
Glioblastoma: A Retrospective Analysis of the Role of the Maximal Surgical Resection on Overall Survival and Progression Free Survival


 ,
, 
Abstract
1. Background
2. Materials and Methods
2.1. Patient Population and Neuroradiological Characteristics of the Tumor
2.2. Extent of Resection and Outcome Evaluation
2.3. Data Analysis
3. Results
3.1. Study Population
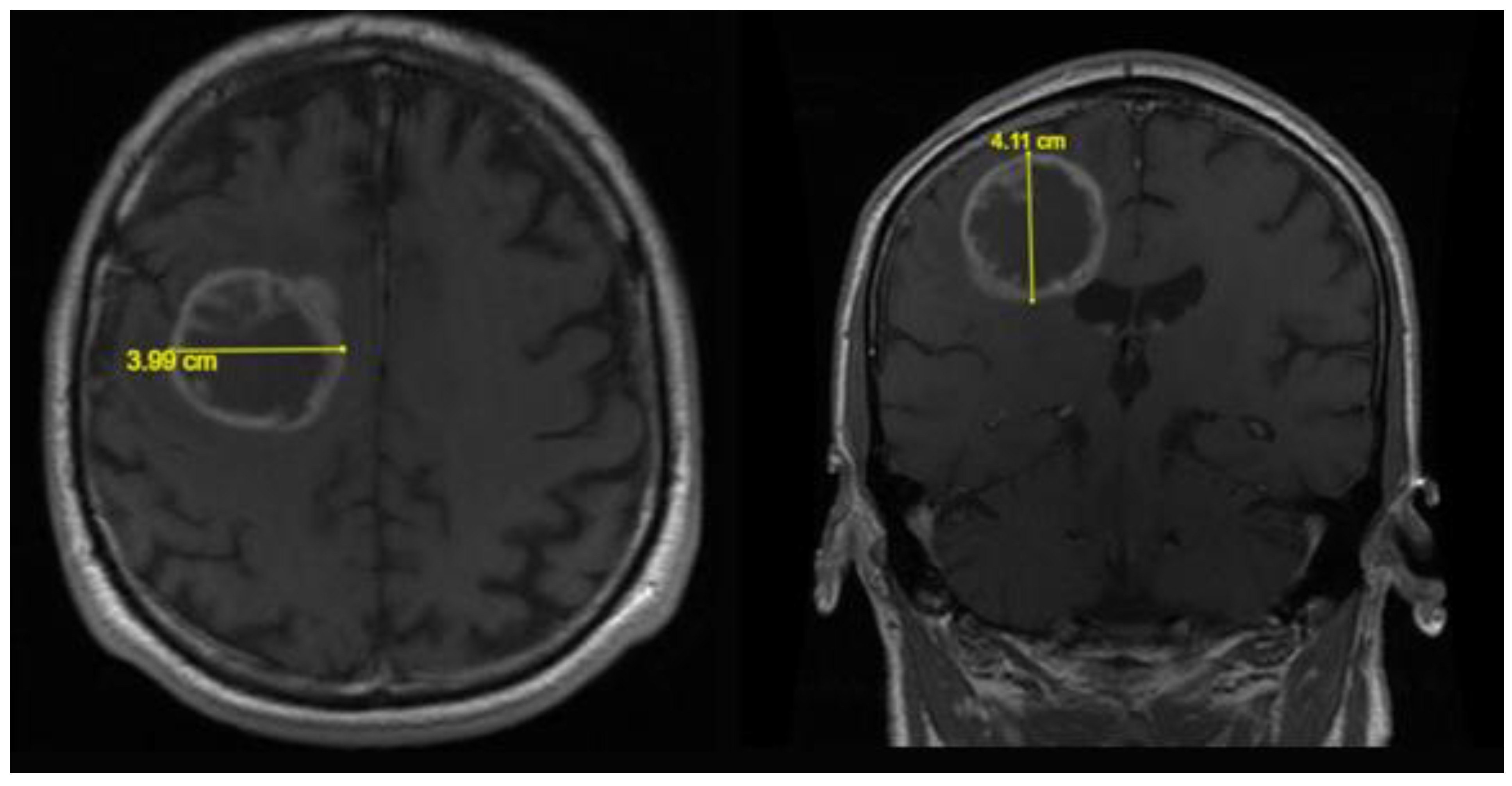
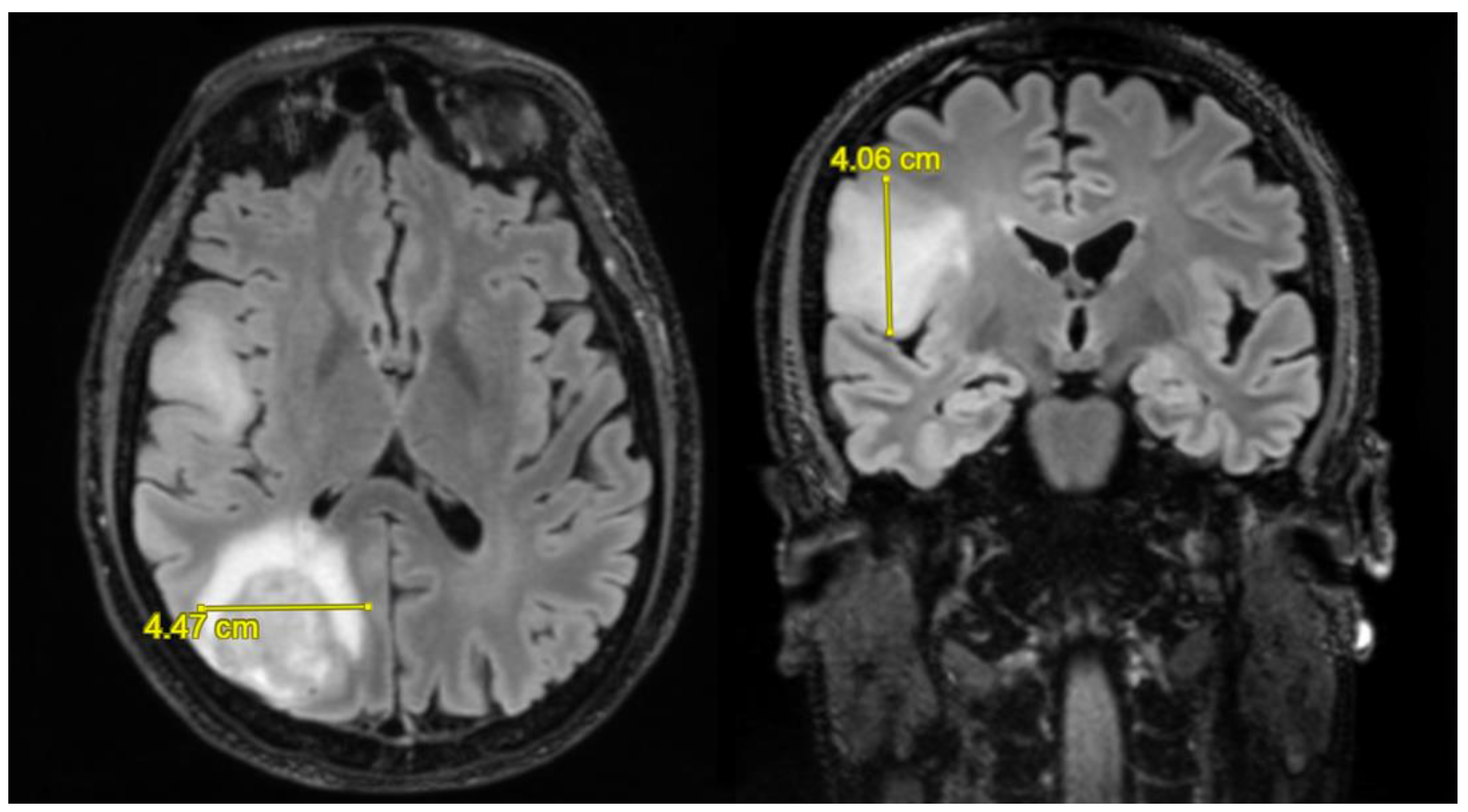
3.2. Neuroradiological Findings
3.3. Patient Outcomes
3.4. Statistical Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Fulop, J.; Liu, M.; Blanda, R.; Kromer, C.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2008–2012. Neuro-Oncol. 2015, 17 (Suppl. S4), iv1–iv62. [Google Scholar] [CrossRef] [PubMed]
- Pessina, F.; Navarria, P.; Cozzi, L.; Ascolese, A.M.; Simonelli, M.; Santoro, A.; Clerici, E.; Rossi, M.; Scorsetti, M.; Bello, L. Maximize surgical resection beyond contrast-enhancing boundaries in newly diagnosed glioblastoma multiforme: Is it useful and safe? A single institution retrospective experience. J. Neuro-Oncol. 2017, 135, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.F.; Ottaviani, D.; Tazare, J.; Gregson, J.; Kitchen, N.; Brandner, S.; Fersht, N.; Mulholland, P. Survival outcomes and prognostic factors in Glioblastoma. Cancers 2022, 14, 3161. [Google Scholar] [CrossRef] [PubMed]
- Abedi, A.A.; Grunnet, K.; Christensen, I.J.; Michaelsen, S.R.; Muhic, A.; Møller, S.; Hasselbalch, B.; Poulsen, H.S.; Urup, T. A Prognostic Model for Glioblastoma Patients Treated With Standard Therapy Based on a Prospective Cohort of Consecutive Non-Selected Patients From a Single Institution. Front. Oncol. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Lamborn, K.R.; Chang, S.M.; Prados, M.D. Prognostic factors for survival of patients with glioblastoma: Recursive partitioning analysis. Neuro-Oncol. 2004, 6, 227–235. [Google Scholar] [CrossRef]
- Swanson, K.R.; Rockne, R.C.; Claridge, J.; Chaplain, M.A.; Alvord, E.C.; Anderson, A.R. Quantifying the role of angiogenesis in malignant progression of gliomas: In silico modeling integrates imaging and histology. Cancer Res. 2011, 71, 7366–7375. [Google Scholar] [CrossRef] [PubMed]
- Yordanova, Y.; Duffau, H. Supratotal resection of diffuse gliomas—An overview of its multifaceted implications. Neurochirurgie 2017, 63, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro-Oncol. 2013, 16, 113–122. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef]
- Incekara, F.; Smits, M.; Van Der Voort, S.R.; Dubbink, H.J.; Atmodimedjo, P.N.; Kros, J.M.; Vincent, A.J.P.E.; Bent, M.V.D. The association between the extent of glioblastoma resection and survival in light of MGMT promoter methylation in 326 patients with newly diagnosed IDH-wildtype glioblastoma. Front. Oncol. 2020, 10, 1087. [Google Scholar] [CrossRef]
- Wang, J.; Hu, G.; Quan, X. Analysis of the factors affecting the prognosis of glioma patients. Open Med. 2019, 14, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Pessina, F.; Navarria, P.; Cozzi, L.; Ascolese, A.M.; Simonelli, M.; Santoro, A.; Tomatis, S.; Riva, M.; Fava, E.; Scorsetti, M.; et al. Value of surgical resection in patients with newly diagnosed grade III glioma treated in a multimodal approach: Surgery, chemotherapy and radiotherapy. Ann. Surg. Oncol. 2016, 23, 3040–3046. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Berger, M.S. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008, 62, 753–766. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, M.M.; Recinos, P.F.; Nowacki, A.S.; Schroeder, J.L.; Angelov, L.; Barnett, G.H.; Vogelbaum, M.A. Residual tumor volume versus extent of resection: Predictors of survival after surgery for glioblastoma. J. Neurosurg. 2014, 121, 1115–1123. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Clavreul, A.; Menei, P. Intratumoral heterogeneity in glioblastoma: Don’t forget the peritumoral brain zone. Neuro-Oncol. 2015, 17, 1322–1332. [Google Scholar] [CrossRef]
- Dobelbower, M.C.; Burnett Iii, O.L.; Nordal, R.A.; Nabors, L.B.; Markert, J.M.; Hyatt, M.D.; Fiveash, J.B. Patterns of failure for glioblastoma multiforme following concurrent radiation and temozolomide. J. Med. Imaging Radiat. Oncol. 2011, 55, 77–81. [Google Scholar] [CrossRef]
- Smith, J.S.; Chang, E.F.; Lamborn, K.R.; Chang, S.M.; Prados, M.D.; Cha, S.; Tihan, T.; Vandenberg, S.; McDermott, M.W.; Berger, M.S. Role of extent of resection in the long-term outcome of low-grade hemispheric gliomas. J. Clin. Oncol. 2008, 26, 1338–1345. [Google Scholar] [CrossRef]
- Eidel, O.; Burth, S.; Neumann, J.-O.; Kieslich, P.J.; Sahm, F.; Jungk, C.; Kickingereder, P.; Bickelhaupt, S.; Mundiyanapurath, S.; Bäumer, P.; et al. Tumor Infiltration in Enhancing and Non-Enhancing Parts of Glioblastoma: A Correlation with Histopathology. PLoS ONE 2017, 12, e0169292. [Google Scholar] [CrossRef]
- Marina, O.; Suh, J.H.; Reddy, C.; Barnett, G.H.; Vogelbaum, M.A.; Peereboom, D.M.; Stevens, G.H.J.; Elinzano, H.; Chao, S.T. Treatment outcomes for patients with glioblastoma multiforme and a low Karnofsky Performance Scale score on presentation to a tertiary care institution. J. Neurosurg. 2011, 115, 220–229. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Morshed, R.A.; Berger, M.S. FLAIRectomy: Resecting beyond the Contrast Margin for Glioblastoma. Brain Sci. 2022, 12, 544. [Google Scholar] [CrossRef]
- Dobran, M.; Nasi, D.; Chiriatti, S.; Gladi, M.; di Somma, L.; Iacoangeli, M.; Scerrati, M. Prognostic factors in glioblastoma: Is there a role for epilepsy? Neurol. Med.-Chir. 2018, 58, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Revilla-Pacheco, F.; Rodríguez-Salgado, P.; Barrera-Ramírez, M.; Morales-Ruiz, M.P.; Loyo-Varela, M.; Rubalcava-Ortega, J.; Herrada-Pineda, T. Extent of resection and survival in patients with glioblastoma multiforme. Medicine 2021, 100, e26432. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. of Patients | % | |
|---|---|---|
| Total | 64 | 100 |
| Gender | ||
| Female | 30 | 47 |
| Male | 34 | 53 |
| Median Age | 62 | (Range 25–84 yrs) |
| Adjuvant treatment | ||
| CHT | 56 | 87.5 |
| RT | 57 | 89 |
| CHT + RT | 57 | 89 |
| No adjuvant treatment | 7 | 11 |
| Long surviving (OS > 60 mos) | 2 | 3 |
| No. of Patients | % | |
|---|---|---|
| Surgical resection | ||
| Supratotal resection (SUPr) | 14 | 22 |
| Gross total resection (GTR) | 10 | 16 |
| Subtotal resection (STR) | 35 | 55 |
| Biopsy (B) | 5 | 8 |
| Total resection | ||
| >90% | 27 | 42 |
| ≤90% | 37 | 58 |
| Tumor volume (TV) | ||
| Median pre-operative T1 TV | 40.1 cm³ | (Range 1.2–201.8 cm³) |
| Median pre-operative FLAIR TV | 50.3 cm³ | (Range 10–183.1 cm³) |
| Mean (Months) | Median (Months) | |
|---|---|---|
| Overall survival (OS) | ||
| SUPr group | 37.3 | 24 |
| GTR group | 20.7 | 16 |
| STR group | 14.2 | 14 |
| B group | 9.4 | 10 |
| 1 month OS | ||
| KPS ≤ 70 | 11 | |
| KPS > 70 | 16 | |
| 3 months OS | ||
| KPS ≤ 70 | 7 | |
| KPS > 70 | 17 | |
| 6 months OS | ||
| KPS ≤ 70 | 11 | |
| KPS > 70 | 19 | |
| Progression-free survival | ||
| SUPr group | 12.6 | 8 |
| GTR group | 10 | 9.5 |
| Subtotal resection (STR) | 5.9 | 5 |
| Biopsy (B) | 3.2 | 3 |
| Factors Analyzed | No. of Patients | Median OS Mos | Univ. (p Value) | Multiv. (p Value) |
|---|---|---|---|---|
| Total resection | 0.018 | 0.027 | ||
| >90% | 27 | 18 ± 1.7 | ||
| ≤90% | 37 | 14 ± 2.8 | ||
| Surgical tumor residue | 0.019 | 0.028 | ||
| + | 40 | 14 ± 2.2 | ||
| − | 24 | 18 ± 1.1 | ||
| Extent of resection | 0.003 | 0.001 | ||
| SUPr | 14 | 24 ± 4.8 | ||
| GTR | 10 | 16 ± 2.4 | ||
| STR | 35 | 14 ± 3.6 | ||
| BIOPSY | 5 | 10 ± 2.2 | ||
| 1 month KPS | 0.081 | 0.074 | ||
| KPS ≤ 70 | 11 | 11 ± 4.5 | ||
| KPS > 70 | 53 | 16 ± 1.2 | ||
| 3 months KPS | 0.012 | 0.011 | ||
| KPS ≤ 70 | 16 | 7 ± 2.4 | ||
| KPS > 70 | 48 | 17 ± 3.7 | ||
| 6 months KPS | <0.0001 | <0.0001 | ||
| KPS ≤ 70 | 23 | 11 ± 3.7 | ||
| KPS > 70 | 43 | 19 ± 1.2 | ||
| CHT | <0.0001 | <0.0001 | ||
| + | 56 | 17 ± 1.3 | ||
| − | 8 | 4 ± 1.4 | ||
| RT | <0.0001 | <0.0001 | ||
| + | 57 | 17 ± 0.7 | ||
| − | 7 | 3 ± 1.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polonara, G.; Aiudi, D.; Iacoangeli, A.; Raggi, A.; Ottaviani, M.M.; Antonini, R.; Iacoangeli, M.; Dobran, M. Glioblastoma: A Retrospective Analysis of the Role of the Maximal Surgical Resection on Overall Survival and Progression Free Survival. Biomedicines 2023, 11, 739. https://doi.org/10.3390/biomedicines11030739
Polonara G, Aiudi D, Iacoangeli A, Raggi A, Ottaviani MM, Antonini R, Iacoangeli M, Dobran M. Glioblastoma: A Retrospective Analysis of the Role of the Maximal Surgical Resection on Overall Survival and Progression Free Survival. Biomedicines. 2023; 11(3):739. https://doi.org/10.3390/biomedicines11030739
Chicago/Turabian StylePolonara, Gabriele, Denis Aiudi, Alessio Iacoangeli, Alessio Raggi, Matteo Maria Ottaviani, Ruggero Antonini, Maurizio Iacoangeli, and Mauro Dobran. 2023. "Glioblastoma: A Retrospective Analysis of the Role of the Maximal Surgical Resection on Overall Survival and Progression Free Survival" Biomedicines 11, no. 3: 739. https://doi.org/10.3390/biomedicines11030739
APA StylePolonara, G., Aiudi, D., Iacoangeli, A., Raggi, A., Ottaviani, M. M., Antonini, R., Iacoangeli, M., & Dobran, M. (2023). Glioblastoma: A Retrospective Analysis of the Role of the Maximal Surgical Resection on Overall Survival and Progression Free Survival. Biomedicines, 11(3), 739. https://doi.org/10.3390/biomedicines11030739