
PET/MRI and Novel Targets for Breast Cancer

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Technical Aspects of PET/MRI
2.1. Integration of PET and MRI
2.2. Patient Preparation
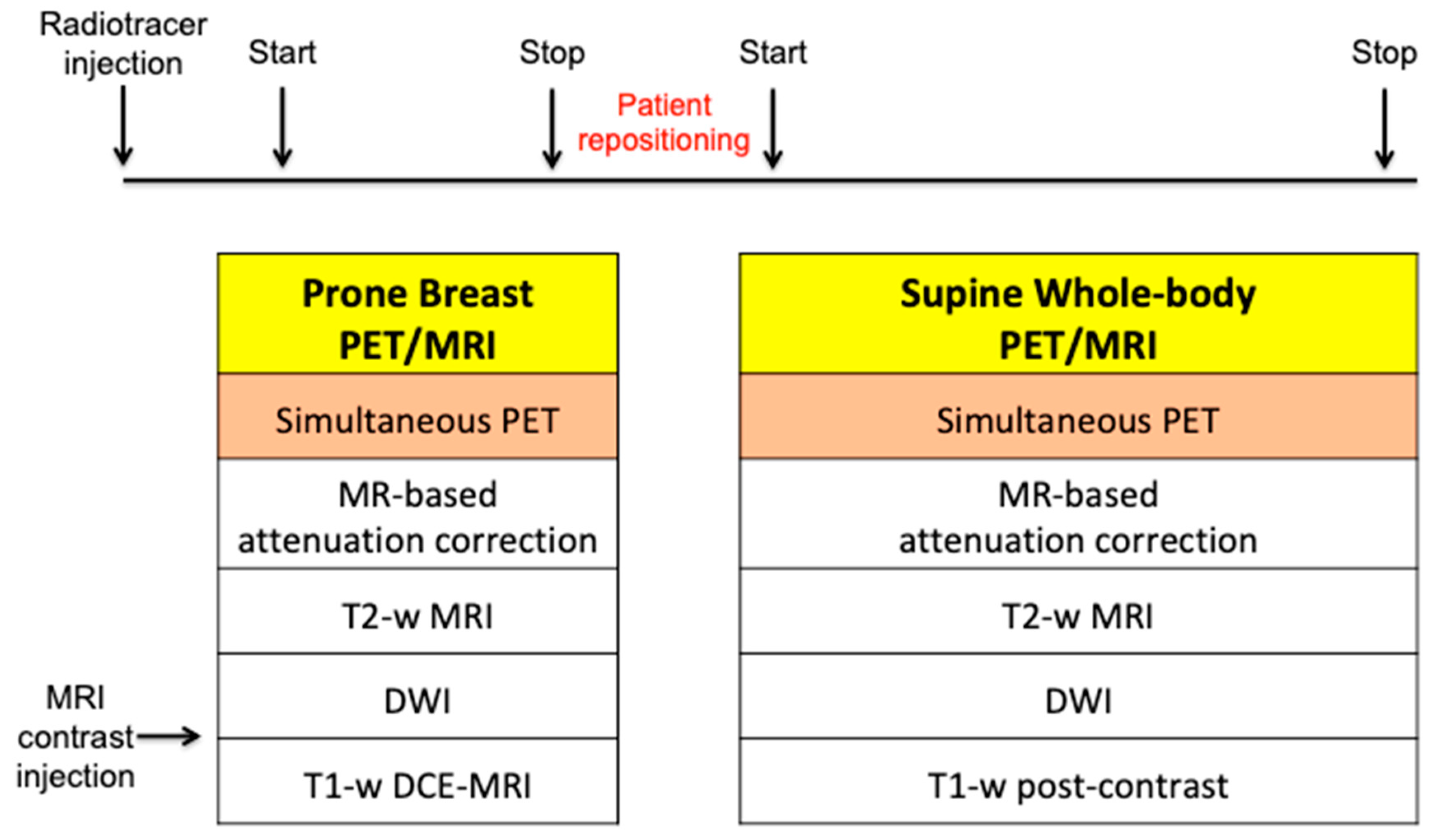
2.3. Image Acquisition
3. 18F-FDG PET/MRI for Breast Cancer
3.1. Diagnosis
3.2. Initial Staging
3.3. Therapy Response Assessment
3.4. Restaging
4. Novel Targets beyond Glucose Metabolism
4.1. Estrogen Receptor (ER)
4.2. Human Epidermal Growth Factor Receptor-2 (HER2)
4.3. Fibroblast Activation Protein (FAP)
4.4. Hypoxia
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Roginski, M.; Sifaki-Pistolla, D.; Stomby, A.; Velivasaki, G.; Faresjö, T.; Lionis, C.; Faresjö, Å. Paradoxes of breast cancer incidence and mortality in two corners of Europe. BMC Cancer 2022, 22, 1123. [Google Scholar] [CrossRef]
- Fowler, A.M.; Strigel, R.M. Clinical advances in PET-MRI for breast cancer. Lancet Oncol. 2022, 23, e32–e43. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Pujara, A.C.; Kim, E.; Axelrod, D.; Melsaether, A.N. PET/MRI in Breast Cancer. J. Magn. Reson. Imaging 2019, 49, 328–342. [Google Scholar] [CrossRef] [PubMed]
- Quick, H.H. Integrated PET/MR. J. Magn. Reson. Imaging 2014, 39, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Delso, G.; Fürst, S.; Jakoby, B.; Ladebeck, R.; Ganter, C.; Nekolla, S.G.; Schwaiger, M.; Ziegler, S.I. Performance measurements of the Siemens mMR integrated whole-body PET/MR scanner. J. Nucl. Med. 2011, 52, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Veit-Haibach, P.; Ahlström, H.; Boellaard, R.; Delgado Bolton, R.C.; Hesse, S.; Hope, T.; Huellner, M.W.; Iagaru, A.; Johnson, G.B.; Kjaer, A.; et al. International EANM-SNMMI-ISMRM consensus recommendation for PET/MRI in oncology. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3513–3537. [Google Scholar] [CrossRef] [PubMed]
- Levin, C.S.; Maramraju, S.H.; Khalighi, M.M.; Deller, T.W.; Delso, G.; Jansen, F. Design Features and Mutual Compatibility Studies of the Time-of-Flight PET Capable GE SIGNA PET/MR System. IEEE Trans. Med. Imaging 2016, 35, 1907–1914. [Google Scholar] [CrossRef]
- Seifert, S.; van der Lei, G.; van Dam, H.T.; Schaart, D.R. First characterization of a digital SiPM based time-of-flight PET detector with 1 mm spatial resolution. Phys. Med. Biol. 2013, 58, 3061–3074. [Google Scholar] [CrossRef] [PubMed]
- López-Mora, D.A.; Carrió, I.; Flotats, A. Digital PET vs. Analog PET: Clinical Implications? Semin. Nucl. Med. 2022, 52, 302–311. [Google Scholar] [CrossRef]
- Sekine, T.; Delso, G.; Zeimpekis, K.G.; de Galiza Barbosa, F.; Ter Voert, E.E.G.W.; Huellner, M.; Veit-Haibach, P. Reduction of 18F-FDG Dose in Clinical PET/MR Imaging by Using Silicon Photomultiplier Detectors. Radiology 2018, 286, 249–259. [Google Scholar] [CrossRef]
- Tsai, L.L.; Grant, A.K.; Mortele, K.J.; Kung, J.W.; Smith, M.P. A Practical Guide to MR Imaging Safety: What Radiologists Need to Know. Radiographics 2015, 35, 1722–1737. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Helbich, T.H.; Pinker, K. Breast PET/MRI Hybrid Imaging and Targeted Tracers. J. Magn. Reson. Imaging 2023, 57, 370–386. [Google Scholar] [CrossRef]
- Ruhlmann, V.; Heusch, P.; Kühl, H.; Beiderwellen, K.; Antoch, G.; Forsting, M.; Bockisch, A.; Buchbender, C.; Quick, H.H. Potential influence of Gadolinium contrast on image segmentation in MR-based attenuation correction with Dixon sequences in whole-body 18F-FDG PET/MR. MAGMA 2016, 29, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.T.; Rahbar, H.; Olson, M.L.; Liu, C.L.; Lehman, C.D.; Partridge, S.C. Diffusion-weighted imaging: Effects of intravascular contrast agents on apparent diffusion coefficient measures of breast malignancies at 3 Tesla. J. Magn. Reson. Imaging 2015, 42, 788–800. [Google Scholar] [CrossRef]
- Umutlu, L.; Beyer, T.; Grueneisen, J.S.; Rischpler, C.; Quick, H.H.; Veit-Haibach, P.; Eiber, M.; Purz, S.; Antoch, G.; Gatidis, S.; et al. Whole-Body [18F]-FDG-PET/MRI for Oncology: A Consensus Recommendation. Nuklearmedizin 2019, 58, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Jannusch, K.; Lindemann, M.E.; Bruckmann, N.M.; Morawitz, J.; Dietzel, F.; Pomykala, K.L.; Herrmann, K.; Bittner, A.K.; Hoffmann, O.; Mohrmann, S.; et al. Towards a fast PET/MRI protocol for breast cancer imaging: Maintaining diagnostic confidence while reducing PET and MRI acquisition times. Eur. Radiol. 2023, 33, 6179–6188. [Google Scholar] [CrossRef]
- Grueneisen, J.; Schaarschmidt, B.M.; Heubner, M.; Suntharalingam, S.; Milk, I.; Kinner, S.; Heubner, A.; Forsting, M.; Lauenstein, T.; Ruhlmann, V.; et al. Implementation of FAST-PET/MRI for whole-body staging of female patients with recurrent pelvic malignancies: A comparison to PET/CT. Eur. J. Radiol. 2015, 84, 2097–2102. [Google Scholar] [CrossRef]
- Mann, R.M.; Cho, N.; Moy, L. Breast MRI: State of the Art. Radiology 2019, 292, 520–536. [Google Scholar] [CrossRef]
- Chen, H.L.; Zhou, J.Q.; Chen, Q.; Deng, Y.C. Comparison of the sensitivity of mammography, ultrasound, magnetic resonance imaging and combinations of these imaging modalities for the detection of small (≤2 cm) breast cancer. Medicine 2021, 100, e26531. [Google Scholar] [CrossRef]
- Bitencourt, A.G.; Lima, E.N.; Chojniak, R.; Marques, E.F.; Souza, J.A.; Andrade, W.P.; Guimarães, M.D. Can 18F-FDG PET improve the evaluation of suspicious breast lesions on MRI? Eur. J. Radiol. 2014, 83, 1381–1386. [Google Scholar] [CrossRef]
- Kirchner, J.; Grueneisen, J.; Martin, O.; Oehmigen, M.; Quick, H.H.; Bittner, A.K.; Hoffmann, O.; Ingenwerth, M.; Catalano, O.A.; Heusch, P.; et al. Local and whole-body staging in patients with primary breast cancer: A comparison of one-step to two-step staging utilizing 18F-FDG-PET/MRI. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2328–2337. [Google Scholar] [CrossRef] [PubMed]
- Ruan, D.; Sun, L. Diagnostic Performance of PET/MRI in Breast Cancer: A Systematic Review and Bayesian Bivariate Meta-analysis. Clin. Breast Cancer 2023, 23, 108–124. [Google Scholar] [CrossRef] [PubMed]
- Romeo, V.; Clauser, P.; Rasul, S.; Kapetas, P.; Gibbs, P.; Baltzer, P.A.T.; Hacker, M.; Woitek, R.; Helbich, T.H.; Pinker, K. AI-enhanced simultaneous multiparametric 18F-FDG PET/MRI for accurate breast cancer diagnosis. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 596–608. [Google Scholar] [CrossRef] [PubMed]
- Teichgraeber, D.C.; Guirguis, M.S.; Whitman, G.J. Breast Cancer Staging: Updates in the AJCC Cancer Staging Manual, 8th Edition, and Current Challenges for Radiologists, From the AJR Special Series on Cancer Staging. AJR Am. J. Roentgenol. 2021, 217, 278–290. [Google Scholar] [CrossRef]
- Panico, C.; Ferrara, F.; Woitek, R.; D’Angelo, A.; Di Paola, V.; Bufi, E.; Conti, M.; Palma, S.; Cicero, S.L.; Cimino, G.; et al. Staging Breast Cancer with MRI, the T. A Key Role in the Neoadjuvant Setting. Cancers 2022, 14, 5786. [Google Scholar] [CrossRef] [PubMed]
- Grueneisen, J.; Nagarajah, J.; Buchbender, C.; Hoffmann, O.; Schaarschmidt, B.M.; Poeppel, T.; Forsting, M.; Quick, H.H.; Umutlu, L.; Kinner, S. Positron Emission Tomography/Magnetic Resonance Imaging for Local Tumor Staging in Patients with Primary Breast Cancer: A Comparison with Positron Emission Tomography/Computed Tomography and Magnetic Resonance Imaging. Investig. Radiol. 2015, 50, 505–513. [Google Scholar] [CrossRef]
- Goorts, B.; Vöö, S.; van Nijnatten, T.J.A.; Kooreman, L.F.S.; de Boer, M.; Keymeulen, K.B.M.I.; Aarnoutse, R.; Wildberger, J.E.; Mottaghy, F.M.; Lobbes, M.B.I.; et al. Hybrid 18F-FDG PET/MRI might improve locoregional staging of breast cancer patients prior to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1796–1805. [Google Scholar] [CrossRef]
- Botsikas, D.; Kalovidouri, A.; Becker, M.; Copercini, M.; Djema, D.A.; Bodmer, A.; Monnier, S.; Becker, C.D.; Montet, X.; Delattre, B.M.; et al. Clinical utility of 18F-FDG-PET/MR for preoperative breast cancer staging. Eur. Radiol. 2016, 26, 2297–2307. [Google Scholar] [CrossRef]
- Morawitz, J.; Bruckmann, N.M.; Dietzel, F.; Ullrich, T.; Bittner, A.K.; Hoffmann, O.; Ruckhäberle, E.; Mohrmann, S.; Häberle, L.; Ingenwerth, M.; et al. Comparison of nodal staging between CT, MRI, and [18F]-FDG PET/MRI in patients with newly diagnosed breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 992–1001. [Google Scholar] [CrossRef]
- Morawitz, J.; Sigl, B.; Rubbert, C.; Bruckmann, N.M.; Dietzel, F.; Häberle, L.J.; Ting, S.; Mohrmann, S.; Ruckhäberle, E.; Bittner, A.K.; et al. Clinical Decision Support for Axillary Lymph Node Staging in Newly Diagnosed Breast Cancer Patients Based on 18F-FDG PET/MRI and Machine Learning. J. Nucl. Med. 2023, 64, 304–311. [Google Scholar] [CrossRef]
- Di Micco, R.; Santurro, L.; Gasparri, M.L.; Zuber, V.; Cisternino, G.; Baleri, S.; Morgante, M.; Rotmensz, N.; Canevari, C.; Gallivanone, F.; et al. PET/MRI for Staging the Axilla in Breast Cancer: Current Evidence and the Rationale for SNB vs. PET/MRI Trials. Cancers 2021, 13, 3571. [Google Scholar] [CrossRef]
- Morawitz, J.; Bruckmann, N.M.; Jannusch, K.; Dietzel, F.; Milosevic, A.; Bittner, A.K.; Hoffmann, O.; Mohrmann, S.; Ruckhäberle, E.; Häberle, L.; et al. Conventional Imaging, MRI and 18F-FDG PET/MRI for N and M Staging in Patients with Newly Diagnosed Breast Cancer. Cancers 2023, 15, 3646. [Google Scholar] [CrossRef] [PubMed]
- de Mooij, C.M.; Sunen, I.; Mitea, C.; Lalji, U.C.; Vanwetswinkel, S.; Smidt, M.L.; van Nijnatten, T.J.A. Diagnostic performance of PET/computed tomography versus PET/MRI and diffusion-weighted imaging in the N- and M-staging of breast cancer patients. Nucl. Med. Commun. 2020, 41, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Lai, J.; Huang, D.; Qiu, S.; Hu, H.; Luo, Y.; Cao, J. Comparing the diagnostic efficacy of [18F]FDG PET/CT and [18F]FDG PET/MRI for detecting bone metastases in breast cancer: A meta-analysis. Radiol Oncol. 2023, 57, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Liang, Z.; Liu, W.; Zeng, X.; Mo, Y. Comparison of whole-body 18F-FDG PET/CT and PET/MRI for distant metastases in patients with malignant tumors: A meta-analysis. BMC Cancer 2023, 23, 37. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.; Taneja, S.; Singh, A.; Negi, P.; Mehta, S.B.; Ahuja, A.; Singhal, M.; Sarin, R. Association of pharmacokinetic and metabolic parameters derived using simultaneous PET/MRI: Initial findings and impact on response evaluation in breast cancer. Eur. J. Radiol. 2017, 92, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Shih, T.T.; Yen, R.F. Multiparametric Evaluation of Treatment Response to Neoadjuvant Chemotherapy in Breast Cancer Using Integrated PET/MR. Clin. Nucl. Med. 2017, 42, 506–513. [Google Scholar] [CrossRef]
- Cho, N.; Im, S.A.; Cheon, G.J.; Park, I.A.; Lee, K.H.; Kim, T.Y.; Kim, Y.S.; Kwon, B.R.; Lee, J.M.; Suh, H.Y.; et al. Integrated 18F-FDG PET/MRI in breast cancer: Early prediction of response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 328–339. [Google Scholar] [CrossRef]
- Sekine, C.; Uchiyama, N.; Watase, C.; Murata, T.; Shiino, S.; Jimbo, K.; Iwamoto, E.; Takayama, S.; Kurihara, H.; Satomi, K.; et al. Preliminary experiences of PET/MRI in predicting complete response in patients with breast cancer treated with neoadjuvant chemotherapy. Mol. Clin. Oncol. 2022, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- de Mooij, C.M.; van Nijnatten, T.J.A.; Goorts, B.; Kooreman, L.F.S.; Raymakers, I.W.M.; van Meijl, S.P.L.; de Boer, M.; Keymeulen, K.B.M.I.; Wildberger, J.E.; Mottaghy, F.M.; et al. Prediction of Primary Tumour and Axillary Lymph Node Response to Neoadjuvant Chemo(Targeted) Therapy with Dedicated Breast [18F]FDG PET/MRI in Breast Cancer. Cancers 2023, 15, 401. [Google Scholar] [CrossRef] [PubMed]
- Umutlu, L.; Kirchner, J.; Bruckmann, N.M.; Morawitz, J.; Antoch, G.; Ting, S.; Bittner, A.K.; Hoffmann, O.; Häberle, L.; Ruckhäberle, E.; et al. Multiparametric 18F-FDG PET/MRI-Based Radiomics for Prediction of Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer. Cancers 2022, 14, 1727. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Kim, H.A.; Kim, W.; Lim, I.; Lee, I.; Byun, B.H.; Noh, W.C.; Seong, M.K.; Lee, S.S.; Kim, B.I.; et al. Early prediction of neoadjuvant chemotherapy response for advanced breast cancer using PET/MRI image deep learning. Sci. Rep. 2020, 10, 21149. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Cochet, A.; Humbert, O.; Alberini, J.L.; Hindié, E.; Mankoff, D. 18F-FDG PET/CT for Staging and Restaging of Breast Cancer. J. Nucl. Med. 2016, 57 (Suppl. 1), 17S–26S. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, L.M.; Grueneisen, J.; Schaarschmidt, B.M.; Buchbender, C.; Nagarajah, J.; Umutlu, L.; Antoch, G.; Kinner, S. Evaluation of 18F-FDG PET/MRI, 18F-FDG PET/CT, MRI, and CT in whole-body staging of recurrent breast cancer. Eur. J. Radiol. 2016, 85, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lin, C.L.; Kao, C.H. Staging/restaging performance of F18-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging in breast cancer: A review and meta-analysis. Eur. J. Radiol. 2018, 107, 158–165. [Google Scholar] [CrossRef]
- Kwon, H.W.; Becker, A.K.; Goo, J.M.; Cheon, G.J. FDG Whole-Body PET/MRI in Oncology: A Systematic Review. Nucl. Med. Mol. Imaging 2017, 51, 22–31. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef]
- Mankoff, D.; Balogová, S.; Dunnwald, L.; Dehdashti, F.; DeVries, E.; Evangelista, L.; Van Kruchten, M.; Vaz, S.C.; Fowler, A.; Linden, H.; et al. Summary: SNMMI Procedure Standard/EANM Practice Guideline for Estrogen Receptor Imaging of Patients with Breast Cancer Using 16α-[18F]Fluoro-17β-Estradiol PET. J. Nucl. Med. 2024, 65. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.; Jeong, J.H.; Moon, D.H.; Lee, D.Y. Determination of the Estrogen Receptor Status of Leptomeningeal Metastasis in Patients with Metastatic Breast Cancer Using [18F]-FES PET/CT: A Case Report. Nucl. Med. Mol. Imaging 2022, 56, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Mankoff, D.A.; Clark, A.S.; Fowler, A.M.; Linden, H.M.; Peterson, L.M.; Dehdashti, F.; Kurland, B.F.; Mortimer, J.; Mouabbi, J.; et al. Summary: Appropriate Use Criteria for Estrogen Receptor-Targeted PET Imaging with 16α-18F-Fluoro-17β-Fluoroestradiol. J. Nucl. Med. 2023, 64, 351–354. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.R.; Edmonds, C.E.; Lanzo, S.M.; Weeks, J.K.; Mankoff, D.A.; Pantel, A.R. 18F-Fluoroestradiol: Current Applications and Future Directions. Radiographics 2023, 43, e220143. [Google Scholar] [CrossRef] [PubMed]
- Covington, M.F.; O’Brien, S.R.; Lawhn-Heath, C.; Pantel, A.R.; Ulaner, G.A.; Linden, H.M.; Dehdashti, F. Fluo-rine-18-Labeled Fluoroestradiol PET/CT: Current Status, Gaps in Knowledge, and Controversies-AJR Expert Panel Narrative Review. AJR Am. J. Roentgenol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Seban, R.D.; Champion, L.; Bellesoeur, A.; Vincent-Salomon, A.; Bidard, F.C. Clinical Potential of HER2 PET as a Predictive Biomarker to Guide the Use of Trastuzumab Deruxtecan in Breast Cancer Patients. J. Nucl. Med. 2023, 64, 1164–1165. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Hyman, D.M.; Ross, D.S.; Corben, A.; Chandarlapaty, S.; Goldfarb, S.; McArthur, H.; Erinjeri, J.P.; Solomon, S.B.; Kolb, H.; et al. Detection of HER2-Positive Metastases in Patients with HER2-Negative Primary Breast Cancer Using 89Zr-Trastuzumab PET/CT. J. Nucl. Med. 2016, 57, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Bensch, F.; Brouwers, A.H.; Lub-de Hooge, M.N.; de Jong, J.R.; van der Vegt, B.; Sleijfer, S.; de Vries, E.G.E.; Schröder, C.P. 89Zr-trastuzumab PET supports clinical decision making in breast cancer patients, when HER2 status cannot be determined by standard work up. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2300–2306. [Google Scholar] [CrossRef]
- Lee, I.; Lim, I.; Byun, B.H.; Kim, B.I.; Choi, C.W.; Lee, K.C.; Kang, C.M.; Seong, M.K.; Kim, H.A.; Noh, W.C.; et al. The Prediction of HER2-Targeted Treatment Response Using 64Cu-Tetra-Azacyclododecanetetra-Acetic Acid (DOTA)-Trastuzumab PET/CT in Metastatic Breast Cancer: A Case Report. J. Breast Cancer 2022, 25, 69–73. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Fernandez, A.I.; Liu, M.; Bellizzi, A.; Brock, J.; Fadare, O.; Hanley, K.; Harigopal, M.; Jorns, J.M.; Kuba, M.G.; Ly, A.; et al. Examination of Low ERBB2 Protein Expression in Breast Cancer Tissue. JAMA Oncol. 2022, 8, 607–610. [Google Scholar] [CrossRef]
- Siveke, J.T. Fibroblast-Activating Protein: Targeting the Roots of the Tumor Microenvironment. J. Nucl. Med. 2018, 59, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.A.; Weiner, L.M. The role of fibroblast activation protein in health and malignancy. Cancer Metastasis Rev. 2020, 39, 783–803. [Google Scholar] [CrossRef]
- Evangelista, L.; Filippi, L.; Schillaci, O. What radiolabeled FAPI pet can add in breast cancer? A systematic review from literature. Ann. Nucl. Med. 2023, 37, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Loktev, A.; Lindner, T.; Mier, W.; Debus, J.; Altmann, A.; Jäger, D.; Giesel, F.; Kratochwil, C.; Barthe, P.; Roumestand, C.; et al. A Tumor-Imaging Method Targeting Cancer-Associated Fibroblasts. J. Nucl. Med. 2018, 59, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Dendl, K.; Cardinale, J.; Kratochwil, C.; Giesel, F.L.; Haberkorn, U. FAPI PET: Fibroblast Activation Protein Inhibitor Use in Oncologic and Nononcologic Disease. Radiology 2023, 306, e220749. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zheng, S.; Chen, L.; Xu, S.; Wu, K.; Kong, L.; Xue, J.; Chen, X.; Miao, W.; Zhu, Y. 68Ga-Labeled Fibroblast Activation Protein Inhibitor PET/CT for the Early and Late Prediction of Pathologic Response to Neoadjuvant Chemotherapy in Breast Cancer Patients: A Prospective Study. J. Nucl. Med. 2023, 64, 1899–1905. [Google Scholar] [CrossRef]
- Backhaus, P.; Burg, M.C.; Roll, W.; Büther, F.; Breyholz, H.J.; Weigel, S.; Heindel, W.; Pixberg, M.; Barth, P.; Tio, J.; et al. Simultaneous FAPI PET/MRI Targeting the Fibroblast-Activation Protein for Breast Cancer. Radiology 2022, 302, 39–47. [Google Scholar] [CrossRef]
- Backhaus, P.; Burg, M.C.; Asmus, I.; Pixberg, M.; Büther, F.; Breyholz, H.J.; Yeh, R.; Weigel, S.B.; Stichling, P.; Heindel, W.; et al. Initial Results of 68Ga-FAPI-46 PET/MRI to Assess Response to Neoadjuvant Chemotherapy in Breast Cancer. J. Nucl. Med. 2023, 64, 717–723. [Google Scholar] [CrossRef]
- Giesel, F.L.; Adeberg, S.; Syed, M.; Lindner, T.; Jiménez-Franco, L.D.; Mavriopoulou, E.; Staudinger, F.; Tonndorf-Martini, E.; Regnery, S.; Rieken, S.; et al. FAPI-74 PET/CT Using Either 18F-AlF or Cold-Kit 68Ga Labeling: Biodistribution, Radiation Dosimetry, and Tumor Delineation in Lung Cancer Patients. J. Nucl. Med. 2021, 62, 201–207. [Google Scholar] [CrossRef]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of Quinoline-Based Theranostic Ligands for the Targeting of Fibroblast Activation Protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Loktev, A.; Lindner, T.; Burger, E.M.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Marmé, F.; Jäger, D.; Mier, W.; et al. Development of Fibroblast Activation Protein-Targeted Radiotracers with Improved Tumor Retention. J. Nucl. Med. 2019, 60, 1421–1429. [Google Scholar] [CrossRef]
- Yadav, M.P.; Ballal, S.; Martin, M.; Roesch, F.; Satapathy, S.; Moon, E.S.; Tripathi, M.; Gogia, A.; Bal, C. Therapeutic potential of [177Lu]Lu-DOTAGA-FAPi dimers in metastatic breast cancer patients with limited treatment options: Efficacy and safety assessment. Eur. J. Nucl. Med. Mol. Imaging 2023. [Google Scholar] [CrossRef]
- Muz, B.; de la Puente, P.; Azab, F.; Azab, A.K. The role of hypoxia in cancer progression, angiogenesis, metastasis, and resistance to therapy. Hypoxia 2015, 3, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, S.N.; Wuest, M.; Jans, H.S.; Woodfield, J.; Nario, A.P.; Krys, D.; Dufour, J.; Glubrecht, D.; Bergman, C.; Bernardes, E.S.; et al. Comparison of three 18F-labeled 2-nitroimidazoles for imaging hypoxia in breast cancer xenografts: [18F]FBNA, [18F]FAZA and [18F]FMISO. Nucl. Med. Biol. 2023, 124–125, 108383. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, J.G.; Krohn, K.A. F-18 fluoromisonidazole for imaging tumor hypoxia: Imaging the microenvironment for personalized cancer therapy. Semin. Nucl. Med. 2015, 45, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Postema, E.J.; McEwan, A.J.; Riauka, T.A.; Kumar, P.; Richmond, D.A.; Abrams, D.N.; Wiebe, L.I. Initial results of hypoxia imaging using 1-alpha-D:-(5-deoxy-5-[18F]-fluoroarabinofuranosyl)-2-nitroimidazole (18F-FAZA). Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1565–1573. [Google Scholar] [CrossRef]
- Carmona-Bozo, J.C.; Manavaki, R.; Woitek, R.; Torheim, T.; Baxter, G.C.; Caracò, C.; Provenzano, E.; Graves, M.J.; Fryer, T.D.; Patterson, A.J.; et al. Hypoxia and perfusion in breast cancer: Simultaneous assessment using PET/MR imaging. Eur. Radiol. 2021, 31, 333–344. [Google Scholar] [CrossRef]
- Kirchner, J.; Martin, O.; Umutlu, L.; Herrmann, K.; Bittner, A.K.; Hoffmann, O.; Mohrmann, S.; Gauler, T.; Theurer, S.; Antke, C.; et al. Impact of 18F-FDG PET/MR on therapeutic management in high risk primary breast cancer patients—A prospective evaluation of staging algorithms. Eur. J. Radiol. 2020, 128, 108975. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, H.W.; Park, K.S.; Lim, I.; Noh, W.C.; Yoo, Y.B.; Nam, S.E.; So, Y.; Lee, E.J. PET/MRI and Novel Targets for Breast Cancer. Biomedicines 2024, 12, 172. https://doi.org/10.3390/biomedicines12010172
Chung HW, Park KS, Lim I, Noh WC, Yoo YB, Nam SE, So Y, Lee EJ. PET/MRI and Novel Targets for Breast Cancer. Biomedicines. 2024; 12(1):172. https://doi.org/10.3390/biomedicines12010172
Chicago/Turabian StyleChung, Hyun Woo, Kyoung Sik Park, Ilhan Lim, Woo Chul Noh, Young Bum Yoo, Sang Eun Nam, Young So, and Eun Jeong Lee. 2024. "PET/MRI and Novel Targets for Breast Cancer" Biomedicines 12, no. 1: 172. https://doi.org/10.3390/biomedicines12010172
APA StyleChung, H. W., Park, K. S., Lim, I., Noh, W. C., Yoo, Y. B., Nam, S. E., So, Y., & Lee, E. J. (2024). PET/MRI and Novel Targets for Breast Cancer. Biomedicines, 12(1), 172. https://doi.org/10.3390/biomedicines12010172