
Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
- adult age ≥ 18 years,
- presence of clinically confirmed chylous effusion refractory to conservative treatment,
- clinical confirmation of chylous fluid by laboratory investigation (triglyceride levels > 110 mg/dL) and exclusion of a pseudo-chylous effusion (cholesterol levels < 50 mg/dL; ratio cholesterol: triglycerides < 1) [9]
- XRL with or without transabdominal LVE.
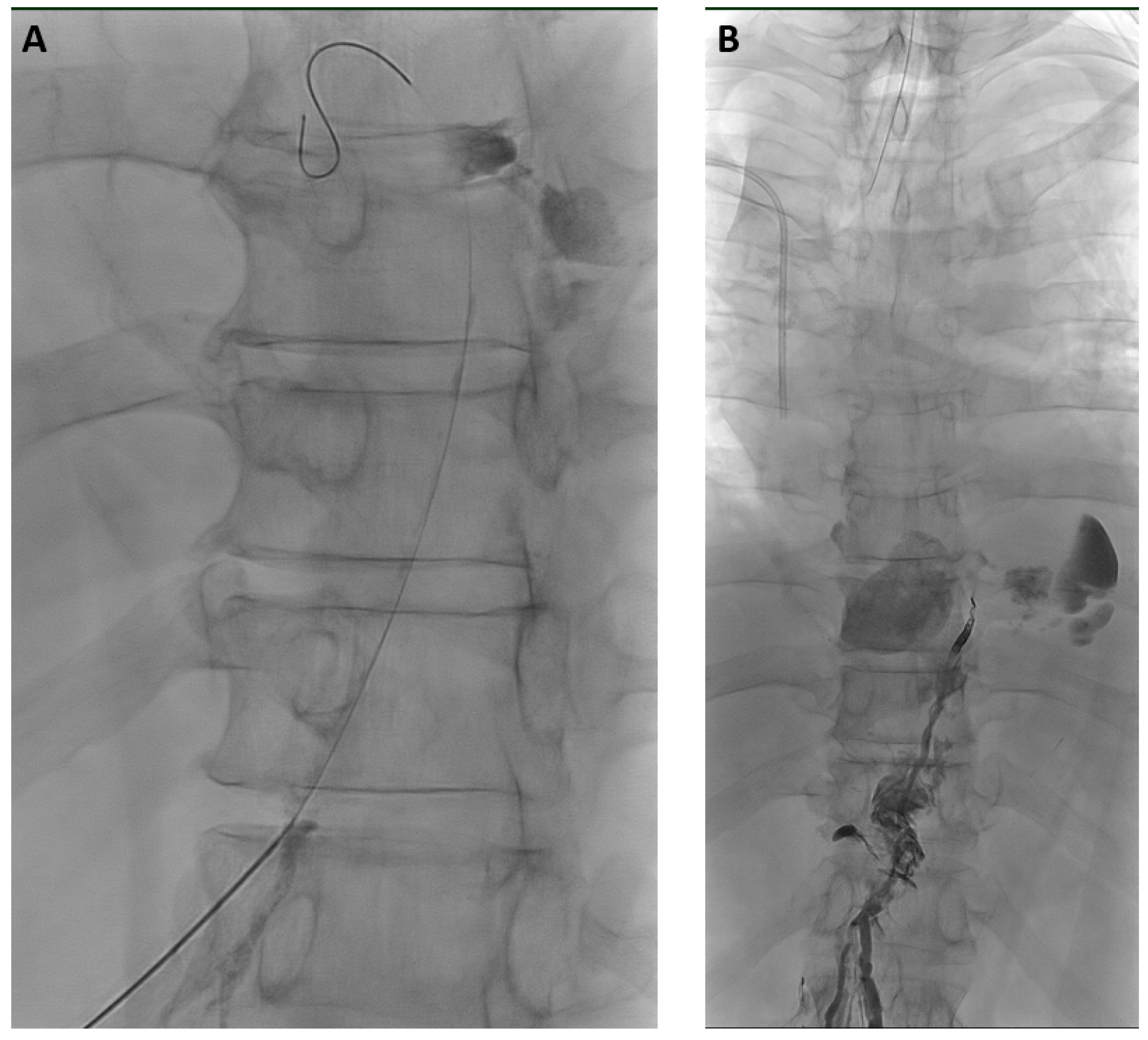
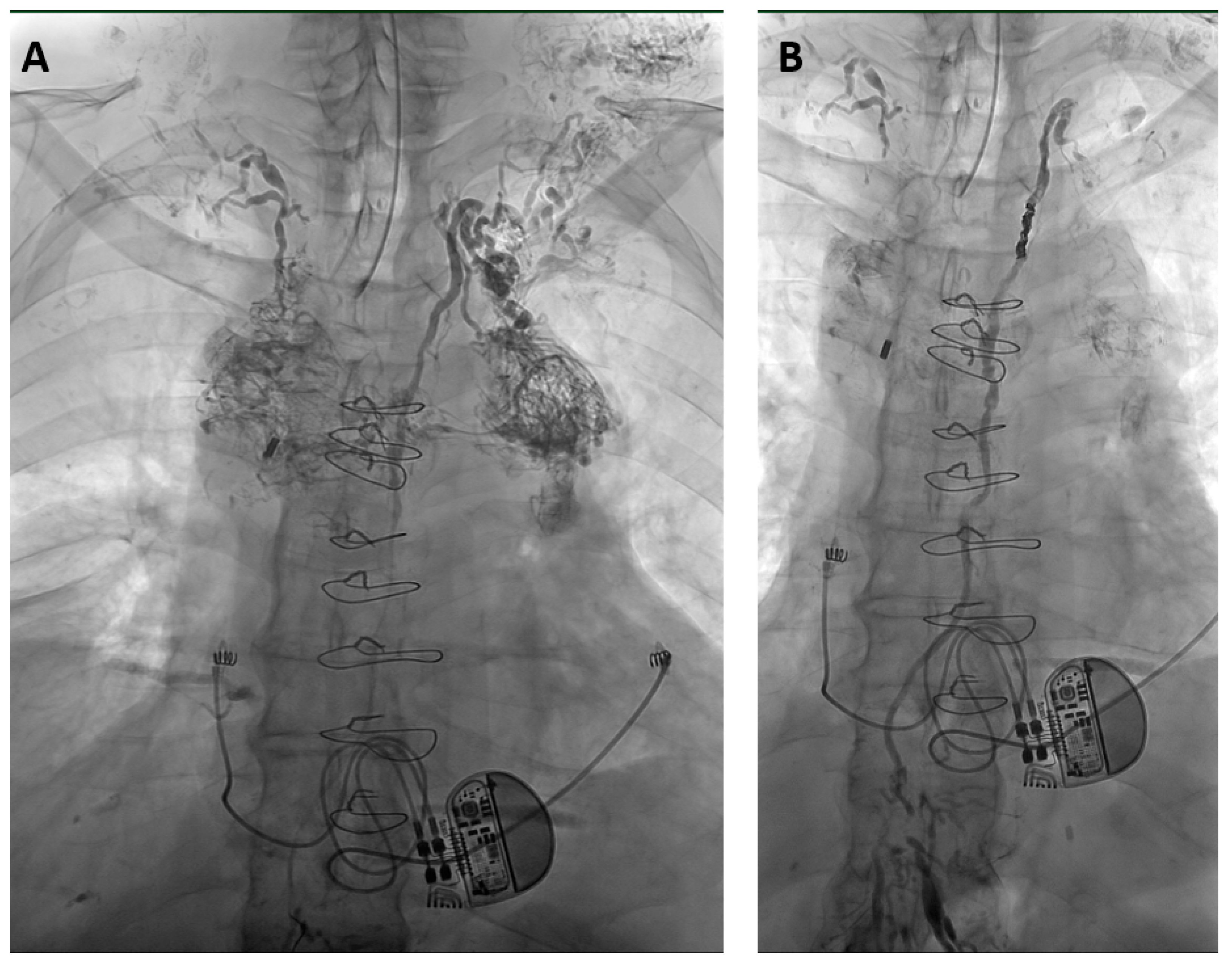
2.2. Interventional Technique
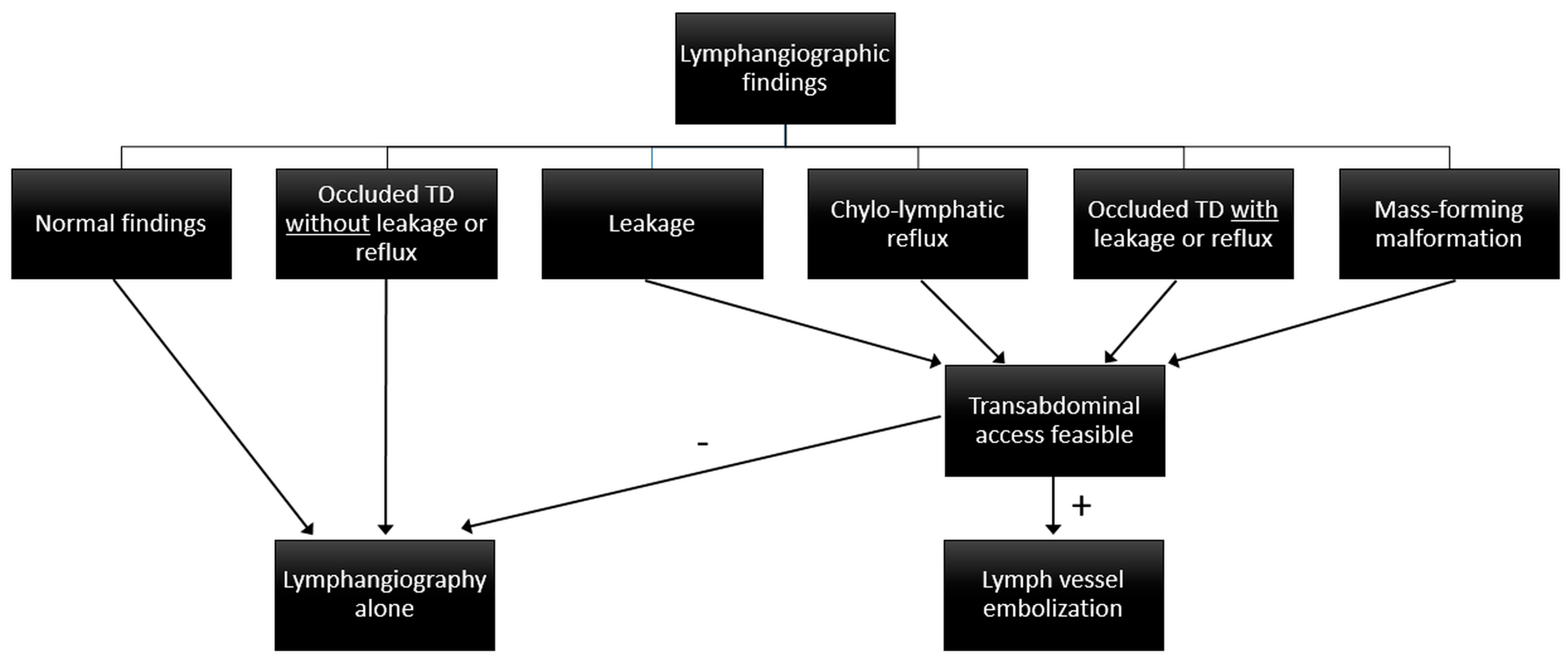
2.3. Imaging Findings
- Normal findings (no lymphatic leakage, reflux, obstruction, or mass)
- Localized lymphatic leakage (i.e., extravasation of contrast medium)
- Chylo-lymphatic reflux (i.e., retrograde flow away from the TD)
- Obstruction of central lymphatic run-off (with or without alternate lymphatic pathways)
- Mass-forming lymphatic malformations.
2.4. Treatment Strategy
- XRL-only was done when normal findings, lymphatic obstruction without leakage or reflux, or no accessible lymph vessel or node were seen.
- LVE was done when lymphatic leakage, reflux, lymphatic obstruction with leakage or reflux, or lymphatic malformations were identified.
- Chylous ascites was a contraindication for central embolization if no pathology of abdominal lymphatics was identified, as this might impair lymphatic run-off and worsen ascites formation.
2.5. Data Analysis and Definitions
2.6. Statistical Analysis
3. Results
3.1. Patients
- 48/78 patients (61.5%) had thoracic chylous effusions [chylothorax (n = 44), chylopericardium (n = 4)],
- 22/78 (28.2%) had chylous ascites,
- and 8/78 (10.3%) had a combination thereof.
- MCT diet (n = 21),
- parenteral nutrition (n = 23) or
- a sequential combination of both (n = 34) and
- additional octreotide therapy (n = 11).
3.2. Imaging Findings
3.3. Interventional Procedures
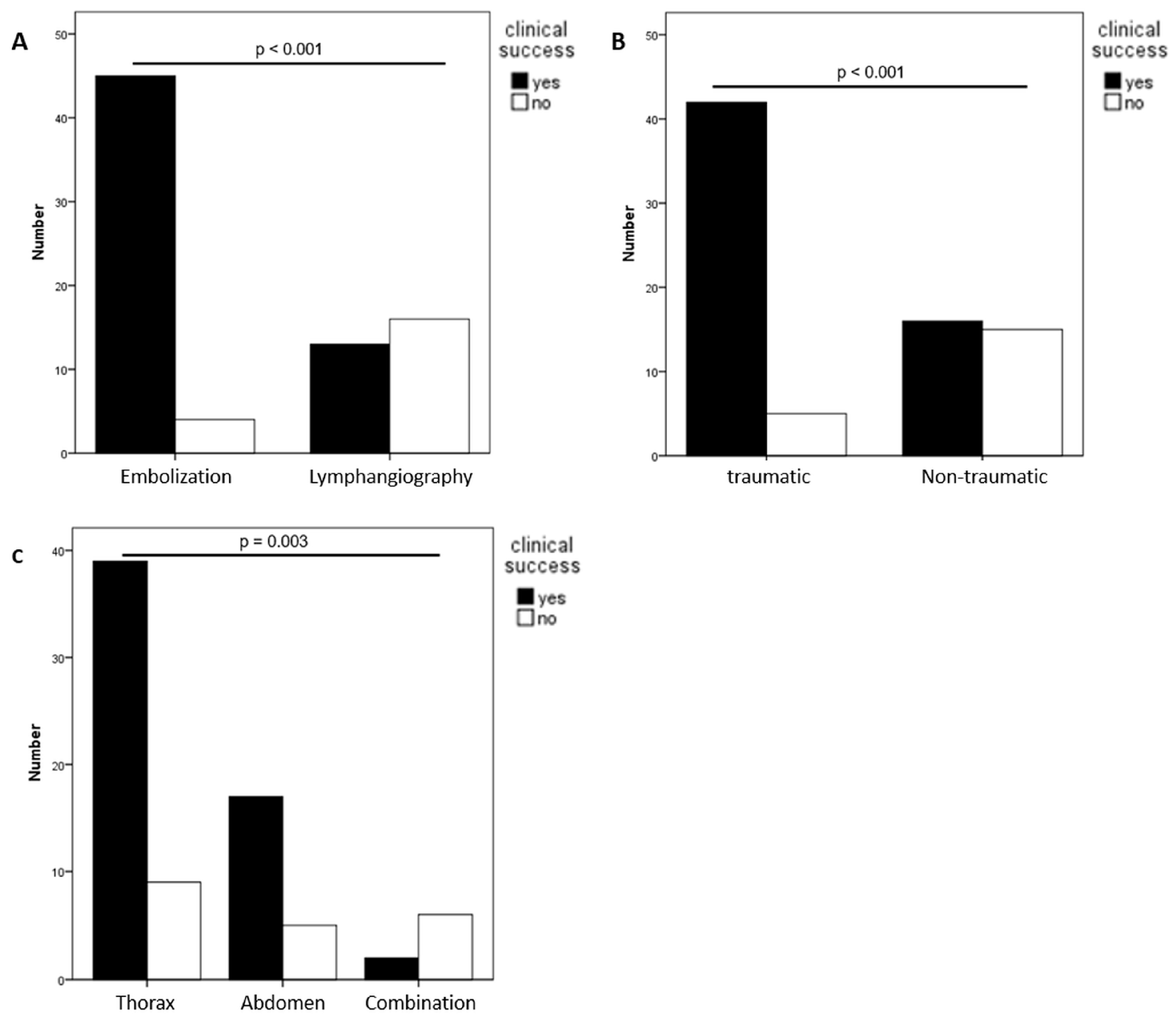
3.4. Clinical Success
3.5. Complications
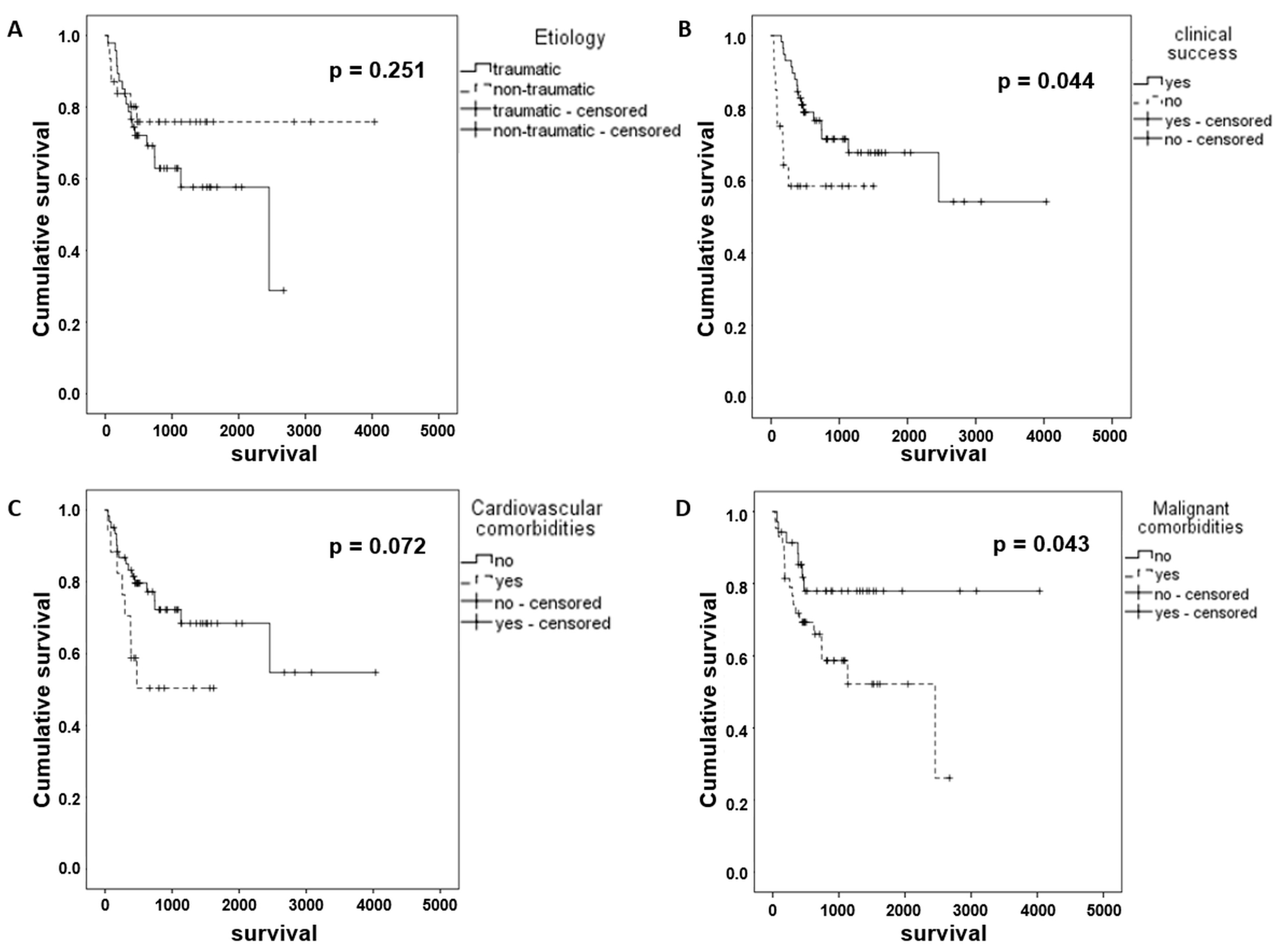
3.6. Clinical Course and Survival
4. Discussion
- XRL-only as first-line treatment, with LVE as second-line intervention in cases unresponsive to XRL-only,
- XRL with planned LVE—if indicated and feasible—in the same intervention.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schild, H.H.; Strassburg, C.P.; Welz, A.; Kalff, J. Treatment options in patients with chylothorax. Dtsch. Ärzteblatt Int. 2013, 110, 819–826. [Google Scholar]
- Pieper, C.C.; Hur, S.; Sommer, C.M.; Nadolski, G.; Maleux, G.; Kim, J.; Itkin, M. Back to the Future: Lipiodol in Lymphography-From Diagnostics to Theranostics. Investig. Radiol. 2019, 54, 600–615. [Google Scholar]
- Lee, E.W.; Shin, J.H.; Ko, H.K.; Park, J.; Kim, S.H.; Sung, K.B. Lymphangiography to treat postoperative lymphatic leakage: A technical review. Korean J. Radiol. 2014, 15, 724–732. [Google Scholar] [CrossRef]
- Nadolski, G. Nontraumatic Chylothorax: Diagnostic Algorithm and Treatment Options. Tech. Vasc. Interv. Radiol. 2016, 19, 286–290. [Google Scholar] [PubMed]
- Goity, L.D.; Itkin, M.; Nadolski, G. An Algorithmic Approach to Minimally Invasive Management of Nontraumatic Chylothorax. Semin. Interv. Radiol. 2020, 37, 269–273. [Google Scholar]
- Sommer, C.M.; Pieper, C.C.; Itkin, M.; Nadolski, G.J.; Hur, S.; Kim, J.; Maleux, G.; Kauczor, H.U.; Richter, G.M. Conventional Lymphangiography (CL) in the Management of Postoperative Lymphatic Leakage (PLL): A Systematic Review. RöFo-Fortschritte Auf Dem Geb. Der Röntgenstrahlen Und Der Bildgeb. Verfahr. 2020, 192, 1025–1035. [Google Scholar]
- Alejandre-Lafont, E.; Krompiec, C.; Rau, W.S.; Krombach, G.A. Effectiveness of therapeutic lymphography on lymphatic leakage. Acta Radiol. 2011, 52, 305–311. [Google Scholar] [PubMed]
- Gruber-Rouh, T.; Naguib, N.N.N.; Lehnert, T.; Harth, M.; Thalhammer, A.; Beeres, M.; Tsaur, I.; Hammersting, R.; Wichmann, J.L.; Vogl, T.J.; et al. Direct lymphangiography as treatment option of lymphatic leakage: Indications, outcomes and role in patient’s management. Eur. J. Radiol. 2014, 83, 2167–2171. [Google Scholar]
- Pieper, C.C. Back to the Future II-A Comprehensive Update on the RapidlyEvolving Field of Lymphatic Imaging and Interventions. Investig. Radiol. 2023, 58, 610–640. [Google Scholar]
- McGrath, E.E.; Blades, Z.; Anderson, P.B. Chylothorax: Aetiology, diagnosis and therapeutic options. Respir. Med. 2010, 105, 1–8. [Google Scholar]
- Cope, C. Diagnosis and treatment of postoperative chyle leakage via percutaneous transabdominal catheterization of the cisterna chyli: A preliminary study. J. Vasc. Interv. Radiol. 1998, 9, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Nadolski, G.J.; Chauhan, N.R.; Itkin, M. Lymphangiography and Lymphatic Embolization for the Treatment of Refractory Chylous Ascites. Cardiovasc. Interv. Radiol. 2018, 41, 415–423. [Google Scholar] [CrossRef]
- Weniger, M.; D’Haese, J.G.; Angele, M.K.; Kleespies, A.; Werner, J.; Hartwig, W. Treatment options for chylous ascites after major abdominal surgery: A systematic review. Am. J. Surg. 2016, 211, 206–213. [Google Scholar] [CrossRef]
- Schild, H.H.; Naehle, C.P.; Wilhelm, K.E.; Kuhl, C.K.; Thomas, D.; Meyer, C.; Textor, J.; Strunk, H.; Willinek, W.A.; Pieper, C.C. Lymphatic Interventions for Treatment of Chylothorax. RöFo-Fortschritte Auf Dem Geb. Der Röntgenstrahlen Und Der Bildgeb. Verfahr. 2015, 187, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Cerfolio, R.J.; Allen, M.S.; Deschamps, C.; Trastek, V.F.; Pairolero, P.C. Postoperative chylothorax. J. Thorac. Cardiovasc. Surg. 1996, 112, 1361–1365. [Google Scholar] [CrossRef]
- Reisenauer, J.S.; Puig, C.A.; Reisenauer, C.J.; Allen, M.S.; Bendel, E.; Cassivi, S.D.; Nichols, F.C.; Shen, R.K.; Wigle, D.A.; Blackmon, S.H. Treatment of Postsurgical Chylothorax. Ann. Thorac. Surg. 2018, 105, 254–262. [Google Scholar] [CrossRef]
- Kariya, S.; Nakatani, M.; Ueno, Y.; Yoshida, A.; Ono, Y.; Maruyama, T.; Komemushi, A.; Tanigawa, N. Transvenous retrograde thoracic ductography: Initial experience with 13 consecutive cases. Cardiovasc. Interv. Radiol. 2018, 41, 406–414. [Google Scholar] [CrossRef]
- Kim, P.H.; Tsauo, J.; Shin, J.H. Lymphatic Interventions for Chylothorax: A Systematic Review and Meta-Analysis. J. Vasc. Interv. Radiol. 2018, 29, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Schild, H.; Hirner, A. Percutaneous translymphatic thoracic duct embolization for treatment of chylothorax. RöFo-Fortschritte Auf Dem Geb. Der Röntgenstrahlen Und Der Bildgeb. Verfahr. 2001, 173, 580–582. [Google Scholar] [CrossRef] [PubMed]
- Itkin, M.; Kucharczuk, J.C.; Kwak, A.; Trerotola, S.O.; Kaiser, L.R. Nonoperative thoracic duct embolization for traumatic thoracic duct leak: Experience in 109 patients. J. Thorac. Cardiovasc. Surg. 2010, 139, 584–589. [Google Scholar] [CrossRef]
- Pamarthi, V.; Stecker, M.S.; Schenker, M.P.; Baum, R.A.; Killoran, T.P.; Suzuki Han, A.; O’Horo, S.K.; Rabkin, D.J.; Fan, C.M. Thoracic duct embolization and disruption for treatment of chylous effusions: Experience with 105 patients. J. Vasc. Interv. Radiol. 2014, 25, 1398–1404. [Google Scholar] [CrossRef] [PubMed]
- Kuetting, D.; Schild, H.H.; Pieper, C.C. In Vitro Evaluation of the Polymerization Properties of N-Butyl Cyanoacrylate/Iodized Oil Mixtures for Lymphatic Interventions. J. Vasc. Interv. Radiol. 2019, 30, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Kuetting, D.; Kupczyk, P.; Dell, T.; Luetkens, J.A.; Meyer, C.; Attenberger, U.I.; Pieper, C.C. In Vitro Evaluation of Acrylic Adhesives in Lymphatic Fluids-Influence of Glue Type and Procedural Parameters. Biomedicines 2022, 10, 1195. [Google Scholar] [CrossRef]
- Nadolski, G.J.; Itkin, M. Thoracic duct embolization for nontraumatic chylous effusion: Experience in 34 patients. Chest 2013, 143, 158–163. [Google Scholar] [CrossRef]
- Pieper, C.C.; Schild, H.H. Direct Cervical Puncture for Retrograde Thoracic Duct Embolization in a Postoperative Cervical Lymphatic Fistula. J. Vasc. Interv. Radiol. 2015, 26, 1405–1408. [Google Scholar] [CrossRef]
- Jun, H.; Hur, S. Interventional Radiology Treatment for Postoperative Chylothorax. Korean J. Thorac. Cardiovasc. Surg. 2020, 53, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Nadolski, G.; Itkin, M. Thoracic duct embolization for the management of chylothoraces. Curr. Opin. Pulm. Med. 2013, 19, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, F.; Cartin-Ceba, R.; Hawkins, F.J.; Ryu, J.H. Medical and surgical management of chylothorax and associated outcomes. Am. J. Med. Sci. 2010, 339, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Lindenblatt, N.; Gutschow, C.A.; Vetter, D.; Puippe, G.; Broglie Däppen, M.; Schneiter, D.; Uyulmaz, S.; Giovanoli, P.; Pieper, C.C.; Grünherz. Lympho-venous anastomosis for the treatment of congenital and acquired lesions of the central lymphtic system: A multidisciplinary treatment approach. Eur. J. Plast. Surg. 2022, 45, 841–849, online ahead of print. [Google Scholar] [CrossRef]
- McGraw, J.R.; Itkin, M.; Kovach, S.J., 3rd. Lymphangiography-Guided Thoracic Duct Surgical Lymphovenous Bypass for Distal Thoracic Duct Occlusion. J. Vasc. Interv. Radiol. 2023, 34, 1472–1473. [Google Scholar] [CrossRef]
- Smith, C.L.; Hoffman, T.M.; Dori, Y.; Rome, J.J. Decompression of the thoracic duct: A novel transcatheter approach. Catheter. Cardiovasc. Interv. 2020, 95, E56–E61. [Google Scholar] [CrossRef] [PubMed]
- Pimpalwar, S.; Chinnadurai, P.; Chau, A.; Pereyra, M.; Ashton, D.; Masand, P.; Krishnamurthy, R.; Jadhav, S. Dynamic contrast enhanced magnetic resonance lymphangiography: Categorization of imaging findings and correlation with patient management. Eur. J. Radiol. 2018, 101, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Majdalany, B.S.; Khayat, M.; Downing, T.; Killoran, T.P.; El-Haddad, G.; Khaja, M.S.; Saad, W.A. Lymphatic interventions for isolated, iatrogenic chylous ascites: A multi-institution experience. Eur. J. Radiol. 2018, 109, 41–47. [Google Scholar] [CrossRef]
- Verhaeghe, L.; Holsbeeck, A.V.; Bonne, L.; Claus, E.; Marrannes, J.; Vandenbulcke, R.; Jochmans, I.; Pirenne, J.; Maleux, G. Therapeutic lymphangiography with ethiodized oil for the management of lymphoceles and chylous ascites. In Diagnostic and Interventional Imaging; Elsevier: Amsterdam, The Netherlands, 2023. [Google Scholar]
- Benjamin, J.; O’Leary, C.; Hur, S.; Gurevich, A.; Klein, W.M.; Itkin, M. Imaging and Interventions for Lymphatic and Lymphatic-related Disorders. Radiology 2023, 307, e220231. [Google Scholar] [CrossRef]
- Kuetting, D.; Luetkens, J.; Fimmers, R.; Sprinkart, A.M.; Attenberger, U.; Pieper, C.C. MRI Assessment of Chylous and Nonchylous Effusions: Use of Multipoint Dixon Fat Quantification. Radiology 2020, 296, 698–705. [Google Scholar] [CrossRef]
- Milsom, J.W.; Kron, I.L.; Rheuban, K.S.; Rodgers, B.M. Chylothorax: An assessment of current surgical management. J. Thorac. Cardiovasc. Surg. 1985, 89, 221–227. [Google Scholar] [CrossRef]
- Laslett, D.; Trerotola, S.O.; Itkin, M. Delayed complications following technically successful thoracic duct embolization. J. Vasc. Interv. Radiol. 2012, 23, 76–79. [Google Scholar] [CrossRef]
- Shackcloth, M.J.; Poullis, M.; Lu, J.; Page, R.D. Preventing of chylothorax after oesophagectomy by routine pre-operative administration of oral cream. Eur. J. Cardiotharac. Surg 2001, 20, 1035–1036. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall | Thoracic | Abdominal | Abdomino-Thoracic |
|---|---|---|---|---|
| Number of patients (percentage) | 78 | 48 (61.5%) | 22 (28.2%) | 8 (10.3%) |
| Male:Female | 47:31 | 27:21 | 14:8 | 6:2 |
| Median age (range) | 56.3 (18–86) years | 59.4 (18–86) years | 64.2 (29–80) years | 53.0 (19–61) years |
| Median daily drainage volume (range) | 1000 mL (250–8000 mL) | 1000 mL (285–8000 mL) | 1000 mL (250–3500 mL) | 1850 mL (315–2250 mL) |
| Indication for lymphatic intervention | ||||
| Thoracic (chylothorax/chylopericardium) | 48 (61.5%) | |||
| Abdominal (chylous ascites) | 22 (28.2%) | |||
| Abdomino-thoracic (Combined chylothorax/chylous ascites) | 8 (10.3%) | |||
| Etiology | ||||
| Traumatic | 47 (60.3%) | 30 (62.5%) | 16 (72.7%) | 1 (12.5%) |
| Tumor surgery | 37 | 23 | 13 | 1 |
| Vascular surgery | 3 | 1 | 2 | 0 |
| Heart surgery | 3 | 3 | 0 | 0 |
| Other surgery | 4 | 3 | 1 | 0 |
| Non-traumatic | 31 (39.7%) | 18 (37.5%) | 6 (27.3%) | 7 (87.5%) |
| No known underlying disease | 16 | 8 | 4 | 4 |
| Lymphoma | 6 | 4 | 1 | 1 |
| Syndrome (e.g., LAM) | 5 | 5 | 0 | 0 |
| Congestive heart failure | 2 | 1 | 1 | 0 |
| Venous obstruction | 2 | 0 | 0 | 2 |
| Comorbidities | ||||
| Cardiovascular disease | 17 (21.8%) | 10 (20.8%) | 6 (27.3%) | 1 (12.5%) |
| Malignancy | 49 (62.8%) | 31 (64.6%) | 15 (68.2%) | 3 (37.5%) |
| Liver cirrhosis | 4 (5.1%) | 1 (2.1%) | 3 (13.6%) | 0 (0.0%) |
| Overall [n = 78] | Thoracic [n = 48] | Abdominal [n = 22] | Abdomino-Thoracic [n = 8] | |
|---|---|---|---|---|
| Leakage | 38 (48.7%) | 29 (60.4%) | 8 (36.4%) | 1 (12.5%) |
| Chylolymphatic reflux | 11 (14.1%) | 10 (20.8%) | 0 (0.0%) | 1 (12.5%) |
| Obstruction with reflux or leakage | 4 (5.1%) | 3 (6.3%) | 0 (0.0%) | 1 (12.5%) |
| Obstruction without reflux or leakage | 18 (23.1%) | 3 (6.3%) | 11 (50.0%) | 4 (50.0%) |
| Lymphatic mass | 4 (5.1%) | 3 (6.3%) | 0 (0.0%) | 1 (12.5%) |
| Normal findings | 3 (3.8%) | 0 (0.0%) | 3 (13.6%) | 0 (0.0%) |
| Location/Etiology | Success Overall | Success Embolization | Success lymphangiography | p-Value |
|---|---|---|---|---|
| Overall | 58/78 (74.4%) | 45/49 (91.8%) | 13/29 (44.8%) | <0.001 |
| Traumatic | 42/47 (89.4%) | 33/35 (94.3%) | 9/12 (75.0%) | 0.062 |
| Non-traumatic | 16/31 (51.6%) | 12/14 (85.7%) | 4/17 (23.5%) | 0.001 |
| p-value (Traumatic vs. Non-traumatic) | <0.001 | 0.332 | 0.006 | |
| Thoracic | 39/48 (81.3%) | 37/40 (92.5%) | 2/8 (25.0%) | <0.001 |
| Traumatic | 27/30 (90.0%) | 26/28 (92.9%) | 1/2 (50.0%) | 0.051 |
| Non-traumatic | 12/18 (66.7%) | 11/12 (91.7%) | 1/6 (16.7%) | 0.001 |
| p-value (Traumatic vs. Non-traumatic) | 0.045 | 0.896 | 0.346 | |
| Abdominal | 17/22 (77.3%) | 6/6 (100%) | 11/16 (68.8%) | 0.119 |
| Traumatic | 14/16 (87.5%) | 6/6 (100%) | 8/10 (80.0%) | 0.242 |
| Non-traumatic | 3/6 (50.0%) | 0/0 (0%) | 3/6 (50.0%) | NA |
| p-value (Traumatic vs. Non-traumatic) | 0.062 | NA | 0.210 | |
| Combined | 2/8 (25.0%) | 2/3 (66.7%) | 0/5 (0.0%) | 0.035 |
| Traumatic | 1/1 (100%) | 1/1 (100%) | 0/0 (0.0%) | NA |
| Non-traumatic | 1/7 (14.3%) | 1/2 (50.0%) | 0/5 (0.0%) | 0.088 |
| p-value (Traumatic vs. Non-traumatic) | 0.064 | 0.386 | NA | |
| p-value (Thoracic vs. Abdominal vs. abdomino-thoracic)) | 0.003 | 0.213 | 0.011 |
| Complication | No. | Cause | CTCAE Grade | Treatment | Outcome |
|---|---|---|---|---|---|
| Biliary peritonitis | 1 | Transgression of gallbladder | 4 | Cholecystectomy | Further course unremarkable |
| Bleeding from branch of left hepatic artery | 1 | Mandatory therapeutic anticoagulation due to cardiac-assist-device | 3 | Transcatheter embolization of bleeding vessel | Further course unremarkable |
| Edematous pancreatitis | 1 | Transgression of pancreas | 2 | Parenteral nutrition | Further course unremarkable |
| Upper extremity vein thrombosis | 1 | unknown | 2 | Heparinization | Further course unremarkable |
| Pulmonary glue migration | 1 | Transgression of vein near lymphtic puncture site | 1 | none | Further course unremarkable |
| Parameter | Mean Survival [Days] (95% CI) | Univariate p-Value |
|---|---|---|
| Overall | 2536 (2004;3068) | |
| Gender | 0.397 | |
| Female | 1941 (1405;2478) | |
| Male | 2518 (1785;3251) | |
| Etiology | 0.251 | |
| Traumatic | 1675 (1328;2022) | |
| Non-traumatic | 3111 (2510;3713) | |
| Location | 0.587 | |
| Thorax | 2522 (1866;3177) | |
| Abdomen | 1956 (1423;2489) | |
| Combination | 875 (441;1309) | |
| Treatment | 0.907 | |
| Embolization | 2655 (2096;3214) | |
| Lymphangiography | 2081 (1560;2603) | |
| Clinical success | 0.044 | |
| Yes | 2679 (2104;3253) | |
| No | 927 (621;1234) | |
| Comorbidities | ||
| Cardiovascular | 0.072 | |
| Yes | 2687 (2110;3264) | |
| No | 952 (614;1290) | |
| Malignant | 0.043 | |
| Yes | 3214 (2672;3756) | |
| No | 1550 (1170;1930) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaminski, L.C.; Wagenpfeil, J.; Buermann, J.; Lutz, P.L.; Luetkens, J.A.; Attenberger, U.I.; Strassburg, C.P.; Kalff, J.C.; Schild, H.H.; Pieper, C.C. Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults. Biomedicines 2023, 11, 2556. https://doi.org/10.3390/biomedicines11092556
Kaminski LC, Wagenpfeil J, Buermann J, Lutz PL, Luetkens JA, Attenberger UI, Strassburg CP, Kalff JC, Schild HH, Pieper CC. Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults. Biomedicines. 2023; 11(9):2556. https://doi.org/10.3390/biomedicines11092556
Chicago/Turabian StyleKaminski, Lea C., Julia Wagenpfeil, Jens Buermann, Philipp L. Lutz, Julian A. Luetkens, Ulrike I. Attenberger, Christian P. Strassburg, Jörg C. Kalff, Hans H. Schild, and Claus C. Pieper. 2023. "Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults" Biomedicines 11, no. 9: 2556. https://doi.org/10.3390/biomedicines11092556
APA StyleKaminski, L. C., Wagenpfeil, J., Buermann, J., Lutz, P. L., Luetkens, J. A., Attenberger, U. I., Strassburg, C. P., Kalff, J. C., Schild, H. H., & Pieper, C. C. (2023). Long-Term Clinical Outcome of Abdomino-Thoracic Lymphatic Interventions of Traumatic and Non-Traumatic Lymphatic Leakage in Adults. Biomedicines, 11(9), 2556. https://doi.org/10.3390/biomedicines11092556