
Calcium Channel Blockers and the Risk of Exacerbation in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Study of 48,488 Outpatients


 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sources
- Danish nationwide register of outpatients with COPD [2] (DrCOPD—Danish Register of Chronic Obstructive Pulmonary Disease). The COPD diagnosis was based on spirometry and verified by a respiratory physician. From this register, we obtained the following variables: age, gender, forced expiratory volume in 1 s (FEV1), body mass index (BMI), date of out-patient visits, Medical Research Council (MRC) breathlessness score, smoking status, and the date of death.
- The Danish National Patient Registry (DNPR) [15], where all hospital admissions since 1995 are registered. Each hospital visit is coded by a physician with one primary diagnosis and one or more secondary diagnoses, according to the International Classification of Diseases, 10th revision (ICD10) from 1994. We extracted the following primary or secondary diagnoses: J19, J440–J441, DJ448-DJ449.
- The Danish National Health Service Prescription Database [16] (DNHSPD) holds all prescriptions that have been dispensed in Danish pharmacies since 2004, coded according to the Anatomical Therapeutic Chemical (ATC) classification system. The date of dispensation, the quantity dispensed, and the formulation and strength of the prescription are all included. Danish legislation requires pharmacies to provide information that ensures complete and accurate registration. The DNHSPD was used for information on amlodipine, bendroflumethiazide, prednisolone, and antibiotics.
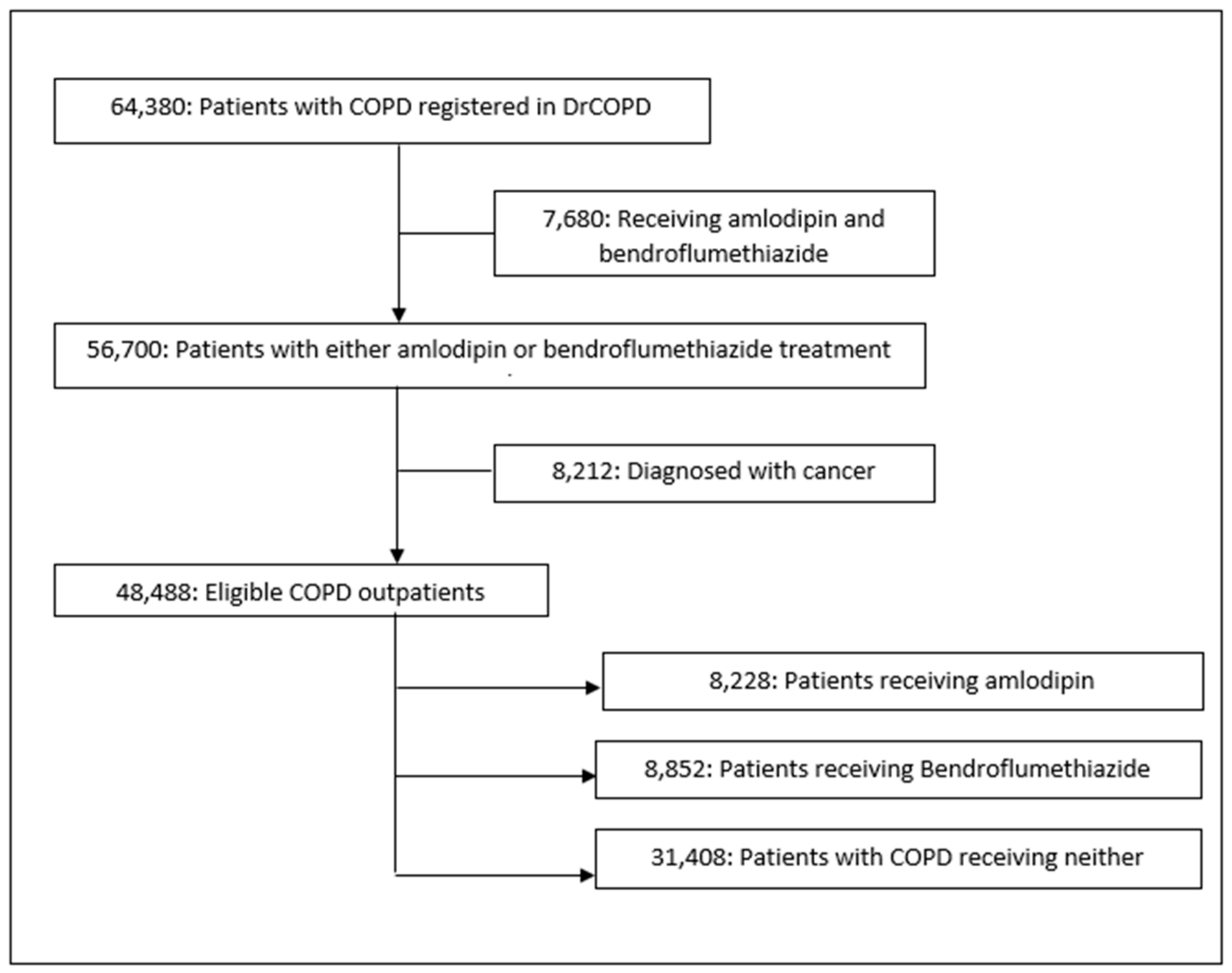
2.3. Study Participants
2.4. Outcomes
2.5. Statistics
2.6. Main Analysis
2.7. Sensitivity Analysis
2.8. Ethics Statement
3. Results
3.1. Descriptive Analyses
3.2. Statistical Analyses
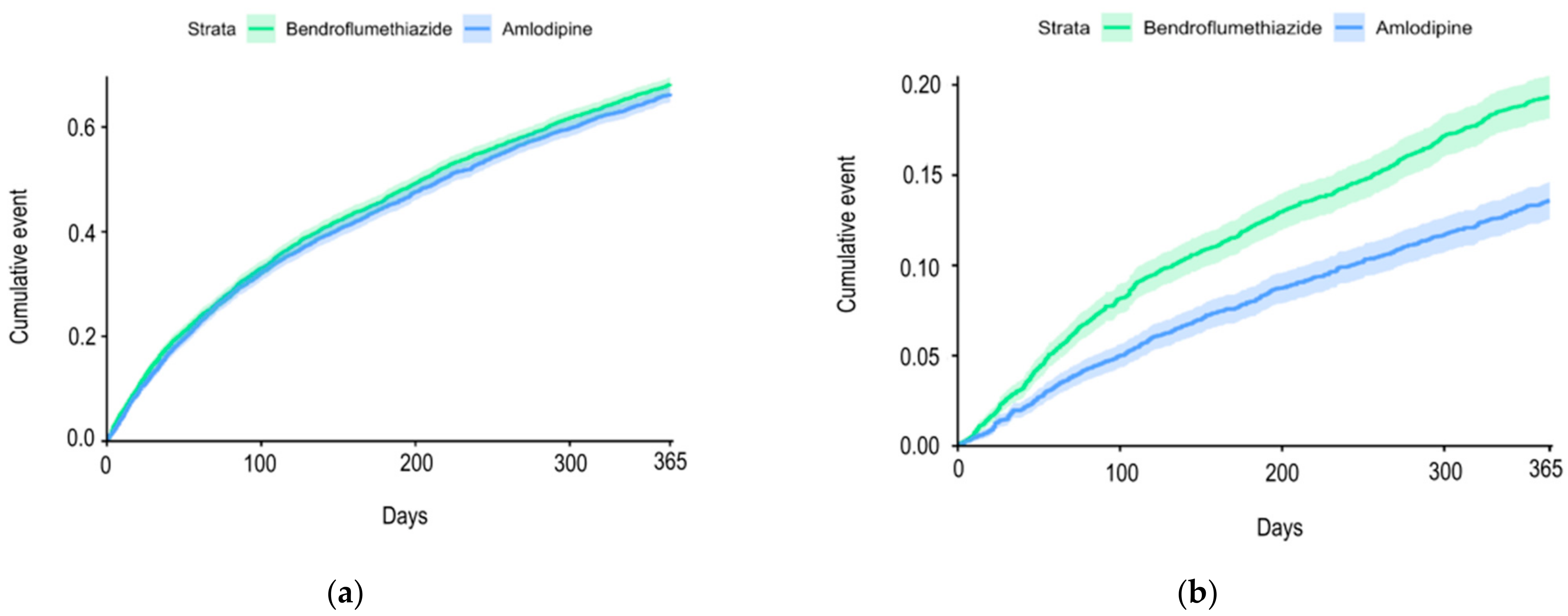
3.2.1. Main Analysis
3.2.2. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Medicament | ATC Code |
| Calcium channel antagonist | |
| Amlodipine | C08CA01 |
| Thiazide | |
| Bendroflumethiazide and potassium | C03AB01 |
| Corticosteroids | |
| Prednisolone | H02AB06 |
Appendix B
| Diagnosis | ICD Code |
| Neoplasms | |
| Malignant neoplasms | C00-C97 |
| Other malignant neoplasms of skin | C44 |
| In situ neoplasms | D00-D09 |
| In situ carcinoma of skin | D04 |
| Kidney diseases | |
| Chronic kidney disease | N18 |
| Type 1 diabetes mellitus with kidney complications | E102 |
| Type 2 diabetes mellitus with kidney complications | E112 |
| Heart diseases | |
| Rheumatic heart disease, unspecified | I099 |
| Hypertensive heart disease with heart failure | I110 |
| Hypertensive heart and chronic kidney disease | I13 |
| Ischemic cardiomyopathy | I255 |
| Dilated cardiomyopathy | I420 |
| Restrictive and other cardiomyopathies | I425, I426, I427, I428, I429 |
| Cardiomyopathy in diseases classified elsewhere | I43 |
| Congestive heart failure | I50 |
References
- WHO. Chronic Obstructive Pulmonary Disease Fact Sheet. 22 May 2022. Available online: https://www.who.int/en/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 20 February 2023).
- Lange, P.; Tøttenborg, S.S.; Sorknæs, A.D.; Andersen, J.S.; Søgaard, M.; Nielsen, H.; Thomsen, R.; Nielsen, K.A. Danish Register of chronic obstructive pulmonary disease. Clin. Epidemiol. 2016, ume 8, 673–678. [Google Scholar] [CrossRef]
- Hillas, G.; Perlikos, F.; Tzanakis, N. Acute exacerbation of COPD: Is it the “stroke of the lungs”? Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1579–1586. [Google Scholar]
- Mannino, D.M.; Thorn, D.; Swensen, A.; Holguin, F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur. Respir. J. 2008, 32, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Sajadieh, A.; Bojer, A.S.; Christensen, K.L. Arteriel Hypertension: Dansk Cardiologisk Selskab; [Updated 3 May 2019]. Available online: https://www.nbv.cardio.dk/hypertension (accessed on 9 July 2023).
- Banach, M.; Aronow, W.S.; Chandy, D. Current perspectives on treatment of hypertensive patients with chronic obstructive pulmonary disease. Integr. Blood Press. Control 2013, 6, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Dransfield, M.T.; Voelker, H.; Bhatt, S.P.; Brenner, K.; Casaburi, R.; Come, C.E.; Cooper, J.A.D.; Criner, G.J.; Curtis, J.L.; Han, M.K.; et al. Metoprolol for the Prevention of Acute Exacerbations of COPD. N. Engl. J. Med. 2019, 381, 2304–2314. [Google Scholar] [CrossRef] [PubMed]
- Finks, S.W.; Rumbak, M.J.; Self, T.H. Treating Hypertension in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2020, 382, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Elliott, W.J.; Ram, C.V. Calcium channel blockers. J. Clin. Hypertens. 2011, 13, 687–689. [Google Scholar] [CrossRef] [PubMed]
- Elmslie, K.S. Calcium channel blockers in the treatment of disease. J. Neurosci. Res. 2004, 75, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Andersson, C.; Hansen, P.W.; Steffensen, I.E.; Andreasen, C.; Weeke, P.E.; Køber, L.; Gislason, G.H.; Torp-Pedersen, C. Mortality associated with cardiovascular drugs in patients with chronic obstructive pulmonary disease and right-sided heart failure—A danish nationwide registry-based study. Eur. J. Intern. Med. 2019, 63, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Sajkov, D.; McEvoy, R.D.; Cowie, R.J.; Bradley, J.A.; Antic, R.; Morris, R.G.; Frith, B.A. Felodipine Improves Pulmonary Hemodynamics in Chronic Obstructive Pulmonary Disease. Chest 1993, 103, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Clemens, R.A.; Lowell, C.A. Store-operated calcium signaling in neutrophils. J. Leukoc. Biol. 2015, 98, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.V.; Hallett, M. Cytosolic Ca2+ signalling in inflammatory neutrophils: Implications for rheumatoid arthritis (Review). Int. J. Mol. Med. 1998, 1, 485–575. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Schmidt, S.A.J.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sørensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef] [PubMed]
- Pottegård, A.; Schmidt, S.A.J.; Wallach-Kildemoes, H.; Sørensen, H.T.; Hallas, J.; Schmidt, M. Data Resource Profile: The Danish National Prescription Registry. Int. J. Epidemiol. 2017, 46, 798–798f. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. GOLD-REPORT-2022-v1.1-22Nov2021_WMV (1). Available online: https://goldcopd.org/2022-gold-reports/ (accessed on 9 July 2023).
- Lund, J.L.; Richardson, D.B.; Stürmer, T. The Active Comparator, New User Study Design in Pharmacoepidemiology: Historical Foundations and Contemporary Application. Curr. Epidemiol. Rep. 2015, 2, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.mayo.edu/research/documents/biostat-56pdf/doc-10026923 (accessed on 26 October 2021).
- Dahlöf, B.; Sever, P.S.; Poulter, N.R.; Wedel, H.; Beevers, D.G.; Caulfield, M.; Collins, R.; E Kjeldsen, S.; Kristinsson, A.; McInnes, G.T.; et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): A multicentre randomised controlled trial. Lancet 2005, 366, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.; Borrild, N.; Andersen, J.V. Efficacy and safety of 24 weeks of therapy with bendroflumethiazide 1.25 mg/day or 2.5 mg/day and potassium chloride compared with enalapril 10 mg/day and amlodipine 5 mg/day in patients with mild to moderate primary hypertension: A multicentre, randomised, open study. Clin. Drug Investig. 2006, 26, 91–101. [Google Scholar] [PubMed]
- Golan, D.E.; Armstrong, E.J.; Armstrong, A.W. Principles of Pharmacology the Pathophysiologic Basis of Drug Therapy; Lippincott Williams and Wilkins, 2001 Market Street 2 Commerce Square: Philadelphia, PA, USA, 2012; pp. 363–365. [Google Scholar]
- Immler, R.; Simon, S.I.; Sperandio, M. Calcium signalling and related ion channels in neutrophil recruitment and function. Eur. J. Clin. Investig. 2018, 48 (Suppl. 2), e12964. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ATC/DDD Index 2022; WHO Collaborating Centre for Drug Statistics Methodology, Marcus Thranes Gate 6: Oslo, Norway, 2022; p. 1. [Google Scholar]
- Sundhedsdatastyrelsen. SKS-Browser, Vers 4.06; Sundhedsdatastyrelsen: Copenhagen, Denmark, 2021. [Google Scholar]



{kind=link}
{kind=link}
| Active Comparator Population | Entire Unmatched Population | |||
|---|---|---|---|---|
| Amlodipine Users | Bendroflumethiazide Users | Amlodipine Users | Non-Users | |
| (n = 4271) | (n = 4271) | (n = 8228) | (n = 40,260) | |
| Age, years, median (IQR) | 70 (63–77) | 72 (64–78) | 71 (64–78) | 70 (62–78) |
| Age | ||||
| ≤62 years | 986 (23.1%) | 915 (21.4%) | 1672 (20.3%) | 10,819(26.9%) |
| 63–70 years | 1174 (27.5%) | 1069 (25.0%) | 2251 (27.4%) | 9909 (24.6%) |
| 71–77 years | 1083 (25.4%) | 1099 (25.7%) | 2130 (25.9%) | 9353 (23.2%) |
| ≥78 years | 1028 (24.1%) | 1188 (27.8%) | 2175 (26.4%) | 10,179 (25.3%) |
| Sex | ||||
| Female | 2213 (51.8%) | 2182 (51.1%) | 4280 (52.0%) | 21,200 (52.7%) |
| Male | 2058 (48.2%) | 2089 (48.9%) | 3948 (48.0%) | 19,060 (47.3%) |
| Smoking | ||||
| Active | 1508 (35.3%) | 1255 (29.4%) | 2718 (33.0%) | 13,826 (34.3%) |
| Former smoker/never smoked | 2394 (56.1%) | 2648 (62.0%) | 4874 (59.2%) | 22,626 (56.2%) |
| Missing data | 372 (8.7%) | 368 (8.6%) | 636 (7.73%) | 3808 (9.5%) |
| BMI | ||||
| ≤18.4 kg/m2 | 268 (6.3%) | 318 (7.5%) | 558 (6.8%) | 3755 (9.3%) |
| 18.5–24.9 kg/m2 | 1452 (34.0%) | 1303 (30.5%) | 2783 (33.8%) | 14,304 (35.5%) |
| 25–30 kg/m2 | 1700 (39.8%) | 1757 (41.1%) | 3194 (38.8%) | 15,699 (38.8%) |
| >30 kg/m2 | 851 (19.9%) | 893 (20.9%) | 1693 (20.6%) | 6501 (16.2%) |
| Missing | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (0.0%) |
| GOLD stage | ||||
| GOLD 1 | 299 (7.0%) | 231 (5.4%) | 496 (6.0%) | 2386 (5.9%) |
| GOLD 2 | 2302 (53.9%) | 1994 (46.7%) | 4059 (49.3%) | 18,364 (45.6%) |
| GOLD 3 | 1352 (31.7%) | 1485 (34.8%) | 2835 (34.5%) | 13,889 (34.5%) |
| GOLD 4 | 318 (7.5%) | 561 (13.1%) | 838 (10.2%) | 5621 (14.0%) |
| Severe exacerbations 12 months prior to baseline | ||||
| 0 | 2937 (68.8%) | 2921 (68.4%) | 5300 (64.4%) | 26,599 (66.1%) |
| 1 | 259 (6.1%) | 257 (6.0%) | 484 (5.9%) | 2346 (5.8%) |
| ≥2 | 1075 (25.2%) | 1093 (25.6%) | 2444 (29.7%) | 11,315(28.1%) |
| Comorbidities | ||||
| Diabetes mellitus | 333 (7.8%) | 238 (5.6%) | 801 (9.7%) | 2187 (5.4%) |
| Myocardial infarction | 342 (8.0%) | 226 (5.3%) | 766 (9.3%) | 2391 (5.9%) |
| Peripheral vascular disease | 534 (12.5%) | 373 (8.7%) | 1204 (14.6%) | 3446 (8.6%) |
| Cerebrovascular disease | 417 (9.8%) | 349 (8.2%) | 850 (10.3%) | 2888 (7.2%) |
| Renal failure | 71 (1.7%) | 61 (1.4%) | 622 (7.6%) | 1020 (2.5%) |
| Heart failure | 276 (6.5%) | 280 (6.6%) | 869 (10.6%) | 3954 (9.8%) |
| Depression | 17 (0.4%) | 11 (0.3%) | 52 (0.6%) | 198 (0.5%) |
| Asthma | 268 (6.3%) | 314 (7.4%) | 532 (6.5%) | 2970 (7.4%) |
| Atrial fibrillation | 375 (8.8%) | 437 (10.2%) | 1019 (12.4%) | 4376 (10.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rastoder, E.; Sivapalan, P.; Eklöf, J.; Achir Alispahic, I.; Jordan, A.S.; Laursen, C.B.; Vestbo, J.; Jenkins, C.; Nielsen, R.; Bakke, P.; et al. Calcium Channel Blockers and the Risk of Exacerbation in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Study of 48,488 Outpatients. Biomedicines 2023, 11, 1974. https://doi.org/10.3390/biomedicines11071974
Rastoder E, Sivapalan P, Eklöf J, Achir Alispahic I, Jordan AS, Laursen CB, Vestbo J, Jenkins C, Nielsen R, Bakke P, et al. Calcium Channel Blockers and the Risk of Exacerbation in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Study of 48,488 Outpatients. Biomedicines. 2023; 11(7):1974. https://doi.org/10.3390/biomedicines11071974
Chicago/Turabian StyleRastoder, Ema, Pradeesh Sivapalan, Josefin Eklöf, Imane Achir Alispahic, Alexander Svorre Jordan, Christian B. Laursen, Jørgen Vestbo, Christine Jenkins, Rune Nielsen, Per Bakke, and et al. 2023. "Calcium Channel Blockers and the Risk of Exacerbation in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Study of 48,488 Outpatients" Biomedicines 11, no. 7: 1974. https://doi.org/10.3390/biomedicines11071974
APA StyleRastoder, E., Sivapalan, P., Eklöf, J., Achir Alispahic, I., Jordan, A. S., Laursen, C. B., Vestbo, J., Jenkins, C., Nielsen, R., Bakke, P., Fernandez-Romero, G., Modin, D., Johansen, N., Davidovski, F. S., Biering-Sørensen, T., Carlsen, J., & Jensen, J. U. S. (2023). Calcium Channel Blockers and the Risk of Exacerbation in Patients with Chronic Obstructive Pulmonary Disease: A Nationwide Study of 48,488 Outpatients. Biomedicines, 11(7), 1974. https://doi.org/10.3390/biomedicines11071974