

A Dusty Road for Astronauts
 , ,
, ,  ,
,  , , and
, , and 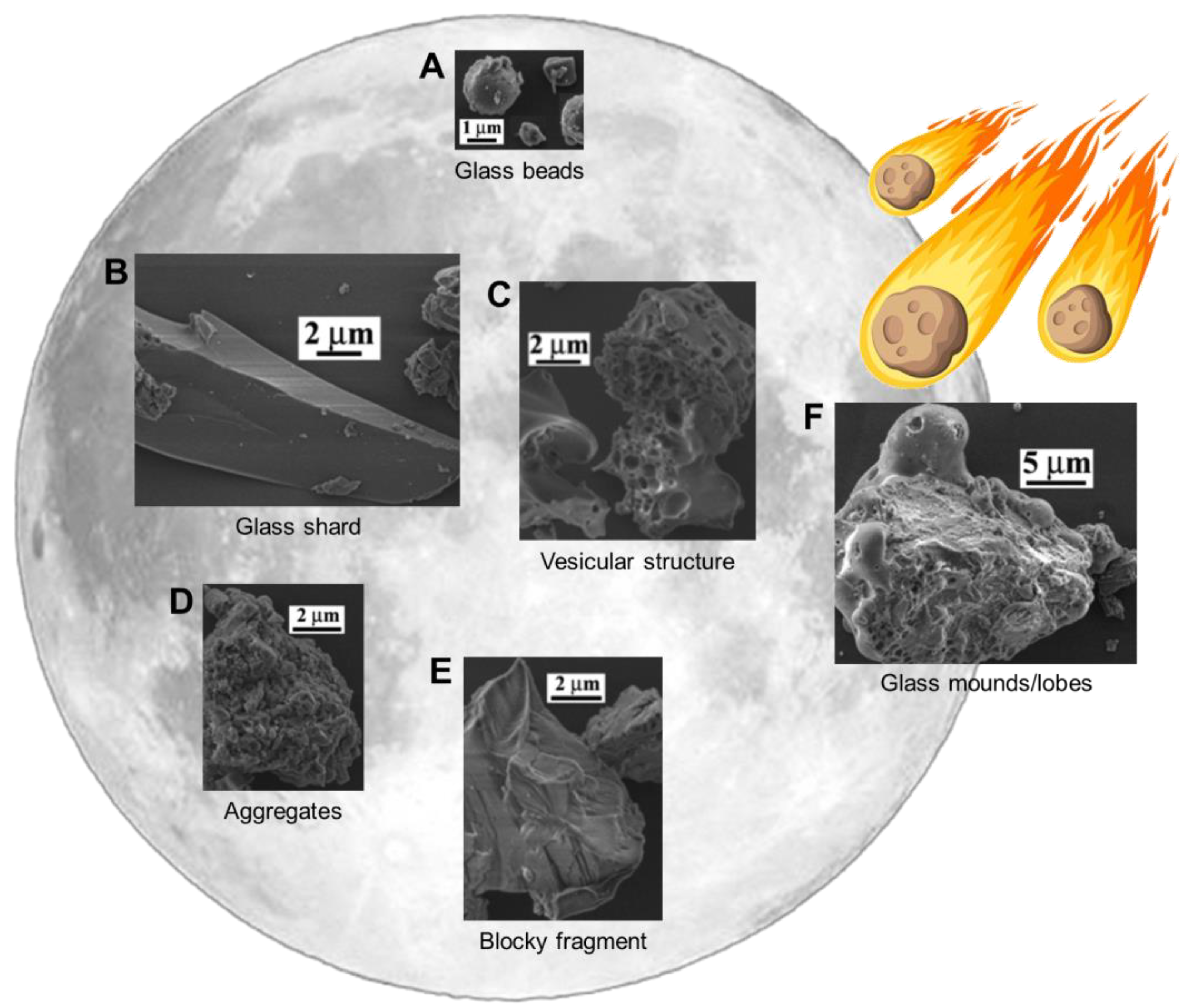{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Lunar Dust Physicochemical Properties
2.1. Creation and Maturation of Lunar Dust
2.2. Grain Shape
- Glassy beads consisting of material that melted due to micrometeoroid impact and was quenched in flight, thus forming round and elongated glassy beads (Figure 1A);
- Angular shards, being glassy in nature and having formed from the breakage or crushing of larger glassy fragments, exhibit sharp edges and an elongated shape (Figure 1B);
- Particles with a vesicular texture, mostly grains with holes or vesicles, were likely left by solar wind volatiles escaping the structure (Figure 1C);
- Aggregated particles, loosely attached or other, larger grains (Figure 1D);
- Blocky fragments, consisting of broken minerals and rocks, with irregular edges due to their formation through breakage (Figure 1E).
2.3. Composition
3. Human Health Effects
3.1. Lessons Learned from Earth
3.2. Formation of Reactive Oxygen Species
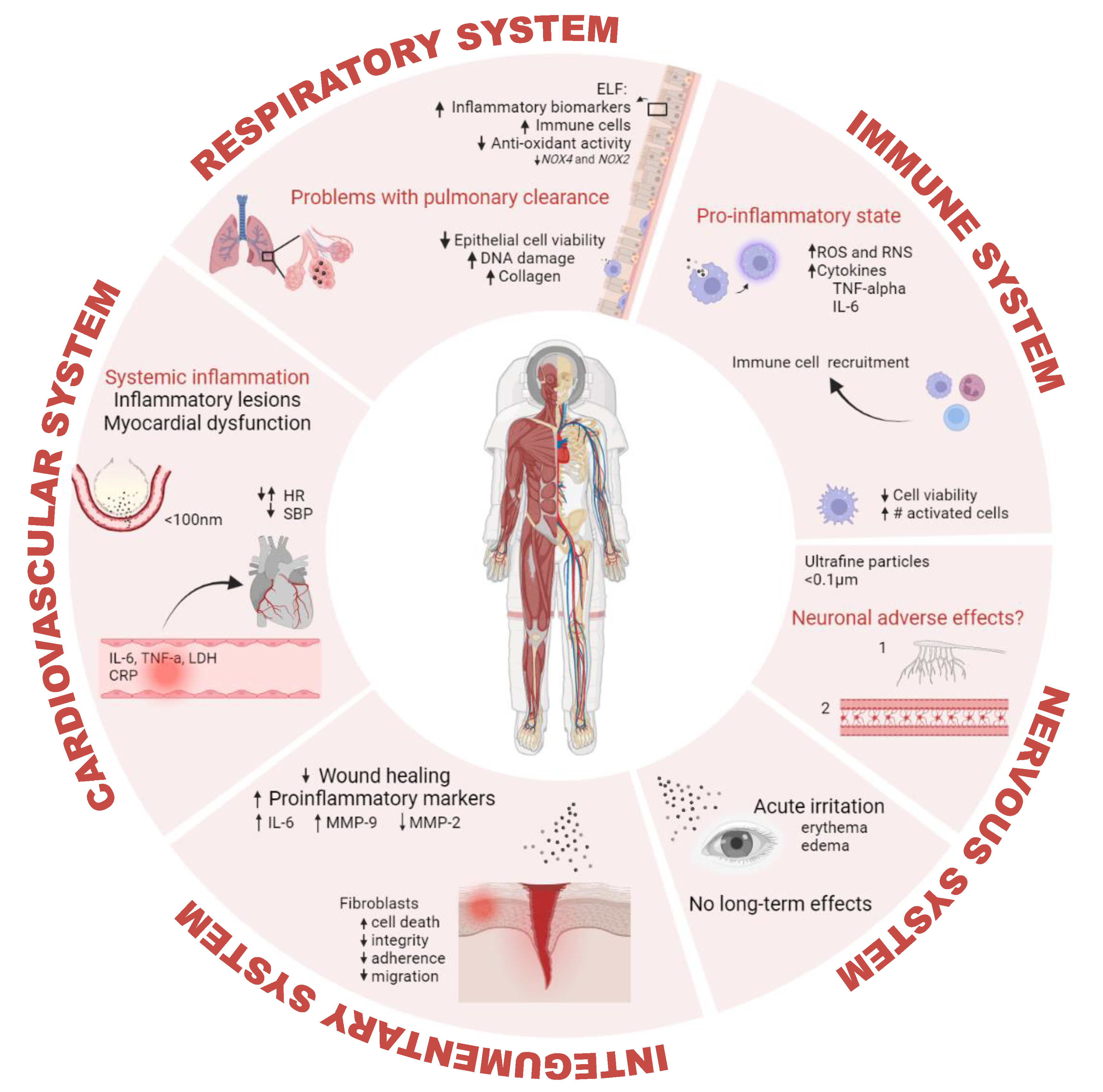
3.3. Organ-Specific Health Effects
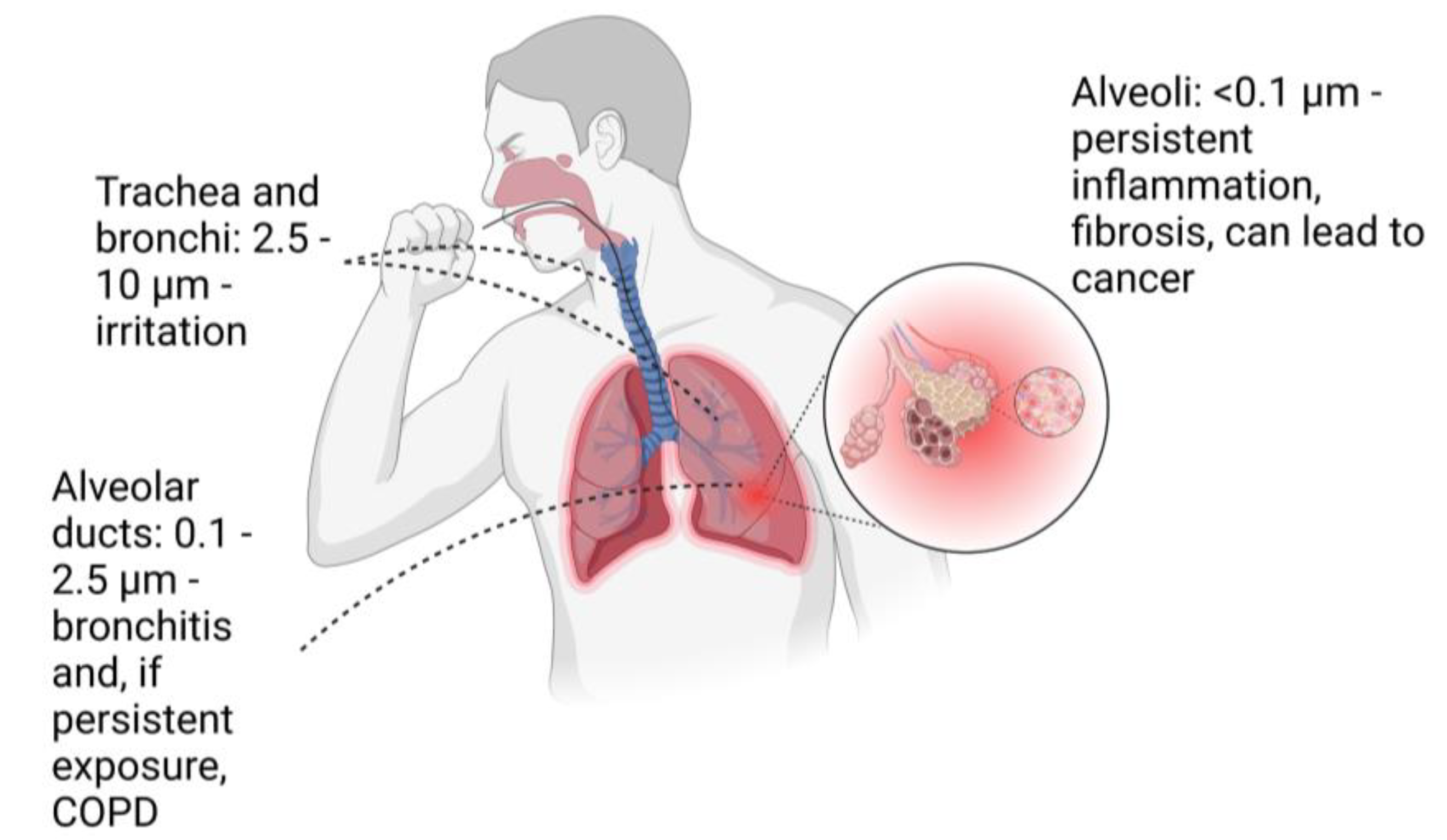
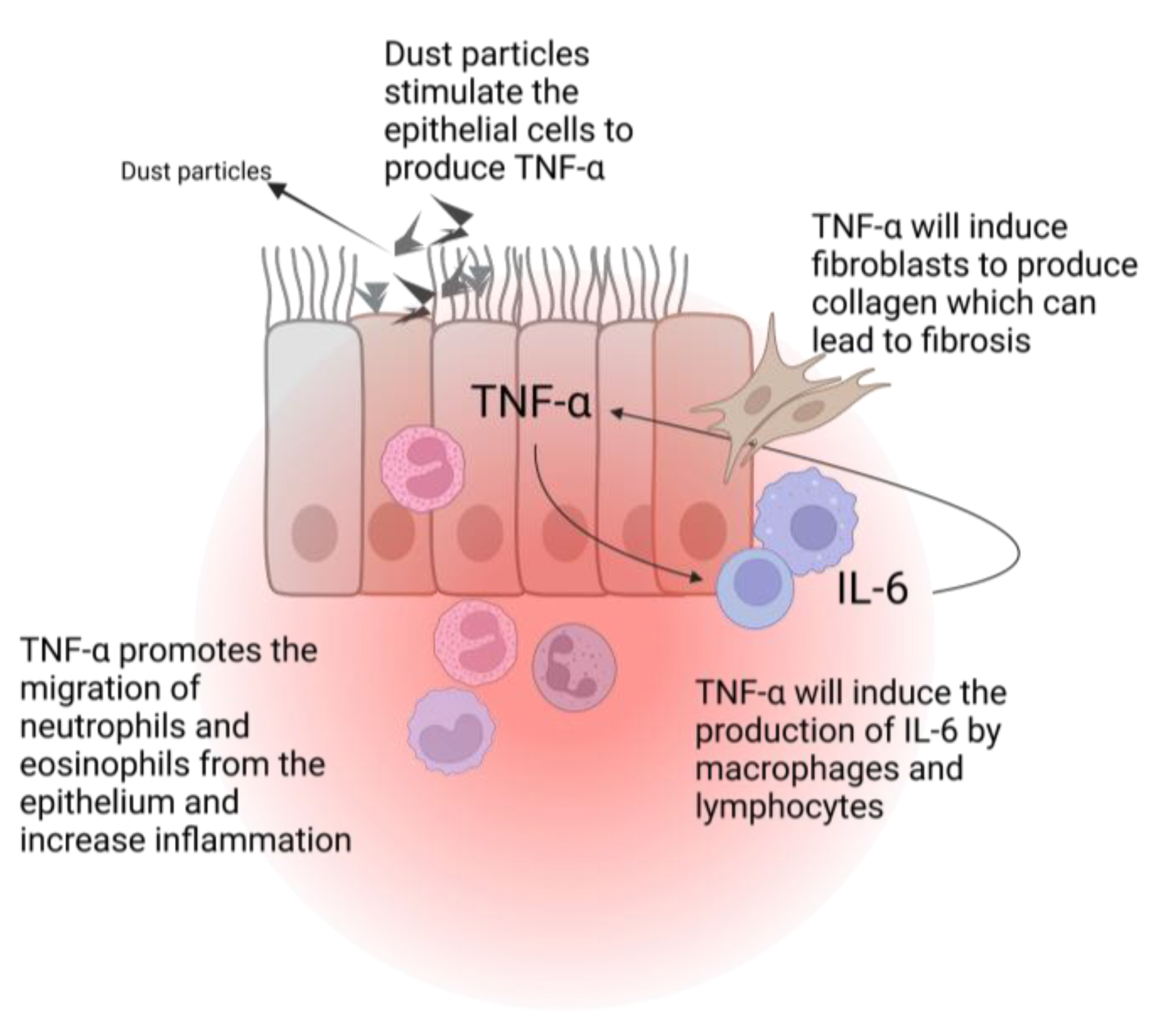
3.3.1. Respiratory Adverse Effects
3.3.2. Immunological Adverse Effects
3.3.3. Cardiovascular Adverse Effects
3.3.4. Dermal Adverse Effects
3.3.5. Ocular and Neuronal Adverse Effects
4. Dust Mitigation and Countermeasures
4.1. Technical Countermeasures
- Dust Generation Avoidance. Encompasses designs and methods that reduce dust generation, such as dust barriers, fixing the surfaces where rovers and other vehicles will traverse on the lunar surface, and reducing the travel speed;
- Passive Mitigation. Special coatings and finishes for the surfaces of instruments will help minimize the adhesion of the lunar dust particles; seals and barriers that prevent the dust from entering the internal mechanisms of certain instruments;
- Active Mitigation. Technologies that will remove dust that has already entered facilities or instruments range from vibrational strategies to pressurized gas, brushes, or magnetic rollers;
- Dust Tolerant Design. Designs and materials that are resistant to the abrasion caused by dust. For example, for bearings, the materials proposed for space applications are zirconia and silicon nitride (ceramic bearings), stainless steel bearings, and superconducting magnetic bearings.
4.2. Biological Countermeasures
4.2.1. Pharmacological Countermeasures
4.2.2. Crew Protection Strategies
4.3. Follow-Up Measures
5. Open Questions for Future Human Space Exploration
5.1. Chronic Effects and Chronic Exposure Effects
5.2. Individual Susceptibility to Lunar Dust
5.3. Combined Effects with Other Space Environmental Factors
6. Research Focus and Future Perspectives
6.1. Advanced In Vitro Models
6.2. Importance of Lunar Dust Simulants
6.3. Lessons for Mars
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heiken, G.H.; Vaniman, D.T.; French, B.M. Lunar Sourcebook, A User’s Guide to the Moon; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Crawford, I.A. The scientific case for renewed human activities on the Moon. Space Policy 2004, 20, 91–97. [Google Scholar] [CrossRef]
- Meurisse, A.; Carpenter, J. Past, the present and future rationale for space resource utilisation. Planet. Space Sci. 2020, 182, 104853. [Google Scholar] [CrossRef]
- NASA. NASA’s Lunar Exploration Program Overview; 2020. Available online: https://www.nasa.gov/sites/default/files/atoms/files/artemis_plan-20200921.pdf (accessed on 13 June 2023).
- NASA. The Artemis Accords: Principles for Cooperation in the Civil Exploration and Use of the Moon, Mars, Comets, and Asteroids. 2020. Available online: https://www.nasa.gov/specials/artemis-accords/img/Artemis-Accords-signed-13Oct2020.pdf (accessed on 13 June 2023).
- ESA. ESA Space Resources Strategy; 2019. Available online: https://sci.esa.int/documents/34161/35992/1567260390250-ESA_Space_Resources_Strategy.pdf (accessed on 13 June 2023).
- ESA. ESA Strategy for Science at the Moon; 2019. Available online: https://exploration.esa.int/web/moon/-/61371-esa-strategy-for-science-at-the-moon (accessed on 13 June 2023).
- Xu, F.; Ou, J. Promoting international cooperation on the International Lunar Research Station: Inspiration from the ITER. Acta Astronaut. 2023, 203, 341–350. [Google Scholar] [CrossRef]
- Taylor, L.; Schmitt, H.; Carrier, W.; Nakagawa, M. The Lunar Dust Problem: From Liability to Asset. In Proceedings of the 1st Space Exploration Conference: Continuing the Voyage of Discovery, Orlando, FL, USA, 30 January–1 February 2005. [Google Scholar] [CrossRef]
- Turci, F.; Corazzari, I.; Alberto, G.; Martra, G.; Fubini, B. Free-Radical Chemistry as a Means to Evaluate Lunar Dust Health Hazard in View of Future Missions to the Moon. Astrobiology 2015, 15, 371–380. [Google Scholar] [CrossRef]
- Benaroya, H. Lunar Habitats: A Brief Overview of Issues and Concepts. Reach 2018, 7–8, 14–33. [Google Scholar] [CrossRef]
- Grün, E.; Horanyi, M.; Sternovsky, Z. The lunar dust environment. Planet. Space Sci. 2011, 59, 1672–1680. [Google Scholar] [CrossRef]
- Colwell, J.E.; Batiste, S.; Horányi, M.; Robertson, S.; Sture, S. Lunar surface: Dust dynamics and regolith mechanics. Rev. Geophys. 2007, 45. [Google Scholar] [CrossRef]
- Zakharov, A.V.; Zelenyi, L.M.; Popel’, S.I. Lunar Dust: Properties and Potential Hazards. Sol. Syst. Res. 2020, 54, 455–476. [Google Scholar] [CrossRef]
- Bhardwaj, A.; Dhanya, M.B.; Alok, A.; Barabash, S.; Wieser, M.; Futaana, Y.; Wurz, P.; Vorburger, A.; Holmström, M.; Lue, C.; et al. A new view on the solar wind interaction with the Moon. Geosci. Lett. 2015, 2, 10. [Google Scholar] [CrossRef]
- Liu, Y.; Park, J.; Schnare, D.; Hill, E.; Taylor Lawrence, A. Characterization of Lunar Dust for Toxicological Studies. II: Texture and Shape Characteristics. J. Aerosp. Eng. 2008, 21, 272–279. [Google Scholar] [CrossRef]
- Park, J.; Liu, Y.; Kihm Kenneth, D.; Taylor Lawrence, A. Characterization of Lunar Dust for Toxicological Studies. I: Particle Size Distribution. J. Aerosp. Eng. 2008, 21, 266–271. [Google Scholar] [CrossRef]
- Liu, Y.; Taylor, L.A. Characterization of lunar dust and a synopsis of available lunar simulants. Planet. Space Sci. 2011, 59, 1769–1783. [Google Scholar] [CrossRef]
- Linnarsson, D.; Carpenter, J.; Fubini, B.; Gerde, P.; Karlsson, L.L.; Loftus, D.J.; Prisk, G.K.; Staufer, U.; Tranfield, E.M.; van Westrenen, W. Toxicity of lunar dust. Planet. Space Sci. 2012, 74, 57–71. [Google Scholar] [CrossRef]
- Taylor, L.A.; Pieters, C.; Patchen, A.; Taylor, D.-H.S.; Morris, R.V.; Keller, L.P.; McKay, D.S. Mineralogical and chemical characterization of lunar highland soils: Insights into the space weathering of soils on airless bodies. J. Geophys. Res. Planets 2010, 115. [Google Scholar] [CrossRef]
- Wallace, W.T.; Phillips, C.J.; Jeevarajan, A.S.; Chen, B.; Taylor, L.A. Nanophase iron-enhanced chemical reactivity of ground lunar soil. Earth Planet. Sci. Lett. 2010, 295, 571–577. [Google Scholar] [CrossRef]
- Taylor Lawrence, A.; Meek Thomas, T. Microwave Sintering of Lunar Soil: Properties, Theory, and Practice. J. Aerosp. Eng. 2005, 18, 188–196. [Google Scholar] [CrossRef]
- Fujimura, N. Pathology and pathophysiology of pneumoconiosis. Curr. Opin. Pulm. Med. 2000, 6, 140–144. [Google Scholar] [CrossRef]
- Qi, X.M.; Luo, Y.; Song, M.Y.; Liu, Y.; Shu, T.; Liu, Y.; Pang, J.L.; Wang, J.; Wang, C. Pneumoconiosis: Current status and future prospects. Chin. Med. J. 2021, 134, 898–907. [Google Scholar] [CrossRef]
- McKay, D.S.; Carter, J.L.; Boles, W.W.; Allen, C.C.; Allton, J.H. JSC-1: A New Lunar Regolith Simulant. In Engineering, Construction, and Operations in Space IV; American Society of Civil Engineers: Reston, VA, USA, 1994; pp. 857–866. [Google Scholar]
- Dubinsky, A.Y.; Popel, S.I. On a Possible Process for the Formation of Iron Oxide in the Lunar Regolith. Sol. Syst. Res. 2021, 55, 309–314. [Google Scholar] [CrossRef]
- Guo, Z.; Li, C.; Li, Y.; Wen, Y.; Wu, Y.; Jia, B.; Tai, K.; Zeng, X.; Li, X.; Liu, J.; et al. Sub-microscopic magnetite and metallic iron particles formed by eutectic reaction in Chang’E-5 lunar soil. Nat. Commun. 2022, 13, 7177. [Google Scholar] [CrossRef]
- Kim, B.E.; Kim, J.; Goleva, E.; Berdyshev, E.; Lee, J.; Vang, K.A.; Lee, U.H.; Han, S.; Leung, S.; Hall, C.F.; et al. Particulate matter causes skin barrier dysfunction. JCI Insightig. 2021, 6, e145185. [Google Scholar] [CrossRef] [PubMed]
- Scully, R.R.; Meyers, V.E. Risk of Adverse Health and Performance Effects of Celestial Dust Exposure; NASA Technical Reports Server: Austin, TX, USA, 2015. [Google Scholar]
- Wallace, W.T.; Taylor, L.A.; Liu, Y.; Cooper, B.L.; Mckay, D.S.; Chen, B.; Jeevarajan, A.S. Lunar dust and lunar simulant activation and monitoring. Meteorit. Planet. Sci. 2009, 44, 961–970. [Google Scholar] [CrossRef]
- Nel, A.; Xia, T.; Mädler, L.; Li, N. Toxic Potential of Materials at the Nanolevel. Science 2006, 311, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Nel, A.E.; Mädler, L.; Velegol, D.; Xia, T.; Hoek, E.M.V.; Somasundaran, P.; Klaessig, F.; Castranova, V.; Thompson, M. Understanding biophysicochemical interactions at the nano–bio interface. Nat. Mater. 2009, 8, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Fubini, B.; Otero Areán, C. Chemical aspects of the toxicity of inhaled mineral dusts. Chem. Soc. Rev. 1999, 28, 373–381. [Google Scholar] [CrossRef]
- Geiser, M.; Kreyling, W.G. Deposition and biokinetics of inhaled nanoparticles. Part. Fibre Toxicol. 2010, 7, 2. [Google Scholar] [CrossRef]
- Nemmar, A.; Hoet, P.H.; Vanquickenborne, B.; Dinsdale, D.; Thomeer, M.; Hoylaerts, M.F.; Vanbilloen, H.; Mortelmans, L.; Nemery, B. Passage of inhaled particles into the blood circulation in humans. Circulation 2002, 105, 411–414. [Google Scholar] [CrossRef]
- Mills, N.L.; Amin, N.; Robinson, S.D.; Anand, A.; Davies, J.; Patel, D.; de la Fuente, J.M.; Cassee, F.R.; Boon, N.A.; Macnee, W.; et al. Do inhaled carbon nanoparticles translocate directly into the circulation in humans? Am. J. Respir. Crit Care Med. 2006, 173, 426–431. [Google Scholar] [CrossRef]
- Peterson, J.B.; Prisk, G.K.; Darquenne, C. Aerosol deposition in the human lung periphery is increased by reduced-density gas breathing. J. Aerosol. Med. Pulm. Drug Deliv. 2008, 21, 159–168. [Google Scholar] [CrossRef]
- Darquenne, C.; Prisk, G.K. Deposition of inhaled particles in the human lung is more peripheral in lunar than in normal gravity. Eur. J. Appl. Physiol. 2008, 103, 687–695. [Google Scholar] [CrossRef]
- Prisk, G.K. Pulmonary challenges of prolonged journeys to space: Taking your lungs to the moon. Med. J. Aust. 2019, 211, 271–276. [Google Scholar] [CrossRef]
- Prisk, G.K. Microgravity and the respiratory system. Eur. Respir. J. 2014, 43, 1459–1471. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, J.G.; Zheng, Y.C.; Xiao, C.L.; Wan, B.; Guo, L.; Wang, X.G.; Bo, W. Research on rat’s pulmonary acute injury induced by lunar soil simulant. J. Chin. Med. Assoc. 2018, 81, 133–140. [Google Scholar] [CrossRef]
- Kaur, J.; Rickman, D.; Schoonen, M.A. Reactive Oxygen Species (ROS) generation by lunar simulants. Acta Astronaut. 2016, 122, 196–208. [Google Scholar] [CrossRef]
- Lam, C.W.; Scully, R.R.; Zhang, Y.; Renne, R.A.; Hunter, R.L.; McCluskey, R.A.; Chen, B.T.; Castranova, V.; Driscoll, K.E.; Gardner, D.E.; et al. Toxicity of lunar dust assessed in inhalation-exposed rats. Inhal. Toxicol. 2013, 25, 661–678. [Google Scholar] [CrossRef] [PubMed]
- Mikuz, G.; Gschwendtner, A. Value of bronchoalvoeolar lavage in the diagnosis of lung disease. Verh. Dtsch. Ges. Pathol. 2000, 84, 129–135. [Google Scholar]
- Yan, S.; Guo, L.J.; Di, K.Y.; Sen, H.J.; Ping, Z.X. Effects of Lunar Soil Simulant on Systemic Oxidative Stress and Immune Response in Acute Rat Lung Injury. Int. J. Pharmacol. 2018, 14, 766–772. [Google Scholar] [CrossRef]
- Cuo, G.; Xia, Y.; Niu, P.; Jiang, L.; Duan, J.; Yu, Y.; Zhou, X.; Li, Y.; Sun, Z. Silica nanoparticles induce oxidative stress, inflammation, and endothelial dysfunction in vitro via activation of the MAPK/Nrf2 pathway and nuclear factor-κB signaling. Int. J. Nanomed. 2015, 10, 1463–1477. [Google Scholar] [CrossRef]
- Wang, G.; Zhao, J.; Jiang, R.; Song, W. Rat lung response to ozone and fine particulate matter (PM2.5) exposures. Environ. Toxicol. 2015, 30, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Kandhare, A.D.; Bodhankar, S.L.; Mohan, V.; Thakurdesai, P.A. Effect of glycosides based standardized fenugreek seed extract in bleomycin-induced pulmonary fibrosis in rats: Decisive role of Bax, Nrf2, NF-κB, Muc5ac, TNF-α and IL-1β. Chem. -Biol. Interact. 2015, 237, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, J.; Zhang, X.; Li, X.; Zhou, B.; Lv, Z. Mechanisms involved in inflammatory pulmonary fibrosis induced by lunar dust simulant in rats. Environ. Toxicol. 2019, 34, 131–140. [Google Scholar] [CrossRef]
- Hamilton, R.F.; de Villiers, W.J.S.; Holian, A. Class A Type II Scavenger Receptor Mediates Silica-Induced Apoptosis in Chinese Hamster Ovary Cell Line. Toxicol. Appl. Pharmacol. 2000, 162, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.W.; James, J.T.; Latch, J.N.; Hamilton, R.F., Jr.; Holian, A. Pulmonary toxicity of simulated lunar and Martian dusts in mice: II. Biomarkers of acute responses after intratracheal instillation. Inhal. Toxicol. 2002, 14, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Latch, J.N.; Hamilton, R.F., Jr.; Holian, A.; James, J.T.; Lam, C.W. Toxicity of lunar and martian dust simulants to alveolar macrophages isolated from human volunteers. Inhal. Toxicol. 2008, 20, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Thompson, K.K.; Nissen, J.C.; Hendrix, D.; Hurowitz, J.A.; Tsirka, S.E. Lunar soil simulants alter macrophage survival and function. J. Appl. Toxicol. 2019, 39, 1413–1423. [Google Scholar] [CrossRef]
- Crucian, B.E.; Chouker, A.; Simpson, R.J.; Mehta, S.; Marshall, G.; Smith, S.M.; Zwart, S.R.; Heer, M.; Ponomarev, S.; Whitmire, A.; et al. Immune System Dysregulation During Spaceflight: Potential Countermeasures for Deep Space Exploration Missions. Front. Immunol. 2018, 9, 1437. [Google Scholar] [CrossRef]
- Sun, Y.; Zhang, L.; Liu, J.; Zhang, X.; Su, Y.; Yin, Q.; He, S. Effects of lunar dust simulant on cardiac function and fibrosis in rats. Toxicol. Res. 2019, 8, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of inhaled ultrafine particles to the brain. Inhal. Toxicol. 2004, 16, 437–445. [Google Scholar] [CrossRef]
- Peters, A.; Veronesi, B.; Calderón-Garcidueñas, L.; Gehr, P.; Chen, L.C.; Geiser, M.; Reed, W.; Rothen-Rutishauser, B.; Schürch, S.; Schulz, H. Translocation and potential neurological effects of fine and ultrafine particles a critical update. Part Fibre Toxicol. 2006, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Semmler, M.; Seitz, J.; Erbe, F.; Mayer, P.; Heyder, J.; Oberdörster, G.; Kreyling, W.G. Long-term clearance kinetics of inhaled ultrafine insoluble iridium particles from the rat lung, including transient translocation into secondary organs. Inhal. Toxicol. 2004, 16, 453–459. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Baez-Ferrer, N.; Rodríguez, S.; Avanzas, P.; Abreu-Gonzalez, P.; Terradellas, E.; Cuevas, E.; Basart, S.; Werner, E. Saharan dust events in the dust belt -canary islands- and the observed association with in-hospital mortality of patients with heart failure. J. Clin. Med. 2020, 9, 376. [Google Scholar] [CrossRef]
- Stafoggia, M.; Zauli-Sajani, S.; Pey, J.; Samoli, E.; Alessandrini, E.; Basagaña, X.; Cernigliaro, A.; Chiusolo, M.; Demaria, M.; Díaz, J.; et al. Desert dust outbreaks in southern europe: Contribution to daily pm10 concentrations and short-term associations with mortality and hospital admissions. Environ. Health Perspect. 2016, 124, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Rublee, C.S.; Sorensen, C.J.; Lemery, J.; Wade, T.J.; Sams, E.A.; Hilborn, E.D.; Crooks, J.L. Associations between dust storms and intensive care unit admissions in the United States, 2000–2015. Geohealth 2020, 4, e2020GH000260. [Google Scholar] [CrossRef] [PubMed]
- Rowe, W.J. Moon Dust may Simulate Vascular Hazards of Urban Pollution. J. Br. Interplanet. Soc. 2007, 60, 133–136. [Google Scholar]
- Seaton, A.; MacNee, W.; Donaldson, K.; Godden, D. Particulate air pollution and acute health effects. Lancet 1995, 345, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Seaton, A.; Soutar, A.; Crawford, V.; Elton, R.; McNerlan, S.; Cherrie, J.; Watt, M.; Agius, R.; Stout, R. Particulate air pollution and the blood. Thorax 1999, 54, 1027–1032. [Google Scholar] [CrossRef]
- Tranfield, E.M.; van Eeden, S.F.; Yatera, K.; Hogg, J.C.; Walker, D.C. Ultrastructural changes in atherosclerotic plaques following the instillation of airborne particulate matter into the lungs of rabbits. Can. J. Cardiol. 2010, 26, e258–e269. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Liu, E.; Verrier, R.L.; Schwartz, J.; Gold, D.R.; Mittleman, M.; Baliff, J.; Oh, J.A.; Allen, G.; Monahan, K.; et al. Air pollution and incidence of cardiac arrhythmia. Epidemiology 2000, 11, 11–17. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Verrier, R.L.; Lovett, E.G.; Larson, A.C.; Raizenne, M.E.; Kanner, R.E.; Schwartz, J.; Villegas, G.M.; Gold, D.R.; Dockery, D.W. Heart rate variability associated with particulate air pollution. Am. Heart J. 1999, 138, 890–899. [Google Scholar] [CrossRef]
- Rowe, W.J. Neil Armstrong’s Lunar Diastolic Hypertension. J. Hypertens Manag. 2017, 3, 029. [Google Scholar] [CrossRef]
- Rehders, M.; Grosshäuser, B.B.; Smarandache, A.; Sadhukhan, A.; Mirastschijski, U.; Kempf, J.; Dünne, M.; Slenzka, K.; Brix, K. Effects of lunar and mars dust simulants on HaCaT keratinocytes and CHO-K1 fibroblasts. Adv. Space Res. 2011, 47, 1200–1213. [Google Scholar] [CrossRef]
- Pohlen, M.; Carroll, D.; Prisk, G.K.; Sawyer, A.J. Overview of lunar dust toxicity risk. Npj Microgravity 2022, 8, 55. [Google Scholar] [CrossRef] [PubMed]
- Radstake, W.E.; Baselet, B.; Baatout, S.; Verslegers, M. Spaceflight Stressors and Skin Health. Biomedicines 2022, 10, 364. [Google Scholar] [CrossRef]
- Jones, L.; Jacques, S.; Tranfield, E.; Rask, J.; Kerschmann, R.; Loftus, D. Skin Abrasion Effects of Lunar Dust Relevant to Astronauts. In Proceedings of the 39th Annual Lunar Planetary Science Conference, League City, Texas, 1 March 2008; p. 2541. [Google Scholar]
- Monici, M.; Cialdai, F.; Lulli, M.; Capaccioli, S.; Marziliano, N.; Sundaresan, A. Effect of lunar dust simulant on wound healing: An in vitro study. Eur. Space Agency ESA SP 2013, 706, 2. [Google Scholar]
- Ahmadli, G.; Schnabel, R.; Jokuszies, A.; Vogt, P.M.; Zier, U.; Mirastschijski, U. Impact of Martian and Lunar dust simulants on cellular inflammation in human skin wounds ex vivo. Handchir. Mikrochir. Plast. Chir. 2014, 46, 361–368. [Google Scholar] [CrossRef]
- Meyers, V.E.; Garcìa, H.D.; Monds, K.; Cooper, B.L.; James, J.T. Ocular toxicity of authentic lunar dust. BMC Ophthalmol. 2012, 12, 26. [Google Scholar] [CrossRef]
- Fraunfelder, F.T.; Kalina, R.E.; Buist, A.S.; Bernstein, R.S.; Johnson, D.S. Ocular effects following the volcanic eruptions of Mount St Helens. Arch. Ophthalmol. 1983, 101, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Mu, H.; Battsetseg, B.; Ito, T.Y.; Otani, S.; Onishi, K.; Kurozawa, Y. Health effects of dust storms: Subjective eye and respiratory system symptoms in inhabitants in Mongolia. J. Environ. Health 2011, 73, 18–20. [Google Scholar] [PubMed]
- Kimura, K.; Sakamoto, T.; Miyazaki, M.; Uchino, E.; Kinukawa, N.; Isashiki, M. Effects of volcanic ash on ocular symptoms: Results of a 10-year survey on schoolchildren. Ophthalmology 2005, 112, 478–481. [Google Scholar] [CrossRef]
- Krisanova, N.; Kasatkina, L.; Sivko, R.; Borysov, A.; Nazarova, A.; Slenzka, K.; Borisova, T. Neurotoxic potential of lunar and martian dust: Influence on em, proton gradient, active transport, and binding of glutamate in rat brain nerve terminals. Astrobiology 2013, 13, 679–692. [Google Scholar] [CrossRef]
- Boyes, W.K.; van Thriel, C. Neurotoxicology of Nanomaterials. Chem. Res. Toxicol. 2020, 33, 1121–1144. [Google Scholar] [CrossRef]
- Cannon, K.M.; Dreyer, C.B.; Sowers, G.F.; Schmit, J.; Nguyen, T.; Sanny, K.; Schertz, J. Working with lunar surface materials: Review and analysis of dust mitigation and regolith conveyance technologies. Acta Astronaut. 2022, 196, 259–274. [Google Scholar] [CrossRef]
- Carr, C.E.; Newman, D.J. Space suit bioenergetics: Framework and analysis of unsuited and suited activity. Aviat. Space Environ. Med. 2007, 78, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.J. Life in extreme environments: How will humans perform on Mars? Gravit. Space Biol. 2000, 13, 35–47. [Google Scholar] [PubMed]
- Christoffersen, R.; Lindsay, J.; Noble, S.; Lawrence, J. Lunar Dust Effects on Spacesuit Systems: Insights from the Apollo Spacesuits. 2008. Available online: https://www.lpi.usra.edu/lunar/strategies/ChristoffersenEtAl_NASA-TP-2009-214786_LunarDustEffectsSpacesuitSystems.pdf (accessed on 13 June 2023).
- Manyapu, K.K.; Peltz, L.; De Leon, P. Self-cleaning spacesuits for future planetary missions using carbon nanotube technology. Acta Astronaut. 2019, 157, 134–144. [Google Scholar] [CrossRef]
- Jarman, E.R.; Khambata, V.S.; Cope, C.; Jones, P.; Roger, J.; Ye, L.Y.; Duggan, N.; Head, D.; Pearce, A.; Press, N.J.; et al. An inhibitor of NADPH oxidase-4 attenuates established pulmonary fibrosis in a rodent disease model. Am. J. Respir. Cell Mol. Biol. 2014, 50, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Hector, A.; Griese, M.; Hartl, D. Oxidative stress in cystic fibrosis lung disease: An early event, but worth targeting? Eur. Respir. J. 2014, 44, 17–19. [Google Scholar] [CrossRef]
- Gaylor, D.W. The use of Haber’s law in standard setting and risk assessment. Toxicology 2000, 149, 17–19. [Google Scholar] [CrossRef]
- James, J.T.; Lam, C.W.; Santana, P.A.; Scully, R.R. Estimate of safe human exposure levels for lunar dust based on comparative benchmark dose modeling. Inhal. Toxicol. 2013, 25, 243–256. [Google Scholar] [CrossRef]
- Klima, R. The Lunar Surface Innovation Consortium (LSIC). In Proceedings of the 44th COSPAR Scientific Assembly, Athens, Greece, 16–24 July 2022; p. 296. [Google Scholar]
- NASA. Medical Examination Requirements (MER) for Former Astronauts. Available online: https://www.nasa.gov/hhp/medical-examination-requirements (accessed on 6 April 2023).
- Ghatak, S.; Hascall, V.C.; Markwald, R.R.; Feghali-Bostwick, C.; Artlett, C.M.; Gooz, M.; Bogatkevich, G.S.; Atanelishvili, I.; Silver, R.M.; Wood, J.; et al. Transforming growth factor β1 (TGFβ1)-induced CD44V6-NOX4 signaling in pathogenesis of idiopathic pulmonary fibrosis. J. Biol. Chem. 2017, 292, 10490–10519. [Google Scholar] [CrossRef]
- Caston, R.; Luc, K.; Hendrix, D.; Hurowitz, J.A.; Demple, B. Assessing Toxicity and Nuclear and Mitochondrial DNA Damage Caused by Exposure of Mammalian Cells to Lunar Regolith Simulants. GeoHealth 2018, 2, 139–148. [Google Scholar] [CrossRef]
- Yauk, C.; Polyzos, A.; Rowan-Carroll, A.; Somers, C.M.; Godschalk, R.W.; Van Schooten, F.J.; Berndt, M.L.; Pogribny, I.P.; Koturbash, I.; Williams, A.; et al. Germ-line mutations, DNA damage, and global hypermethylation in mice exposed to particulate air pollution in an urban/industrial location. Proc. Natl. Acad. Sci. USA 2008, 105, 605–610. [Google Scholar] [CrossRef]
- Upadhyay, D.; Panduri, V.; Ghio, A.; Kamp, D.W. Particulate matter induces alveolar epithelial cell DNA damage and apoptosis: Role of free radicals and the mitochondria. Am. J. Respir. Cell Mol. Biol. 2003, 29, 180–187. [Google Scholar] [CrossRef]
- Azmanova, M.; Pitto-Barry, A. Oxidative Stress in Cancer Therapy: Friend or Enemy? Chembiochem A Eur. J. Chem. Biol. 2022, 23, e202100641. [Google Scholar] [CrossRef]
- Sato, T.; Shimosato, T.; Klinman, D.M. Silicosis and lung cancer: Current perspectives. Lung Cancer 2018, 9, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Norseth, T. The carcinogenicity of chromium. Environ. Health Perspect. 1981, 40, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.D.; Stanek, L.W.; Luben, T.J.; Johns, D.O.; Buckley, B.J.; Brown, J.S.; Ross, M. Particulate matter-induced health effects: Who is susceptible? Environ. Health Perspect. 2011, 119, 446–454. [Google Scholar] [CrossRef] [PubMed]
- ESA. Astronaut Selection 2021-22 FAQs. Available online: https://www.esa.int/About_Us/Careers_at_ESA/ESA_Astronaut_Selection/Astronaut_selection_2021-22_FAQs#Eligibility%20and%20how%20to%20apply (accessed on 6 April 2023).
- Peake, T.; ESA. The Astronaut Selection Test Book: Do You Have What It Takes for Space? Cornerstone: Katy, TX, USA, 2019. [Google Scholar]
- Durante, M.; Cucinotta, F.A. Heavy ion carcinogenesis and human space exploration. Nat. Rev. Cancer 2008, 8, 465–472. [Google Scholar] [CrossRef]
- Afshinnekoo, E.; Scott, R.T.; MacKay, M.J.; Pariset, E.; Cekanaviciute, E.; Barker, R.; Gilroy, S.; Hassane, D.; Smith, S.M.; Zwart, S.R.; et al. Fundamental Biological Features of Spaceflight: Advancing the Field to Enable Deep-Space Exploration. Cell 2020, 183, 1162–1184. [Google Scholar] [CrossRef]
- Spence, H.E.; Case, A.W.; Golightly, M.J.; Heine, T.; Larsen, B.A.; Blake, J.B.; Caranza, P.; Crain, W.R.; George, J.; Lalic, M.; et al. CRaTER: The Cosmic Ray Telescope for the Effects of Radiation Experiment on the Lunar Reconnaissance Orbiter Mission. Space Sci. Rev. 2010, 150, 243–284. [Google Scholar] [CrossRef]
- Wiese-Rischke, C.; Murkar, R.S.; Walles, H. Biological Models of the Lower Human Airways-Challenges and Special Requirements of Human 3D Barrier Models for Biomedical Research. Pharmaceutics 2021, 13, 2115. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; Teng, Y. Is It Time to Start Transitioning From 2D to 3D Cell Culture? Front. Mol. Biosci. 2020, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, S.; Singh, S. Cultivating human tissues and organs over lab-on-a-chip models: Recent progress and applications. Prog. Mol. Biol. Transl. Sci. 2022, 187, 205–240. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.M.; de Haan, P.; Ronaldson-Bouchard, K.; Kim, G.-A.; Ko, J.; Rho, H.S.; Chen, Z.; Habibovic, P.; Jeon, N.L.; Takayama, S.; et al. A guide to the organ-on-a-chip. Nat. Rev. Methods Prim. 2022, 2, 33. [Google Scholar] [CrossRef]
- Yang, J.-W.; Shen, Y.-C.; Lin, K.-C.; Cheng, S.-J.; Chen, S.-L.; Chen, C.-Y.; Kumar, P.V.; Lin, S.-F.; Lu, H.-E.; Chen, G.-Y. Organ-on-a-Chip: Opportunities for Assessing the Toxicity of Particulate Matter. Front. Bioeng. Biotechnol. 2020, 8, 519. [Google Scholar] [CrossRef]
- Mu, X.; He, W.; Rivera, V.A.M.; De Alba, R.A.D.; Newman, D.J.; Zhang, Y.S. Small tissue chips with big opportunities for space medicine. Life Sci. Space Res. 2022, 35, 150–157. [Google Scholar] [CrossRef]
- Singh, D.; Mathur, A.; Arora, S.; Roy, S.; Mahindroo, N. Journey of organ on a chip technology and its role in future healthcare scenario. Appl. Surf. Sci. Adv. 2022, 9, 100246. [Google Scholar] [CrossRef]
- Taylor, L.; Pieters, C.; Britt, D. Evaluations of lunar regolith simulants. Planet. Space Sci. 2016, 126, 1–7. [Google Scholar] [CrossRef]
- Long-Fox, J.M.; Landsman, Z.A.; Easter, P.B.; Millwater, C.A.; Britt, D.T. Geomechanical properties of lunar regolith simulants lhs-1 and lms-1. Adv. Space Res. 2023, 71, 5400–5412. [Google Scholar] [CrossRef]
- Stoeser, D.; Rickman, D.; Wilson, S. Design and Specifications for the Highland Regolith Prototype Simulants NU-LHT-1M and-2M; NASA Technical Reports Server: Austin, TX, USA, 2011. [Google Scholar]
- Council, N.R. Safe on Mars: Precursor Measurements Necessary to Support Human Operations on the Martian Surface; The National Academies Press: Washington, DC, USA, 2002; p. 64. [Google Scholar]
- Geib, C. The Biggest Health Risk for Lunar and Martian Explorers: Tiny Dust. Available online: https://futurism.com/extraterrestrial-dust-moon-mars-health (accessed on 6 April 2023).
- NASA. Why Colonize the Moon before Going to Mars? NASA Scientists Give Their Reasons. Available online: https://www.nasa.gov/audience/forstudents/postsecondary/features/18mar_moonfirst_prt.htm (accessed on 6 April 2023).
- Calle, C.I. The electrostatic environments of Mars and the Moon. J. Phys. Conf. Ser. 2011, 301, 012006. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, S.; Marchal, S.; Cumps, L.; Dierckx, J.; Krüger, M.; Grimm, D.; Baatout, S.; Tabury, K.; Baselet, B. A Dusty Road for Astronauts. Biomedicines 2023, 11, 1921. https://doi.org/10.3390/biomedicines11071921
Miranda S, Marchal S, Cumps L, Dierckx J, Krüger M, Grimm D, Baatout S, Tabury K, Baselet B. A Dusty Road for Astronauts. Biomedicines. 2023; 11(7):1921. https://doi.org/10.3390/biomedicines11071921
Chicago/Turabian StyleMiranda, Silvana, Shannon Marchal, Lina Cumps, Jenne Dierckx, Marcus Krüger, Daniela Grimm, Sarah Baatout, Kevin Tabury, and Bjorn Baselet. 2023. "A Dusty Road for Astronauts" Biomedicines 11, no. 7: 1921. https://doi.org/10.3390/biomedicines11071921
APA StyleMiranda, S., Marchal, S., Cumps, L., Dierckx, J., Krüger, M., Grimm, D., Baatout, S., Tabury, K., & Baselet, B. (2023). A Dusty Road for Astronauts. Biomedicines, 11(7), 1921. https://doi.org/10.3390/biomedicines11071921