
Metals in Alzheimer’s Disease

 ,
, 
Abstract
1. Alzheimer’s Disease
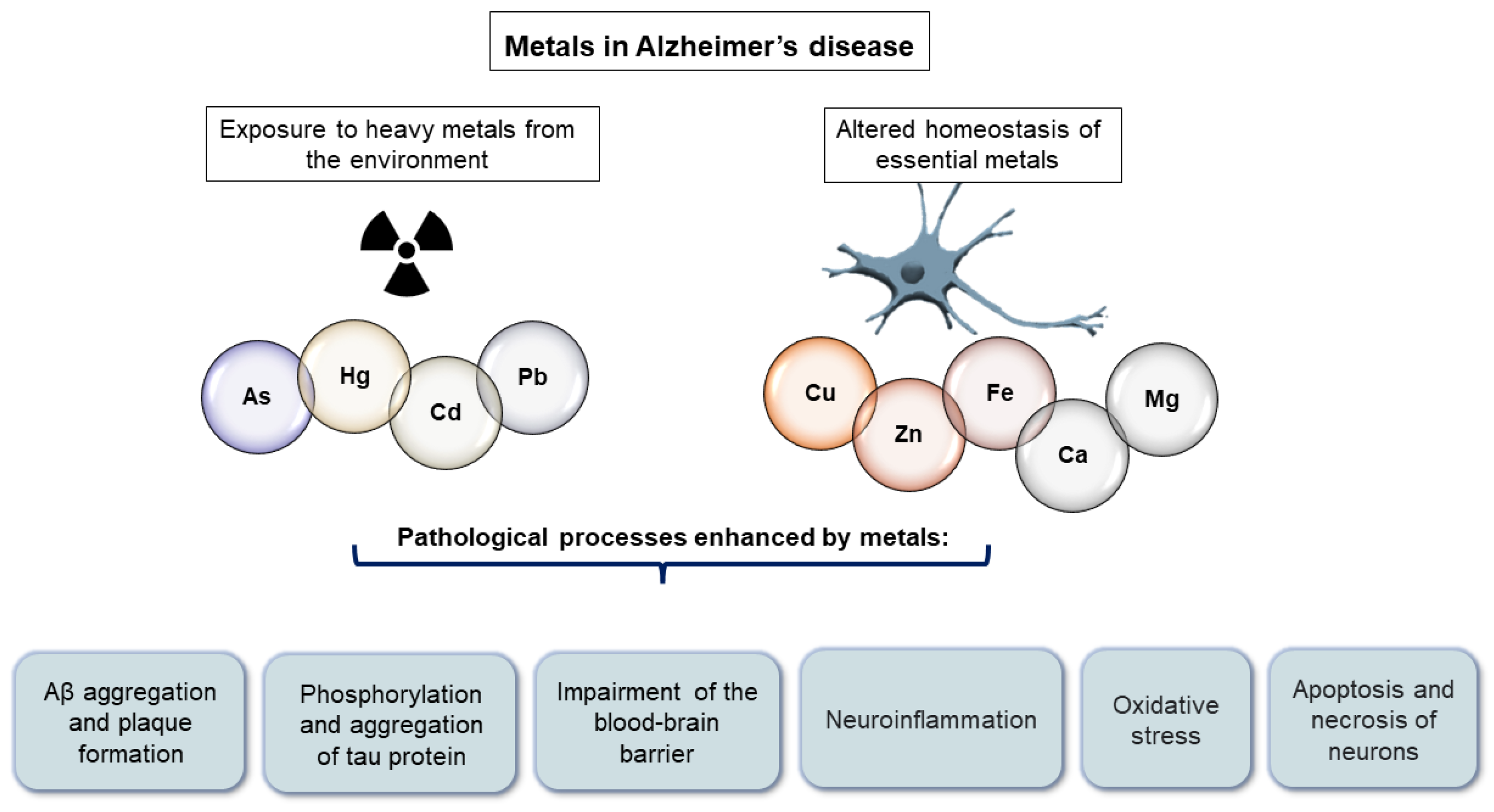
2. Molecular Mechanisms through Which Metals Contribute to Alzheimer’s Disease Pathology
3. Heavy Metals in Alzheimer’s Disease
3.1. Arsenic
3.2. Cadmium
3.3. Mercury
3.4. Lead
3.5. Aluminum
4. Essential Metals in Alzheimer’s Disease
4.1. Iron
4.2. Zinc
4.3. Copper
4.4. Calcium
4.5. Manganese
4.6. Magnesium
4.7. Other Essential Metals
5. Treatment of Alzheimer’s Disease Based on the Metal Hypothesis
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Roda, A.; Serra-Mir, G.; Montoliu-Gaya, L.; Tiessler, L.; Villegas, S. Amyloid-beta peptide and tau protein crosstalk in Alzheimer’s disease. Neural Regen. Res. 2022, 17, 1666–1674. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.S. Amyloid-β and Tau: The Trigger and Bullet in Alzheimer Disease Pathogenesis. JAMA Neurol. 2014, 71, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kang, J.; Ho, A.; Watanabe, H.; Bolshakov, V.Y.; Shen, J. APP Family Regulates Neuronal Excitability and Synaptic Plasticity but Not Neuronal Survival. Neuron 2020, 108, 676–690. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.W.; Thompson, R.; Zhang, H.; Xu, H. APP processing in Alzheimer’s disease. Mol. Brain 2011, 4, 3. [Google Scholar] [CrossRef]
- Masters, C.L.; Simms, G.; Weinman, N.A.; Multhaupt, G.; Mcdonald, B.L.; Beyreuthert, K. Amyloid plaque core protein in Alzheimer disease and Down syndrome. Med. Sci. 1985, 82, 4245–4249. [Google Scholar] [CrossRef]
- Jarrett, J.T.; Berger, E.P.; Lansbury, P.T. The carboxy terminus of the beta amyloid protein is critical for the seeding of amyloid formation: Implications for the pathogenesis of Alzheimer’s disease. Biochemistry 1993, 32, 4693–4697. [Google Scholar] [CrossRef]
- Cai, Z.; Hussain, M.D.; Yan, L.-J. Microglia, neuroinflammation, and beta-amyloid protein in Alzheimer’s disease. Int. J. Neurosci. 2014, 124, 307–321. [Google Scholar] [CrossRef]
- Attems, J.; Lintner, F.; Jellinger, K.A. Amyloid beta peptide 1–42 highly correlates with capillary cerebral amyloid angiopathy and Alzheimer disease pathology. Acta Neuropathol. 2004, 107, 479–480. [Google Scholar] [CrossRef]
- Jellinger, K.A. Alzheimer disease and cerebrovascular pathology: An update. J. Neural Transm. 2002, 109, 813–836. [Google Scholar] [CrossRef]
- Preston, S.D.; Steart, P.V.; Wilkinson, A.; Nicoll, J.A.R.; Weller, R.O. Capillary and arterial cerebral amyloid angiopathy in Alzheimer’s disease: Defining the perivascular route for the elimination of amyloid beta from the human brain. Neuropathol. Appl. Neurobiol. 2003, 29, 106–117. [Google Scholar] [CrossRef]
- Zekry, D.; Duyckaerts, C.; Belmin, J.; Geoffre, C.; Moulias, R.; Hauw, J.-J. Cerebral amyloid angiopathy in the elderly: Vessel walls changes and relationship with dementia. Acta Neuropathol. 2003, 106, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Barbier, P.; Zejneli, O.; Martinho, M.; Lasorsa, A.; Belle, V.; Smet-Nocca, C.; Tsvetkov, P.O.; Devred, F.; Landrieu, I. Role of tau as a microtubule-associated protein: Structural and functional aspects. Front. Aging Neurosci. 2019, 10, 204. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.V.; Jenkins, S.M. Tau protein in normal and Alzheimer’s disease brain. J. Alzheimers Dis. 1999, 1, 307–328. [Google Scholar] [CrossRef] [PubMed]
- Grundke-Iqbal, I.; Iqbal, K.; Tung, Y.C.; Quinlan, M.; Wisniewski, H.M.; Binder, L.I. Abnormal phosphorylation of the microtubule-associated protein tau (tau) in Alzheimer cytoskeletal pathology. Proc. Natl. Acad. Sci. USA 1986, 83, 4913–4917. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.; Selkoe, D.J. The amyloid hypothesis of Alzheimer’s disease: Progress and problems on the road to therapeutics. Science 2002, 297, 353–356. [Google Scholar] [CrossRef]
- Blazquez-Llorca, L.; Valero-Freitag, S.; Rodrigues, E.F.; Merchán-Pérez, Á.; Rodríguez, J.R.; Dorostkar, M.M.; DeFelipe, J.; Herms, J. High plasticity of axonal pathology in Alzheimer’s disease mouse models. Acta Neuropathol. Commun. 2017, 5, 14. [Google Scholar] [CrossRef]
- Masliah, E.; Mallory, M.; Hansen, L.; Alford, M.; Albright, T.; DeTeresa, R.; Terry, R.; Baudier, J.; Saitoh, T. Patterns of aberrant sprouting in Alzheimer’s disease. Neuron 1991, 6, 729–739. [Google Scholar] [CrossRef]
- Šimić, G.; Babić Leko, M.; Wray, S.; Harrington, C.; Delalle, I.; Jovanov-Milošević, N.; Bažadona, D.; Buée, L.; de Silva, R.; Di Giovanni, G.; et al. Tau Protein Hyperphosphorylation and Aggregation in Alzheimer’s Disease and Other Tauopathies, and Possible Neuroprotective Strategies. Biomolecules 2016, 6, 6. [Google Scholar] [CrossRef]
- Teter, B.; Ashford, J.W. Neuroplasticity in Alzheimer’s disease. J. Neurosci. Res. 2002, 70, 402–437. [Google Scholar] [CrossRef]
- Mandelkow, E.M.; Mandelkow, E. Tau in Alzheimer’s disease. Trends Cell Biol. 1998, 8, 425–427. [Google Scholar] [CrossRef]
- Skrabana, R.; Kontsek, P.; Mederlyova, A.; Iqbal, K.; Novak, M. Folding of Alzheimer’s core PHF subunit revealed by monoclonal antibody 423. FEBS Lett. 2004, 568, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Jurcău, M.C.; Andronie-Cioara, F.L.; Jurcău, A.; Marcu, F.; Ţiț, D.M.; Pașcalău, N.; Nistor-Cseppentö, D.C. The Link between Oxidative Stress, Mitochondrial Dysfunction and Neuroinflammation in the Pathophysiology of Alzheimer’s Disease: Therapeutic Implications and Future Perspectives. Antioxidants 2022, 11, 2167. [Google Scholar] [CrossRef] [PubMed]
- Šimić, G.; Španić, E.; Langer Horvat, L.; Hof, P.R. Blood-brain barrier and innate immunity in the pathogenesis of Alzheimer’s disease. Prog. Mol. Biol. Transl. Sci. 2019, 168, 99–145. [Google Scholar] [CrossRef] [PubMed]
- Španić, E.; Langer Horvat, L.; Ilić, K.; Hof, P.R.; Šimić, G. NLRP1 Inflammasome Activation in the Hippocampal Formation in Alzheimer’s Disease: Correlation with Neuropathological Changes and Unbiasedly Estimated Neuronal Loss. Cells 2022, 11, 2223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xu, C.; Sun, J.; Shen, H.M.; Wang, J.; Yang, C. Impairment of the autophagy–lysosomal pathway in Alzheimer’s diseases: Pathogenic mechanisms and therapeutic potential. Acta Pharm. Sin. B 2022, 12, 1019–1040. [Google Scholar] [CrossRef] [PubMed]
- Bush, A.I. The metal theory of Alzheimer’s disease. J. Alzheimer’s Dis. 2013, 33 (Suppl. S1), S277–S281. [Google Scholar] [CrossRef]
- Babić Leko, M.; Jurasović, J.; Nikolac Perković, M.; Španić, E.; Sekovanić, A.; Orct, T.; Lukinović Škudar, V.; Bačić Baronica, K.; Kiđemet-Piskač, S.; Vogrinc, Ž.; et al. The Association of Essential Metals with APOE Genotype in Alzheimer’s Disease. J. Alzheimer’s Dis. 2021, 82, 661–672. [Google Scholar] [CrossRef]
- Zubčić, K.; Hof, P.R.; Šimić, G.; Jazvinšćak Jembrek, M. The Role of Copper in Tau-Related Pathology in Alzheimer’s Disease. Front. Mol. Neurosci. 2020, 13, 572308. [Google Scholar] [CrossRef]
- Elonheimo, H.M.; Andersen, H.R.; Katsonouri, A.; Tolonen, H. Environmental Substances Associated with Alzheimer’s Disease-A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11839. [Google Scholar] [CrossRef]
- Yano, K.; Hirosawa, N.; Sakamoto, Y.; Katayama, H.; Moriguchi, T. Aggregations of amyloid beta-proteins in the presence of metal ions. Toxicol. Lett. 2003, 144, 134. [Google Scholar] [CrossRef]
- Wallin, C.; Sholts, S.B.; Österlund, N.; Luo, J.; Jarvet, J.; Roos, P.M.; Ilag, L.; Gräslund, A.; Wärmländer, S.K.T.S. Alzheimer’s disease and cigarette smoke components: Effects of nicotine, PAHs, and Cd(II), Cr(III), Pb(II), Pb(IV) ions on amyloid-β peptide aggregation. Sci. Rep. 2017, 7, 14423. [Google Scholar] [CrossRef] [PubMed]
- Wisessaowapak, C.; Visitnonthachai, D.; Watcharasit, P.; Satayavivad, J. Prolonged arsenic exposure increases tau phosphorylation in differentiated SH-SY5Y cells: The contribution of GSK3 and ERK1/2. Environ. Toxicol. Pharmacol. 2021, 84, 103626. [Google Scholar] [CrossRef] [PubMed]
- Shati, A.A.; Alfaifi, M.Y. Trans-resveratrol Inhibits Tau Phosphorylation in the Brains of Control and Cadmium Chloride-Treated Rats by Activating PP2A and PI3K/Akt Induced-Inhibition of GSK3β. Neurochem. Res. 2019, 44, 357–373. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Yang, J.; Zhang, Y.; Li, T.; Wang, C.; Xu, L.; Hu, Q.; Wang, X.; Jiang, S.; Nie, X.; et al. Arsenic trioxide mediates HAPI microglia inflammatory response and subsequent neuron apoptosis through p38/JNK MAPK/STAT3 pathway. Toxicol. Appl. Pharmacol. 2016, 303, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Augusti, P.R.; Conterato, G.M.M.; Somacal, S.; Sobieski, R.; Spohr, P.R.; Torres, J.V.; Charão, M.F.; Moro, A.M.; Rocha, M.P.; Garcia, S.C.; et al. Effect of astaxanthin on kidney function impairment and oxidative stress induced by mercuric chloride in rats. Food Chem. Toxicol. 2008, 46, 212–219. [Google Scholar] [CrossRef]
- Gu, H.; Territo, P.R.; Persohn, S.A.; Bedwell, A.A.; Eldridge, K.; Speedy, R.; Chen, Z.; Zheng, W.; Du, Y. Evaluation of chronic lead effects in the blood brain barrier system by DCE-CT. J. Trace Elem. Med. Biol. 2020, 62, 126648. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Bhaumik, S.; Purkayastha, M.; Basu, S.; Nag Chaudhuri, A.; Das Gupta, S. Apoptosis and necrosis in developing brain cells due to arsenic toxicity and protection with antioxidants. Toxicol. Lett. 2002, 136, 65–76. [Google Scholar] [CrossRef]
- Bashir, S.; Sharma, Y.; Irshad, M.; Gupta, S.D.; Dogra, T.D. Arsenic-induced cell death in liver and brain of experimental rats. Basic Clin. Pharmacol. Toxicol. 2006, 98, 38–43. [Google Scholar] [CrossRef]
- Wang, L.; Yin, Y.L.; Liu, X.Z.; Shen, P.; Zheng, Y.G.; Lan, X.R.; Lu, C.B.; Wang, J.Z. Current understanding of metal ions in the pathogenesis of Alzheimer’s disease. Transl. Neurodegener. 2020, 9, 10. [Google Scholar] [CrossRef]
- Syme, C.D.; Viles, J.H. Solution 1H NMR investigation of Zn2+ and Cd2+ binding to amyloid-beta peptide (Abeta) of Alzheimer’s disease. Biochim. Biophys. Acta 2006, 1764, 246–256. [Google Scholar] [CrossRef]
- Jiao, Y.; Han, D.; Yang, P. Molecular modeling of the inhibitory mechanism of copper(II) on aggregation of amyloid β-peptide. Sci. China Ser. B 2005, 48, 580. [Google Scholar] [CrossRef]
- Kitazawa, M.; Cheng, D.; Laferla, F.M. Chronic copper exposure exacerbates both amyloid and tau pathology and selectively dysregulates cdk5 in a mouse model of AD. J. Neurochem. 2009, 108, 1550–1560. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.-X.; Du, J.-T.; Zeng, Z.-Y.; Wu, W.-H.; Zhao, Y.-F.; Kanazawa, K.; Ishizuka, Y.; Nemoto, T.; Nakanishi, H.; Li, Y.-M. Copper (II) modulates in vitro aggregation of a tau peptide. Peptides 2007, 28, 2229–2234. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.F.; Yao, T.M.; Zhu, Z.L.; Wang, C.; Ji, L.N. Impacts of Cd(II) on the conformation and self-aggregation of Alzheimer’s tau fragment corresponding to the third repeat of microtubule-binding domain. Biochim. Biophys. Acta 2007, 1774, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Ashok, A.; Rai, N.K.; Tripathi, S.; Bandyopadhyay, S. Exposure to As-, Cd-, and Pb-mixture induces Aβ, amyloidogenic APP processing and cognitive impairments via oxidative stress-dependent neuroinflammation in young rats. Toxicol. Sci. 2015, 143, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Kanti Das, T.; Wati, M.R.; Fatima-Shad, K. Oxidative Stress Gated by Fenton and Haber Weiss Reactions and Its Association with Alzheimer’s Disease. Arch. Neurosci. 2015, 2, e20078. [Google Scholar] [CrossRef]
- Gaetke, L.M.; Chow, C.K. Copper toxicity, oxidative stress, and antioxidant nutrients. Toxicology 2003, 189, 147–163. [Google Scholar] [CrossRef]
- Branca, J.J.V.; Maresca, M.; Morucci, G.; Mello, T.; Becatti, M.; Pazzagli, L.; Colzi, I.; Gonnelli, C.; Carrino, D.; Paternostro, F.; et al. Effects of Cadmium on ZO-1 Tight Junction Integrity of the Blood Brain Barrier. Int. J. Mol. Sci. 2019, 20, 6010. [Google Scholar] [CrossRef]
- Zhang, T.; Xu, Z.; Wen, L.; Lei, D.; Li, S.; Wang, J.; Huang, J.; Wang, N.; Durkan, C.; Liao, X.; et al. Cadmium-induced dysfunction of the blood-brain barrier depends on ROS-mediated inhibition of PTPase activity in zebrafish. J. Hazard. Mater. 2021, 412, 125198. [Google Scholar] [CrossRef]
- Wolonciej, M.; Milewska, E.; Roszkowska-Jakimiec, W. Trace elements as an activator of antioxidant enzymes. Postep. Hig. Med. Dosw. 2016, 70, 1483–1498. [Google Scholar] [CrossRef]
- Charlet, L.; Chapron, Y.; Faller, P.; Kirsch, R.; Stone, A.T.; Baveye, P.C. Neurodegenerative diseases and exposure to the environmental metals Mn, Pb, and Hg. Coord. Chem. Rev. 2012, 256, 2147–2163. [Google Scholar] [CrossRef]
- Garza-Lombó, C.; Pappa, A.; Panayiotidis, M.I.; Gonsebatt, M.E.; Franco, R. Arsenic-induced neurotoxicity: A mechanistic appraisal. J. Biol. Inorg. Chem. 2019, 24, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Sunderman Jr, F. Nasal toxicity, carcinogenicity, and olfactory uptake of metals. Ann. Clin. Lab. Sci. 2001, 31, 3–24. [Google Scholar] [PubMed]
- Niño, S.A.; Vázquez-Hernández, N.; Arevalo-Villalobos, J.; Chi-Ahumada, E.; Martín-Amaya-Barajas, F.L.; Díaz-Cintra, S.; Martel-Gallegos, G.; González-Burgos, I.; Jiménez-Capdeville, M.E. Cortical Synaptic Reorganization Under Chronic Arsenic Exposure. Neurotox. Res. 2021, 39, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Bihaqi, S.W.; Bahmani, A.; Subaiea, G.M.; Zawia, N.H. Infantile exposure to lead and late-age cognitive decline: Relevance to AD. Alzheimers Dement. 2014, 10, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Gustin, K.; Tofail, F.; Vahter, M.; Kippler, M. Cadmium exposure and cognitive abilities and behavior at 10 years of age: A prospective cohort study. Environ. Int. 2018, 113, 259–268. [Google Scholar] [CrossRef]
- Borenstein, A.R.; Copenhaver, C.I.; Mortimer, J.A. Early-life risk factors for Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2006, 20, 63–72. [Google Scholar] [CrossRef]
- Miller, D.B.; O’Callaghan, J.P. Do early-life insults contribute to the late-life development of Parkinson and Alzheimer diseases? Metabolism 2008, 57 (Suppl. S2), 244–249. [Google Scholar] [CrossRef]
- Gauvrit, T.; Benderradji, H.; Buée, L.; Blum, D.; Vieau, D. Early-Life Environment Influence on Late-Onset Alzheimer’s Disease. Front. Cell Dev. Biol. 2022, 10, 834661. [Google Scholar] [CrossRef]
- Podgorski, J.; Berg, M. Global threat of arsenic in groundwater. Science 2020, 368, 845–850. [Google Scholar] [CrossRef]
- O’Bryant, S.E.; Edwards, M.; Menon, C.V.; Gong, G.; Barber, R. Long-term low-level arsenic exposure is associated with poorer neuropsychological functioning: A Project FRONTIER study. Int. J. Environ. Res. Public Health 2011, 8, 861–874. [Google Scholar] [CrossRef]
- Yang, Y.W.; Liou, S.H.; Hsueh, Y.M.; Lyu, W.S.; Liu, C.S.; Liu, H.J.; Chung, M.C.; Hung, P.H.; Chung, C.J. Risk of Alzheimer’s disease with metal concentrations in whole blood and urine: A case-control study using propensity score matching. Toxicol. Appl. Pharmacol. 2018, 356, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Li, X.L.; Zhan, R.Q.; Zheng, W.; Jiang, H.; Zhang, D.F.; Shen, X.L. Positive association between soil arsenic concentration and mortality from Alzheimer’s disease in mainland China. J. Trace Elem. Med. Biol. 2020, 59, 126452. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhang, C.; Liu, W. Effects of arsenic on the offspring development in mice. Zhonghua Yu Fang Yi Xue Za Zhi 1994, 28, 20–23. [Google Scholar] [PubMed]
- Tyler, C.R.; Allan, A.M. The Effects of Arsenic Exposure on Neurological and Cognitive Dysfunction in Human and Rodent Studies: A Review. Curr. Environ. Health Rep. 2014, 1, 132–147. [Google Scholar] [CrossRef] [PubMed]
- Samad, N.; Jabeen, S.; Imran, I.; Zulfiqar, I.; Bilal, K. Protective effect of gallic acid against arsenic-induced anxiety-/depression- like behaviors and memory impairment in male rats. Metab. Brain Dis. 2019, 34, 1091–1102. [Google Scholar] [CrossRef]
- Zarazúa, S.; Bürger, S.; Delgado, J.M.; Jiménez-Capdeville, M.E.; Schliebs, R. Arsenic affects expression and processing of amyloid precursor protein (APP) in primary neuronal cells overexpressing the Swedish mutation of human APP. Int. J. Dev. Neurosci. 2011, 29, 389–396. [Google Scholar] [CrossRef]
- Giasson, B.I.; Sampathu, D.M.; Wilson, C.A.; Vogelsberg-Ragaglia, V.; Mushynski, W.E.; Lee, V.M.Y. The environmental toxin arsenite induces tau hyperphosphorylation. Biochemistry 2002, 41, 15376–15387. [Google Scholar] [CrossRef]
- Pakzad, D.; Akbari, V.; Sepand, M.R.; Aliomrani, M. Risk of neurodegenerative disease due to tau phosphorylation changes and arsenic exposure via drinking water. Toxicol. Res. 2021, 10, 325–333. [Google Scholar] [CrossRef]
- Hassani, S.; Yaghoubi, H.; Khosrokhavar, R.; Jafarian, I.; Mashayekhi, V.; Hosseini, M.J.; Shahraki, J. Mechanistic view for toxic effects of arsenic on isolated rat kidney and brain mitochondria. Biologia 2015, 70, 683–689. [Google Scholar] [CrossRef]
- Tsinovoi, C.L.; Xun, P.; McClure, L.A.; Carioni, V.M.O.; Brockman, J.D.; Cai, J.; Guallar, E.; Cushman, M.; Unverzagt, F.W.; Howard, V.J.; et al. Arsenic Exposure in Relation to Ischemic Stroke: The Reasons for Geographic and Racial Differences in Stroke Study. Stroke 2018, 49, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Koseoglu, E.; Kutuk, B.; Nalbantoglu, O.U.; Koseoglu, R.; Kendirci, M. Arsenic and selenium measurements in nail and hair show important relationships to Alzheimer’s disease in the elderly. J. Trace Elem. Med. Biol. 2021, 64, 126684. [Google Scholar] [CrossRef] [PubMed]
- Strumylaite, L.; Kregzdyte, R.; Kucikiene, O.; Baranauskiene, D.; Simakauskiene, V.; Naginiene, R.; Damuleviciene, G.; Lesauskaite, V.; Zemaitiene, R. Alzheimer’s Disease Association with Metals and Metalloids Concentration in Blood and Urine. Int. J. Environ. Res. Public Health 2022, 19, 7309. [Google Scholar] [CrossRef] [PubMed]
- Babić Leko, M.; Mihelčić, M.; Jurasović, J.; Nikolac Perković, M.; Španić, E.; Sekovanić, A.; Orct, T.; Zubčić, K.; Langer Horvat, L.; Pleić, N.; et al. Heavy Metals and Essential Metals Are Associated with Cerebrospinal Fluid Biomarkers of Alzheimer’s Disease. Int. J. Mol. Sci. 2023, 24, 467. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Moore, M.R. Adverse Health Effects of Chronic Exposure to Low-Level Cadmium in Foodstuffs and Cigarette Smoke. Environ. Health Perspect. 2004, 112, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- ATSDR. Toxicological Profile for Cadmium; Agency for Toxic Substances & Disease Registry, Department of Health and Human Services, Public Health Service: Atlanta, GA, USA, 2012.
- Min, J.Y.; Min, K.B. Blood cadmium levels and Alzheimer’s disease mortality risk in older US adults. Environ. Health A Glob. Access Sci. Source 2016, 15, 69. [Google Scholar] [CrossRef]
- Peng, Q.; Bakulski, K.M.; Nan, B.; Park, S.K. Cadmium and Alzheimer’s disease mortality in U.S. adults: Updated evidence with a urinary biomarker and extended follow-up time. Environ. Res. 2017, 157, 44–51. [Google Scholar] [CrossRef]
- Souza-Talarico, J.N.; Marcourakis, T.; Barbosa, F.; Moraes Barros, S.B.; Rivelli, D.P.; Pompéia, S.; Caramelli, P.; Plusquellec, P.; Lupien, S.J.; Catucci, R.F.; et al. Association between heavy metal exposure and poor working memory and possible mediation effect of antioxidant defenses during aging. Sci. Total Environ. 2017, 575, 750–757. [Google Scholar] [CrossRef]
- Li, H.; Wang, Z.; Fu, Z.; Yan, M.; Wu, N.; Wu, H.; Yin, P. Associations between blood cadmium levels and cognitive function in a cross-sectional study of US adults aged 60 years or older. BMJ Open 2018, 8, e020533. [Google Scholar] [CrossRef]
- Huang, G.; Ren, G. Interaction between ω-6 fatty acids intake and blood cadmium on the risk of low cognitive performance in older adults from National Health and Nutrition Examination Survey (NHANES) 2011-2014. BMC Geriatr. 2022, 22, 292. [Google Scholar] [CrossRef]
- Ruczaj, A.; Brzóska, M.M. Environmental exposure of the general population to cadmium as a risk factor of the damage to the nervous system: A critical review of current data. J. Appl. Toxicol. 2022, 43, 66–88. [Google Scholar] [CrossRef]
- Notarachille, G.; Arnesano, F.; Calò, V.; Meleleo, D. Heavy metals toxicity: Effect of cadmium ions on amyloid beta protein 1–42. Possible implications for Alzheimer’s disease. Biometals 2014, 27, 371–388. [Google Scholar] [CrossRef] [PubMed]
- del Pino, J.; Zeballos, G.; Anadón, M.J.; Moyano, P.; Díaz, M.J.; García, J.M.; Frejo, M.T. Cadmium-induced cell death of basal forebrain cholinergic neurons mediated by muscarinic M1 receptor blockade, increase in GSK-3β enzyme, β-amyloid and tau protein levels. Arch. Toxicol. 2016, 90, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lv, Y.; Yu, S.; Zhao, H.; Yao, L. The effect of cadmium on Aβ levels in APP/PS1 transgenic mice. Exp. Ther. Med. 2012, 4, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Yadav, J.; Verma, A.K.; Ahmad, M.K.; Garg, R.K.; Shiuli; Mahdi, A.A.; Srivastava, S. Metals toxicity and its correlation with the gene expression in Alzheimer’s disease. Mol. Biol. Rep. 2021, 48, 3245–3252. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Li, A.; Mei, Y.; Zhao, J.; Zhou, Q.; Li, Y.; Yang, M.; Xu, Q. Trace elements and Alzheimer dementia in population-based studies: A bibliometric and meta-analysis. Environ. Pollut. 2023, 318, 120782. [Google Scholar] [CrossRef]
- Kazemi, T.; Moodi, M.; Rajabi, S.; Sharifi, F.; Samarghandian, S.; Khorashadizadeh, M.; Farkhondeh, T. Trace Element Concentration and Cognitive Dysfunction in Elderly Residents in Birjand. Curr. Alzheimer Res. 2022, 19, 674–680. [Google Scholar] [CrossRef]
- Du, K.; Zheng, X.; Ma, Z.T.; Lv, J.Y.; Jiang, W.J.; Liu, M.Y. Association of Circulating Magnesium Levels in Patients with Alzheimer’s Disease From 1991 to 2021: A Systematic Review and Meta-Analysis. Front. Aging Neurosci. 2022, 13, 799824. [Google Scholar] [CrossRef]
- Banerjee, G.; Forsgard, N.; Ambler, G.; Keshavan, A.; Paterson, R.W.; Foiani, M.S.; Toombs, J.; Heslegrave, A.; Thompson, E.J.; Lunn, M.P.; et al. Cerebrospinal fluid metallomics in cerebral amyloid angiopathy: An exploratory analysis. J. Neurol. 2022, 269, 1470–1475. [Google Scholar] [CrossRef]
- Socha, K.; Klimiuk, K.; Naliwajko, S.K.; Soroczyńska, J.; Puścion-jakubik, A.; Markiewicz-żukowska, R.; Kochanowicz, J. Dietary Habits, Selenium, Copper, Zinc and Total Antioxidant Status in Serum in Relation to Cognitive Functions of Patients with Alzheimer’s Disease. Nutrients 2021, 13, 287. [Google Scholar] [CrossRef]
- Squitti, R.; Ventriglia, M.; Simonelli, I.; Bonvicini, C.; Costa, A.; Perini, G.; Binetti, G.; Benussi, L.; Ghidoni, R.; Koch, G.; et al. Copper Imbalance in Alzheimer’s Disease: Meta-Analysis of Serum, Plasma, and Brain Specimens, and Replication Study Evaluating ATP7B Gene Variants. Biomolecules 2021, 11, 960. [Google Scholar] [CrossRef] [PubMed]
- Ficiarà, E.; Boschi, S.; Ansari, S.; D’Agata, F.; Abollino, O.; Caroppo, P.; Di Fede, G.; Indaco, A.; Rainero, I.; Guiot, C. Machine Learning Profiling of Alzheimer’s Disease Patients Based on Current Cerebrospinal Fluid Markers and Iron Content in Biofluids. Front. Aging Neurosci. 2021, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, C.Q.d.; Barros-Neto, J.A.; Vieira, N.F.L.; Menezes-Filho, J.A.; Neves, S.J.F.; Lima, S.O. Selenium concentrations in elderly people with Alzheimer’s disease: A cross-sectional study with control group. Rev. Bras. Enferm. 2021, 74, e20200984. [Google Scholar] [CrossRef] [PubMed]
- Thomassen, J.Q.; Tolstrup, J.S.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Frikke-Schmidt, R. Plasma Concentrations of Magnesium and Risk of Dementia: A General Population Study of 102 648 Individuals. Clin. Chem. 2021, 67, 899–911. [Google Scholar] [CrossRef] [PubMed]
- Souza, L.A.C.; Trebak, F.; Kumar, V.; Satou, R.; Kehoe, P.G.; Yang, W.; Wharton, W.; Earley, Y.F. Elevated cerebrospinal fluid sodium in hypertensive human subjects with a family history of Alzheimer’s disease. Physiol. Genom. 2020, 52, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Ben Zaken, S.; Radomysky, Z.; Koren, G. Association Between Serum Magnesium Levels and Alzheimer’s Disease or Mixed Dementia Patients: A Population-Based Retrospective Controlled Study. J. Alzheimer’s Dis. Rep. 2020, 4, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Giil, L.M.; Solvang, S.E.H.; Giil, M.M.; Hellton, K.H.; Skogseth, R.E.; Vik-Mo, A.O.; Hortobágyi, T.; Aarsland, D.; Nordrehaug, J.E. Serum Potassium Is Associated with Cognitive Decline in Patients with Lewy Body Dementia. J. Alzheimer’s Dis. 2019, 68, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Giacconi, R.; Giuli, C.; Casoli, T.; Balietti, M.; Costarelli, L.; Provinciali, M.; Basso, A.; Piacenza, F.; Postacchini, D.; Galeazzi, R.; et al. Acetylcholinesterase inhibitors in Alzheimer’s disease influence Zinc and Copper homeostasis. J. Trace Elem. Med. Biol. 2019, 55, 58–63. [Google Scholar] [CrossRef]
- Ashraf, A.; Stosnach, H.; Parkes, H.G.; Hye, A.; Powell, J.; Soinine, H.; Tsolaki, M.; Vellas, B.; Lovestone, S.; Aarsland, D.; et al. Pattern of Altered Plasma Elemental Phosphorus, Calcium, Zinc, and Iron in Alzheimer’s Disease. Sci. Rep. 2019, 9, 3147. [Google Scholar] [CrossRef]
- Vaz, F.N.C.; Fermino, B.L.; Haskel, M.V.L.; Wouk, J.; de Freitas, G.B.L.; Fabbri, R.; Montagna, E.; Rocha, J.B.T.; Bonini, J.S. The Relationship Between Copper, Iron, and Selenium Levels and Alzheimer Disease. Biol. Trace Elem. Res. 2018, 181, 185–191. [Google Scholar] [CrossRef]
- Vintimilla, R.M.; Large, S.E.; Gamboa, A.; Rohlfing, G.D.; O’Jile, J.R.; Hall, J.R.; O’Bryant, S.E.; Johnson, L.A. The Link between Potassium and Mild Cognitive Impairment in Mexican-Americans. Dement. Geriatr. Cogn. Dis. Extra 2018, 8, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Fathabadi, B.; Dehghanifiroozabadi, M.; Aaseth, J.; Sharifzadeh, G.; Nakhaee, S.; Rajabpour-Sanati, A.; Amirabadizadeh, A.; Mehrpour, O. Comparison of Blood Lead Levels in Patients with Alzheimer’s Disease and Healthy People. Am. J. Alzheimers Dis. Other Demen. 2018, 33, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Kushnir, M.M.; Michno, W.; Rockwood, A.L.; Blennow, K.; Strathmann, F.G.; Hanrieder, J. Association of PTHrP levels in CSF with Alzheimer’s disease biomarkers. Clin. Mass Spectrom. 2018, 14 Pt B, 124–129. [Google Scholar] [CrossRef]
- Squitti, R.; Ghidoni, R.; Simonelli, I.; Ivanova, I.D.; Colabufo, N.A.; Zuin, M.; Benussi, L.; Binetti, G.; Cassetta, E.; Rongioletti, M.; et al. Copper dyshomeostasis in Wilson disease and Alzheimer’s disease as shown by serum and urine copper indicators. J. Trace Elem. Med. Biol. 2018, 45, 181–188. [Google Scholar] [CrossRef]
- Xu, J.; Church, S.J.; Patassini, S.; Begley, P.; Kellett, K.A.B.; Vardy, E.R.L.C.; Unwin, R.D.; Hooper, N.M.; Cooper, G.J.S. Plasma metals as potential biomarkers in dementia: A case-control study in patients with sporadic Alzheimer’s disease. Biometals 2018, 31, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Guan, C.; Dang, R.; Cui, Y.; Liu, L.; Chen, X.; Wang, X.; Zhu, J.; Li, D.; Li, J.; Wang, D. Characterization of plasma metal profiles in Alzheimer’s disease using multivariate statistical analysis. PLoS ONE 2017, 12, e0178271. [Google Scholar] [CrossRef]
- Kieboom, B.C.T.; Licher, S.; Wolters, F.J.; Ikram, M.K.; Hoorn, E.J.; Zietse, R.; Stricker, B.H.; Ikram, M.A. Serum magnesium is associated with the risk of dementia. Neurology 2017, 89, 1716–1722. [Google Scholar] [CrossRef]
- Balmuș, I.M.; Strungaru, S.A.; Ciobica, A.; Nicoara, M.N.; Dobrin, R.; Plavan, G.; Ștefănescu, C. Preliminary Data on the Interaction between Some Biometals and Oxidative Stress Status in Mild Cognitive Impairment and Alzheimer’s Disease Patients. Oxid. Med. Cell. Longev. 2017, 2017, 7156928. [Google Scholar] [CrossRef]
- Du, K.; Liu, M.; Pan, Y.; Zhong, X.; Wei, M. Association of Serum Manganese Levels with Alzheimer’s Disease and Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 231. [Google Scholar] [CrossRef]
- Reddy, V.S.; Bukke, S.; Dutt, N.; Rana, P.; Pandey, A.K. A systematic review and meta-analysis of the circulatory, erythrocellular and CSF selenium levels in Alzheimer’s disease: A metal meta-analysis (AMMA study-I). J. Trace Elem. Med. Biol. 2017, 42, 68–75. [Google Scholar] [CrossRef]
- Pu, Z.; Xu, W.; Lin, Y.; He, J.; Huang, M. Oxidative Stress Markers and Metal Ions are Correlated with Cognitive Function in Alzheimer’s Disease. Am. J. Alzheimers. Dis. Other Demen. 2017, 32, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, B.R.; Hare, D.J.; Bush, A.I.; Li, Q.X.; Fowler, C.J.; Masters, C.L.; Martins, R.N.; Ganio, K.; Lothian, A.; Mukherjee, S.; et al. Selenium Levels in Serum, Red Blood Cells, and Cerebrospinal Fluid of Alzheimer’s Disease Patients: A Report from the Australian Imaging, Biomarker & Lifestyle Flagship Study of Ageing (AIBL). J. Alzheimer’s Dis. 2017, 57, 183–193. [Google Scholar] [CrossRef]
- Chmatalova, Z.; Vyhnalek, M.; Laczo, J.; Hort, J.; Pospisilova, R.; Pechova, M.; Skoumalova, A.; Chmátalová, Z. Relation of Plasma Selenium and Lipid Peroxidation End Products in Patients with Alzheimer’s Disease. Physiol. Res. 2017, 66, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- de Wilde, M.C.; Vellas, B.; Girault, E.; Yavuz, A.C.; Sijben, J.W. Lower brain and blood nutrient status in Alzheimer’s disease: Results from meta-analyses. Alzheimer’s Dement. 2017, 3, 416–431. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.R.; Doecke, J.D.; Rembach, A.; Yévenes, L.F.; Fowler, C.J.; McLean, C.A.; Lind, M.; Volitakis, I.; Masters, C.L.; Bush, A.I.; et al. Rubidium and potassium levels are altered in Alzheimer’s disease brain and blood but not in cerebrospinal fluid. Acta Neuropathol. Commun. 2016, 4, 119. [Google Scholar] [CrossRef]
- Paglia, G.; Miedico, O.; Cristofano, A.; Vitale, M.; Angiolillo, A.; Chiaravalle, A.E.; Corso, G.; Di Costanzo, A. Distinctive Pattern of Serum Elements During the Progression of Alzheimer’s Disease. Sci. Rep. 2016, 6, 22769. [Google Scholar] [CrossRef]
- Hare, D.J.; Faux, N.G.; Roberts, B.R.; Volitakis, I.; Martins, R.N.; Bush, A.I. Lead and manganese levels in serum and erythrocytes in Alzheimer’s disease and mild cognitive impairment: Results from the Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing. Metallomics 2016, 8, 628–632. [Google Scholar] [CrossRef]
- Hare, D.J.; Doecke, J.D.; Faux, N.G.; Rembach, A.; Volitakis, I.; Fowler, C.J.; Grimm, R.; Doble, P.A.; Cherny, R.A.; Masters, C.L.; et al. Decreased plasma iron in Alzheimer’s disease is due to transferrin desaturation. ACS Chem. Neurosci. 2015, 6, 398–402. [Google Scholar] [CrossRef]
- Koç, E.R.; Ilhan, A.; Aytürk, Z.; Acar, B.; Gürler, M.; Altuntaş, A.; Karapirli, M.; Bodur, A.S. A comparison of hair and serum trace elements in patients with Alzheimer disease and healthy participants. Turk. J. Med. Sci. 2015, 45, 1034–1039. [Google Scholar] [CrossRef]
- Negahdar, H.; Hosseini, S.R.; Parsian, H.; Kheirkhah, F.; Mosapour, A.; Khafri, S.; Haghighi, A.H. Homocysteine, trace elements and oxidant/antioxidant status in mild cognitively impaired elderly persons: A cross-sectional study. Rom. J. Intern. Med. 2015, 53, 336–342. [Google Scholar] [CrossRef]
- Wang, Z.-X.; Tan, L.; Wang, H.-F.; Ma, J.; Liu, J.; Tan, M.-S.; Sun, J.-H.; Zhu, X.-C.; Jiang, T.; Yu, J.-T. Serum Iron, Zinc, and Copper Levels in Patients with Alzheimer’s Disease: A Replication Study and Meta-Analyses. J. Alzheimer’s Dis. 2015, 47, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Ventriglia, M.; Brewer, G.J.; Simonelli, I.; Mariani, S.; Siotto, M.; Bucossi, S.; Squitti, R. Zinc in Alzheimer’s Disease: A Meta-Analysis of Serum, Plasma, and Cerebrospinal Fluid Studies. J. Alzheimer’s Dis. 2015, 46, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Giacoppo, S.; Galuppo, M.; Calabrò, R.S.; D’Aleo, G.; Marra, A.; Sessa, E.; Bua, D.G.; Potortì, A.G.; Dugo, G.; Bramanti, P.; et al. Heavy metals and neurodegenerative diseases: An observational study. Biol. Trace Elem. Res. 2014, 161, 151–160. [Google Scholar] [CrossRef]
- Faux, N.G.; Rembach, A.; Wiley, J.; Ellis, K.A.; Ames, D.; Fowler, C.J.; Martins, R.N.; Pertile, K.K.; Rumble, R.L.; Trounson, B.; et al. An anemia of Alzheimer’s disease. Mol. Psychiatry 2014, 19, 1227–1234. [Google Scholar] [CrossRef]
- Olde Rikkert, M.G.M.; Verhey, F.R.; Sijben, J.W.C.; Bouwman, F.H.; Dautzenberg, P.L.J.; Lansink, M.; Sipers, W.M.W.; Van Asselt, D.Z.B.; Van Hees, A.M.J.; Stevens, M.; et al. Differences in nutritional status between very mild Alzheimer’s disease patients and healthy controls. J. Alzheimer’s Dis. 2014, 41, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Lee, D.-W.; Park, K.S.; Joung, H. Serum Trace Metal Levels in Alzheimer’s Disease and Normal Control Groups. Am. J. Alzheimer’s Dis. Other Dement. 2014, 29, 76–83. [Google Scholar] [CrossRef]
- González-Domínguez, R.; García-Barrera, T.; Gómez-Ariza, J.L. Characterization of metal profiles in serum during the progression of Alzheimer’s disease. Metallomics 2014, 6, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Wang, Y.; Rogers, J.T.; Wang, F. Perturbed iron distribution in Alzheimer’s disease serum, cerebrospinal fluid, and selected brain regions: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2014, 42, 679–690. [Google Scholar] [CrossRef]
- Rembach, A.; Hare, D.J.; Doecke, J.D.; Burnham, S.C.; Volitakis, I.; Fowler, C.J.; Cherny, R.A.; McLean, C.; Grimm, R.; Martins, R.; et al. Decreased serum zinc is an effect of ageing and not Alzheimer’s disease. Metallomics 2014, 6, 1216–1219. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, J.H.; Choi, D.W.; Lee, D.W.; Park, J.H.; Yoon, H.J.; Pyo, H.S.; Kwon, H.J.; Park, K.S. The Association of Heavy Metal of Blood and Serum in the Alzheimer’s Diseases. Toxicol. Res. 2012, 28, 93–98. [Google Scholar] [CrossRef]
- Hozumi, I.; Hasegawa, T.; Honda, A.; Ozawa, K.; Hayashi, Y.; Hashimoto, K.; Yamada, M.; Koumura, A.; Sakurai, T.; Kimura, A.; et al. Patterns of levels of biological metals in CSF differ among neurodegenerative diseases. J. Neurol. Sci. 2011, 303, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Bucossi, S.; Ventriglia, M.; Panetta, V.; Salustri, C.; Pasqualetti, P.; Mariani, S.; Siotto, M.; Rossini, P.M.; Squitti, R. Copper in Alzheimer’s disease: A meta-analysis of serum, plasma, and cerebrospinal fluid studies. J. Alzheimer’s Dis. 2011, 24, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Gerhardsson, L.; Lundh, T.; Londos, E.; Minthon, L. Cerebrospinal fluid/plasma quotients of essential and non-essential metals in patients with Alzheimer’s disease. J. Neural Transm. 2011, 118, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Baum, L.; Chan, I.H.S.; Cheung, S.K.-K.; Goggins, W.B.; Mok, V.; Lam, L.; Leung, V.; Hui, E.; Ng, C.; Woo, J.; et al. Serum zinc is decreased in Alzheimer’s disease and serum arsenic correlates positively with cognitive ability. Biometals 2010, 23, 173–179. [Google Scholar] [CrossRef]
- Boström, F.; Hansson, O.; Gerhardsson, L.; Lundh, T.; Minthon, L.; Stomrud, E.; Zetterberg, H.; Londos, E. CSF Mg and Ca as diagnostic markers for dementia with Lewy bodies. Neurobiol. Aging 2009, 30, 1265–1271. [Google Scholar] [CrossRef]
- Lavados, M.; Guillón, M.; Mujica, M.C.; Rojo, L.E.; Fuentes, P.; Maccioni, R.B. Mild cognitive impairment and Alzheimer patients display different levels of redox-active CSF iron. J. Alzheimer’s Dis. 2008, 13, 225–232. [Google Scholar] [CrossRef]
- Dong, J.; Robertson, J.D.; Markesbery, W.R.; Lovell, M.A. Serum Zinc in the Progression of Alzheimer’s Disease. J. Alzheimer’s Dis. 2008, 15, 443–450. [Google Scholar] [CrossRef]
- Gerhardsson, L.; Lundh, T.; Minthon, L.; Londos, E. Metal concentrations in plasma and cerebrospinal fluid in patients with Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2008, 25, 508–515. [Google Scholar] [CrossRef]
- Alimonti, A.; Ristori, G.; Giubilei, F.; Stazi, M.A.; Pino, A.; Visconti, A.; Brescianini, S.; Monti, M.S.; Forte, G.; Stanzione, P.; et al. Serum chemical elements and oxidative status in Alzheimer’s disease, Parkinson disease and multiple sclerosis. Neurotoxicology 2007, 28, 450–456. [Google Scholar] [CrossRef]
- Bocca, B.; Forte, G.; Petrucci, F.; Pino, A.; Marchione, F.; Bomboi, G.; Senofonte, O.; Giubilei, F.; Alimonti, A. Monitoring of chemical elements and oxidative damage in patients affected by Alzheimer’s disease. Ann. Ist. Super. Sanita 2005, 41, 197–203. [Google Scholar]
- Smorgon, C.; Mari, E.; Atti, A.R.; Dalla Nora, E.; Zamboni, P.F.; Calzoni, F.; Passaro, A.; Fellin, R. Trace elements and cognitive impairment: An elderly cohort study. Arch. Gerontol. Geriatr. 2004, 38, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Meseguer, I.; Molina, J.A.; Jiménez-Jiménez, F.J.; Aguilar, M.V.; Mateos-Vega, C.J.; González-Muñoz, M.J.; de Bustos, F.; Ortí-Pareja, M.; Zurdo, M.; Berbel, A.; et al. Cerebrospinal fluid levels of selenium in patients with Alzheimer’s disease. J. Neural Transm. 1999, 106, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Snaedal, J.; Kristinsson, J.; Gunnarsdóttir, S.; Ólafsdóttir, Á.; Baldvinsson, M.; Jóhannesson, T. Copper, ceruloplasmin and superoxide dismutase in patients with Alzheimer’s disease. a case-control study. Dement. Geriatr. Cogn. Disord. 1998, 9, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Hock, C.; Drasch, G.; Golombowski, S.; Müller-Spahn, F.; Willershausen-Zönnchen, B.; Schwarz, P.; Hock, U.; Growdon, J.H.; Nitsch, R.M. Increased blood mercury levels in patients with Alzheimer’s disease. J. Neural Transm. 1998, 105, 59–68. [Google Scholar] [CrossRef]
- Molina, J.A.; Jiménez-Jiménez, F.J.; Aguilar, M.V.; Meseguer, I.; Mateos-Vega, C.J.; González-Muñoz, M.J.; de Bustos, F.; Porta, J.; Ortí-Pareja, M.; Zurdo, M.; et al. Cerebrospinal fluid levels of transition metals in patients with Alzheimer’s disease. J. Neural Transm. 1998, 105, 479–488. [Google Scholar] [CrossRef]
- Zapatero, M.D.; Garcia de Jalon, A.; Pascual, F.; Calvo, M.L.; Escanero, J.; Marro, A. Serum aluminum levels in Alzheimer’s disease and other senile dementias. Biol. Trace Elem. Res. 1995, 47, 235–240. [Google Scholar] [CrossRef]
- Basun, H.; Lind, B.; Nordberg, M.; Nordström, M.; Björkstén, K.S.; Winblad, B. Cadmium in blood in Alzheimer’s disease and non-demented subjects: Results from a population-based study. Biometals 1994, 7, 130–134. [Google Scholar] [CrossRef]
- Subhash, M.N.; Padmashree, T.S.; Srinivas, K.N.; Subbakrishna, D.K.; Shankar, S.K. Calcium and phosphorus levels in serum and CSF in dementia. Neurobiol. Aging 1991, 12, 267–269. [Google Scholar] [CrossRef]
- Sahu, R.N.; Pandey, R.S.; Subhash, M.N.; Arya, B.Y.; Padmashree, T.S.; Srinivas, K.N. CSF zinc in Alzheimer’s type dementia. Biol. Psychiatry 1988, 24, 480–482. [Google Scholar] [CrossRef]
- Hershey, C.O.; Hershey, L.A.; Varnes, A.; Vibhakar, S.D.; Lavin, P.; Strain, W.H. Cerebrospinal fluid trace element content in dementia: Clinical, radiologic, and pathologic correlations. Neurology 1983, 33, 1350–1353. [Google Scholar] [CrossRef]
- Morris, M.C.; Brockman, J.; Schneider, J.A.; Wang, Y.; Bennett, D.A.; Tangney, C.C.; van de Rest, O. Association of Seafood Consumption, Brain Mercury Level, and APOE ε4 Status with Brain Neuropathology in Older Adults. JAMA 2016, 315, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Engstrom, D.R.; Fitzgerald, W.F.; Cooke, C.A.; Lamborg, C.H.; Drevnick, P.E.; Swain, E.B.; Balogh, S.J.; Balcom, P.H. Atmospheric Hg emissions from preindustrial gold and silver extraction in the Americas: A reevaluation from lake-sediment archives. Environ. Sci. Technol. 2014, 48, 6533–6543. [Google Scholar] [CrossRef] [PubMed]
- Mutter, J.; Curth, A.; Naumann, J.; Deth, R.; Walach, H. Does inorganic mercury play a role in Alzheimer’s disease? A systematic review and an integrated molecular mechanism. J. Alzheimer’s Dis. 2010, 22, 357–374. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Zhang, W.; Liu, X.; Zhang, C.; Wang, P.; Zhao, X. Circulatory Levels of Toxic Metals (Aluminum, Cadmium, Mercury, Lead) in Patients with Alzheimer’s Disease: A Quantitative Meta-Analysis and Systematic Review. J. Alzheimer’s Dis. 2018, 62, 361–372. [Google Scholar] [CrossRef]
- Olayinka, O.; Olayinka, O.O.; Alemu, B.T.; Akpinar-Elci, M.; Grossberg, G.T. Toxic Environmental Risk Factors for Alzheimer’s Disease: A Systematic Review. Aging Med. Healthc. 2019, 10, 4–17. [Google Scholar] [CrossRef]
- Alattia, J.-R.; Kuraishi, T.; Dimitrov, M.; Chang, I.; Lemaitre, B.; Fraering, P.C. Mercury is a direct and potent γ-secretase inhibitor affecting Notch processing and development in Drosophila. FASEB J. 2011, 25, 2287–2295. [Google Scholar] [CrossRef]
- Olivieri, G.; Brack, C.; Müller-Spahn, F.; Stähelin, H.B.; Herrmann, M.; Renard, P.; Brockhaus, M.; Hock, C. Mercury induces cell cytotoxicity and oxidative stress and increases beta-amyloid secretion and tau phosphorylation in SHSY5Y neuroblastoma cells. J. Neurochem. 2000, 74, 231–236. [Google Scholar] [CrossRef]
- Fujimura, M.; Usuki, F.; Sawada, M.; Takashima, A. Methylmercury induces neuropathological changes with tau hyperphosphorylation mainly through the activation of the c-jun-N-terminal kinase pathway in the cerebral cortex, but not in the hippocampus of the mouse brain. Neurotoxicology 2009, 30, 1000–1007. [Google Scholar] [CrossRef]
- Yang, D.-J.; Shi, S.; Zheng, L.-F.; Yao, T.-M.; Ji, L.-N. Mercury(II) promotes the in vitro aggregation of tau fragment corresponding to the second repeat of microtubule-binding domain: Coordination and conformational transition. Biopolymers 2010, 93, 1100–1107. [Google Scholar] [CrossRef]
- Yin, X.; Sun, J.; Mei, Y.; Guo, X.; Chen, S.-I.; Wang, Z.-I.; Yang, L. Effect of Hg2+ on voltage-dependent calcium channels and intracellular free calcium in trigeminal ganglion neurons of rats. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2008, 26, 542–545. [Google Scholar]
- Weisskopf, M.G.; Wright, R.O.; Schwartz, J.; Spiro, A.; Sparrow, D.; Aro, A.; Hu, H. Cumulative lead exposure and prospective change in cognition among elderly men: The VA Normative Aging Study. Am. J. Epidemiol. 2004, 160, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.O.; Tsaih, S.W.; Schwartz, J.; Spiro, A.; McDonald, K.; Weiss, S.T.; Hu, H. Lead exposure biomarkers and mini-mental status exam scores in older men. Epidemiology 2003, 14, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Gu, H.; Wei, X.; Monnot, A.D.; Fontanilla, C.V.; Behl, M.; Farlow, M.R.; Zheng, W.; Du, Y. Lead exposure increases levels of β-amyloid in the brain and CSF and inhibits LRP1 expression in APP transgenic mice. Neurosci. Lett. 2011, 490, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Bihaqi, S.W.; Eid, A.; Zawia, N.H. Lead exposure and tau hyperphosphorylation: An in vitro study. Neurotoxicology 2017, 62, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Bakulski, K.M.; Rozek, L.S.; Dolinoy, D.C.; Paulson, H.L.; Hu, H. Alzheimer’s disease and environmental exposure to lead: The epidemiologic evidence and potential role of epigenetics. Curr. Alzheimer Res. 2012, 9, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, J.; Xu, Y. Epigenetic Basis of Lead-Induced Neurological Disorders. Int. J. Environ. Res. Public Health 2020, 17, 4878. [Google Scholar] [CrossRef]
- Andrade, V.M.; Aschner, M.; Marreilha dos Santos, A.P. Neurotoxicity of Metal Mixtures. Adv. Neurobiol. 2017, 18, 227–265. [Google Scholar] [CrossRef]
- Patra, R.C.; Rautray, A.K.; Swarup, D. Oxidative Stress in Lead and Cadmium Toxicity and Its Amelioration. Vet. Med. Int. 2011, 2011, 457327. [Google Scholar] [CrossRef]
- Li, C.; Zhang, Y.; Liang, J.; Wu, C.; Zou, X. Assessing the Association Between Lead Pollution and Risk of Alzheimer’s Disease by Integrating Multigenomics. Front. Neurosci. 2022, 16, 880105. [Google Scholar] [CrossRef]
- Masten, S.; Carson, B.L. Aluminum Compounds Review of Toxicological Literature Abridged Final Report; Integrated Laboratory Systems: Morrisville, NC, USA, 2000. [Google Scholar]
- Exley, C.; Mold, M.J. The binding, transport and fate of aluminium in biological cells. J. Trace Elem. Med. Biol. 2015, 30, 90–95. [Google Scholar] [CrossRef]
- Exley, C.; Mold, M.J. Aluminium in human brain tissue: How much is too much? J. Biol. Inorg. Chem. 2019, 24, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Exley, C.; Mold, M.J. Imaging of aluminium and amyloid β in neurodegenerative disease. Heliyon 2020, 6, e03839. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.R. Brain lesions comprised of aluminum-rich cells that lack microtubules may be associated with the cognitive deficit of Alzheimer’s disease. Neurotoxicology 2009, 30, 1059–1069. [Google Scholar] [CrossRef]
- Walton, J.R. Aluminum in hippocampal neurons from humans with Alzheimer’s disease. Neurotoxicology 2006, 27, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Mold, M.; Linhart, C.; Gómez-Ramírez, J.; Villegas-Lanau, A.; Exley, C. Aluminum and Amyloid-β in Familial Alzheimer’s Disease. J. Alzheimers. Dis. 2020, 73, 1627–1635. [Google Scholar] [CrossRef]
- Lopera, F.; Ardilla, A.; Martínez, A.; Madrigal, L.; Arango-Viana, J.C.; Lemere, C.A.; Arango-Lasprilla, J.C.; Hincapié, L.; Arcos-Burgos, M.; Ossa, J.E.; et al. Clinical Features of Early-Onset Alzheimer Disease in a Large Kindred with an E280A Presenilin-1 Mutation. JAMA 1997, 277, 793–799. [Google Scholar] [CrossRef]
- Díaz-Nido, J.; Avila, J. Aluminum induces the in vitro aggregation of bovine brain cytoskeletal proteins. Neurosci. Lett. 1990, 110, 221–226. [Google Scholar] [CrossRef]
- Mirza, A.; King, A.; Troakes, C.; Exley, C. Aluminium in brain tissue in familial Alzheimer’s disease. J. Trace Elem. Med. Biol. 2017, 40, 30–36. [Google Scholar] [CrossRef]
- Mold, M.J.; O’Farrell, A.; Morris, B.; Exley, C. Aluminum and Tau in Neurofibrillary Tangles in Familial Alzheimer’s Disease. J. Alzheimer’s Dis. Rep. 2021, 5, 283. [Google Scholar] [CrossRef]
- Mold, M.J.; O’Farrell, A.; Morris, B.; Exley, C. Aluminum and Neurofibrillary Tangle Co-Localization in Familial Alzheimer’s Disease and Related Neurological Disorders. J. Alzheimer’s Dis. 2020, 78, 139. [Google Scholar] [CrossRef]
- Flaten, T.P. Aluminium as a risk factor in Alzheimer’s disease, with emphasis on drinking water. Brain Res. Bull. 2001, 55, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Martyn, C.N.; Osmond, C.; Edwardson, J.A.; Barker, D.J.P.; Harris, E.C.; Lacey, R.F. Geographical relation between Alzheimer’s disease and aluminum in drinking water. Lancet 1989, 333, 59–62. [Google Scholar] [CrossRef]
- Luo, J.; Su, L.; He, X.; Du, Y.; Xu, N.; Wu, R.; Zhu, Y.; Wang, T.; Shao, R.; Unverzagt, F.W.; et al. Blood Selenium and Serum Glutathione Peroxidase Levels Were Associated with Serum β-Amyloid in Older Adults. Biol. Trace Elem. Res. 2022, 200, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.Z.; Wang, Z.X.; Wang, Z.T.; Hou, X.H.; Shen, X.N.; Ou, Y.N.; Dong, Q.; Tan, L.; Yu, J.T. Serum Calcium Predicts Cognitive Decline and Clinical Progression of Alzheimer’s Disease. Neurotox. Res. 2021, 39, 609–617. [Google Scholar] [CrossRef]
- Mohammed, R.S.; Ibrahim, W.; Sabry, D.; El-Jaafary, S.I. Occupational metals exposure and cognitive performance among foundry workers using tau protein as a biomarker. Neurotoxicology 2020, 76, 10–16. [Google Scholar] [CrossRef]
- Shams, M.; Martola, J.; Charidimou, A.; Granberg, T.; Ferreira, D.; Westman, E.; Wintermark, M.; Iv, M.; Larvie, M.; Kristoffersen Wiberg, M.; et al. Cerebrospinal Fluid Metals and the Association with Cerebral Small Vessel Disease. J. Alzheimer’s Dis. 2020, 78, 1229–1236. [Google Scholar] [CrossRef]
- Vinceti, M.; Chiari, A.; Eichmüller, M.; Rothman, K.J.; Filippini, T.; Malagoli, C.; Weuve, J.; Tondelli, M.; Zamboni, G.; Nichelli, P.F.; et al. A selenium species in cerebrospinal fluid predicts conversion to Alzheimer’s dementia in persons with mild cognitive impairment. Alzheimers. Res. Ther. 2017, 9, 100. [Google Scholar] [CrossRef]
- Krishnan, S.; Rani, P. Evaluation of selenium, redox status and their association with plasma amyloid/tau in Alzheimer’s disease. Biol. Trace Elem. Res. 2014, 158, 158–165. [Google Scholar] [CrossRef]
- Tong, Y.; Yang, H.; Tian, X.; Wang, H.; Zhou, T.; Zhang, S.; Yu, J.; Zhang, T.; Fan, D.; Guo, X.; et al. High manganese, a risk for Alzheimer’s disease: High manganese induces amyloid-β related cognitive impairment. J. Alzheimer’s Dis. 2014, 42, 865–878. [Google Scholar] [CrossRef]
- Gerhardsson, L.; Blennow, K.; Lundh, T.; Londos, E.; Minthon, L. Concentrations of metals, beta-amyloid and tau-markers in cerebrospinal fluid in patients with Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2009, 28, 88–94. [Google Scholar] [CrossRef]
- Strozyk, D.; Launer, L.J.; Adlard, P.A.; Cherny, R.A.; Tsatsanis, A.; Volitakis, I.; Blennow, K.; Petrovitch, H.; White, L.R.; Bush, A.I. Zinc and copper modulate Alzheimer Abeta levels in human cerebrospinal fluid. Neurobiol. Aging 2009, 30, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Kessler, H.; Pajonk, F.G.; Bach, D.; Schneider-Axmann, T.; Falkai, P.; Herrmann, W.; Multhaup, G.; Wiltfang, J.; Schäfer, S.; Wirths, O.; et al. Effect of copper intake on CSF parameters in patients with mild Alzheimer’s disease: A pilot phase 2 clinical trial. J. Neural Transm. 2008, 115, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Mielke, M.M.; Zandi, P.P.; Blennow, K.; Gustafson, D.; Sjögren, M.; Rosengren, L.; Skoog, I. Low serum potassium in mid life associated with decreased cerebrospinal fluid Abeta42 in late life. Alzheimer Dis. Assoc. Disord. 2006, 20, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Squitti, R.; Barbati, G.; Rossi, L.; Ventriglia, M.; Dal Forno, G.; Cesaretti, S.; Moffa, F.; Caridi, I.; Cassetta, E.; Pasqualetti, P.; et al. Excess of nonceruloplasmin serum copper in AD correlates with MMSE, CSF beta-amyloid, and h-tau. Neurology 2006, 67, 76–82. [Google Scholar] [CrossRef]
- Jia, M.; Haldar, S.; Khan, M.A.; Sharma, S.D.; Merrick, W.C.; Theil, E.C.; Goss, D.J. Fe2+ binds iron responsive element-RNA, selectively changing protein-binding affinities and regulating mRNA repression and activation. Proc. Natl. Acad. Sci. USA 2012, 109, 8417–8422. [Google Scholar] [CrossRef]
- Pfeifhofer-Obermair, C.; Tymoszuk, P.; Nairz, M.; Schroll, A.; Klais, G.; Demetz, E.; Engl, S.; Brigo, N.; Weiss, G. Regulation of Th1 T Cell Differentiation by Iron via Upregulation of T Cell Immunoglobulin and Mucin Containing Protein-3 (TIM-3). Front. Immunol. 2021, 12, 637809. [Google Scholar] [CrossRef]
- Pourcelot, E.; Lénon, M.; Mobilia, N.; Cahn, J.Y.; Arnaud, J.; Fanchon, E.; Moulis, J.M.; Mossuz, P. Iron for proliferation of cell lines and hematopoietic progenitors: Nailing down the intracellular functional iron concentration. Biochim. Biophys. Acta -Mol. Cell Res. 2015, 1853, 1596–1605. [Google Scholar] [CrossRef]
- Andreini, C.; Putignano, V.; Rosato, A.; Banci, L. The human iron-proteome. Metallomics 2018, 10, 1223–1231. [Google Scholar] [CrossRef]
- Hirota, K. An intimate crosstalk between iron homeostasis and oxygen metabolism regulated by the hypoxia-inducible factors (HIFs). Free Radic. Biol. Med. 2019, 133, 118–129. [Google Scholar] [CrossRef]
- Schulz, K.; Kroner, A.; David, S. Iron efflux from astrocytes plays a role in remyelination. J. Neurosci. 2012, 32, 4841–4847. [Google Scholar] [CrossRef]
- Beard, J. Iron deficiency alters brain development and functioning. J. Nutr. 2003, 133, 1468S–1472S. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, K.N. Iron and the brain: Neurotransmitter receptors and magnetic resonance spectroscopy. Br. J. Nutr. 2001, 85 (Suppl. S2), S147–S150. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.A.; Harris, P.L.; Sayre, L.M.; Perry, G. Iron accumulation in Alzheimer disease is a source of redox-generated free radicals. Proc. Natl. Acad. Sci. USA 1997, 94, 9866–9868. [Google Scholar] [CrossRef] [PubMed]
- Mantyh, P.W.; Ghilardi, J.R.; Rogers, S.; DeMaster, E.; Allen, C.J.; Stimson, E.R.; Maggio, J.E. Aluminum, iron, and zinc ions promote aggregation of physiological concentrations of beta-amyloid peptide. J. Neurochem. 1993, 61, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Egaña, J.T.; Zambrano, C.; Nuñez, M.T.; Gonzalez-Billault, C.; Maccioni, R.B. Iron-induced oxidative stress modify tau phosphorylation patterns in hippocampal cell cultures. Biometals 2003, 16, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Lovell, M.A.; Xiong, S.; Xie, C.; Davies, P.; Markesbery, W.R. Induction of hyperphosphorylated tau in primary rat cortical neuron cultures mediated by oxidative stress and glycogen synthase kinase-3. J. Alzheimer’s Dis. 2004, 6, 659–671; discussion 673–681. [Google Scholar] [CrossRef] [PubMed]
- Wan, W.; Cao, L.; Kalionis, B.; Murthi, P.; Xia, S.; Guan, Y. Iron Deposition Leads to Hyperphosphorylation of Tau and Disruption of Insulin Signaling. Front. Neurol. 2019, 10, 607. [Google Scholar] [CrossRef]
- Yamamoto, A.; Shin, R.-W.; Hasegawa, K.; Naiki, H.; Sato, H.; Yoshimasu, F.; Kitamoto, T. Iron (III) induces aggregation of hyperphosphorylated tau and its reduction to iron (II) reverses the aggregation: Implications in the formation of neurofibrillary tangles of Alzheimer’s disease. J. Neurochem. 2002, 82, 1137–1147. [Google Scholar] [CrossRef]
- Wong, B.X.; Tsatsanis, A.; Lim, L.Q.; Adlard, P.A.; Bush, A.I.; Duce, J.A. β-Amyloid precursor protein does not possess ferroxidase activity but does stabilize the cell surface ferrous iron exporter ferroportin. PLoS ONE 2014, 9, e114174. [Google Scholar] [CrossRef]
- Frederickson, C.J. Neurobiology of Zinc and Zinc-Containing Neurons. Int. Rev. Neurobiol. 1989, 31, 145–238. [Google Scholar] [CrossRef]
- Takeda, A.; Takada, S.; Ando, M.; Itagaki, K.; Tamano, H.; Suzuki, M.; Iwaki, H.; Oku, N. Impairment of recognition memory and hippocampal long-term potentiation after acute exposure to clioquinol. Neuroscience 2010, 171, 443–450. [Google Scholar] [CrossRef]
- Bush, A.I.; Pettingell, W.H.; de Paradis, M.; Tanzi, R.E.; Wasco, W. The amyloid beta-protein precursor and its mammalian homologues. Evidence for a zinc-modulated heparin-binding superfamily. J. Biol. Chem. 1994, 269, 26618–26621. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.-Y.; Zhu, Y.-Z.; Zhu, H.-L.; Fan, J.-B.; Chen, J.; Liang, Y. Low micromolar zinc accelerates the fibrillization of human tau via bridging of Cys-291 and Cys-322. J. Biol. Chem. 2009, 284, 34648–34657. [Google Scholar] [CrossRef] [PubMed]
- An, W.-L.; Bjorkdahl, C.; Liu, R.; Cowburn, R.F.; Winblad, B.; Pei, J.-J. Mechanism of zinc-induced phosphorylation of p70 S6 kinase and glycogen synthase kinase 3beta in SH-SY5Y neuroblastoma cells. J. Neurochem. 2005, 92, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Pei, J.-J.; An, W.-L.; Zhou, X.-W.; Nishimura, T.; Norberg, J.; Benedikz, E.; Götz, J.; Winblad, B. P70 S6 kinase mediates tau phosphorylation and synthesis. FEBS Lett. 2006, 580, 107–114. [Google Scholar] [CrossRef]
- Meng, L.; Wang, Z.; Ming, Y.C.; Shen, L.; Ji, H.F. Are micronutrient levels and supplements causally associated with the risk of Alzheimer’s disease? A two-sample Mendelian randomization analysis. Food Funct. 2022, 13, 6665–6673. [Google Scholar] [CrossRef]
- Wang, Z.; Meng, L.; Shen, L.; Ji, H.F. Impact of modifiable risk factors on Alzheimer’s disease: A two-sample Mendelian randomization study. Neurobiol. Aging 2020, 91, 167.e11–167.e19. [Google Scholar] [CrossRef]
- Cheng, W.W.; Zhu, Q.; Zhang, H.Y. Mineral Nutrition and the Risk of Chronic Diseases: A Mendelian Randomization Study. Nutrients 2019, 11, 378. [Google Scholar] [CrossRef]
- Corona, C.; Masciopinto, F.; Silvestri, E.; Del Viscovo, A.; Lattanzio, R.; La Sorda, R.; Ciavardelli, D.; Goglia, F.; Piantelli, M.; Canzoniero, L.M.T.; et al. Dietary zinc supplementation of 3xTg-AD mice increases BDNF levels and prevents cognitive deficits as well as mitochondrial dysfunction. Cell Death Dis. 2010, 1, e91. [Google Scholar] [CrossRef]
- Brewer, G.J. Copper excess, zinc deficiency, and cognition loss in Alzheimer’s disease. Biofactors 2012, 38, 107–113. [Google Scholar] [CrossRef]
- Brewer, G.J. Alzheimer’s disease causation by copper toxicity and treatment with zinc. Front. Aging Neurosci. 2014, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; von Stillfried, N.; Walach, H. Zinc diet and Alzheimer’s disease: A systematic review. Nutr. Neurosci. 2012, 15, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Craven, K.M.; Kochen, W.R.; Hernandez, C.M.; Flinn, J.M. Zinc Exacerbates Tau Pathology in a Tau Mouse Model. J. Alzheimers. Dis. 2018, 64, 617–630. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Wang, T.; Zheng, W.; Zhao, B.L.; Danscher, G.; Chen, Y.H.; Wang, Z.Y. Zinc overload enhances APP cleavage and Aβ deposition in the Alzheimer mouse brain. PLoS ONE 2010, 5, e15349. [Google Scholar] [CrossRef] [PubMed]
- Kodama, H.; Murata, Y.; Kobayashi, M. Clinical manifestations and treatment of Menkes disease and its variants. Pediatr. Int. 1999, 41, 423–429. [Google Scholar] [CrossRef]
- Merle, U.; Schaefer, M.; Ferenci, P.; Stremmel, W. Clinical presentation, diagnosis and long-term outcome of Wilson’s disease: A cohort study. Gut 2007, 56, 115–120. [Google Scholar] [CrossRef]
- Žigman, T.; Petković Ramadža, D.; Šimić, G.; Barić, I. Inborn Errors of Metabolism Associated with Autism Spectrum Disorders: Approaches to Intervention. Front. Neurosci. 2021, 15, 624. [Google Scholar] [CrossRef]
- You, H.; Tsutsui, S.; Hameed, S.; Kannanayakal, T.J.; Chen, L.; Xia, P.; Engbers, J.D.T.; Lipton, S.A.; Stys, P.K.; Zamponi, G.W. Aβ neurotoxicity depends on interactions between copper ions, prion protein, and N-methyl-D-aspartate receptors. Proc. Natl. Acad. Sci. USA 2012, 109, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Lovell, M.A.; Robertson, J.D.; Teesdale, W.J.; Campbell, J.L.; Markesbery, W.R. Copper, iron and zinc in Alzheimer’s disease senile plaques. J. Neurol. Sci. 1998, 158, 47–52. [Google Scholar] [CrossRef]
- Ayton, S.; Lei, P.; Bush, A.I. Metallostasis in Alzheimer’s disease. Free Radic. Biol. Med. 2013, 62, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Miyata, M.; Smith, J.D. Apolipoprotein E allele-specific antioxidant activity and effects on cytotoxicity by oxidative insults and β-amyloid peptides. Nat. Genet. 1996, 14, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Moir, R.D.; Atwood, C.S.; Romano, D.M.; Laurans, M.H.; Huang, X.; Bush, A.I.; Smith, J.D.; Tanzi, R.E. Differential effects of apolipoprotein E isoforms on metal-induced aggregation of A beta using physiological concentrations. Biochemistry 1999, 38, 4595–4603. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, E.M.; Vivar, C.; Camandola, S. Physiology and Pathology of Calcium Signaling in the Brain. Front. Pharmacol. 2012, 3, 61. [Google Scholar] [CrossRef] [PubMed]
- Woods, N.K.; Padmanabhan, J. Neuronal Calcium Signaling and Alzheimer’s Disease. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 1193–1217. [Google Scholar]
- Olney, J.W. Brain lesions, obesity, and other disturbances in mice treated with monosodium glutamate. Science 1969, 164, 719–721. [Google Scholar] [CrossRef]
- Sattler, R.; Tymianski, M. Molecular Mechanisms of Glutamate Receptor-Mediated Excitotoxic Neuronal Cell Death. Mol. Neurobiol. 2001, 24, 107–130. [Google Scholar] [CrossRef]
- Tong, B.C.K.; Wu, A.J.; Li, M.; Cheung, K.H. Calcium signaling in Alzheimer’s disease & therapies. Biochim. Biophys. Acta -Mol. Cell Res. 2018, 1865, 1745–1760. [Google Scholar]
- Sato, K.; Mano, T.; Ihara, R.; Suzuki, K.; Tomita, N.; Arai, H.; Ishii, K.; Senda, M.; Ito, K.; Ikeuchi, T.; et al. Lower Serum Calcium as a Potentially Associated Factor for Conversion of Mild Cognitive Impairment to Early Alzheimer’s Disease in the Japanese Alzheimer’s Disease Neuroimaging Initiative. J. Alzheimer’s Dis. 2019, 68, 777–788. [Google Scholar] [CrossRef]
- Shi, Y.; Liu, R.; Guo, Y.; Li, Q.; Zhou, H.; Yu, S.; Liang, H.; Li, Z. An Updated Mendelian Randomization Analysis of the Association Between Serum Calcium Levels and the Risk of Alzheimer’s Disease. Front. Genet. 2021, 12, 1602. [Google Scholar] [CrossRef]
- Kern, J.; Kern, S.; Blennow, K.; Zetterberg, H.; Waern, M.; Guo, X.; Börjesson-Hanson, A.; Skoog, I.; Östling, S. Calcium supplementation and risk of dementia in women with cerebrovascular disease. Neurology 2016, 87, 1674–1680. [Google Scholar] [CrossRef]
- He, Y.; Zhang, H.; Wang, T.; Han, Z.; Ni, Q.B.; Wang, K.; Wang, L.; Zhang, Y.; Hu, Y.; Jin, S.; et al. Impact of Serum Calcium Levels on Alzheimer’s Disease: A Mendelian Randomization Study. J. Alzheimer’s Dis. 2020, 76, 713–724. [Google Scholar] [CrossRef]
- Li, L.; Yang, X. The Essential Element Manganese, Oxidative Stress, and Metabolic Diseases: Links and Interactions. Oxid. Med. Cell. Longev. 2018, 2018, 7580707. [Google Scholar] [CrossRef] [PubMed]
- Rolle-McFarland, D.; Liu, Y.; Mostafaei, F.; Zauber, S.E.; Zhou, Y.; Li, Y.; Fan, Q.; Zheng, W.; Nie, L.H.; Wells, E.M. The association of bone, fingernail and blood manganese with cognitive and olfactory function in Chinese workers. Sci. Total Environ. 2019, 666, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Barahona, A.J.; Bursac, Z.; Veledar, E.; Lucchini, R.; Tieu, K.; Richardson, J.R. Relationship of Blood and Urinary Manganese Levels with Cognitive Function in Elderly Individuals in the United States by Race/Ethnicity, NHANES 2011-2014. Toxics 2022, 10, 191. [Google Scholar] [CrossRef] [PubMed]
- Bardgett, M.E.; Schultheis, P.J.; McGill, D.L.; Richmond, R.E.; Wagge, J.R. Magnesium deficiency impairs fear conditioning in mice. Brain Res. 2005, 1038, 100–106. [Google Scholar] [CrossRef]
- Cherbuin, N.; Kumar, R.; Sachdev, P.S.; Anstey, K.J. Dietary Mineral Intake and Risk of Mild Cognitive Impairment: The PATH through Life Project. Front. Aging Neurosci. 2014, 6, 4. [Google Scholar] [CrossRef]
- Glick, J. Use of magnesium in the management of dementias. Med. Sci. Res. 1990, 18, 831–833. [Google Scholar]
- Ozturk, S.; Cillier, A.E. Magnesium supplementation in the treatment of dementia patients. Med. Hypotheses 2006, 67, 1223–1225. [Google Scholar] [CrossRef]
- Andrási, E.; Igaz, S.; Molnár, Z.; Makó, S. Disturbances of magnesium concentrations in various brain areas in Alzheimer’s disease. Magnes. Res. 2000, 13, 189–196. [Google Scholar]
- Vural, H.; Demirin, H.; Kara, Y.; Eren, I.; Delibas, N. Alterations of plasma magnesium, copper, zinc, iron and selenium concentrations and some related erythrocyte antioxidant enzyme activities in patients with Alzheimer’s disease. J. Trace Elem. Med. Biol. 2010, 24, 169–173. [Google Scholar] [CrossRef]
- Cilliers, K. Trace element alterations in Alzheimer’s disease: A review. Clin. Anat. 2021, 34, 766–773. [Google Scholar] [CrossRef]
- Yu, J.; Sun, M.; Chen, Z.; Lu, J.; Liu, Y.; Zhou, L.; Xu, X.; Fan, D.; Chui, D. Magnesium modulates amyloid-beta protein precursor trafficking and processing. J. Alzheimer’s Dis. 2010, 20, 1091–1106. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.-P.; Li, L.; Bao, J.; Wang, Z.-H.; Zeng, J.; Liu, E.-J.; Li, X.-G.; Huang, R.-X.; Gao, D.; Li, M.-Z.; et al. Magnesium Protects Cognitive Functions and Synaptic Plasticity in Streptozotocin-Induced Sporadic Alzheimer’s Model. PLoS ONE 2014, 9, e108645. [Google Scholar] [CrossRef] [PubMed]
- Faraco, G.; Hochrainer, K.; Segarra, S.G.; Schaeffer, S.; Santisteban, M.M.; Menon, A.; Jiang, H.; Holtzman, D.M.; Anrather, J.; Iadecola, C. Dietary salt promotes cognitive impairment through tau phosphorylation. Nature 2019, 574, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.A.; Herrmann, K.; Adlung, A.; Paschke, N.; Hausner, L.; Frölich, L.; Schad, L.; Groden, C.; Ulrich, H.K. Evaluation of Sodium (23 Na) MR-imaging as a Biomarker and Predictor for Neurodegenerative Changes in Patients with Alzheimer’s Disease. In Vivo 2021, 35, 429–435. [Google Scholar] [CrossRef]
- Zheng, F.; Li, Y.; Zhang, F.; Sun, Y.; Zheng, C.; Luo, Z.; Wang, Y.L.; Aschner, M.; Zheng, H.; Lin, L.; et al. Cobalt induces neurodegenerative damages through Pin1 inactivation in mice and human neuroglioma cells. J. Hazard. Mater. 2021, 419, 126378. [Google Scholar] [CrossRef]
- Adlard, P.A.; Bush, A.I. Metals and Alzheimer’s Disease: How Far Have We Come in the Clinic? J. Alzheimer’s Dis. 2018, 62, 1369. [Google Scholar] [CrossRef]
- Kessler, H.; Bayer, T.A.; Bach, D.; Schneider-Axmann, T.; Supprian, T.; Herrmann, W.; Haber, M.; Multhaup, G.; Falkai, P.; Pajonk, F.G. Intake of copper has no effect on cognition in patients with mild Alzheimer’s disease: A pilot phase 2 clinical trial. J. Neural Transm. 2008, 115, 1181. [Google Scholar] [CrossRef]
- Chen, L.L.; Fan, Y.G.; Zhao, L.X.; Zhang, Q.; Wang, Z.Y. The metal ion hypothesis of Alzheimer’s disease and the anti-neuroinflammatory effect of metal chelators. Bioorg. Chem. 2023, 131, 106301. [Google Scholar] [CrossRef]
- Cherny, R.A.; Atwood, C.S.; Xilinas, M.E.; Gray, D.N.; Jones, W.D.; McLean, C.A.; Barnham, K.J.; Volitakis, I.; Fraser, F.W.; Kim, Y.S.; et al. Treatment with a copper-zinc chelator markedly and rapidly inhibits beta-amyloid accumulation in Alzheimer’s disease transgenic mice. Neuron 2001, 30, 665–676. [Google Scholar] [CrossRef]
- Ritchie, C.W.; Bush, A.I.; Mackinnon, A.; Macfarlane, S.; Mastwyk, M.; MacGregor, L.; Kiers, L.; Cherny, R.; Li, Q.-X.; Tammer, A.; et al. Metal-protein attenuation with iodochlorhydroxyquin (clioquinol) targeting Abeta amyloid deposition and toxicity in Alzheimer disease: A pilot phase 2 clinical trial. Arch. Neurol. 2003, 60, 1685–1691. [Google Scholar] [CrossRef]
- White, A.R.; Du, T.; Laughton, K.M.; Volitakis, I.; Sharples, R.A.; Xilinas, M.E.; Hoke, D.E.; Holsinger, R.M.D.; Evin, G.; Cherny, R.A.; et al. Degradation of the Alzheimer disease amyloid beta-peptide by metal-dependent up-regulation of metalloprotease activity. J. Biol. Chem. 2006, 281, 17670–17680. [Google Scholar] [CrossRef] [PubMed]
- Lannfelt, L.; Blennow, K.; Zetterberg, H.; Batsman, S.; Ames, D.; Harrison, J.; Masters, C.L.; Targum, S.; Bush, A.I.; Murdoch, R.; et al. Safety, efficacy, and biomarker findings of PBT2 in targeting Abeta as a modifying therapy for Alzheimer’s disease: A phase IIa, double-blind, randomised, placebo-controlled trial. Lancet. Neurol. 2008, 7, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Summers, K.L.; Roseman, G.; Schilling, K.M.; Dolgova, N.V.; Pushie, M.J.; Sokaras, D.; Kroll, T.; Harris, H.H.; Millhauser, G.L.; Pickering, I.J.; et al. Alzheimer’s Drug PBT2 Interacts with the Amyloid β 1–42 Peptide Differently than Other 8-Hydroxyquinoline Chelating Drugs. Inorg. Chem. 2022, 61, 14626–14640. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.J.; Gray, N.E.; Caruso, M.; Hunter, M.; Ralle, M.; Quinn, J.F. Copper Modulation and Memory Impairment due to Hippocampal Tau Pathology. J. Alzheimers. Dis. 2020, 78, 49–60. [Google Scholar] [CrossRef]
- Drew, S.C. The Case for Abandoning Therapeutic Chelation of Copper Ions in Alzheimer’s Disease. Front. Neurosci. 2017, 11, 317. [Google Scholar] [CrossRef]
- Pingault, J.B.; O’Reilly, P.F.; Schoeler, T.; Ploubidis, G.B.; Rijsdijk, F.; Dudbridge, F. Using genetic data to strengthen causal inference in observational research. Nat. Rev. Genet. 2018, 19, 566–580. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Analyzed Bodily Fluid | Method Used | Measured Metals | Classification of Participants (Number of Patients) | Number of Participants | Metals in AD Patients versus HC |
|---|---|---|---|---|---|---|
| [74] | CSF and plasma | ICP-MS | In CSF and plasma: As, B, Ca, Cd, Co, Cu, Fe, Hg, Li, Mg, Mn, Mo, Na, Ni, P, Pb, S, Se, Sr, Tl, Zn In CSF: Al, Ba, K | CSF: AD (124), MCI (50), HC (19) Plasma: AD (93), MCI (35), HC (15) | CSF: 193 Plasma: 143 | In CSF: Zn↑ (p = 0.024), Al↓ (p = 0.003), P↑ (p = 0.029) In plasma: Na↑ (p = 0.004) |
| [87] | Bodily fluids | Meta-analysis | Cu, Fe, Zn, Se, Mn, Pb, Al, Cd, Cr, As, Hg, Co | In serum: Cu↑ (SMD [95% CI]); 0.37 (0.1, 0.65) In plasma: Fe↓ −0.68 (−1.34, −0.02), Se↓ −0.61 (−0.97, −0.25) In hair: Zn↓ −0.35 (−0.62, −0.08) | ||
| [88] | Serum | Al, Co, Cd, Cr, Cu, Fe, Mg, Mn, Se, Zn | Elderly with and without cognitive dysfunction | 191 | Cu↑ in elderly with cognitive dysfunction | |
| [73] | Urine and blood | ICP-MS | In urine: As In blood: Cr and Se | AD (53), HC (217) | 270 | As↑ (p = 0.023), Cr↑ (p = 0.005), Se↓ (p = 0.001) |
| [89] | Serum, CSF | Meta-analysis | Mg | Serum and plasma: AD (1112), HC (1001) CSF: AD (284), HC (117) | In serum and plasma: Mg↓ (SMD [95% CI]); −0.89 (−1.36, −0.43) | |
| [90] | CSF | ICP-MS | Fe, Ni, Cr, Zn, Mn, Co, Cu | AD (20), CAA (10), HC (10) | 40 | No difference |
| [27] | CSF and plasma | ICP-MS | Cu, Zn, Fe, Na, Mg, Ca, Co, Mo, Mn, B | CSF: AD (126), MCI (52), HC (19) Plasma: AD (93), MCI (37), HC (14) | CSF: 197 Plasma: 144 | In CSF: Zn↑ (p = 0.027) In plasma: Na↑ (p = 0.004) |
| [72] | Hair and nail samples | ICP-MS | As, Se | AD (40), HC (40) | 80 | In hair and nail samples: As↑ (p < 0.001), Se↑ (p < 0.001) |
| [86] | Blood and serum | ICP-OES | In blood: Cd, Hg, Al, Pb, As In serum: Zn, Cu, Fe | AD (50), HC (50) | 100 | Cd↑ (p < 0.001), Hg↑ (p < 0.001), Al↑ (p = 0.009), Cu↑ (p = 0.025), Fe↓ (p = 0.030), Zn↓ (p < 0.001) |
| [91] | Serum | AAS | Cu, Zn, Se | AD (110), HC (60) | 170 | Se↓ (p < 0.05), Zn↓ (p < 0.001), Cu/Se↑ (p < 0.001) |
| [92] | Serum, plasma, and brain | Meta-analysis | Cu | In serum/plasma: AD (2929), HC (3547) In brain: AD (182), HC (166) | In brain: Cu↓ (SMD [95% CI]); −0.74 (−1.05, −0.43) In serum/plasma: Cu↑ 0.66 (0.34, 0.97) | |
| [93] | CSF | GF-AAS | Fe | AD (16), MCI (17), FTD (22), HC (14) | 69 | Fe↑ (p < 0.001) |
| [94] | Plasma, erythrocytes | GF-AAS | Se | AD (34), HC (68) | 102 | Se↓ (in plasma and erythrocytes) (p < 0.001) |
| [95] | Plasma | Standard hospital assays | Mg | AD (1600), non-AD dementia (855), no dementia (100,193) | 102,648 | Both Mg↓ (multifactorial-adjusted HR [95% CI]; 1.5 [1.21–1.87]) and Mg↑ (1.34 [1.07–1.69]) associated with an increased risk of vascular-related non-AD dementia. There is no correlation observed for AD |
| [96] | CSF and plasma | Flame photometer measurement | Na | At risk for AD (43) | 43 | In CSF: Na↑ in high blood pressure patients at risk for AD (p < 0.01) |
| [97] | Serum | According to a photometric color | Mg | Dementia (2761), HC (42,698) | 45,459 | No difference |
| [98] | Serum | Routinely performed in hospital laboratories | K | AD (105), DLB (78) | 183 | K↑ predicts poorer cognitive prognosis for dementia patients (p = 0.003) |
| [99] | Plasma | ICP-MS | Cu, Zn | AD (95), HC (84) | 179 | No difference |
| [100] | Plasma | Total reflection X-ray fluorescence (TXRF) spectroscopy | Ca, Fe, Zn, Cu, Se, P | AD (44), HC (44) | 88 | Ca↑ (p = 0.025), P↑ (p = 1.33 × 10−12) |
| [101] | Blood (erythrocytes) | ICP-MS | Cu, Fe, Se | AD (32), HC (32) | 64 | Cu↑ (p < 0.001), Fe↑ (p < 0.001) |
| [102] | Serum | Ion-selective electrode method | Na, K | MCI (139), HC (371) | 510 | No difference |
| [62] | Urine and blood | ICP-MS | In blood: Cd, Pb, Hg, Se In urine: As | AD (170), HC (264) | 434 | No difference |
| [103] | Blood | AAS | Pb | AD (27), HC (54) | 81 | Pb↑ (p < 0.001) |
| [104] | CSF | ICP-MS | Ca | AD (45), HC (45) | 90 | No difference |
| [105] | Serum and urine | In serum: AAS In urine: GF-AAS | Cu | AD (385), HC (336), WD (9) | 730 | In serum: Cu↑ (p < 0.001) In urine: Cu↑ (p < 0.001) |
| [106] | Plasma | ICP-MS | Na, K, Ca, Mg, Fe, Zn, Cu, Se | AD (42), HC (43) | 85 | Zn↑ (in males) (p = 0.021) |
| [107] | Plasma | ICP-MS | Li, Mg, Al, Ca, Ti, V, Cr, Ca, Mn, Fe, Co, Ni, Cu, Zn, As, Se, Sr, Mo, Ba, Tl, Pb | AD (92), HC (161) | 253 | Al↑ (p < 0.001), Cu↑ (p < 0.001), Fe↑ (p < 0.001), Li↓ (p < 0.001), Mn↓ (p < 0.001), Zn↓ (p < 0.05) |
| [108] | Serum | Colorimetric endpoint method | Mg | Dementia (823, 662 of them had AD), no dementia (8746) | 9569 | Both Mg↓ (HR [95% CI]; 1.32 [1.02–1.69]) and Mg↑ (1.30 [1.02–1.67]) associated with an increased risk of dementia |
| [109] | Serum | AAS | Mg, Fe, Mn | AD (15), MCI (15), HC (15) | 45 | Mg↓ (p < 0.01), Mn↑ (p < 0.001) |
| [110] | Serum | Meta-analysis | Mn | AD (836), HC (1254) | 2090 | Mn↓ (SMD [95% CI]; −0.39 [−0.71, −0.08]) |
| [111] | Circulatory (plasma/serum and blood), erythrocytes, CSF | Meta-analysis | Se | AD (594), HC (472) | Circulatory: Se↓ (SMD [95% CI]; −0.44 [−0.71, −0.17]) | |
| [112] | Serum | Photoelectric colorimetric assay | Cu, Fe, Zn | AD (125), HC (40) | 165 | Cu↑ (p = 0.014), Fe↑ (p = 0.027), Zn↓ (p = 0.020) |
| [113] | CSF, serum, erythrocytes | SEC-ICP-MS and tandem mass spectrometry | Se | CSF: AD (10), MCI (5), HC (31) Serum: AD (29), MCI (30), HC (30) Erythrocytes: AD (36), HC (39) | CSF: 46 Serum: 89 Erythrocytes: 75 | In erythrocytes: Se↓ (p < 0.05) |
| [114] | Plasma | AAS | Se | AD (11), MCI (17), HC (12) | 40 | Se↓ (in AD, p = 0.049 and MCI, p = 0.003) |
| [115] | Brain and circulatory | Meta- analysis | Circulatory: Se Brain: Se, Zn | Circulatory: AD (660), HC (536) Brain: Se—AD (487), HC (353), Zn—AD (496), HC (306) | Circulatory: Se↓ (p < 0.05) Brain: no difference | |
| [116] | Serum, CSF, and post-mortem brain tissue | ICP-MS | K and Rb | For serum: AD (171), MCI (128), HC (778) For CSF: AD (9), MCI (7), HC (36) For brain tissue: AD (30), HC (30) | For serum: 1077 For CSF: 52 For brain tissue: 60 | In serum: K↑ (p < 0.05), Rb↓ (p < 0.001) In brain: K↓ (p < 0.01), Rb↓ (p < 0.001) |
| [117] | Serum | ICP-MS | Al, Sb, As, Be, Cd, Ca, Cr, Co, Cu, Fe, Pb, Hg, Mn, Mo, Ni, Se, Sr, Tl, Sn, U, V, and Zn | AD (34), MCI (20), SMC (24), HC (40) | 118 | Hg↓ (in AD, p < 0.001), Mn↓ (in AD, p < 0.001 and MCI, p = 0.024), Mo↑ (in AD, p = 0.001), Se↓ (in MCI, p = 0.015) |
| [118] | Serum, erythrocytes | ICP-MS | Pb, Mn | AD (206), MCI (129), HC (758) | 1093 | Mn↓ (in serum, p < 0.001) |
| [119] | Plasma | SEC-ICP-MS, solution nebulization (SN)-ICP-MS | Fe | AD (34), HC (36) | 70 | Fe↓ (p = 0.01) |
| [120] | Serum and hair | ICP-MS | Cu, Se, Zn, Mg, Mn, and Fe | AD (45), HC (33) | 78 | In serum: Mn↓ (p = 0.002) In hair: Se↓ (p = 0.005), Zn↓ (p = 0.02), Cu↑ (p = 0.013), Mn↑ (p = 0.009) |
| [121] | Serum | AAS (Cu, Mn) and Biorex diagnostics kit (Zn) | Cu, Mn, Zn | MCI (120), HC (120) | 240 | No difference |
| [122] | Serum | FAAS | Fe, Cu, Zn | AD (83), HC (83) | 166 | Cu↑ (p < 0.001), Fe↓ (p = 0.001) |
| Meta- analysis | For Fe: AD (1084), HC (1319) For Zn: AD (862), HC (1705) For Cu: AD (1768), HC (2514) | Cu↑ (WMD = 10.474, p < 0.001), Zn↓ (WMD = −5.503; p < 0.001) | ||||
| [123] | Serum, plasma, and CSF | Meta- analysis | Zn | For serum: AD (777), HC (1728) For plasma: AD (287), HC (166) For CSF: AD (292), HC (179) | In serum (plus in serum and plasma): Zn↓ (SMD [95% CI]; −0.46 [−0.76, −0.16]) | |
| [124] | Blood | ICP-MS | Cu, Se, Zn, Pb, and Hg | AD (15), MS (41), HC (23), healthy elderly controls (10) | 89 | Pb↓, Cu↓, Zn↓, Se↓ (for all comparisons p < 0.001) |
| [125] | Plasma | ICP-MS | Fe | AD (211), MCI (133), HC (768) | 1112 | Fe↓ (p = 0.049) |
| [126] | Plasma | GF-AAS | Se | AD (79), HC (93) | 172 | Se↓ (p < 0.001) |
| [127] | Serum | ICP-MS | Pb, Cd, Hg, As | AD (89), HC (118) | 207 | No difference |
| [128] | Serum | ICP-MS | Li, Al, V, Cr, Mn, Fe, Co, Cu, Zn, Se, Mo, Cd, and Pb | AD (30), MCI (16), HC (30) | 76 | Mn↓ (in AD and MCI), Al↑ (in AD and MCI), Se↓ (in AD and MCI), Fe↑ (in AD and MCI), Zn↓ (in AD) |
| [129] | Serum and CSF | Meta-analysis | Fe | AD (1813), HC (2401) | 4214 | In serum: Fe↓ (p < 0.001) |
| [130] | Erythrocytes and serum | ICP-MS | Zn | AD (205), MCI (126), HC (753) | 1084 | No difference |
| [131] | Blood and serum | ICP-MS (for Pb and Cd) and Gold amalgamation (for Hg) | Pb, Cd, and Hg | AD (80), HC (130) | 210 | No difference |
| [132] | CSF | ICP-MS | Cu, Fe, Mg, Mn, and Zn | AD (21), PD (20), ALS (52), HC (15) | 108 | Cu↑ (p < 0.01), Zn↑ (p < 0.01) |
| [133] | Serum, plasma, and CSF | Meta-analysis | Cu | Serum: AD (761), HC (664) Plasma: AD (205), HC (167) CSF: AD (116), HC (129) | In serum: Cu↑ (p = 0.001) | |
| [134] | Plasma and CSF | ICP-MS | CSF/plasma quotients of Mg, Ca, Mn, Fe, Co, Ni, Cu, Zn, Se, Rb, Sr, Mo, Cd, Sn, Sb, Cs, Hg, and Pb | AD (264), HC (54) | 318 | CSF/plasma quotients of Mn↓ (p < 0.001), Rb↓ (p = 0.002), Sb↓ (p = 0.003), Pb↓ (p = 0.001), Hg↓ (p = 0.001), Co↑ (p < 0.001) |
| [135] | Serum | ICP-MS | Al, As, Cr, Co, Cu, I, Fe, Mn, Se, and Zn | AD (44), HC (41) | 85 | Zn↓ (p < 0.001) |
| [136] | CSF, plasma | ICP-MS | Mg, Ca, Mn, Fe, Cu, Zn, Rb, Sr, Cs | AD (174), AD with minor vascular components (90), DLB (29), HC (51) | 344 | In AD compared to LBD: CSF and plasma Mg↓ (p < 0.001), Ca↓ (p ≤ 0.001), Cu↓ (p ≤ 0.004), CSF Cs↓ (p < 0.001), plasma Zn↑ (p = 0.003) In AD compared to HC: No difference |
| [137] | CSF | AAS | Fe | AD (13), early stage of MCI (21), moderate MCI (10), HC (12) | 56 | No difference |
| [138] | Serum | HR-ICP-MS | Zn | AD (18), MCI (19), HC (16) | 53 | No difference |
| [139] | Plasma and CSF | ICP-MS | Mg, Ca, V, Mn, Fe, Co, Ni, Cu, Zn, Se, Rb, Sr, Mo, Cd, Sn, Sb, Cs, Hg, and Pb | AD (173), patients with a combination of AD and minor vascular components (AD + VaD; 87), HC (54) | 314 | In plasma: Mn↑ (p < 0.001), Hg↑ (p < 0.001), Co↓ (p < 0.01), Se↓ (p < 0.01), Cs↓ (p < 0.01) In CSF: V↓, Mn↓, Rb↓, Sb↓, Cs↓, Pb↓ (for all comparisons p < 0.001) |
| [140] | Serum | ICP-MS, ICP-AES | Ca, Cu, Fe, Mg, Si, Zn, Ba, Be, Bi, Cd, Hg, Li, Mo, Pb, Sb, Sn, Sr, Tl, W, Zr, Al, Co, Cr, Mn, Ni, and V | AD (53), PD (71), MS (60), HC (124) | 308 | Ca↑, Sn↑, Co↓, Fe↓, Zn↓ (for all comparisons p < 0.001) |
| [141] | Serum and whole blood | ICP-MS, ICP-AES | Al, Ba, Be, Bi, Ca, Cd, Co, Cr, Cu, Fe, Hg, Li, Mn, Mo, Ni, Pb, Sb, Si, Sn, Sr, Tl, V, W, Zn, and Zr | AD (60), HC (44) | 104 | In serum: Ca↑, Cd↑, Hg↑, Mg↑, Si↑, Sn↑, Al↓, Co↓, Fe↓, Zn↓ In blood: Cu↑, Li↑, Mn↑, Sn↑, Zr↑, Fe↓, Hg↓, Mo↓ (for all comparisons p ≤ 0.05) |
| [142] | Serum | Chromato-graphic or spectro- photometric methods | Fe, Zn, Mn, Se, Co, Cr, Cu, Mo, and AI | AD (8), VaD (8), cognitive impairment non-dementia (8), HC (11) | 35 | Se↓, Co↓, Cr↓, Cu↑, Al↑ (for all comparisons p < 0.001) |
| [143] | CSF, serum | AAS | Se | AD (27), HC (34) | 61 | No difference |
| [144] | Plasma | AAS | Cu | AD (44), HC (44) | 88 | No difference |
| [145] | Blood | AAS | Hg | AD (33), control group with major depression (45), control group with non-psychiatric disorders (65) | 143 | Hg↑ (p < 0.001) |
| [146] | Serum and CSF | AAS | Fe, Cu, Mn, and Zn | AD (26), HC (28) | 54 | CSF Zn↓ (p < 0.05) |
| [147] | Serum | AAS | Al | AD (17), HC (189), other dementias (15) | 221 | Al↑ (p = 0.001) |
| [148] | Whole blood | GF-AAS | Cd | AD (6), demented (10), HC (19) | 35 | No difference |
| [149] | CSF and serum | Ca was determined using the o-Cresol- phthalein method, whereas P was determined using the molybdate method | Ca and P | AD (40), multiple infarct dementia (25), aged controls (20), adult controls (20) | 105 | CSF Ca↓ (p < 0.01), P↓ (p < 0.01) (compared to adult controls) |
| [150] | CSF | AAS | Zn | AD (34), HC (34) | 68 | No difference |
| [151] | CSF | Inductively coupled argon plasma emission spectroscopy | Al, As, Ba, Be, Cd, Co, Cr, Cu, Fe, Mn, Mo, Ni, Pb, Se, Si, Sn, Ti, V, and Zn | AD (33), other dementia (16), no neurological disease (20) | 69 | Si↑ (p < 0.05), Zn↑ (p < 0.05) |
| Reference | Analyzed Bodily Fluid | Measured Metals | Measured Biomarkers | Association of Metals with CSF Protein Biomarkers | Classification of Participants (Number of Patients) | Number of Participants |
|---|---|---|---|---|---|---|
| [74] | CSF and plasma | In CSF and plasma: As, B, Ca, Cd, Co, Cu, Fe, Hg, Li, Mg, Mn, Mo, Na, Ni, P, Pb, S, Se, Sr, Tl, Zn In CSF: Al, Ba, K | CSF Aβ1–42, t-tau, p-tau181, p-tau231, p-tau199, NFL, S100B, VILIP-1, YKL-40, PAPP-A, and albumin | Positive association of CSF heavy metals (As, Cd, Hg, Ni, Pb, and Tl), essential metals (Ca, Co, Cu, Fe, Mg, Mn, Mo, Na, K, and Zn), and essential nonmetals (P, S, and Se) and plasma Ni with CSF p-tau isoforms, VILIP-1, S100B, NFL, and YKL-40 (for all comparisons p ≤ 0.001) | CSF: AD (124), MCI (50), HC (19) Plasma: AD (93), MCI (35), HC (15) | CSF: 193 Plasma: 143 |
| [185] | Serum and blood | Blood Se | Serum Aβ1–40 and Aβ1–42 | Negative association of Se with Aβ1–40 and Aβ1–42 and positive association with Aβ1–42/Aβ1–40 ratio (p < 0.05) | Elderly individuals | 469 |
| [90] | CSF | Ni, Cr, Zn, Mn, Co, and Cu | Aβ1–42, Aβ1–40, t-tau, p-tau181, NFL | The negative correlation of Fe and ferritin with Aβ1–42 (r = −0.506, p < 0.001) | AD (20), cerebral amyloid angiopathy (10), controls (10) | 40 |
| [186] | Serum, CSF | Serum Ca | CSF Aβ1–42, t-tau, p-tau181 | Serum Ca negatively correlated with CSF Aβ1–42 (β = −0.558, p = 0.008) | MCI (811), cognitively normal (413) | 1224 |
| [187] | Serum | Al, Pb, Mn, and Zn | T-tau | The negative correlation between Mn and t-tau (r = −0.341, p = 0.003) | Aluminum foundry workers (75), non-occupationally exposed subjects as controls (75) | 150 |
| [188] | CSF | Fe, Cr, Mn, Ni, Cu, Zn | Aβ1–42, t-tau, p-tau, and CSF/serum albumin ratio | Positive correlation of Fe and Cu with Aβ1–42 (βFe = 0.21, p = 0.004, βCu = 0.23, p = 0.001), t-tau (βFe = 0.27, p < 0.001, βCu = 0.23, p = 0.001), p-tau (βFe = 0.30, p < 0.001, βCu = 0.26, p < 0.001) and CSF/serum albumin ratio (βFe = 0.52, p < 0.001, βCu = 0.65, p < 0.001). Positive correlation of Zn with CSF/serum albumin ratio (β = 0.17, p = 0.02). | AD (85), MCI (72), subjective cognitive impairment (32), VaD (7) | 196 |
| [104] | CSF | Ca | Aβ1–42, t-tau, p-tau181 | No association of CSF Ca with CSF AD biomarkers | AD (45), HC (45) | 90 |
| [189] | CSF | Se | CSF Aβ1–42, t-tau, and p-tau | The negative correlation between Se and Aβ1–42 (β = −0.27, 95% CI; −0.66–0.11) | MCI (56), during the 42 months, 21 developed AD, 4 FTD, and 2 DLB | 56 |
| [190] | Blood, plasma | Blood Se | Plasma Aβ1–42, t-tau | No association of Se with plasma AD biomarkers | AD (30), VaD (35), HC (40) | 105 |
| [191] | Blood and plasma | Blood Mn | Plasma Aβ1–40 and Aβ1–42 | Positive correlation of Mn with Aβ1–40 (R2 = 0.127, p = 0.024) and Aβ1–42 (R2 = 0.163, p = 0.010) | AD (20), MCI (10), HC (10) | 40 |
| [192] | CSF | Mg, Ca, V, Cd, Sn, Sb, Mn, Ni, Cu, Zn, Se, Rb, Fe, Co, Sr, Mo, Cs, Hg, and Pb | Aβ1–42, t-tau, p-tau181 | Positive correlation between Mn and t-tau (rs = 0.22, p = 0.004) and p-tau181 (rs = 0.18, p = 0.021). The negative correlation of Cs with t-tau (rs = −0.49, p = 0.026), and a positive correlation of Cs with Aβ1–42 (rs = 0.49, p = 0.026). | AD (173), AD + minor vascular components (87), HC (54) | 314 |
| [193] | CSF (taken from brain ventricles) | Cu, Zn, Fe, Mn, and Cr | Aβ1–42 | The negative correlation of Cu (β coefficient = −1.3, p < 0.001), Zn (β coefficient = −1.26, p < 0.001), Fe (p = 0.001), Mn (p = 0.003), and Cr (p = 0.01) with Aβ1–42 | AD (25), VaD (18), other dementias (6), clinically non-demented individuals (82) | 131 |
| [194] | CSF | Cu intake | Aβ1–42, t-tau, p-tau181 | Cu intake did not affect the t-tau and p-tau181 levels, but the Aβ1–42 levels decreased by 30% in the placebo group and only by 10% in the verum group | AD (68) | 68 |
| [195] | CSF, serum | Serum K | CSF Aβ1–42 | Low serum K in mid-life, but not late life, is associated with low CSF Aβ1–42 in late life (β = 153.9, p = 0.041) | Women from Goteborg | 1080 |
| [196] | Serum, plasma and CSF | Cu (in serum) | Aβ1–42, t-tau (in CSF) | The negative correlation of Cu with Aβ1–42 (r = −0.46, p = 0.002), and the positive correlation of Cu with t-tau (r = 0.4, p = 0.03) | AD (28), HC (25) | 53 |
| [145] | Blood and CSF | Hg (in the blood) | Aβ1–42 (in CSF) | Positive correlation between Hg and Aβ1–42 (r = 0.744, p < 0.001) | AD (33), age-matched control patients with major depression (45), and a control group of patients with a variety of non-psychiatric disorders (65) served as comparison groups | 143 |
| Reference | MR Analysis | Measured Metals | Observed Association |
|---|---|---|---|
| [218] | Two-sample MR | Mg, Ca, Fe, Cu, Zn, Se, P | Higher Cu levels as a protective factor for AD risk |
| [170] | Two-sample MR | Pb (in the blood) | Higher Pb levels as a risk factor for AD |
| [241] | Two-sample MR | Ca (in serum) | Higher Ca levels as a protective factor for AD risk |
| [243] | MR | Ca (in serum) | Higher Ca levels as a protective factor for AD risk |
| [219] | Two-sample MR | Cu, Zn, Fe | No association |
| [220] | Two-sample MR | Ca, Mg, Fe, Cu, Zn (in the blood) | Higher Cu levels as a protective factor for AD risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babić Leko, M.; Langer Horvat, L.; Španić Popovački, E.; Zubčić, K.; Hof, P.R.; Šimić, G. Metals in Alzheimer’s Disease. Biomedicines 2023, 11, 1161. https://doi.org/10.3390/biomedicines11041161
Babić Leko M, Langer Horvat L, Španić Popovački E, Zubčić K, Hof PR, Šimić G. Metals in Alzheimer’s Disease. Biomedicines. 2023; 11(4):1161. https://doi.org/10.3390/biomedicines11041161
Chicago/Turabian StyleBabić Leko, Mirjana, Lea Langer Horvat, Ena Španić Popovački, Klara Zubčić, Patrick R. Hof, and Goran Šimić. 2023. "Metals in Alzheimer’s Disease" Biomedicines 11, no. 4: 1161. https://doi.org/10.3390/biomedicines11041161
APA StyleBabić Leko, M., Langer Horvat, L., Španić Popovački, E., Zubčić, K., Hof, P. R., & Šimić, G. (2023). Metals in Alzheimer’s Disease. Biomedicines, 11(4), 1161. https://doi.org/10.3390/biomedicines11041161