1. Introduction
Osteoarthritis (OA) affects the entire synovial joint, including the synovium, cartilage, and subchondral bone. The reaction mechanism of the chondrocyte in OA is represented as (1) proliferation and cell death, (2) changes in synthetic activity and degradation, and (3) formation of osteophytes [
1]. The degradation of the cartilage matrix is observed initially in the cartilage superficial zone; however, it extended to deeper as OA advanced. Later, the subchondral bone is also marked as changed, including the increment of cortical plate thickness, change in bone mass of subchondral trabecular bone mass, and alteration of bone turnover [
2]. Knee joint OA is also caused by the failed repair of joint damage from stresses. The symptoms of knee OA are represented as pain, decreased joint motion, stiffness, and reduced physical activity. Factors that known to associated with increased risk of knee OA include female sex, older age, obesity, previous knee injury, and varus or valgus malalignment of the knee joint [
3].
High tibial osteotomy (HTO) is a surgical method performed in medial compartment osteoarthritis within the varus knee in relatively young patients [
4]. In medial compartment osteoarthritis, the mechanical axis is usually medially deviated due to varus deformity, which leads to degenerative changes in the cartilage. HTO is a good surgical option for patients whose mechanical axis is medially deviated, and several studies have shown excellent clinical outcomes after HTO [
5,
6]. Initially, closed-wedge HTO was widely performed. With the advent of the T-shape locking plate, open-wedge HTO, which provides the advantages including easier surgical techniques and less risk of neurovascular injury, gained popularity among orthopedic surgeons [
7].
Numerous anatomical changes could be found following open-wedge HTO. For example, the medial compartment cartilage could be regenerated, the cartilage status of patellofemoral joint or lateral compartment might be degraded, and the alignment of the ankle joint might change [
8,
9,
10]. Among these changes, there is a change in the alignment of the lower extremities from varus to valgus, which leads to a reduction in medial compartment stress. Based on this theoretical basis, remodeling of the medial compartmental articular cartilage could occur after HTO [
11,
12]. Previous studies reported that 55–92% of patients showed cartilage regeneration in the medial femoral condyle (MFC) or medial tibial plateau (MTP) following HTO [
13]. Given the wide range of reported rates of cartilage regeneration in the existing literature, it is crucial to obtain a second-look arthroscopic assessment of cartilage regeneration following open-wedge HTO without additional cartilage regeneration procedures. Moreover, a few studies were focused on the clinical effects of cartilage regeneration after HTO.
The purpose of the present study was (1) to investigate the rate of cartilage regeneration after open-wedge HTO without cartilage regeneration by second-look arthroscopy and (2) to identify the correlation between cartilage regeneration and patients’ reported outcomes. It was hypothesized that approximately one-third of patients would show improvements in cartilage statuses in the medial compartment.
3. Results
A total of 65 patients was enrolled in the current study. The demographic data are shown in
Table 1. The mean period from prior surgery to second-look examination was 26.5 ± 9.1 months.
All inter- and intra-observer ICCs showed good agreement with respect to the reliability of radiographic measurements (>0.80). The preoperative HKA angle (6.4° ± 2.7°) was well corrected postoperatively (−2.7° ± 2.7°,
p < 0.001). The tibial slope was well maintained (preoperative vs. postoperative, 80.6° ± 3.5° vs. 80.4° ± 3.0°,
p = 0.58). Clinical outcomes, including WOMAC index and IKDC subjective score, were significantly improved postoperatively (
Table 2).
The cartilage status of the MFC and MTP according to the ICRS grade is presented in
Table 3. In terms of MFC on second-look arthroscopy, 29 patients (44.6%) showed an improved ICRS grade, 31 patients (47.7%) were maintained, and 5 patients (7.7%) showed a worse ICRS grade since the prior operation. With respect to MTP, 19 patients (29.2%) were improved, 44 patients (67.7%) were maintained, and 2 patients (3.1%) were worse in second-look arthroscopy. The detailed pre- and postoperative ICRS grades of patients who showed improvements are represented in
Table 4. In terms of comparing the ICRS grading change between genders, there was no statistical difference (
Table 5).
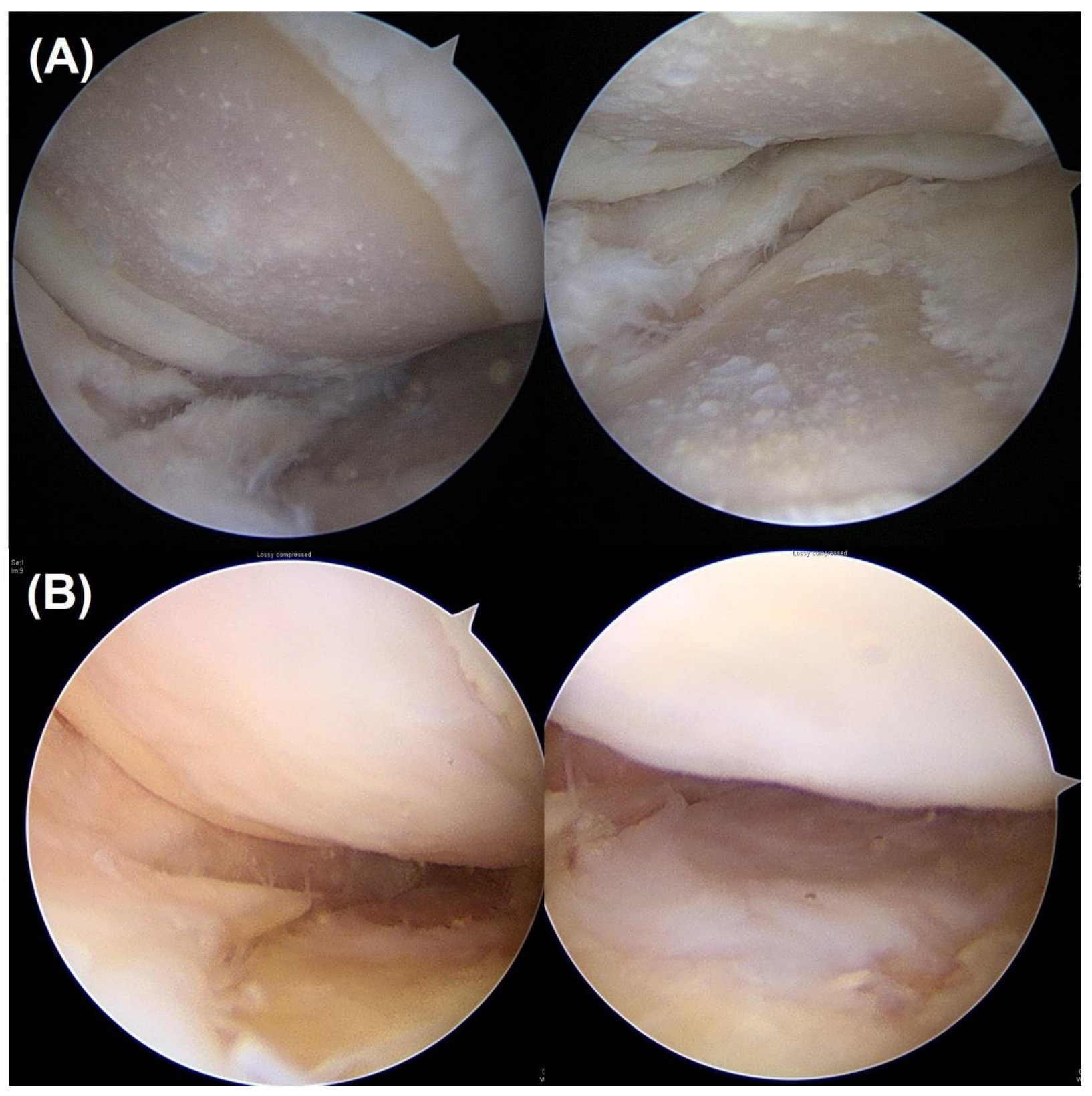
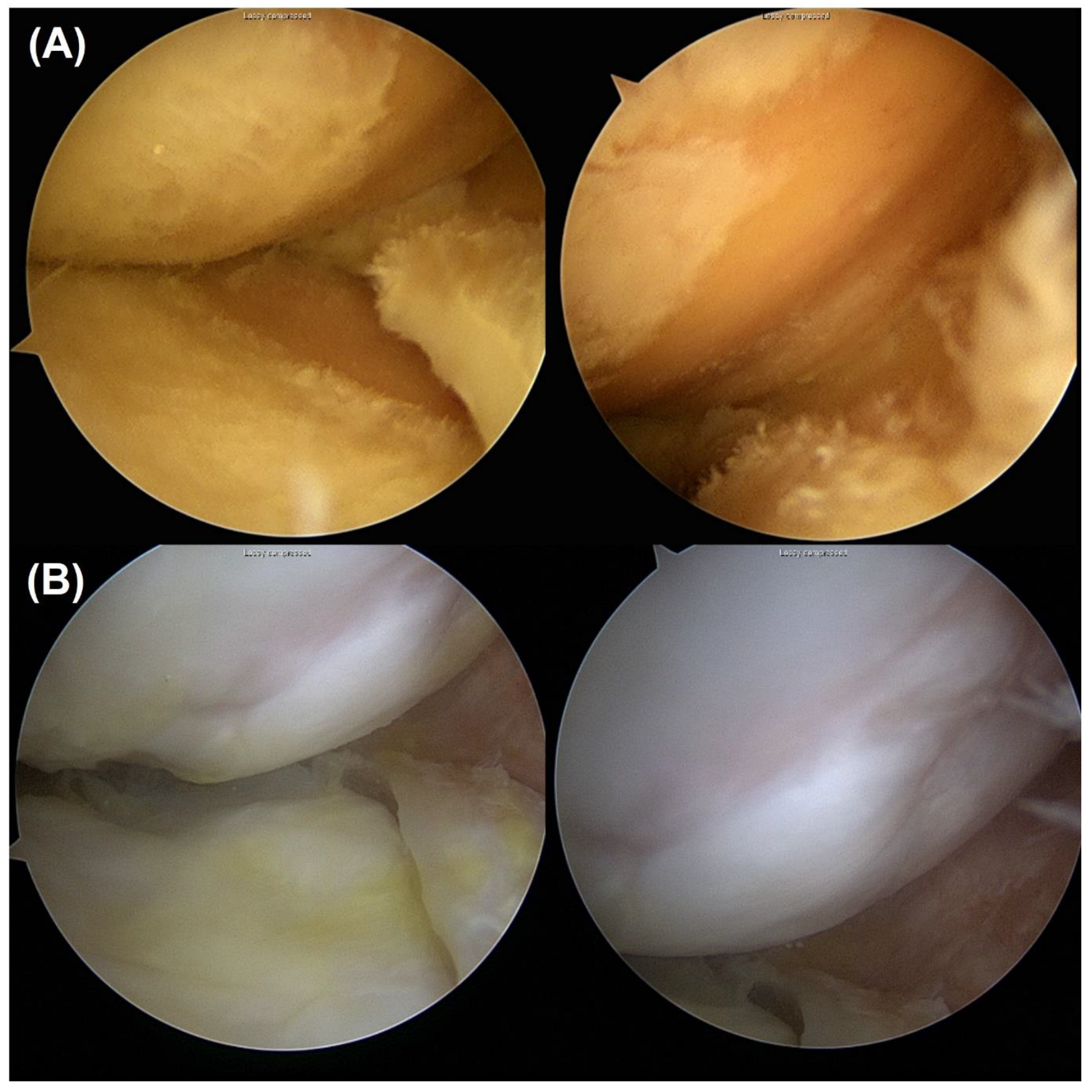
Among the patients who showed improved MFC cartilage status compared to prior surgery, 21 patients showed partial improvement, 5 patients showed full improvement, and 3 patients showed over-coverage. In terms of MTP, 16, 1, and 2 patients showed partial, full, and over improvement, respectively (
Table 6,
Figure 1 and
Figure 2).
In terms of comparing the clinical outcomes between the regeneration and non-regeneration groups on the MFC, pre- and post-operative WOMAC indexes and IKDC subjective scores were not statistically different (
Table 7). These were also not statistically different between the regeneration and non-regeneration groups on the MTP (
Table 8).
In respect of the predictive factor for the regeneration of the MFC, the lesser postoperative HKA angle (more valgus) was the only associated factor (OR 0.5, 95% CI 0.3–0.8,
p = 0.01,
Table 9). On the other hand, no factor was statistically associated with MTP cartilage regeneration on logistic regression analysis (
Table 10).
4. Discussion
The principal finding of our study was that 44.6% and 29.2% of patients showed improved cartilage statuses on the MFC and MTP after open-wedge HTO without any cartilage regeneration procedures. However, cartilage regeneration did not influence clinical outcomes.
The physiological tibiofemoral joint load distribution was not consistent. The load of the medial compartment was more than 60% of the joint load because of the varus alignment [
25]. Therefore, the medial compartment was commonly degraded in the early stage of osteoarthritis. As the osteoarthritis in the medial compartment progressed, the degradation of cartilage in the medial compartment increased, and the severity of the varus malalignment intensified, establishing a self-perpetuating cycle. HTO is an effective surgical option for medial compartmental osteoarthritis. The main principle of HTO is to correct varus lower extremity alignment; the pressure should be transferred from the medial compartment to lateral compartment, which is relatively healthy. Two different HTO techniques are commonly used and performed: a lateral closed-wedge HTO and a medial open-wedge HTO [
7]. Traditionally, the open-wedge HTO has gradually taken the place of the closed-wedge HTO, although closed-wedge HTOs were more commonly performed in the past. The advantages of an open-wedge HTO over a closed-wedge HTO include easier control of the degree of correction, less extensive soft tissue dissection, sparing of the proximal tibiofibular joint or the non-necessity of the fibular osteotomy, and the avoidance of serious complications such as peroneal nerve palsy [
26]. Numerous studies have concentrated on comparing the two different surgical techniques in terms of tibial slope change, patellar height, survival rate, and complications [
7,
25,
27,
28]. The complication rate and survival rate were not different, but open-wedge HTO was associated with increased tibial slope, leg length, and joint line elevation [
19,
29]. Open-wedge HTO has been reported to be beneficial in patients with medial compartmental degeneration, contributing from chronic posterior cruciate ligament insufficiency because it increases the posterior tibial slope as a result of the unique anatomic configuration of the proximal tibia [
30]. However, theoretically, an increased tibial slope is an associated adverse effect on anterior cruciate ligament [
31]. We think that postoperative changes in slope may have an impact on cartilage regeneration by influencing the integrity and function of the cruciate ligaments. Therefore, it is important to preserve the postoperative slope for outcomes. In the current study, statistical significance was not observed in the tibial slope, pre- and post-surgery. Hence, it can be inferred that the alteration in slope had minimal impact on cartilage regeneration in our study. A comparative investigation evaluating the extent of cartilage regeneration between closed-wedge HTO and open-wedge HTO is deemed a valuable avenue for future research.
Knee osteoarthritis is a common chronic joint disease and a major cause of pain and functional limitations. Multifactorial factors are associated with knee joint cartilage degeneration [
32]. Increased joint load and loss of shock absorption could contribute for the progression of knee joint arthritis [
33]. HTO could correct the abnormal biomechanical forces, thereby allowing the medial compartment of the knee joint to be offloaded [
6]. Interestingly, it was shown that cartilage could be regenerated by reducing the medial compartmental load alone without cartilage regeneration, including cartilage debridement, drilling, or microfractures [
11,
33,
34,
35]. Some studies have investigated regeneration after HTO using second-look arthroscopy, but the results varied. Kanamiya et al. [
11] investigated cartilage regeneration in the medial compartment after closed-wedge HTO. A total of 58 patients was enrolled in their study, and the mean period from initial osteotomy surgery to second-look arthroscopy was 18 months. In their study, approximately 55% of knees showed partial or even coverage with cartilage, 34% showed white scattering of fibrocartilage, and 11% showed no repair. Wakabayashi et al. [
35] evaluated 37 cases of eburnation cartilage lesions and 36 cases of fibrillation cartilage lesions on initial arthroscopy. All patients underwent closed-wedge HTO, and second-look arthroscopy was postoperatively performed after 1 year. Among the patients who had grade 4 lesions, 62% and 63% showed improved cartilage statuses on MFC and MTP, respectively. In contrast, in patients who had grade 3 lesions, 9% showed improved cartilage statuses on both MFC and MTP. They concluded that fibrillated cartilage had little potential for cartilage repair after closed-wedge HTO without cartilage procedures. Koshino et al. [
36] also performed closed-wedge HTO and second-look arthroscopy 2 years later. A total of 146 knees was enrolled; 32% showed full coverage with regenerated cartilage, and 68% showed no or partial regeneration. Jung et al. [
34] performed a second-look examination after open-wedge HTO. A total of 159 patients was enrolled in their study, and second-look arthroscopy was performed 2 years after surgery. More than grade 2 regeneration (white scattering, partial coverage, or even coverage) was achieved on the MFC in 92% of knees and on the MTP in 69% of knees. Kim et al. [
33] also evaluated patients who underwent open-wedge HTO and second-look arthroscopy after 25 months. Among 104 knees, 52% and 35% showed improved cartilage on MFC and MTP, respectively. Otsuki et al. [
37] demonstrated that 58% (82 of 142 patients) showed more than partial regeneration of the medial compartmental cartilage on second-look arthroscopy after open-wedge HTO, although the ratio of cartilage regeneration varied among previous studies because the method of evaluating cartilage differed from author to author. However, it seems clear that cartilage was regenerated at a certain rate after HTO without cartilage regeneration procedures.
The main goal of a HTO is to improve patient function and relieve pain [
8]. Undoubtedly, HTO has been revealed to enhance postoperative outcomes in patients with medial compartment osteoarthritis with varus deformity [
38]. Numerous investigations aiming to identify the factors that contribute to favorable patient-reported outcomes following HTO have been actively pursued [
6,
39,
40,
41]. The correlation between postoperative lower extremity alignment and postoperative outcome has been steadily reported. Kettelkamp et al. [
42] reported favorable results in cases with a femorotibial angle (FTA) of 157°. As open-wedge HTO has been widely performed, and whole-leg standing radiographs have been used for analysis, a postoperative HKA angle of 2–7° valgus or a weight-bearing line ratio of 57–67% was considered an ideal target after surgery [
39,
43]. Lee et al. [
6] compared the patients’ reported outcomes, including IKDC subjective score, Knee Injury and Osteoarthritis Outcome Score, and Kujala score between under-correction, appropriate correction, and over-correction. They concluded that over-corrected surgery (weight-bearing line raito > 67%) was correlated with inferior patients’ reported outcomes. Traditionally, younger age is known to be associated with successful outcomes after HTO [
38]. On the other hand, an opposite opinion was suggested. Kohn et al. [
40] had investigated the influence of age on clinical outcomes after HTO. They had generated 13 pairs of patients with a mean age at operation of 57 versus 42 (15 years younger). The patients were matched by gender, operation/osteosynthesis method, body mass index, and follow-up period. The patients were compared in respect of Lysholm score, Tengner score, and visual analog pain scale. All outcomes were not significantly different between both groups. They concluded that HTO is an effective surgery for medial compartment osteoarthritis, independent of the patient’s age. Two different studies investigated the effect of preoperative radiographic kissing lesions on postoperative clinical outcomes. Kim et al. [
38] compared the American knee society (AKS) knee and function scores between patients with radiologic kissing lesions (17 patients) and non-kissing lesions (105 patients). Patients with kissing lesions showed similar improvements of AKS knee scores (11.9 ± 5.4 vs. 10.6 ± 3.9,
p = 0.348) and function scores (21.2 ± 3.3 vs. 21.6 ± 4.2,
p = 0.679) with non-kissing lesions. Shon et al. [
41] also compared the Hospital for Special Surgery score, WOMAC index, and Tegner score between kissing lesions (21 cases) and non-kissing lesions (22 cases). All patients’ reported outcomes were not significantly different. In the current study, cartilage regeneration was not associated with superior patients’ outcomes. It seems that further research is needed on the clinical significance of cartilage regeneration.
Jung et al. [
34] conducted a comparison of the regeneration rate of medial compartmental cartilage between postoperative HKA angles greater than 0° and less than 0° following open-wedge HTO. The group with a postoperative HKA angle greater than 0° (under-corrected group) exhibited a significantly lower rate of cartilage regeneration compared to the group with a postoperative HKA angle less than 0° (appropriate or over-corrected group). Our results aligned with this previous study, showing that a greater degree of valgus correction is associated with regeneration of MFC cartilage. Furthermore, we found that Kim et al. [
33] reported a relationship between lower BMI and cartilage regeneration of MFC and MTP following open-wedge HTO. These findings indicate that the factors influencing cartilage regeneration have yet to be clearly identified. Therefore, we believe that a larger volume study is necessary to identify more accurate predictive factors of cartilage regeneration.
Our study had several limitations. First, our study was a retrospective, nonrandomized, sequential review. Therefore, selection bias could have occurred. Second, the follow-up period was relatively short. Third, histological analysis was not performed; therefore, it was difficult to determine the histology of the regenerated cartilage. Fourth, the size of the cartilage defect was not considered.






{kind=link}
{kind=link}