


Multiple Omics Analysis of the Role of RBM10 Gene Instability in Immune Regulation and Drug Sensitivity in Patients with Lung Adenocarcinoma (LUAD)

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Download and Acquisition
2.2. Data Algorithmic Processing
2.3. Matrix Deconvolution Analysis of Targeted Drug Sensitivity
2.4. Grouping Analysis of Genomic Instability
2.5. Prognostic Model Construction and Survival Analysis of Prognostic RBP
2.6. GO and KEGG Pathway Enrichment Analysis
2.7. Construction of Protein–Protein Interaction (PPI) and Screening of Key Genes
2.8. PCR Assay Analysis
2.9. Analysis of the Pathological Characteristics of Lung Adenocarcinoma
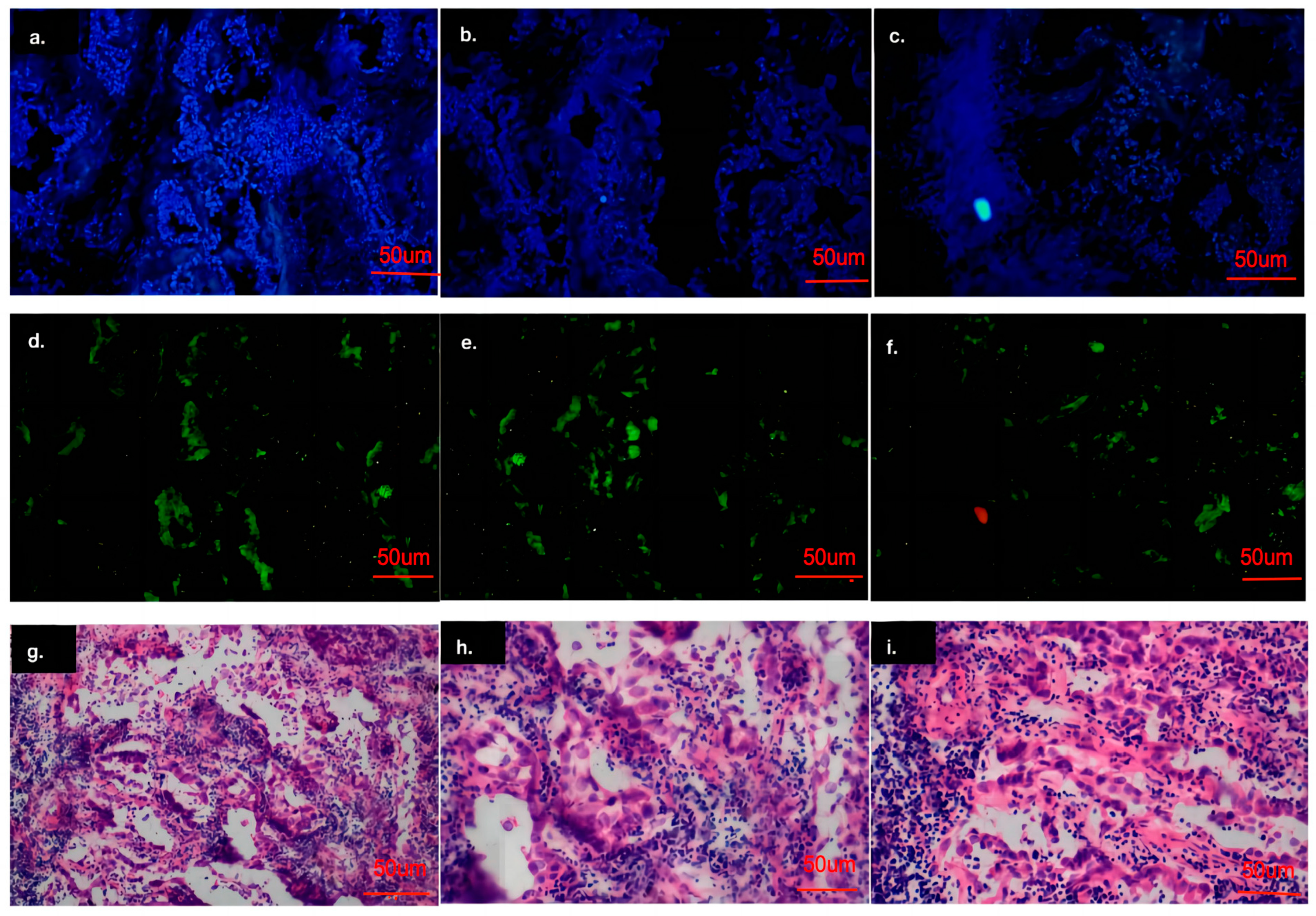
2.10. Immunohistochemical and Cell Immunofluorescence Analysis
3. Results
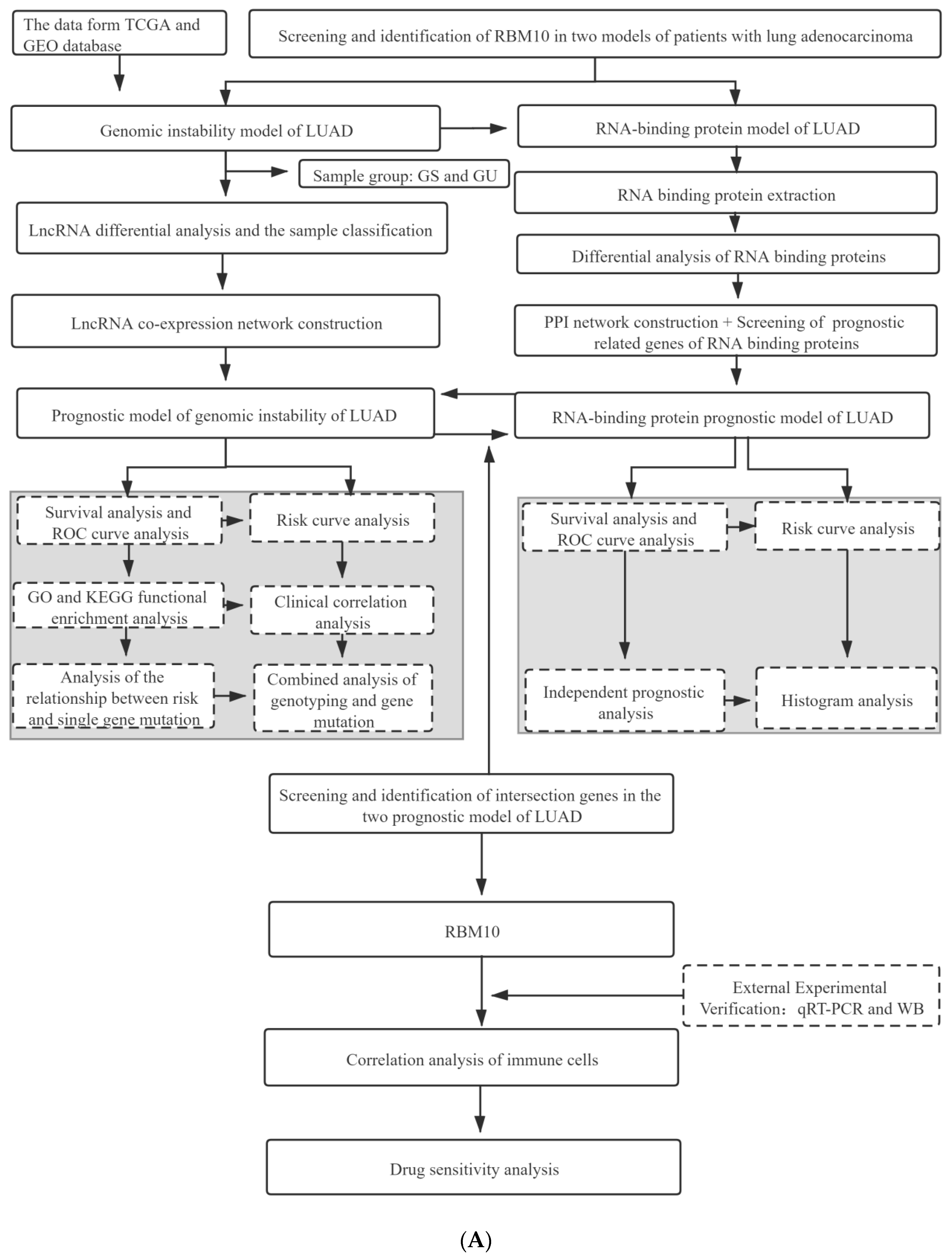
3.1. Project Research and Analysis Process
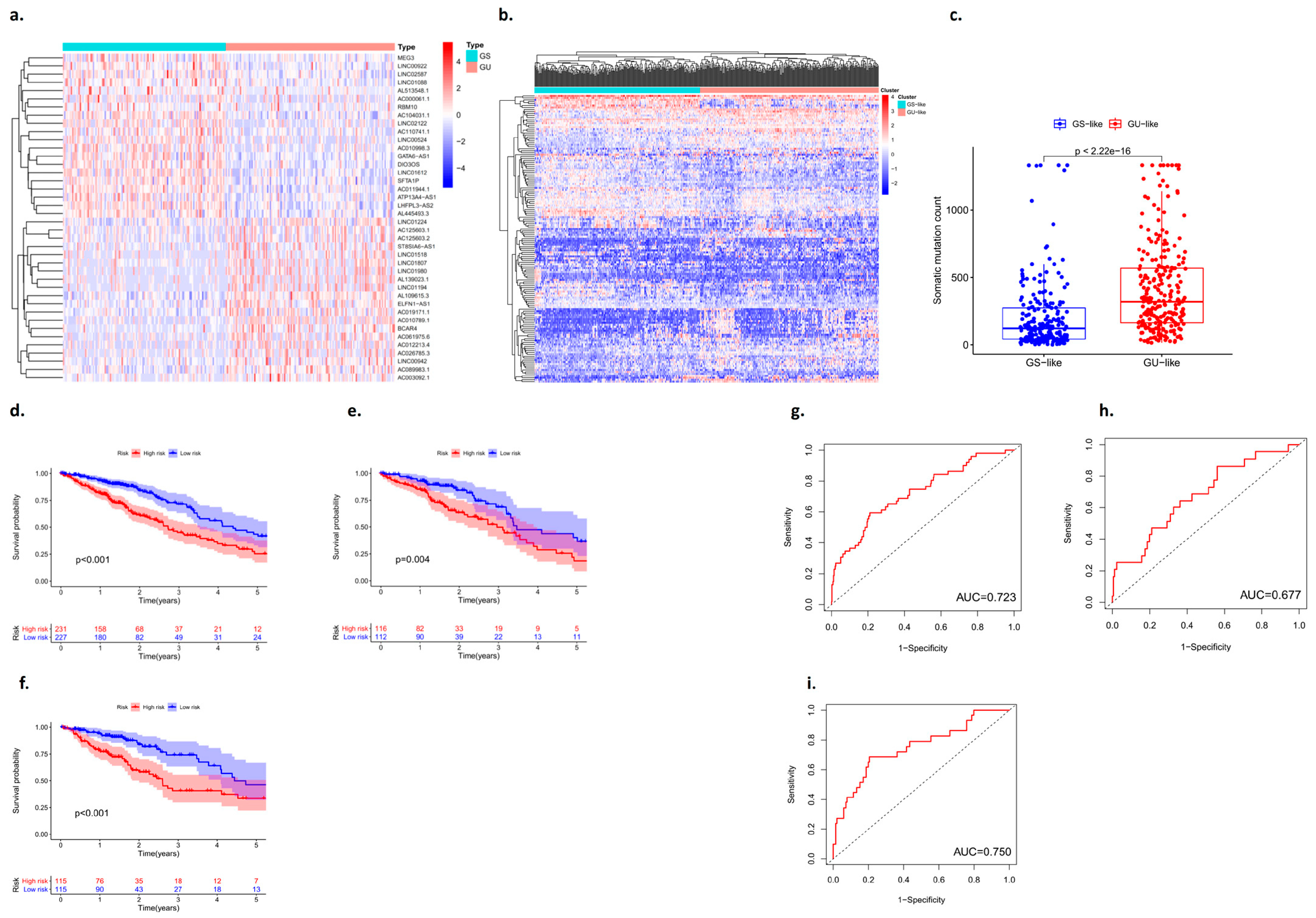
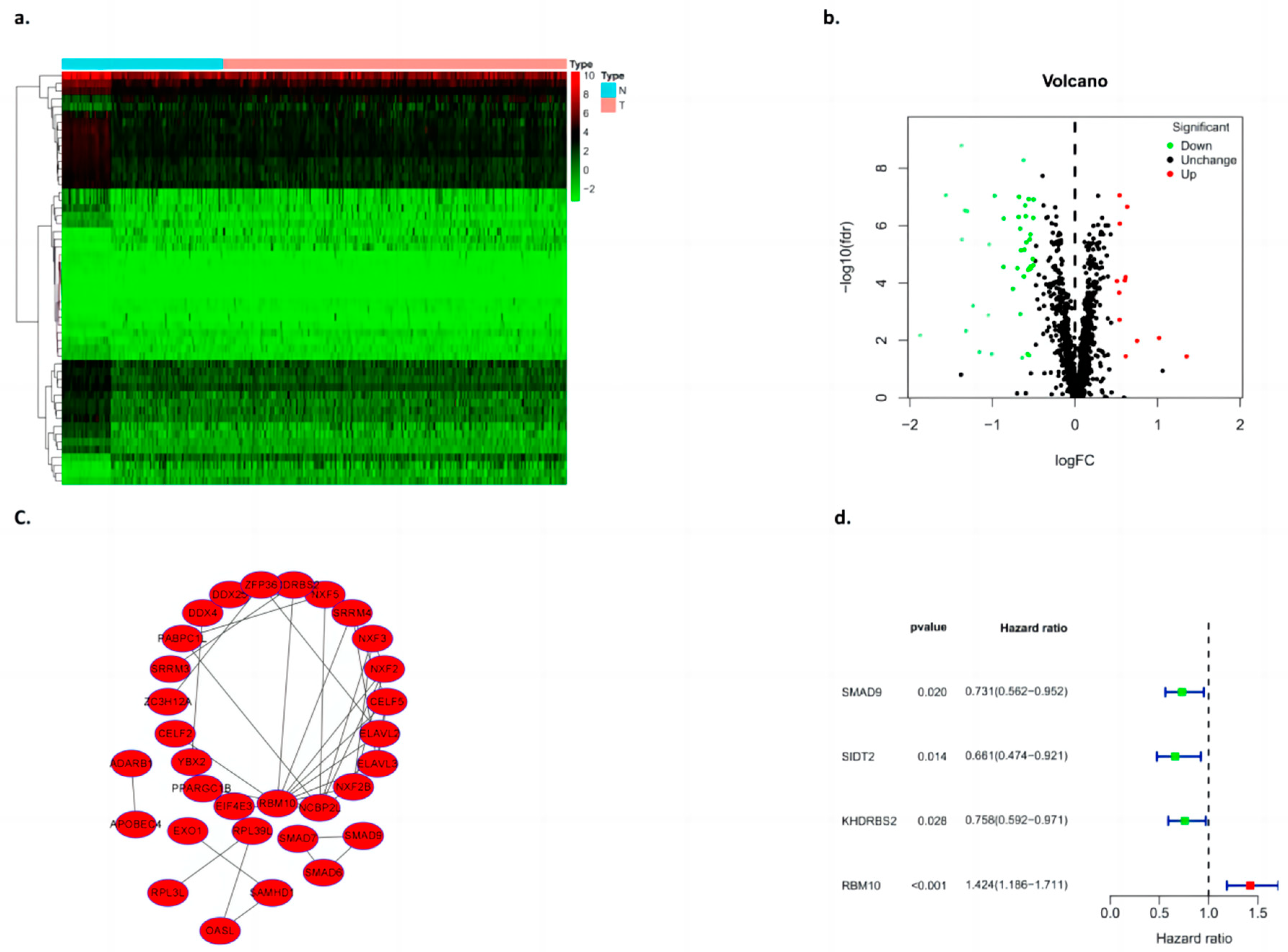
3.2. Identification of RNAs Associated with Genomic Instability in Patients with Lung Adenocarcinoma
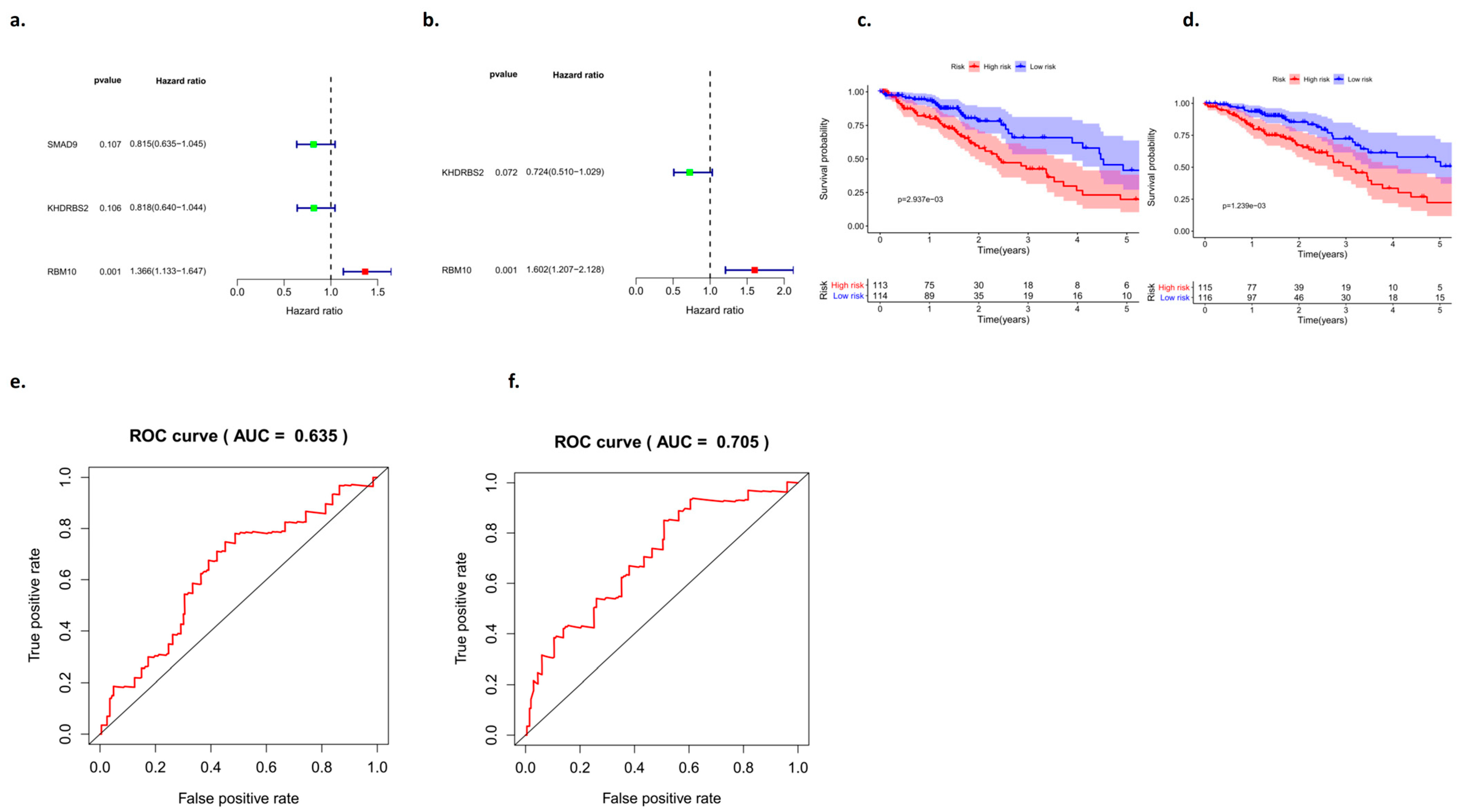
3.3. Validation of the Prognostic Model with an Internal Dataset
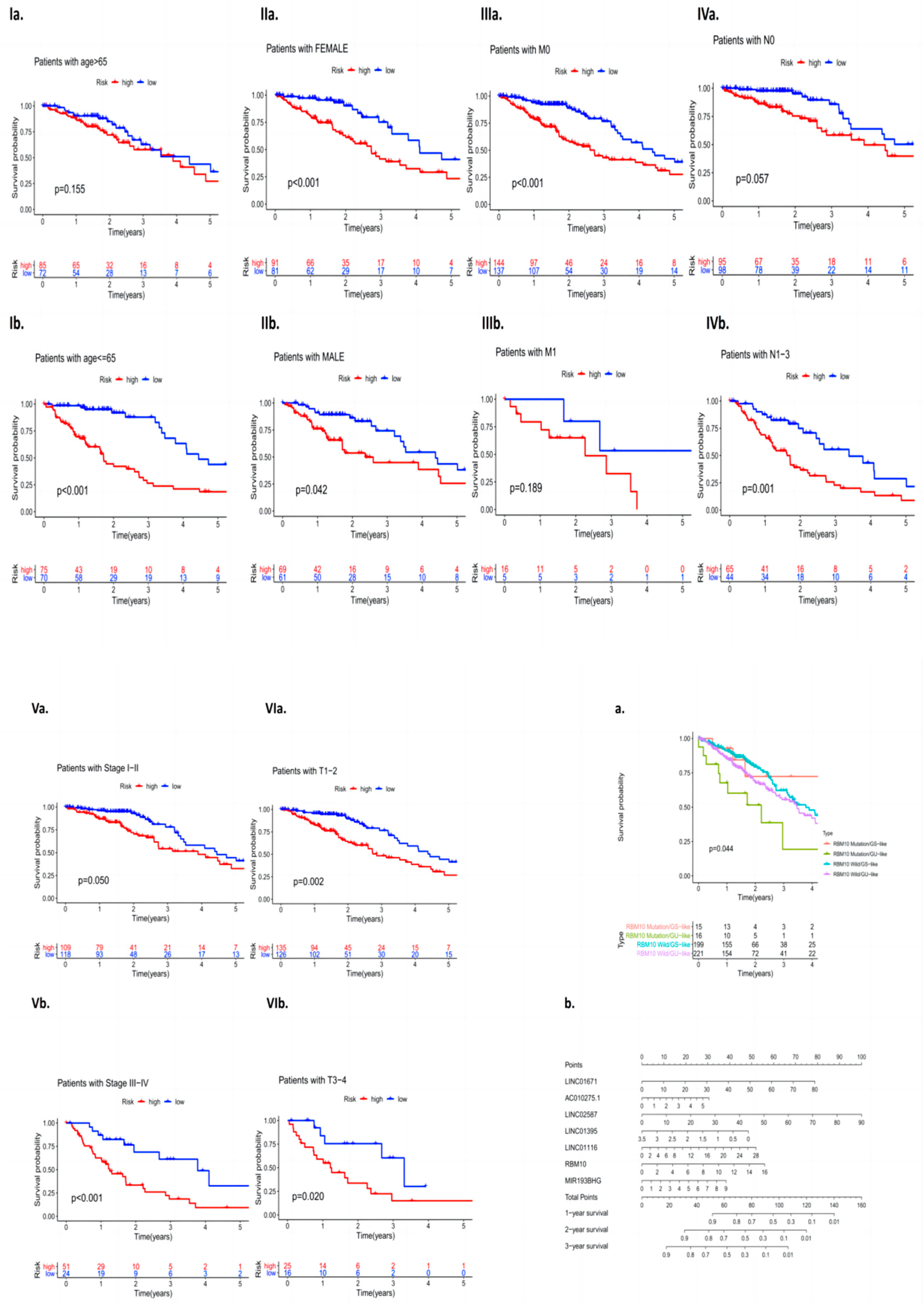
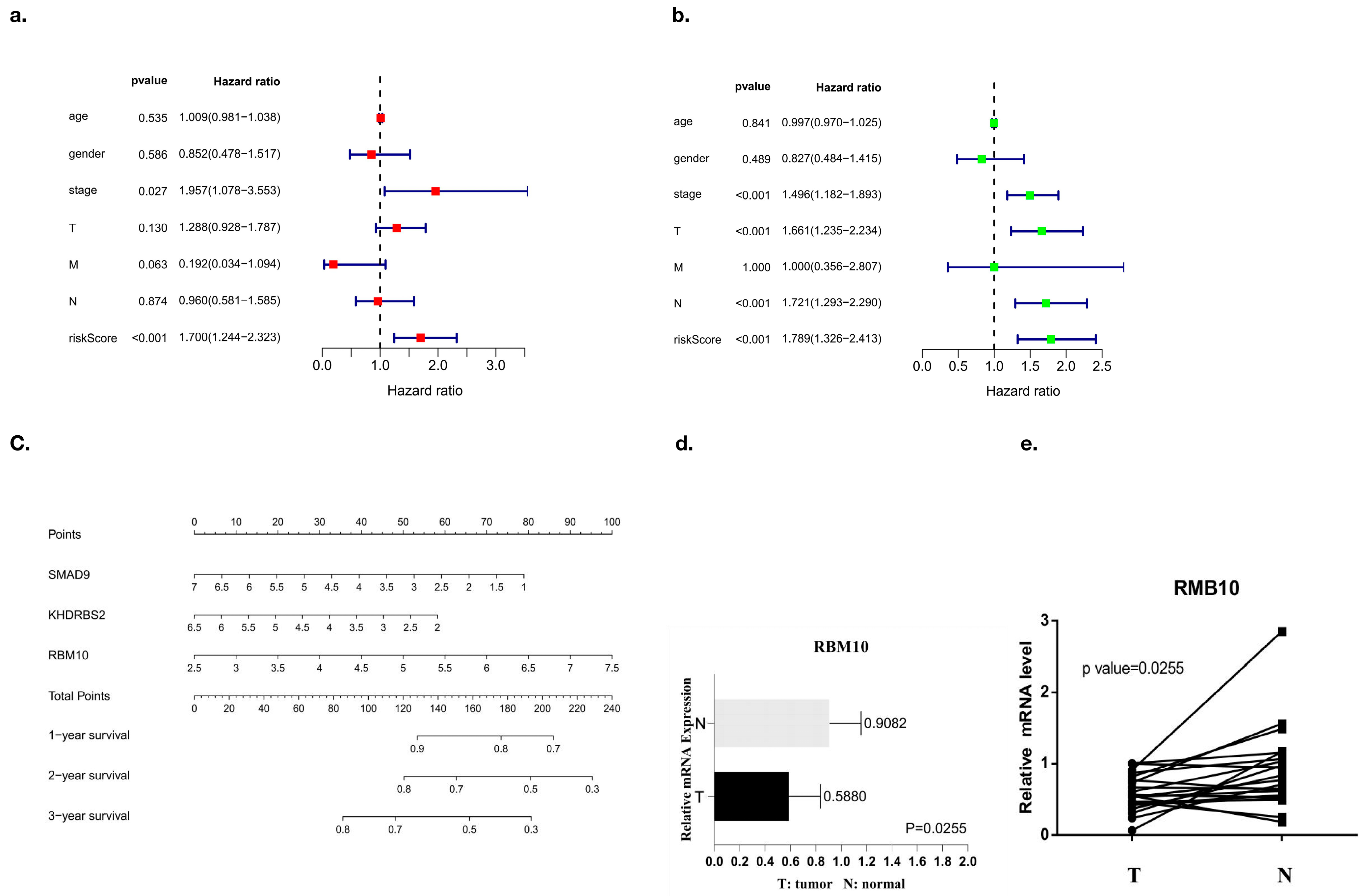
3.4. Analysis of RBM10 in Lung Adenocarcinoma Independent of Other Clinical Features
3.5. PPI Network Analysis of Differential Genes
3.6. Functional Enrichment Analysis of the Algorithm Model
3.7. Comparison of Survival Curves between the Test Group and the Control Group
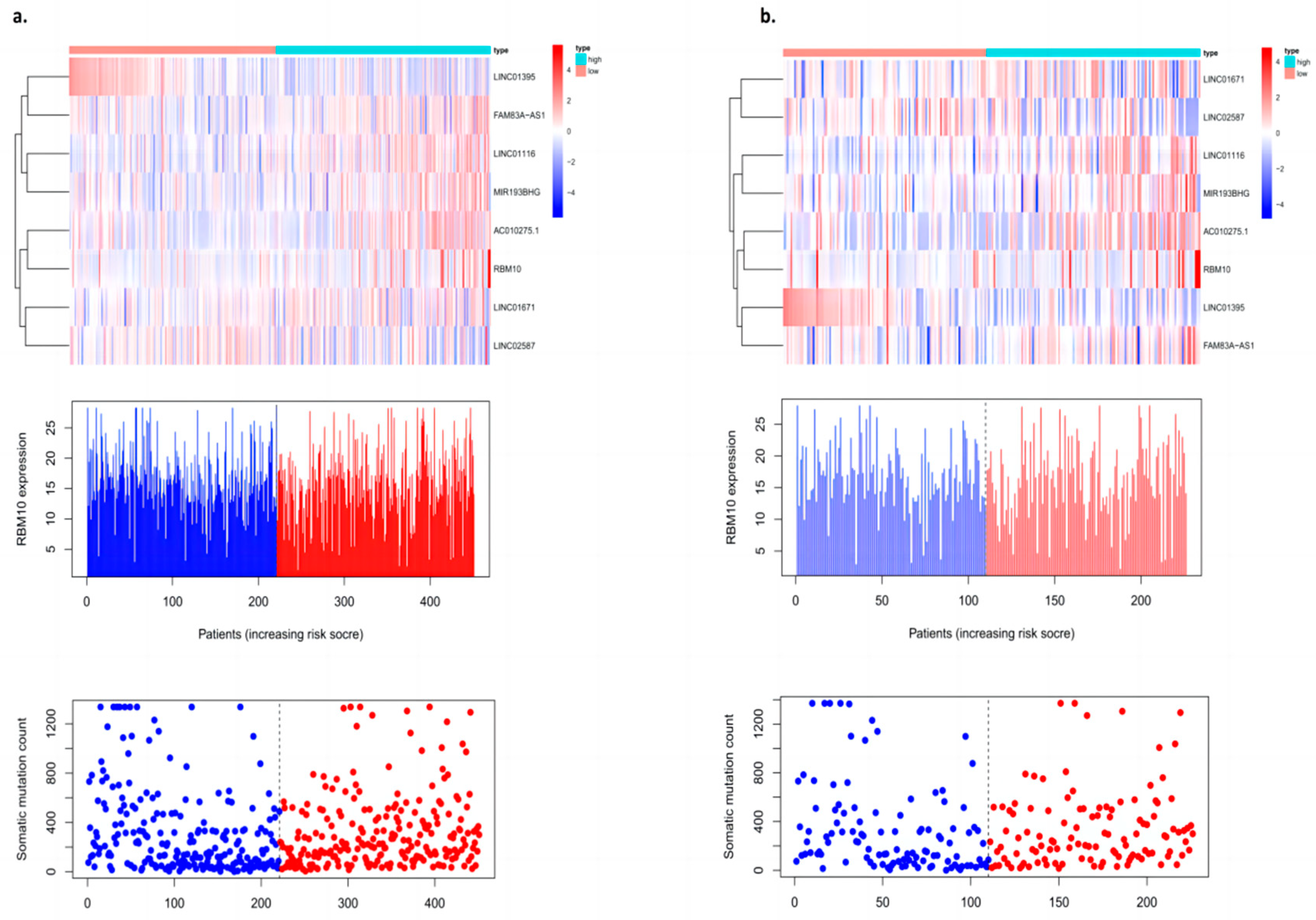
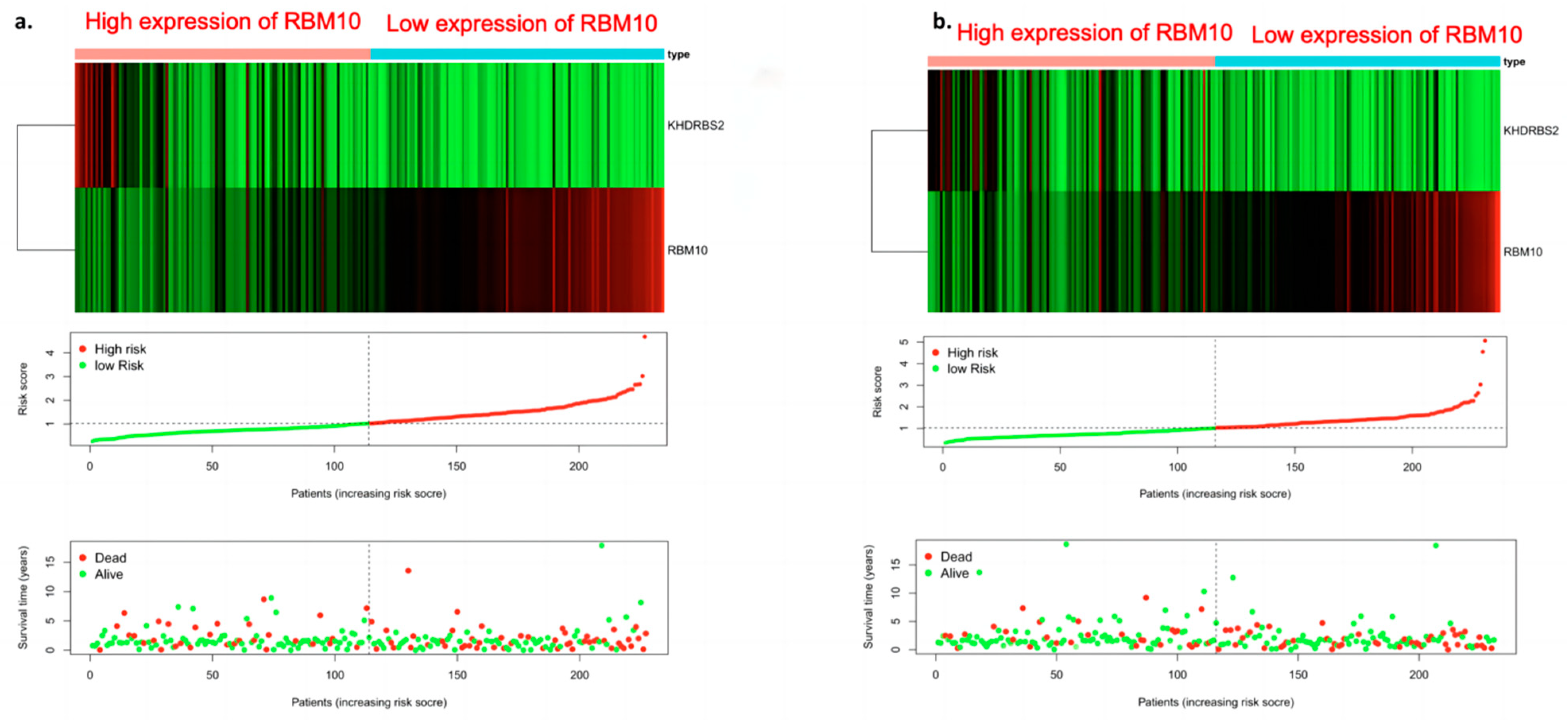
3.8. Risk Curve Analysis
3.9. Analysis of Clinically Independent Prognostic Factors and Nomogram Analysis
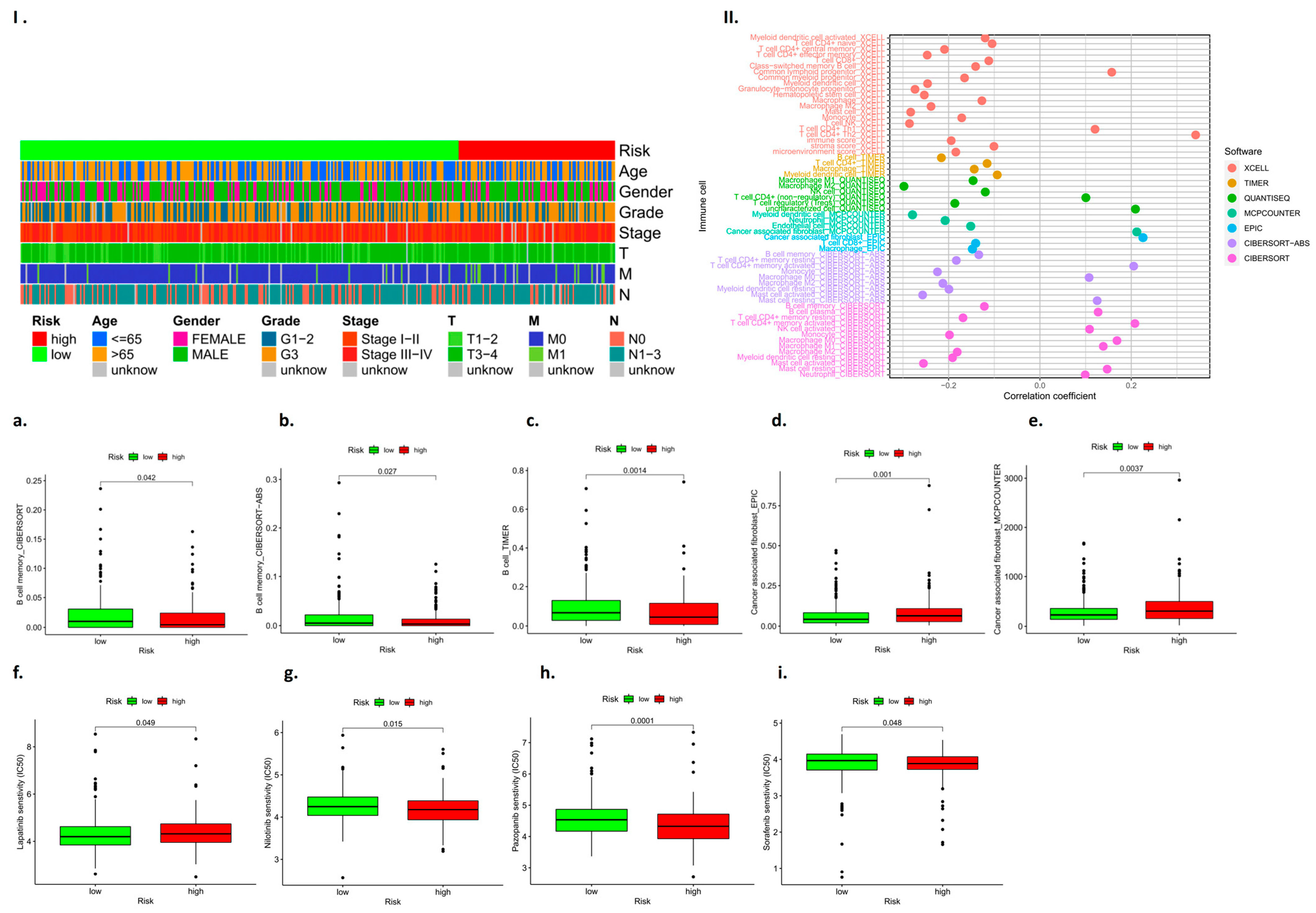
3.10. RBM10 Is Involved in the Immune Regulation of Lung Adenocarcinoma
3.11. Immune Cell Subcomponent Analysis and Drug Sensitivity Analysis
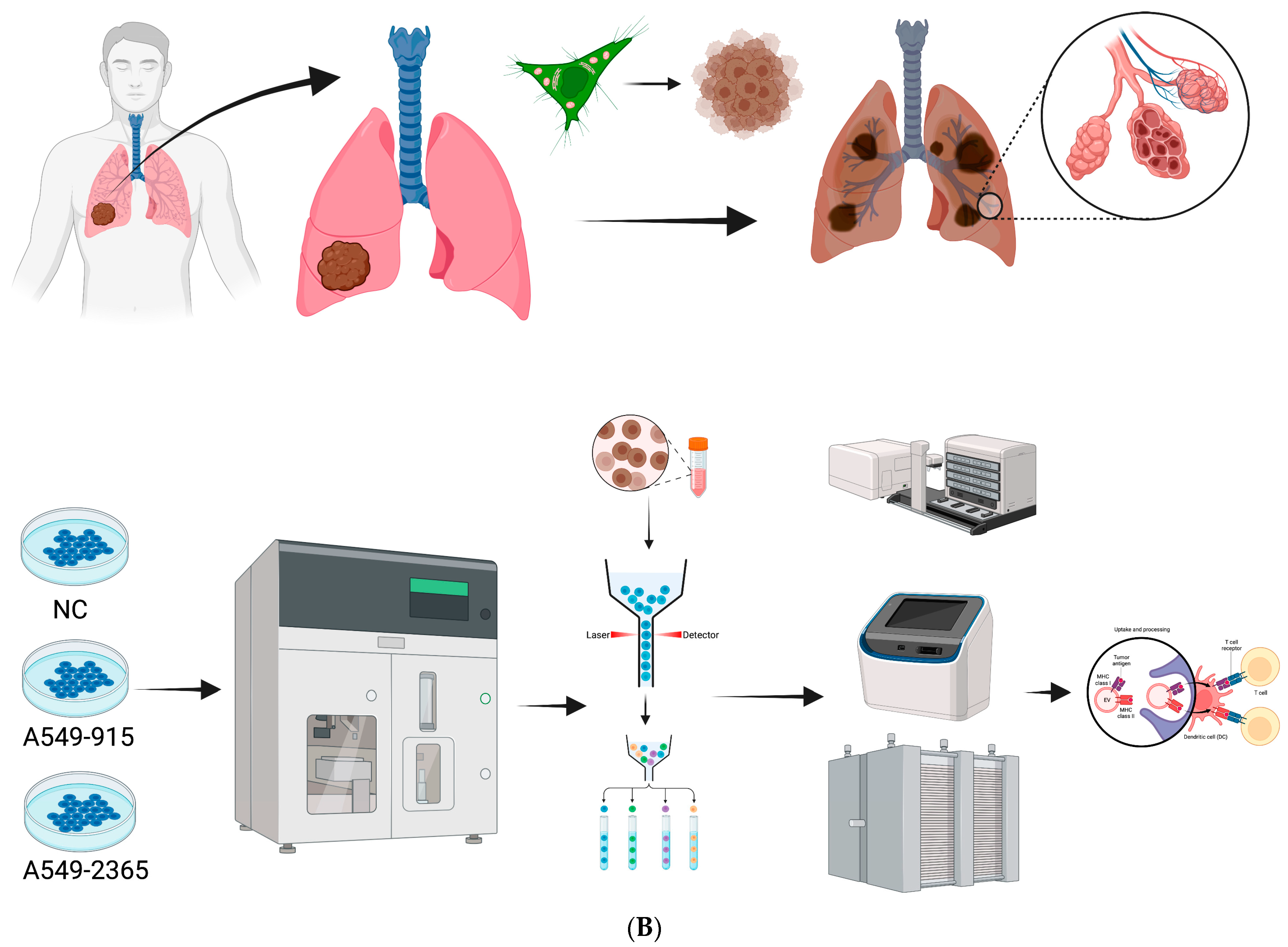
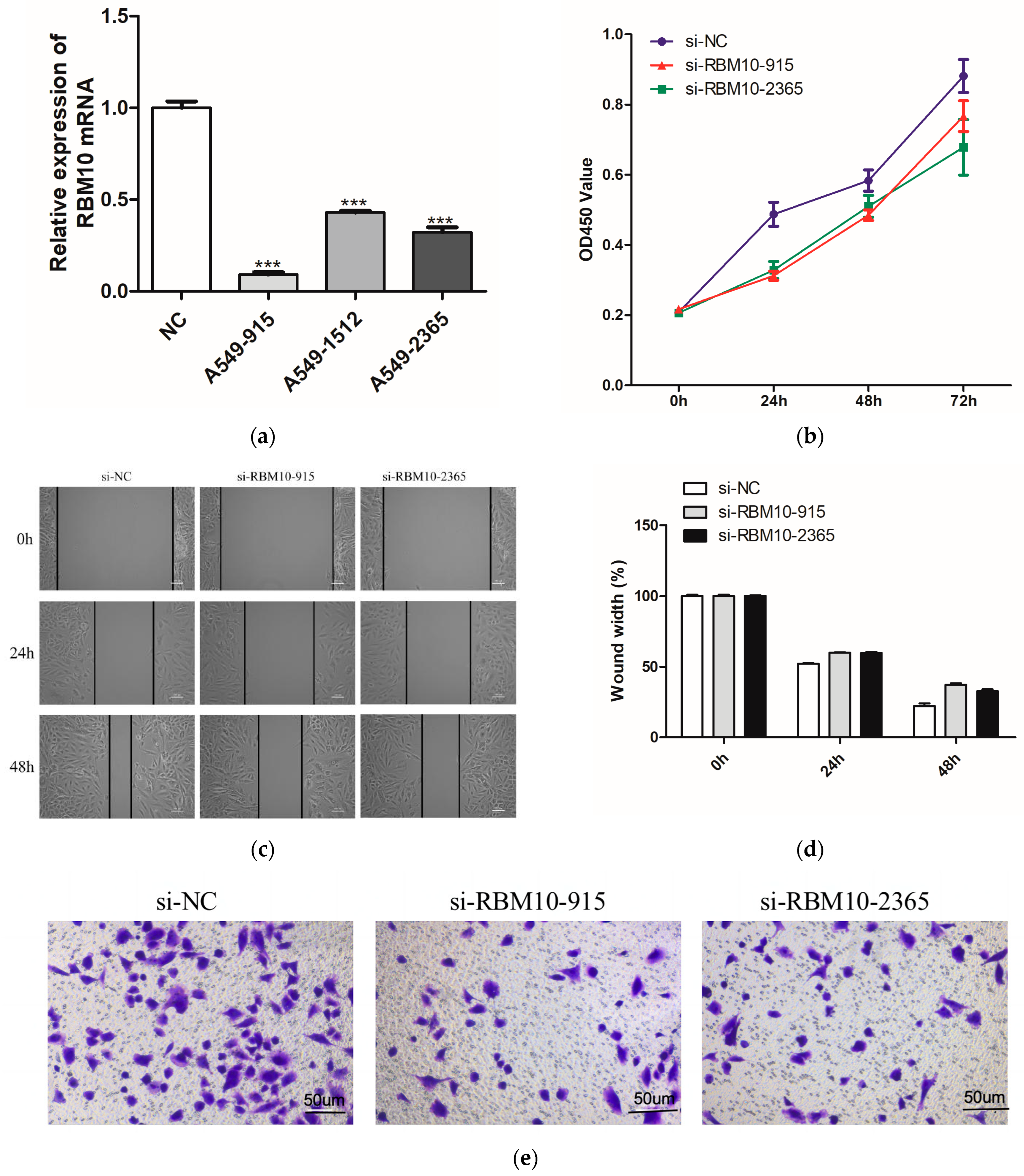
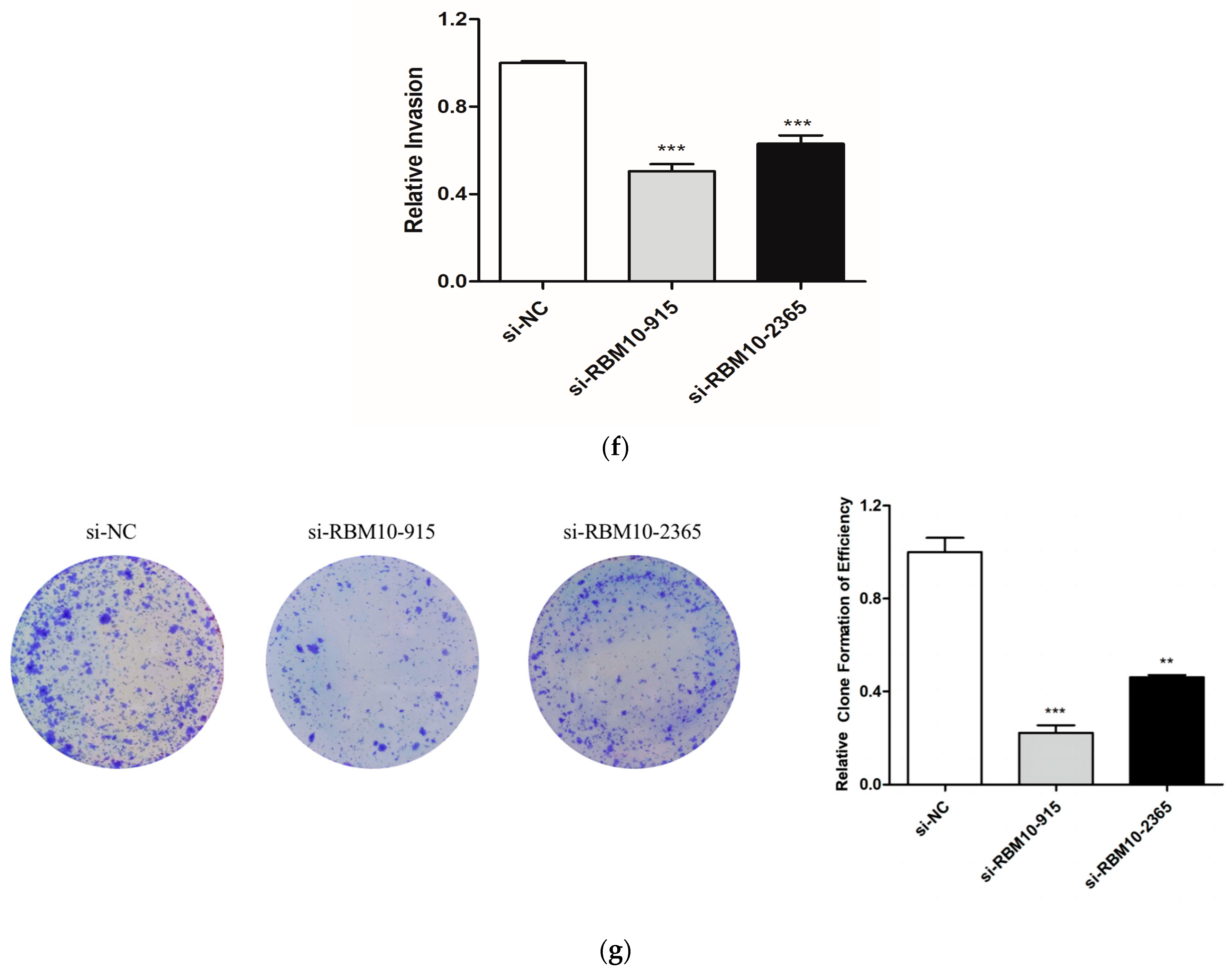
3.12. In Vitro Experimental Verification Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Z.; Xue, Q.; Xu, J.; Zhang, P.; Ding, B. The role of RBM10 mutations in the development, treatment, and prognosis of lung adenocarcinoma. Cell Cycle 2020, 19, 2918–2926. [Google Scholar] [CrossRef]
- Sun, X.; Jia, M.; Sun, W.; Feng, L.; Gu, C.; Wu, T. Functional role of RBM10 in lung adenocarcinoma proliferation. Int. J. Oncol. 2019, 54, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Wang, Y.; Wang, H.; Li, Z.; Yang, L.; Yan, S.; Yang, X.; Ma, Y.; Gao, X.; Guan, Y.; et al. RBM10 Deficiency Is Associated With Increased Immune Activity in Lung Adenocarcinoma. Front. Oncol. 2021, 11, 677826. [Google Scholar] [CrossRef]
- Jin, X.; Di, X.; Wang, R.; Ma, H.; Tian, C.; Zhao, M.; Cong, S.; Liu, J.; Li, R.; Wang, K. RBM10 inhibits cell proliferation of lung adenocarcinoma via RAP1/AKT/CREB signalling pathway. J. Cell. Mol. Med. 2019, 23, 3897–3904. [Google Scholar] [CrossRef]
- Wang, Q.; Li, M.; Yang, M.; Yang, Y.; Song, F.; Zhang, W.; Li, X.; Chen, K. Analysis of immune-related signatures of lung adenocarcinoma identified two distinct subtypes: Implications for immune checkpoint blockade therapy. Aging 2020, 12, 3312–3339. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.Z.; Zhao, T.W. Lung adenocarcinoma pathology stages related gene identification. Math. Biosci. Eng. 2019, 17, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Sun, Y.; Cao, H.; Liu, Z.; Xi, L.; Dong, C.; Yang, R.; Shi, Y. A novel pyroptosis-related lncRNA signature for prognostic prediction in patients with lung adenocarcinoma. Bioengineered 2021, 12, 5932–5949. [Google Scholar] [CrossRef]
- Jin, C.Y.; Du, L.; Nuerlan, A.H.; Wang, X.L.; Yang, Y.W.; Guo, R. High expression of RRM2 as an independent predictive factor of poor prognosis in patients with lung adenocarcinoma. Aging 2020, 13, 3518–3535. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Li, A.; Zhou, L.; Chu, Q.; Luo, S.; Wu, K. Immune signature-based risk stratification and prediction of immune checkpoint inhibitor’s efficacy for lung adenocarcinoma. Cancer Immunol. Immunother. 2021, 70, 1705–1719. [Google Scholar] [CrossRef]
- Zuo, S.; Wei, M.; Wang, S.; Dong, J.; Wei, J. Pan-Cancer Analysis of Immune Cell Infiltration Identifies a Prognostic Immune-Cell Characteristic Score (ICCS) in Lung Adenocarcinoma. Front. Immunol. 2020, 11, 1218. [Google Scholar] [CrossRef]
- Zengin, T.; Önal-Süzek, T. Analysis of genomic and transcriptomic variations as prognostic signature for lung adenocarcinoma. BMC Bioinform. 2020, 21 (Suppl. 14), 368. [Google Scholar] [CrossRef]
- Liu, J.; Han, X.; Chen, L.; Han, D.; Mu, X.; Hu, X.; Wu, H.; Wu, H.; Liu, W.; Zhao, Y. TRIM28 is a distinct prognostic biomarker that worsens the tumor immune microenvironment in lung adenocarcinoma. Aging 2020, 12, 20308–20331. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Rao, X.; Lin, W. Immune landscape and a promising immune prognostic model associated with TP53 in early-stage lung adenocarcinoma. Cancer Med. 2021, 10, 806–823. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Dong, Z.; Shen, Y.; Shi, J.; Wu, Y.; Zhao, Z.; Jiang, G.; Song, X. Cribriform growth pattern in lung adenocarcinoma: More aggressive and poorer prognosis than acinar growth pattern. Lung Cancer 2020, 147, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Nacer, D.F.; Liljedahl, H.; Karlsson, A.; Lindgren, D.; Staaf, J. Pan-cancer application of a lung-adenocarcinoma-derived gene-expression-based prognostic predictor. Brief. Bioinform. 2021, 22, bbab154. [Google Scholar] [CrossRef] [PubMed]
- Xia, Q.Y.; Wang, X.T.; Zhan, X.M.; Tan, X.; Chen, H.; Liu, Y.; Shi, S.S.; Wang, X.; Wei, X.; Ye, S.B.; et al. Xp11 Translocation Renal Cell Carcinomas (RCCs) With RBM10-TFE3 Gene Fusion Demonstrating Melanotic Features and Overlapping Morphology With t(6;11) RCC: Interest and Diagnostic Pitfall in Detecting a Paracentric Inversion of TFE3. Am. J. Surg. Pathol. 2017, 41, 663–676. [Google Scholar] [CrossRef]
- Liu, Y.; Liang, L.; Ji, L.; Zhang, F.; Chen, D.; Duan, S.; Shen, H.; Liang, Y.; Chen, Y. Potentiated lung adenocarcinoma (LUAD) cell growth, migration and invasion by lncRNA DARS-AS1 via miR-188-5p/ KLF12 axis. Aging 2021, 13, 23376–23392. [Google Scholar] [CrossRef]
- Li, W.; Gao, L.N.; Song, P.P.; You, C.G. Development and validation of a RNA binding protein-associated prognostic model for lung adenocarcinoma. Aging 2020, 12, 3558–3573. [Google Scholar] [CrossRef]
- Toraskar, S.; Madhukar Chaudhary, P.; Kikkeri, R. The Shape of Nanostructures Encodes Immunomodulation of Carbohydrate Antigen and Vaccine Development. ACS Chem. Biol. 2022, 17, 1122–1130. [Google Scholar] [CrossRef]
- Lavelle, E.C.; McLachlan, J.B. Editorial overview: Immunomodulation: Striking the right balance: Using immunomodulators to target infectious diseases, cancer, and autoimmunity. Curr. Opin. Pharmacol. 2018, 41, vii–ix. [Google Scholar] [CrossRef]
- Koliakos, N.N.; Renieris, G.; Sotiropoulos, D.; Pavlou, K.; Droggiti, D.E.; Gkavogianni, T.; Charalampopoulos, A.; Giamarellos-Bourboulis, E.J. Immunomodulation Through Beta-D-glucan in Chemically-induced Necrotizing Pancreatitis. J. Surg. Res. 2021, 261, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Lamb, J.; Crawford, E.D.; Peck, D.; Modell, J.W.; Blat, I.C.; Wrobel, M.J.; Lerner, J.; Brunet, J.P.; Subramanian, A.; Ross, K.N.; et al. The Connectivity Map: Using gene-expression signatures to connect small molecules, genes, and disease. Science 2006, 313, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Chiao, C.C.; Phan, N.N.; Li, C.Y.; Sun, Z.D.; Jiang, J.Z.; Hung, J.H.; Chen, Y.L.; Yen, M.C.; Weng, T.Y. Gene signatures and potential therapeutic targets of amino acid metabolism in estrogen receptor-positive breast cancer. Am. J. Cancer Res. 2020, 10, 95–113. [Google Scholar] [PubMed]
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Proteomics. Tissue-based map of the human proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef] [PubMed]
- Kao, T.J.; Wu, C.C.; Phan, N.N.; Liu, Y.H.; Ta, H.D.K.; Anuraga, G.; Wu, Y.F.; Lee, K.H.; Chuang, J.Y.; Wang, C.Y. Prognoses and genomic analyses of proteasome 26S subunit, ATPase (PSMC) family genes in clinical breast cancer. Aging 2021, 13, 17970. [Google Scholar] [CrossRef]
- Modhukur, V.; Iljasenko, T.; Metsalu, T.; Liu, Y.H.; Ta, H.D.K.; Anuraga, G.; Wu, Y.F.; Lee, K.H.; Chuang, J.Y.; Wang, C.Y. MethSurv: A web tool to perform multivariable survival analysis using DNA methylation data. Epigenomics 2018, 10, 277–288. [Google Scholar] [CrossRef]
- Xing, C.; Wang, Z.; Zhu, Y.; Zhang, C.; Liu, M.; Hu, X.; Chen, W.; Du, Y. Integrate analysis of the promote function of Cell division cycle associated protein family to pancreatic adenocarcinoma. Int. J. Med. Sci. 2021, 18, 672–684. [Google Scholar] [CrossRef]
- Grippin, A.J.; Dyson, K.A.; Qdaisat, S.; McGuiness, J.; Wummer, B.; Mitchell, D.A.; Mendez-Gomez, H.R.; Sayour, E.J. Nanoparticles as immunomodulators and translational agents in brain tumors. J. Neurooncol. 2021, 151, 29–39. [Google Scholar] [CrossRef]
- Green, T.C.; Park, J.N.; Gilbert, M.; McKenzie, M.; Struth, E.; Lucas, R.; Clarke, W.; Sherman, S.G. An assessment of the limits of detection, sensitivity and specificity of three devices for public health-based drug checking of fentanyl in street-acquired samples. Int. J. Drug Policy 2020, 77, 102661. [Google Scholar] [CrossRef]
- Cabañas, R.; Calderón, O.; Ramírez, E.; Fiandor, A.; Caballero, T.; Heredia, R.; Herranz, P.; Madero, R.; Quirce, S.; Bellón, T. Sensitivity and specificity of the lymphocyte transformation test in drug reaction with eosinophilia and systemic symptoms causality assessment. Clin. Exp. Allergy 2018, 48, 325–333. [Google Scholar] [CrossRef]
- Romman, A.; Doulatram, G.; Doctor, N.; Krishnamurthy, P. Sensitivity and specificity of SOAPP-SF questionnaire for predicting aberrant urine drug screen. Reg. Anesth. Pain Med. 2020, 45, 763–764. [Google Scholar] [CrossRef]
- Cao, Y.; Di, X.; Zhang, Q.; Li, R.; Wang, K. RBM10 Regulates Tumor Apoptosis, Proliferation, and Metastasis. Front. Oncol. 2021, 11, 603932. [Google Scholar] [CrossRef] [PubMed]
- Weigt, M.; Gao, Q.; Ban, H.; He, H.; Mastrobuoni, G.; Kempa, S.; Chen, W.; Li, F. RBM10 facilitates heterochromatin assembly via the Clr6 HDAC complex. Epigenet. Chromatin. 2021, 14, 8. [Google Scholar] [CrossRef]
- Kato, I.; Furuya, M.; Baba, M.; Kameda, Y.; Yasuda, M.; Nishimoto, K.; Oyama, M.; Yamasaki, T.; Ogawa, O.; Niino, H.; et al. RBM10-TFE3 renal cell carcinoma characterised by paracentric inversion with consistent closely split signals in break-apart fluorescence in-situ hybridisation: Study of 10 cases and a literature review. Histopathology 2019, 75, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, B.; Bragado, L.; Mammi, P.; Torti, M.F.; Gaioli, N.; Gebhard, L.G.; García Solá, M.E.; Vaz-Drago, R.; Iglesias, N.G.; García, C.C. Dengue virus targets RBM10 deregulating host cell splicing and innate immune response. Nucleic Acids Res. 2020, 48, 6824–6838. [Google Scholar] [CrossRef] [PubMed]
- Kunimoto, H.; Inoue, A.; Kojima, H.; Yang, J.; Zhao, H.; Tsuruta, D.; Nakajima, K. RBM10 regulates centriole duplication in HepG2 cells by ectopically assembling PLK4-STIL complexes in the nucleus. Genes Cells 2020, 25, 100–110. [Google Scholar] [CrossRef]
- Wang, L.Y.; Xiao, S.J.; Kunimoto, H.; Tokunaga, K.; Kojima, H.; Kimura, M.; Yamamoto, T.; Yamamoto, N.; Zhao, H.; Nishio, K. Sequestration of RBM10 in Nuclear Bodies: Targeting Sequences and Biological Significance. Int. J. Mol. Sci. 2021, 22, 10526. [Google Scholar] [CrossRef]
- Xiao, W.; Chen, X.; Li, X.; Deng, K.; Liu, H.; Ma, J.; Wang, Z.; Hu, Y.; Hou, J. RBM10 regulates human TERT gene splicing and inhibits pancreatic cancer progression. Am. J. Cancer Res. 2021, 11, 157–170. [Google Scholar] [PubMed]
- Di Mauro, I.; Dadone-Montaudie, B.; Sibony, M.; Ambrosetti, D.; Molinie, V.; Decaussin-Petrucci, M.; Bland, V.; Arbaud, C.; Cenciu, B.; Arbib, F. RBM10-TFE3 fusions: A FISH-concealed anomaly in adult renal cell carcinomas displaying a variety of morphological and genomic features: Comprehensive study of six novel cases. Genes Chromosomes Cancer 2021, 60, 772–784. [Google Scholar] [CrossRef]
- Zhao, Z.; Li, J.; Shen, F. Protective effect of the RNA-binding protein RBM10 in hepatocellular carcinoma. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 6005–6013. [Google Scholar]
- Dou, X.Q.; Chen, X.J.; Wen, M.X.; Zhang, S.Z.; Zhou, Q.; Zhang, S.Q. Alternative splicing of VEGFA is regulated by RBM10 in endometrial cancer. Kaohsiung J. Med. Sci. 2020, 36, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Nanjo, S.; Wu, W.; Karachaliou, N.; Blakely, C.M.; Suzuki, J.; Chou, Y.T.; Ali, S.M.; Kerr, D.L.; Olivas, V.R.; Shue, J.; et al. Deficiency of the splicing factor RBM10 limits EGFR inhibitor response in EGFR-mutant lung cancer. J. Clin. Investig. 2022, 132, e145099. [Google Scholar] [CrossRef] [PubMed]
- Dou, X.Q.; Chen, X.J.; Zhou, Q.; Wen, M.X.; Zhang, S.Z.; Zhang, S.Q. miR-335 modulates Numb alternative splicing via targeting RBM10 in endometrial cancer. Kaohsiung J. Med. Sci. 2020, 36, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Kumps, C.; D’haenens, E.; Vergult, S.; Leus, J.; Van Coster, R.; Jansen, A.; Devriendt, K.; Oostra, A.; Vanakker, O.M. Phenotypic spectrum of the RBM10-mediated intellectual disability and congenital malformation syndrome beyond classic TARP syndrome features. Clin. Genet. 2021, 99, 449–456. [Google Scholar] [CrossRef]
- Mohan, N.; Kumar, V.; Kandala, D.T.; Kartha, C.C.; Laishram, R.S. A Splicing-Independent Function of RBM10 Controls Specific 3’ UTR Processing to Regulate Cardiac Hypertrophy. Cell Rep. 2018, 24, 3539–3553. [Google Scholar] [CrossRef]














Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Liu, Q.; Ruan, X.; Luan, X.; Zhong, Y.; Liu, J.; Yan, J.; Li, X. Multiple Omics Analysis of the Role of RBM10 Gene Instability in Immune Regulation and Drug Sensitivity in Patients with Lung Adenocarcinoma (LUAD). Biomedicines 2023, 11, 1861. https://doi.org/10.3390/biomedicines11071861
Wu L, Liu Q, Ruan X, Luan X, Zhong Y, Liu J, Yan J, Li X. Multiple Omics Analysis of the Role of RBM10 Gene Instability in Immune Regulation and Drug Sensitivity in Patients with Lung Adenocarcinoma (LUAD). Biomedicines. 2023; 11(7):1861. https://doi.org/10.3390/biomedicines11071861
Chicago/Turabian StyleWu, Liusheng, Qi Liu, Xin Ruan, Xinyu Luan, Yanfeng Zhong, Jixian Liu, Jun Yan, and Xiaoqiang Li. 2023. "Multiple Omics Analysis of the Role of RBM10 Gene Instability in Immune Regulation and Drug Sensitivity in Patients with Lung Adenocarcinoma (LUAD)" Biomedicines 11, no. 7: 1861. https://doi.org/10.3390/biomedicines11071861
APA StyleWu, L., Liu, Q., Ruan, X., Luan, X., Zhong, Y., Liu, J., Yan, J., & Li, X. (2023). Multiple Omics Analysis of the Role of RBM10 Gene Instability in Immune Regulation and Drug Sensitivity in Patients with Lung Adenocarcinoma (LUAD). Biomedicines, 11(7), 1861. https://doi.org/10.3390/biomedicines11071861