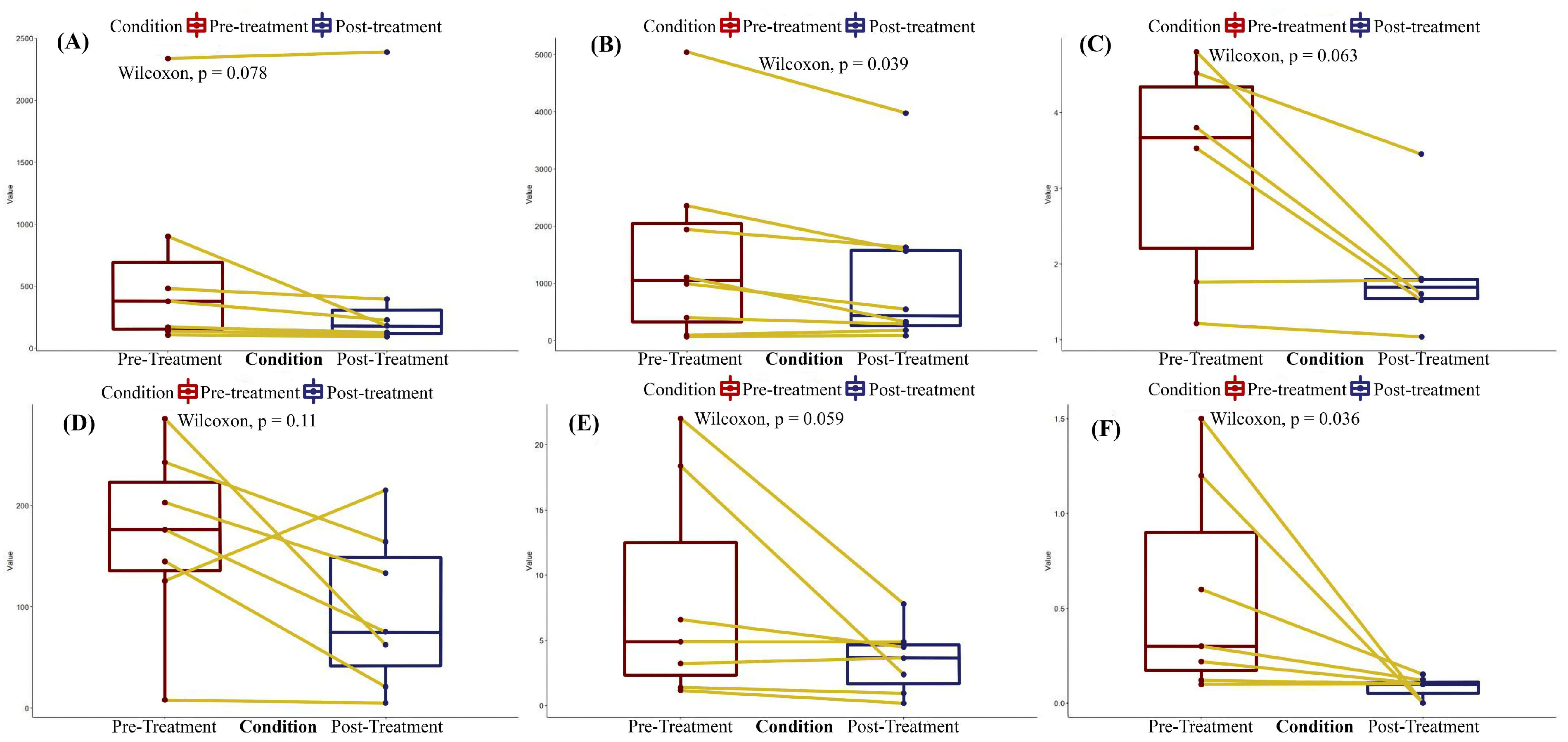
3.4.1. Post-Treatment Organ Function Parameters
3.4.2. Changes in Vital Organ Function
3.4.3. Safety Outcomes
3.5. Risk of Bias and Level of Evidence Certainty Assessments
4. Discussion
4.1. Devices
4.1.1. CytoSorb
4.1.2. Coupled Plasma Filtration Adsorption
4.1.3. oXiris
4.2. Outcomes
4.2.1. Bilirubin
4.2.2. ALT, AST, Bile Acid, Ammonia
4.2.3. Clinical Outcomes and Safety
4.3. Implications for Research and Practice
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year of Publication | Bilirubin (mg/dL): Pre-Treatment/Post-Treatment | CRP (mg/dL): Pre-Treatment/Post-Treatment | ALT (U/L): Pre-Treatment/Post-Treatment | AST (U/L): Pre-Treatment/Post-Treatment | Creatinine (mg/dL): Pre-Treatment/Post-Treatment | Ammonia (μmol/L): Pre-Treatment/Post-Treatment | LDH (U/L): Pre-Treatment/Post-Treatment | Vasopressor Dosage (mcg/kg/min) | Mortality | Changes in Vital Organ Function: Pre-Treatment/Post-Treatment |
|---|---|---|---|---|---|---|---|---|---|---|
| Gunasekera, A.M., 2022 [25] | 4.9/4.9 | - | 2338/2390 | 5049/3795 | 4.8/1.8 | - | - | - | 0 | - |
| Ruiz-Rodriguez, J.C., 2022 [26] | 22/7.8 | 7.7/4.94 | - | 1938/1625 | 7.03/CRRT | - | - | 1.5/0 | 0 * | SOFA Score: 15/16 |
| Cazzato, M.T., 2019 [27] | 3.22/4.99 | - | - | - | 3.53/1.52 | 67/57 | - | 0.16/0.01 | 0 | SOFA Score: 4/2 |
| Daza, J.L., 2022 [28] | - | 145/21 | 900/179 | 1100/320 | 3.8/1.6 | - | 670/178 | 1.2/0 | 1 | - |
| Hinz, B., 2015 [29] | 6.58/5.88 | 203.2/133.4 | 107.4/100.8 | 80.4/87.6 | 1.76/1.78 | - | - | 0.3/0.15 | 0 | - |
| Köhler, T., 2021 [30] | 1.17/0.19 | - | - | - | - | - | - | 0.22/0.1 | 0 | SOFA Score: 12/6 |
| Lau, C.W.M., 2021 [31] | - | 243/164 | - | - | - | - | - | - | 0 | - |
| Li, Y., 2020 [32] | - | - | - | - | - | - | - | - | 0 | CLIF Score: 63/43 |
| Manohar, V., 2017 [33] | - | 176.15/74.97 | 378.5/226.9 | 992.5/540.1 | - | - | - | 0.1/0.1 | 0 | - |
| Markovic, M., 2020 [34] | - | 125.5/214.9 | 482/393 | 2355/1561 | 4.52/3.45 | - | - | 0.6/0.15 | 1 | APACHE-II Score: 35/60 |
| Moretti, R., 2011 [35] | - | - | - | - | - | - | - | - | 0 | - |
| Piwowarczyk, P., 2019 [36] | 18.41/2.4 | - | - | - | - | - | - | - | 0 | SOFA Score: 16/10 |
| Tomescu, D., 2018 [37] | - | - | - | - | - | - | - | - | 0 | - |
| Wiegele, M., 2015 [38] | 1.4/0.94 | - | 137/121 | 395/285 | 1.21/1.04 | - | - | 0.12/0.1 | 0 | - |
| Lévai, T., 2019 [39] | - | - | - | - | - | - | - | - | 0 | - |
| Manini, E., 2019 [40] | - | - | - | - | - | - | - | - | 0 | - |
| Popescu, M., 2017 [41] | - | - | - | - | - | - | - | - | 0 | |
| Kogelman, K., 2021 [42] | - | 285.9/62.6 | - | 13,300/198 | 1.83/no data | - | - | - | 0 * | SAPS II Score: 56/37 |
| Breitkopf, R., 2020 [43] | - | - | - | - | - | - | - | - | 0 | Glasgow Coma Scale: 13/15 |
| Ullo, I., 2017 [44] | - | - | - | - | - | - | - | - | 2 | |
| Popescu, M., 2017 [45] | 17.5 ± 7.9/11.8 ± 6.7 | - | - | - | 0.83 ± 0.41/0.76 ± 0.31 | - | - | - | 0 | |
| Popescu, M. and Tomescu, D., 2018 [46] | 23.6 ± 12.9/17.8 ± 11.2 | - | - | - | - | - | - | - | 0 | |
| Maggi, U., 2013 [47] | - | - | - | - | - | - | - | - | 0 | |
| Popescu, M., 2020 [48] | 14.2 ± 12.6/9.2 ± 9.1 | - | - | - | 1.9 ± 1.4/1.2 ± 0.8 | - | - | - | 11 | CLIF-SOFA Score: 12.0 ± 2.1/10.0 ± 2.6 |
| Dhokia, V.D., 2019 [49] | - | - | - | - | - | - | - | - | 0 | - |
| Acar, U., 2019 [50] | 18.14 ± 4.47/14.32 ± 4.1 | 979 ± 667/982 ± 611 | 117.88 ± 67.10/119.66 ± 73.79 | 180.11 ± 115.10/153.44 ± 78.21 | 347.11 ± 160.34/298.55 ± 53.09 | 0.02 ± 0.04/0.59 ± 1.50 | 3 | - | ||
| Ocskay, K., 2021 [18] | - | - | - | - | - | - | - | - | 65 | SOFA Score: mean = 0.5 (n = 73) |
| Niu, D.G., 2019 [51] | - | - | - | - | - | - | - | - | 14 | |
| Scharf, C., 2021 [52] | - | - | 614 ± 1707/395 ± 1112 | 1512 ± 4338/1033 ± 3003 | - | - | - | - | 10 ** | SAPS II: 6 ± 9 |
| Praxenthaler, J., 2022 [53] | - | - | - | - | - | - | - | - | - | - |
References
- Kanjo, A.; Ocskay, K.; Gede, N.; Kiss, S.; Szakács, Z.; Párniczky, A.; Mitzner, S.; Stange, J.; Hegyi, P.; Molnár, Z. Efficacy and safety of liver support devices in acute and hyperacute liver failure: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 4189. [Google Scholar] [CrossRef]
- Sakr, Y.; Lobo, S.M.; Moreno, R.P.; Gerlach, H.; Ranieri, V.M.; Michalopoulos, A.; Vincent, J.L.; SOAP Investigators. Patterns and early evolution of organ failure in the intensive care unit and their relation to outcome. Crit. Care 2012, 16, R222. [Google Scholar] [CrossRef] [PubMed]
- Bingold, T.M.; Lefering, R.; Zacharowski, K.; Meybohm, P.; Waydhas, C.; Rosenberger, P.; Scheller, B.; Care Registry Group. Individual Organ Failure and Concomitant Risk of Mortality Differs According to the Type of Admission to ICU—A Retrospective Study of SOFA Score of 23,795 Patients. PLoS ONE 2015, 10, e0134329. [Google Scholar] [CrossRef] [PubMed]
- Kramer, L.; Jordan, B.; Druml, W.; Bauer, P.; Metnitz, P.; DEAA for the Austrian Epidemiologic Study on Intensive Care; ASDI Study Group. Incidence and prognosis of early hepatic dysfunction in critically ill patients—A prospective multicenter study. Crit. Care Med 2007, 35, 1099-e7. [Google Scholar] [CrossRef] [PubMed]
- Geier, A.; Fickert, P.; Trauner, M. Mechanisms of Disease: Mechanisms and clinical implications of cholestasis in sepsis. Nat. Rev. Gastroenterol. Hepatol. 2006, 3, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Lu, K. Cellular Pathogenesis of Hepatic Encephalopathy: An Update. Biomolecules 2023, 13, 396. [Google Scholar] [CrossRef] [PubMed]
- Allameh, A.; Niayesh-Mehr, R.; Aliarab, A.; Sebastiani, G.; Pantopoulos, K. Oxidative Stress in Liver Pathophysiology and Disease. Antioxidants 2023, 12, 1653. [Google Scholar] [CrossRef]
- Vega, S.; Neira, J.L.; Marcuello, C.; Lostao, A.; Abian, O.; Velazquez-Campoy, A. NS3 protease from hepatitis C virus: Biophysical studies on an intrinsically disordered protein domain. Int. J. Mol. Sci. 2013, 14, 13282–13306. [Google Scholar] [CrossRef]
- Recknagel, P.; Gonnert, F.A.; Westermann, M.; Lambeck, S.; Lupp, A.; Rudiger, A.; Dyson, A.; Carré, J.E.; Kortgen, A.; Krafft, C.; et al. Liver Dysfunction and Phosphatidylinositol-3-Kinase Signalling in Early Sepsis: Experimental Studies in Rodent Models of Peritonitis. PLoS Med. 2012, 9, e1001338. [Google Scholar] [CrossRef]
- Moseley, R.H. Sepsis and cholestasis. Clin. Liver Dis. 2004, 8, 83–94. [Google Scholar] [CrossRef]
- Ong, K.L.; Allison, M.A.; Cheung, B.M.; Wu, B.J.; Barter, P.J.; Rye, K.A. The relationship between total bilirubin levels and total mortality in older adults: The United States National Health and Nutrition Examination Survey (NHANES) 1999–2004. PLoS ONE 2014, 9, e94479. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Pastor, C.M.; Suter, P.M. Hepatic hemodynamics and cell functions in human and experimental sepsis. Anesth. Analg. 1999, 89, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Stravitz, R.T.; Kramer, A.H.; Davern, T.; Shaikh, A.O.S.; Caldwell, S.H.; Mehta, R.L.; Blei, A.T.; Fontana, R.J.; McGuire, B.M.; Rossaro, L.; et al. Intensive care of patients with acute liver failure: Recommendations of the U.S. Acute Liver Failure Study Group. Crit. Care Med. 2007, 35, 2498–2508. [Google Scholar] [CrossRef]
- Rugg, C.; Klose, R.; Hornung, R.; Innerhofer, N.; Bachler, M.; Schmid, S.; Fries, D.; Ströhle, M. Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective ‘Genetic’ Matched Analysis. Biomedicines 2020, 8, 539. [Google Scholar] [CrossRef]
- Hawchar, F.; László, I.; Öveges, N.; Trásy, D.; Ondrik, Z.; Molnar, Z. Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study. J. Crit. Care 2018, 49, 172–178. [Google Scholar] [CrossRef]
- Brouwer, W.P.; Duran, S.; Kuijper, M.; Ince, C. Hemoadsorption with CytoSorb shows a decreased observed versus expected 28-day all-cause mortality in ICU patients with septic shock: A propensity-score-weighted retrospective study. Crit. Care 2019, 23, 317. [Google Scholar] [CrossRef]
- Ocskay, K.; Tomescu, D.; Faltlhauser, A.; Jacob, D.; Friesecke, S.; Malbrain, M.; Kogelmann, K.; Bogdanski, R.; Bach, F.; Fritz, H.; et al. Hemoadsorption in ‘Liver Indication’—Analysis of 109 Patients’ Data from the CytoSorb International Registry. J. Clin. Med. 2021, 10, 5182. [Google Scholar] [CrossRef]
- Julian Higgins, J.T.; Chandler, J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; Cochrane, Canada. 2019. Available online: https://training.cochrane.org/handbook/current (accessed on 29 August 2020).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 21 February 2022).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University and Evidence Prime: Hamilton, Canada, 2022. Available online: https://gradepro.org (accessed on 23 December 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 23 December 2023).
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide; Chapman & Hall/CRC Press: Boca Raton, FL, USA; London, UK, 2021; ISBN 978-0-367-61007-4. [Google Scholar]
- Gunasekera, A.M.; Eranthaka, U.; Priyankara, D.; Kalupahana, R. A rare case of acute liver failure with intrahepatic cholestasis due to dengue hemorrhagic fever: CytoSorb®® and plasma exchange aided in the recovery: Case report. BMC Infect. Dis. 2022, 22, 938. [Google Scholar] [CrossRef]
- Ruiz-Rodríguez, J.C.; Chiscano-Camón, L.; Ruiz-Sanmartin, A.; Palmada, C.; Bajaña, I.; Iacoboni, G.; Bonilla, C.; García-Roche, A.; Plata-Menchaca, P.E.; Maldonado, C.; et al. Case report: Cytokine hemoadsorption in a case of hemophagocytic lymphohistiocytosis secondary to extranodal NK/T-cell lymphoma. Front. Med. 2022, 9, 925751. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, M.T. CytoSorb as an Organ Support Therapy during Acute Liver Failure after Hepatic Resection: A Case Report; Poster presented at: Workshop Purification Therapies—Le Idee per la Ricerca Clinica, Italy, 2019. Available online: https://www.purificationtherapies.com/wp-content/uploads/01/16-2/P30_Poster_CYTO_Pellis_Case%20Report.pdf (accessed on 21 February 2022).
- Daza, J.L.; Cruz, Y.D.L.; Gutierrez, G.; Sarzuri, H.; Guarnizo, N.; Alexander Ariza, A.; Marin, L. Combined Application of Cytosorb and Sustained Low Efficiency Dialysis (SLED) in Critical Patients. Ann. Case Rep. 2022, 7, 807. [Google Scholar] [CrossRef]
- Hinz, B.; Jauch, O.; Noky, T.; Friesecke, S.; Abel, P.; Kaiser, R. CytoSorb, a Novel Therapeutic Approach for Patients with Septic Shock: A Case Report. Int. J. Artif. Organs 2015, 38, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Köhler, T.; Pletz, M.W.; Altmann, S.; Kirchner, C.; Schwier, E.; Henzler, D.; Winde, G.; Eickmeyer, C. Pericarditis Caused by Enterococcus faecium with Acute Liver Failure Treated by a Multifaceted Approach including Antimicrobials and Hemoadsorption. Case Rep. Crit. Care 2021, 2021, 8824050. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.W.M.; Tam, C.W.Y.; Shum, H.P. Acute Liver Ischemia Secondary to Acute Severe Pancreatitis: A Case Report. J. GHR 2021, 10, 3599–3603. [Google Scholar]
- Li, Y.; Zhou, L.; Yang, L.; Yuan, F. Septic shock after liver transplantation successfully treated with endotoxin and cytokine adsorption continuous renal replacement therapy: A case report and literature review. J. Int. Med. Res. 2020, 48, 0300060520940439. [Google Scholar] [CrossRef] [PubMed]
- Manohar, V.; Raj, S.; Sreekrishnan, T.P.; Gireesh Kumar, K.P. Cytokine hemoadsorption therapy—An adjuvant in the management of septic shock with multi-organ dysfunction: A case report. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 297–299. [Google Scholar] [CrossRef]
- Markovic, M.; Knezevic, V.; Azaševac, T.; Majstorovic, S.; Veselinov, V.; Pencic, D.; Mitić, I. Continuous renal replacement therapy with Cytosorb in a polytrauma patient—When to start? A Case Report. In Proceedings of the 38th Vicenza Course on AKI & CRRT, Online, 2–6 November 2020. [Google Scholar]
- Moretti, R.; Scarrone, S.; Pizzi, B.; Bonato, V.; Vivaldi, N. Coupled plasma filtration-adsorption in Weil’s syndrome: Case report. Minerva Anestesiol. 2011, 77, 846–849. [Google Scholar]
- Piwowarczyk, P.; Kutnik, P.; Potręć-Studzińska, B.; Sysiak-Sławecka, J.; Rypulak, E.; Borys, M.; Czczuwar, M. Hemoadsorption in isolated conjugated hyperbilirubinemia after extracorporeal membrane oxygenation support. Cholestasis of sepsis: A case report and review of the literature on differential causes of jaundice in ICU patient. Int. J. Artif. Organs 2019, 42, 263–268. [Google Scholar] [CrossRef]
- Tomescu, D. First use of Cytosorb™ during living related liver transplantation in a patient with acute liver failure due to Wilson’s disease. In Proceedings of the 2018 Joint International Congress of ILTS, ELITA & LICAGE, Lisbon, Portugal, 23–26 May 2018. [Google Scholar]
- Wiegele, M.; Krenn, C.G. Cytosorb™ in a patient with Legionella pneumonia-associated rhabdomyolysis: A case report. ASAIO J. 2015, 61, e14–e16. [Google Scholar] [CrossRef]
- Lévai, T. Supportive therapy of acute pancreatitis with CytoSorb Adsorber. Case report, Abstract number: 055, 9th International Congress “Sepsis and Multiorgan Dysfunction”. Infection 2019, 47 (Suppl. S1), 49. [Google Scholar] [CrossRef]
- Manini, E.; Volpi, F.; Mencarelli, F.; Bocci, F.; Sini, P.; Ciampichini, R.; Todisco, C.; Beato, V.; Capini, E. Hemoperfusion with Cytosorb for Bilirubin and Cytokine Removal in a Cardiac Surgery Patient. Poster Presented at: Workshop Purification Therapies—Le Idee per la Ricerca Clinica, 2019, Italy. Available online: https://www.purificationtherapies.com/wp-content/uploads/01/16-2/P32_Poster_CYTO_Manini_Case%20report.pdf (accessed on 21 February 2022).
- Tomescu, D.; Popescu, M. The Potential Benefits of a Hemoadsorption Column in a Patient with Severe Inflammatory Syndrome due to Graft Dysfunction and Massive Transfusion after Liver Transplantation. In Proceedings of the 2017 Joint International Congress of ILTS, ELITA & LICAGE, Prague, Czech Republic, 24–27 May 2017. P-215, 187. [Google Scholar]
- Kogelmann, K. Use of CytoSorb in Septic Multiple Organ Failure Following Intestinal Ischemia Due to Volvulus with Concomitant Liver Failure after COVID-19 Disease; CytoSorb Literature Database Case of the Week. 2021. Available online: https://litdb-admin.cytosorb-therapy.com/wp-content/uploads/2021/04/CoW_14_2021_E_web.pdf (accessed on 23 December 2023).
- Breitkopf, R. Use of CytoSorb in a Patient with Sepsis and Acute Liver Failure Following C-Section in the 38th Week of Pregnancy CytoSorb Literature Database Case of the Week. 2020. Available online: https://litdb-admin.cytosorb-therapy.com/wp-content/uploads/2020/08/CoW_35_2020_E_web.pdf (accessed on 23 December 2023).
- Ullo, I.; Zappulo, F.; Bini, C.; Bruno, P.; Scrivo, A.; Donati, G.; La Manna, G. Coupled Plasma Filtration and Adsorption (CPFA) for Extracorporeal Detoxification During Acute or Acute on Chronic Liver Failure. Blood Purif. 2017, 44, 182. [Google Scholar]
- Popescu, M.; Marcu, A.; Calancea, E.; Tomescu, D. The Effects of Using a Hemoadsobtion Column (CytoSorb®®) in Patients with Acute on Chronic Liver Failure. A Pilot Study. In Proceedings of the 2017 Joint International Congress of ILTS, ELITA & LICAGE, Prague, Czech Republic, 24–27 May 2017. P-28, 102. [Google Scholar]
- Popescu, M.; Tomescu, D. The potential utility of a hemoadsobtion column (CytoSorb®®) in patients with acute liver failure. In Proceedings of the 2018 Joint International Congress of ILTS, ELITA & LICAGE, Lisbon, Portugal, 23–26 May 2018. [Google Scholar]
- Maggi, U.; Nita, G.; Gatti, S.; Antonelli, B.; Paolo, R.; Como, G.; Messa, P.; Rossi, G. Hyperbilirubinemia After Liver Transplantation: The Role of Coupled Plasma Filtration Adsorption. Transplant. Proc. 2013, 45, 2715–2717. [Google Scholar] [CrossRef]
- Popescu, M.; Vasile, A.; Tanase, A.; Dinca, A.; David, C.; Tomescu, D. Potential benefits of hemoadsorption in patients with acute liver failure. Crit. Care 2020, 24 (Suppl. S1), 279. [Google Scholar]
- Dhokia, V.D.; Madhavan, D.; Austin, A.; Morris, C.G. Novel use of Cytosorb™ haemadsorption to provide biochemical control in liver impairment. J. Intensive Care Soc. 2019, 20, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Acar, U.; Gökkaya, Z.; Akbulut, A.; Freah, O.; Yenidünya, Ö.; Açik, M.E.; Tokat, Y.; Yentür, E. Impact of Cytokine Adsorption Treatment in Liver Failure. Transplant. Proc. 2019, 51, 2420–2424. [Google Scholar] [CrossRef] [PubMed]
- Niu, D.G.; Huang, Q.; Yang, F.; Tian, W.L.; Zhao, Y.Z. Efficacy of Coupled Plasma Filtration Adsorption in Treating Patients with Severe Intra-Abdominal Infection: A Retrospective Study. J. Laparoendosc. Adv. Surg. Tech. A 2019, 29, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Scharf, C.; Liebchen, U.; Paal, M.; Becker-Pennrich, A.; Irlbeck, M.; Zoller, M.; Schroeder, I. Successful elimination of bilirubin in critically ill patients with acute liver dysfunction using a cytokine adsorber and albumin dialysis: A pilot study. Sci. Rep. 2021, 11, 10190. [Google Scholar] [CrossRef]
- Praxenthaler, J.; Schwier, E.; Altmann, S.; Kirchner, C.; Bialas, J.; Henzler, D.; Köhler, T. Immunomodulation by Hemoadsorption—Changes in Hepatic Biotransformation Capacity in Sepsis and Septic Shock: A Prospective Study. Biomedicines. 2022, 10, 2340. [Google Scholar] [CrossRef]
- Poli, E.C.; Rimmelé, T.; Schneider, A.G. Hemoadsorption with CytoSorb®®. Intensive Care Med. 2019, 45, 236–239. [Google Scholar] [CrossRef]
- Gruda, M.C.; Ruggeberg, K.G.; O’Sullivan, P.; Guilashvili, T.; Schreier, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb®® sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Brendolan, A.; d’Intini, V.; Ricci, Z.; Wratten, M.L.; Bellomo, R. Coupled plasma filtration adsorption: Rationale, technical development and early clinical experience. Blood Purif. 2003, 21, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Monard, C.; Rimmelé, T.; Ronco, C. Extracorporeal Blood Purification Therapies for Sepsis. Blood Purif. 2019, 47 (Suppl. S3), 2–15. [Google Scholar] [CrossRef]
- Kluge, M.; Tacke, F. Liver impairment in critical illness and sepsis: The dawn of new biomarkers? Ann. Transl. Med. 2019, 7 (Suppl. S8), S258. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Yoshikai, Y.; Kamiya, J.; Nagino, M.; Uesaka, K.; Yuasa, N.; Oda, K.; Sano, T.; Nimura, Y. Bilirubin impairs bactericidal activity of neutrophils through an antioxidant mechanism in vitro. J. Surg. Res. 2001, 96, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Dominik, A.; Stange, J. Similarities, Differences, and Potential Synergies in the Mechanism of Action of Albumin Dialysis Using the MARS Albumin Dialysis Device and the CytoSorb Hemoperfusion Device in the Treatment of Liver Failure. Blood Purif. 2021, 50, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, J.; Harm, S. Removal of bile acids by extracorporeal therapies: An in vitro study. Int. J. Artif. Organs 2017, 41, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Liebchen, U.; Paal, M.; Gräfe, C.; Zoller, M.; Scharf, C.; Cyto-SOLVE Study Group. The cytokine adsorber Cytosorb®® does not reduce ammonia concentrations in critically ill patients with liver failure. Intensive Care Med. 2023, 49, 360–362. [Google Scholar] [CrossRef]
- Ocskay, K.; Kanjo, A.; Gede, N.; Szakács, Z.; Pár, G.; Erőss, B.; Stange, J.; Steffen, M.; Hegyi, P.; Molnár, Z. Uncertainty in the impact of liver support systems in acute-on-chronic liver failure: A systematic review and network meta-analysis. Ann. Intensive Care 2021, 11, 10. [Google Scholar] [CrossRef]
- Mitzner, S.; Klammt, S.; Stange, J.; Schmidt, R. Albumin regeneration in liver support-comparison of different. Ther Apher Dial. 2006, 10, 108–117. [Google Scholar] [CrossRef]
- Hegyi, P.; Petersen, O.H.; Holgate, S.; Erőss, B.; Garami, A.; Szakács, Z.; Dobszai, D.; Balaskó, M.; Kemény, L.; Peng, S. Academia Europaea Position Paper on Translational Medicine: The Cycle Model for Translating Scientific Results into Community Benefits. J. Clin. Med. 2020, 9, 1532. [Google Scholar] [CrossRef] [PubMed]
- Hegyi, P.; Erőss, B.; Izbéki, F.; Párniczky, A.; Szentesi, A. Accelerating the translational medicine cycle: The Academia Europaea pilot. Nat. Med. 2021, 27, 1317–1319. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]


| Publication Data | Study Design | Number of Patients | Age | Used Device | Intervention | Number of Sessions | |
|---|---|---|---|---|---|---|---|
| First Author | Year of Publication | ||||||
| Gunasekera, A.M. [25] | 2022 | Case report | 1 | 54 a | CytoSorb | CRRT with CytoSorb | 1 |
| Ruiz-Rodriguez, J.C. [26] | 2022 | Case report | 1 | 50 a | CytoSorb | CVVHDF with CytoSorb | 1 |
| Cazzato, M.T. [27] | 2019 | Case report | 1 | No data | CytoSorb | CRRT with CytoSorb (24 h) | 4 |
| Daza, J.L. [28] | 2022 | Case report | 1 | 41 a | CytoSorb | SLED combined with CytoSorb (12 h) | 2 |
| Hinz, B. [29] | 2015 | Case report | 1 | 72 a | CytoSorb | CVVHD with CytoSorb (24-6-24 h) | 3 |
| Köhler, T. [30] | 2021 | Case report | 1 | 29 a | CytoSorb | CRRT with CytoSorb (24 h) | Unclear |
| Lau, C.W.M. [31] | 2021 | Case report | 1 | 47 a | oXiris | Blood purification with oXiris (5 days in total) | No data |
| Li, Y. [32] | 2020 | Case report | 1 | 35 a | oXiris | CVVH with oXiris (24 h) | 2 |
| Manohar, V. [33] | 2017 | Case report | 1 | 22 a | CytoSorb | Extracorporeal cytokine hemofiltration (12 h) | 1 |
| Markovic, M. [34] | 2020 | Case report | 1 | 31 a | CytoSorb and oXiris | CytoSorb (day 1) and oXiris (day 2) | 2 |
| Moretti, R. [35] | 2011 | Case report | 1 | 27 a | CPFA | CPFA (24 h) | 5 |
| Piwowarczyk, P. [36] | 2019 | Case report | 1 | 57 a | CytoSorb | CytoSorb with anticoagulated CVVHD (24 h) | 2 |
| Tomescu, D. [37] | 2018 | Case report | 1 | 17 a | CytoSorb | CytoSorb (before and throughout liver transplantation) | 1 |
| Wiegele, M. [38] | 2015 | Case report | 1 | 44 a | CytoSorb | CytoSorb (6 h) | 2 |
| Lévai, T. [39] | 2019 | Case report | 1 | 42 a | CytoSorb | CytoSorb with anticoagulated CVVRRT | 4 |
| Manini, E. [40] | 2019 | Case report | 1 | 62 a | CytoSorb | CytoSorb with anticoagulated CVVRRT | 1 |
| Popescu, M. [41] | 2017 | Case report | 1 | 47 a | CytoSorb | CytoSorb (24 h) | 4 |
| Kogelman, K. [42] | 2021 | Case report | 1 | 45 a | CytoSorb | CytoSorb with CRRT (in CVVHD mode) | 3 |
| Breitkopf, R. [43] | 2020 | Case report | 1 | 40 a | CytoSorb | CytoSorb with CRRT (in CVVHD mode) | 2 |
| Ullo, I. [44] | 2017 | Case series | 9 | 21–63 b | CPFA | CPFA with citrate anticoagulation | No data |
| Popescu, M. [45] | 2017 | Case series | 5 | 49 ± 13 c | CytoSorb | CytoSorb with CVVHF | No data |
| Popescu, M. and Tomescu, D. [46] | 2018 | Case series | 13 | 46 ± 17 c | CytoSorb | CytoSorb with CVVHF | No data |
| Maggi, U. [47] | 2013 | Case series | 2 | 22–64 b | CPFA | CPFA | 3 |
| Popescu, M. [48] | 2020 | Case series | 29 | 34 ± 14 c | CytoSorb | CytoSorb with CVVHDF | 3 |
| Dhokia, V.D. [49] | 2019 | Case series | 3 | 51–71 b | CytoSorb | CytoSorb with CVVHDF (1); CytoSorb with Prismaflex (1); CytoSorb with CRRT (1) | 2 |
| Acar, U. [50] | 2019 | Case series | 4 | 26–73 b | CytoSorb | CytoSorb with CVVHD | No data |
| Ocskay, K. [18] | 2021 | Registry analysis | 109 | 49.2 ± 17.1 c | CytoSorb | Varies: CytoSorb alone or CytoSorb with CRRT | 2 |
| Niu, D.G. [51] | 2019 | Retrospective observational study | 76 | 51.4 ± 15.6 c | CPFA | CPFA with CRRT | No data |
| Scharf, C. [52] | 2021 | Retrospective observational study | 33 | 55 (18–76) d | CytoSorb | CytoSorb | 1 |
| Praxenthaler, J. [53] | 2022 | Retrospective observational study | 21 | 74 (58–80) d | CytoSorb | CVVHD with CytoSorb | varies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turan, C.; Szigetváry, C.E.; Kói, T.; Engh, M.A.; Atakan, I.; Zubek, L.; Terebessy, T.; Hegyi, P.; Molnár, Z. Hemoadsorption Therapy for Critically Ill Patients with Acute Liver Dysfunction: A Meta-Analysis and Systematic Review. Biomedicines 2024, 12, 67. https://doi.org/10.3390/biomedicines12010067
Turan C, Szigetváry CE, Kói T, Engh MA, Atakan I, Zubek L, Terebessy T, Hegyi P, Molnár Z. Hemoadsorption Therapy for Critically Ill Patients with Acute Liver Dysfunction: A Meta-Analysis and Systematic Review. Biomedicines. 2024; 12(1):67. https://doi.org/10.3390/biomedicines12010067
Chicago/Turabian StyleTuran, Caner, Csenge Erzsébet Szigetváry, Tamás Kói, Marie Anne Engh, Işıl Atakan, László Zubek, Tamás Terebessy, Péter Hegyi, and Zsolt Molnár. 2024. "Hemoadsorption Therapy for Critically Ill Patients with Acute Liver Dysfunction: A Meta-Analysis and Systematic Review" Biomedicines 12, no. 1: 67. https://doi.org/10.3390/biomedicines12010067
APA StyleTuran, C., Szigetváry, C. E., Kói, T., Engh, M. A., Atakan, I., Zubek, L., Terebessy, T., Hegyi, P., & Molnár, Z. (2024). Hemoadsorption Therapy for Critically Ill Patients with Acute Liver Dysfunction: A Meta-Analysis and Systematic Review. Biomedicines, 12(1), 67. https://doi.org/10.3390/biomedicines12010067