
The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Definition of Metabolic Syndrome and Homocysteine Levels
2.4. Statistical Analysis
3. Results
3.1. The Characteristics of Study Subjects by Metabolic Syndrome Status
3.2. The Characteristics of Study Subjects According to Tertiles of Homocysteine
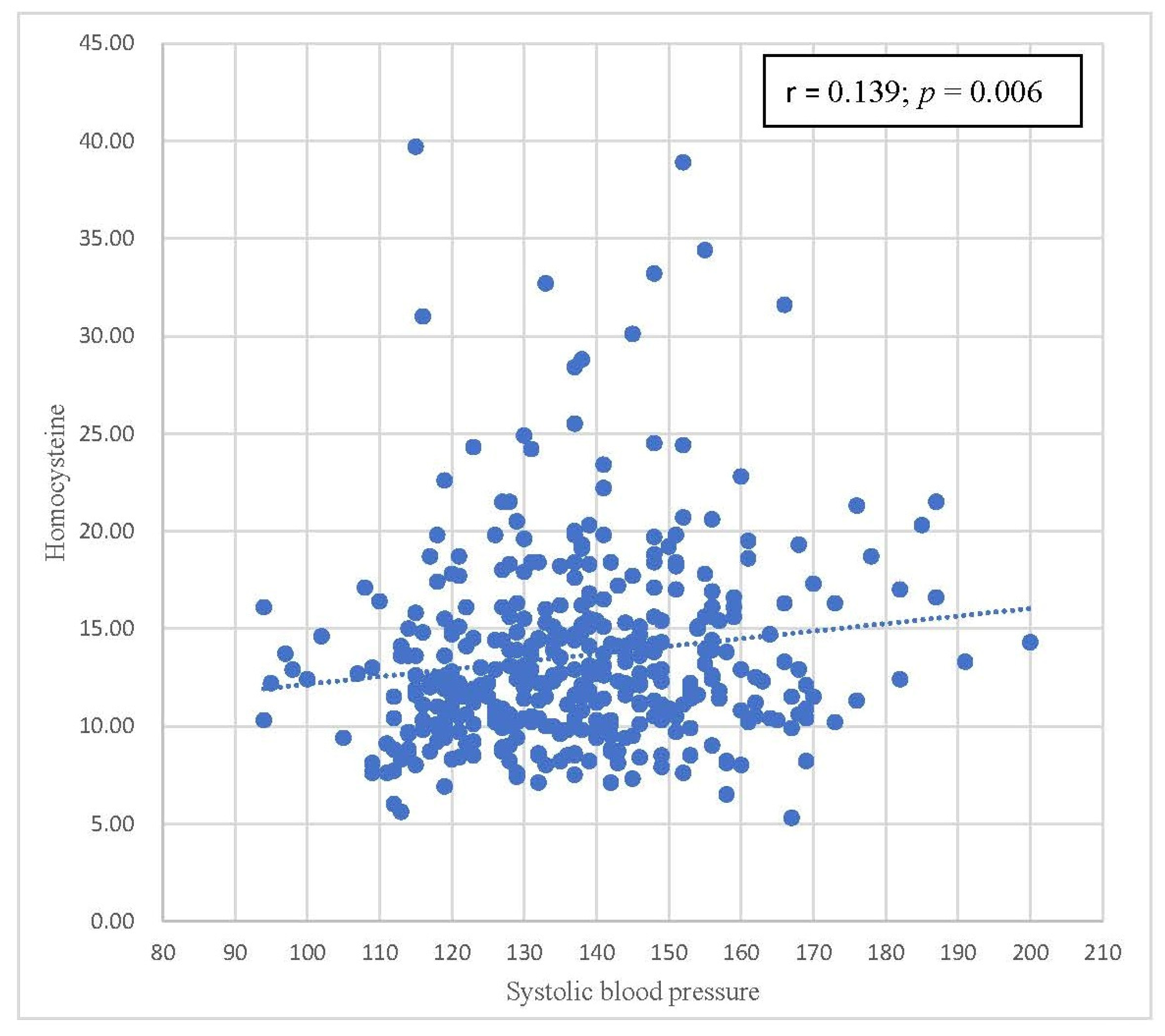
3.3. Pearson’s Correlation between Homocysteine and Components of Metabolic Syndrome
3.4. Multiple Logistic Regression Analysis of the Association between Homocysteine Level and Metabolic Syndrome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jarrett, R.J. The MetS. Lancet 2005, 366, 1922. [Google Scholar] [CrossRef]
- Grundy, S.M. MetS: Connecting and reconciling cardiovascular and diabetes worlds. J. Am. Coll. Cardiol. 2006, 47, 1000–1093. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, J.P.; McKinley, B.; Eckel, R.H. The MetS and inflammation. MetS Relat. Disord. 2004, 2, 82–104. [Google Scholar] [CrossRef]
- Grundy, S.M. Obesity, metabolic syndrome, and cardiovascular disease. J. Clin. Endocrinol. Metab. 2004, 89, 2595–2600. [Google Scholar] [CrossRef] [PubMed]
- Abate, N.; Sallam, S.H.; Rizzo, M.; Nikolic, D.; Obradovic, M.; Bjelogrlic, P.; Isenovic, R.E. Resistin: An inflammatory cytokine. Role in cardiovascular diseases, diabetes and the metabolic syndrome. Curr. Pharm. Pharm. Design 2014, 20, 4961–4969. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, R.; Passalacqua, W.; Araya, J.; Orellana, M.; Rivera, G. Implications of oxidative stress and homocysteine in the pathophysiology of essential hypertension. J. Cardiovasc. Pharmacol. 2003, 42, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Cruciani-Guglielmacci, C.; Meneyrol, K.; Denom, J.; Kassis, N.; Rachdi, L.; Makaci, F.; Migrenne-Li, S.; Daubigney, F.; Georgiadou, E.; Denis, R.G.; et al. Homocysteine Metabolism Pathway Is Involved in the Control of Glucose Homeostasis: A Cystathionine Beta Synthase Deficiency Study in Mouse. Cells 2022, 11, 1737. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J.; LeRoith, D.; Karnieli, E. Insulin resistance in obesity as the underlying cause for the metabolic syndrome. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2010, 77, 511–523. [Google Scholar] [CrossRef]
- North, B.J.; Sinclair, D.A. The intersection between aging and cardiovascular disease. Circ. Res. 2012, 110, 1097–1108. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Kerner, W.; Brückel, J. Definition, classification and diagnosis of diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 2014, 122, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.F.; Chang, Y.H.; Chien, S.C.; Lin, Y.H.; Yeh, H.Y. Epidemiology of dyslipidemia in the Asia Pacific region. Int. J. Gerontol. 2018, 12, 2–6. [Google Scholar] [CrossRef]
- Lin, C.H.; Lai, S.W.; Liu, C.S. Prevalence of metabolic syndrome in Taiwanese adults: A hospital-based study. Ann. Saudi Med. 2006, 26, 46–48. [Google Scholar] [CrossRef] [PubMed]
- Katsimardou, A.; Imprialos, K.; Stavropoulos, K.; Sachinidis, A.; Doumas, M.; Athyros, V. Hypertension in Metabolic Syndrome: Novel Insights. Curr. Hypertens. Rev. 2020, 16, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Raal, F.J. Pathogenesis and management of the dyslipidemia of the metabolic syndrome. Metab. Syndr. Relat. Disord. 2009, 7, 83–88. [Google Scholar] [CrossRef]
- Grundy, S.M. Pre-diabetes, metabolic syndrome, and cardiovascular risk. J. Am. Coll. Cardiol. 2012, 59, 635–643. [Google Scholar] [CrossRef]
- Krauss, R.M.; Siri, P.W. Metabolic abnormalities: Triglyceride and low-density lipoprotein. Endocrinol. Metab. Clin. North Am. 2004, 33, 405–415. [Google Scholar] [CrossRef]
- Nilsson, P.M.; Tuomilehto, J.; Rydén, L. The metabolic syndrome—What is it and how should it be managed? Eur. J. Prev. Cardiol. 2019, 26, 33–46. [Google Scholar] [CrossRef]
- Mani, P.; Ren, H.Y.; Neeland, I.J.; McGuire, D.K.; Ayers, C.R.; Khera, A.; Rohatgi, A. The association between HDL particle concentration and incident metabolic syndrome in the multi-ethnic Dallas Heart Study. Diabetes Metab. Syndr. 2017, 11 (Suppl. S1), S175–S179. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, J.; Zhu, L.; Song, L.; Meng, Z.; Jia, Q.; Li, X.; Liu, N.; Hu, T.; Zhou, P.; et al. Association between liver function and metabolic syndrome in Chinese men and women. Sci Rep. 2017, 7, 44844. [Google Scholar] [CrossRef] [PubMed]
- Joyce, T.; Chirino, Y.I.; Natalia, M.T.; Jose, P.C. Renal damage in the metabolic syndrome (MetSx): Disorders implicated. Eur. J. Pharmacol. 2018, 818, 554–568. [Google Scholar] [CrossRef] [PubMed]
- Soltani, Z.; Rasheed, K.; Kapusta, D.R.; Reisin, E. Potential role of uric acid in metabolic syndrome, hypertension, kidney injury, and cardiovascular diseases: Is it time for reappraisal? Curr. Hypertens. Rep. 2013, 15, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Xu, Y. Hyperhomocysteinemia as a Metabolic Risk Factor for Glucose Intolerance Among High-Risk Groups of Chinese Adults. Med. Sci. Monit. 2017, 23, 2775–2781. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, S.; Yao, T.; Li, D.; Wang, Y.; Li, Y.; Wu, S.; Cai, J. Homocysteine as a risk factor for hypertension: A 2-year follow-up study. PLoS ONE 2014, 9, e108223. [Google Scholar] [CrossRef]
- Bowman, T.S.; Gaziano, J.M.; Stampfer, M.J.; Sesso, H.D. Homocysteine and risk of developing hypertension in men. J. Hum. Hypertens. 2006, 20, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Momin, M.; Jia, J.; Fan, F.; Li, J.; Dou, J.; Chen, D.; Huo, Y.; Zhang, Y. Relationship between plasma homocysteine level and lipid profiles in a community-based Chinese population. Lipids Health Dis. 2017, 16, 54. [Google Scholar] [CrossRef]
- Kaur, J. A comprehensive review on metabolic syndrome. Cardiol. Res. Pract. 2014, 2014, 943162, Retraction in: Cardiol. Res. Pract. 2019, 2019, 4301528. [Google Scholar] [CrossRef]
- Smith, U.; Kahn, B.B. Adipose tissue regulates insulin sensitivity: Role of adipogenesis, de novo lipogenesis and novel lipids. J. Intern. Med. 2016, 280, 465–475, Epub 3 October 2016. [Google Scholar] [CrossRef]
- Kelesidis, T.; Kelesidis, I.; Chou, S.; Mantzoros, C.S. Narrative review: The role of leptin in human physiology: Emerging clinical applications. Ann. Intern. Med. 2010, 152, 93–100. [Google Scholar] [CrossRef]
- Fantuzzi, G.; Mazzone, T. Adipose tissue and atherosclerosis: Exploring the connection. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M. Metabolic syndrome pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, L.; Miao, Y.; Yang, J.; Wang, X.; Wang, C.C.; Feng, J.; Wang, L. Homocysteine causes vascular endothelial dysfunction by disrupting endoplasmic reticulum redox homeostasis. Redox Biol. 2019, 20, 46–59. [Google Scholar] [PubMed]
- Pushpakumar, S.; Kundu, S.; Sen, U. Endothelial dysfunction: The link between homocysteine and hydrogen sulfide. Curr. Med. Chem. 2014, 21, 3662–3672. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Leira, Y.; Proenca, L.; Mendes, J.J. Periodontal Inflamed Surface Area Mediates the Link between Homocysteine and Blood Pressure. Biomolecules 2021, 11, 875. [Google Scholar] [CrossRef] [PubMed]
- Balint, B.; Jepchumba, V.K.; Guéant, J.L.; Guéant-Rodriguez, R.M. Mechanisms of homocysteine-induced damage to the endothelial, medial and adventitial layers of the arterial wall. Biochimie 2020, 173, 100–106. [Google Scholar]
- Zhao, Q.; Song, W.; Huang, J.; Wang, D.; Xu, C. Metformin decreased myocardial fibrosis and apoptosis in hyperhomocysteinemia-induced cardiac hypertrophy. Curr. Res. Transl. Med. 2021, 69, 103270. [Google Scholar]
- Shih, Y.L.; Shih, C.C.; Chen, J.Y. Elevated homocysteine level as an indicator for chronic kidney disease in community-dwelling middle-aged and elderly populations in Taiwan: A community-based cross-sectional study. Front. Med. 2022, 9, 964101. [Google Scholar]
- Ebrahimpour, A.; Vaghari-Tabari, M.; Qujeq, D.; Moein, S. Direct correlation between serum homocysteine level and insulin resistance index in patients with subclinical hypothyroidism: Does subclinical hypothyroidism increase the risk of diabetes and cardio vascular disease together? Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 863–867. [Google Scholar] [CrossRef]
- Karas Kuželički, N. S-Adenosyl methionine in the therapy of depression and other psychiatric disorders. Drug Dev. Res. 2016, 77, 346–356. [Google Scholar]
- Rehman, T.; Shabbir, M.A.; Inam-Ur-Raheem, M.; Manzoor, M.F.; Ahmad, N.; Liu, Z.-W.; Ahmad, M.H.; Siddeeg, A.; Abid, M.; Aadil, R.M. Cysteine and homocysteine as biomarker of various diseases. Food Sci. Nutr. 2020, 8, 4696–4707. [Google Scholar] [CrossRef] [PubMed]
- Messerschmidt, A.; Worbs, M.; Steegborn, C.; Wahl, M.C.; Huber, R.; Laber, B.; Clausen, T. Determinants of enzymatic specificity in the cys-met-metabolism PLP-dependent enzyme family: Crystal structure of cystathionine γ-lyase from yeast and intrafamiliar structure comparison. Biol. Chem. 2003, 384, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Blake, S.; Chan, K.T.; Pearson, R.B.; Kang, J. Cystathionine β-synthase in physiology and cancer. BioMed Res. Int. 2018, 3205125. [Google Scholar]
- Noll, C.; Lacraz, G.; Ehses, J.; Coulaud, J.; Bailbe, D.; Paul, J.L.; Portha, B.; Homo-Delarche, F.; Janel, N. Early reduction of circulating homocysteine levels in Goto–Kakizaki rat, a spontaneous nonobese model of type 2 diabetes. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2011, 1812, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Feldman, E.L. Insulin resistance as a key link for the increased risk of cognitive impairment in the metabolic syndrome. Exp. Mol. Med. 2015, 47, e149. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Please Be Variable | Total | Nonmetabolic Syndrome Group | Metabolic Syndrome Group | p-Value |
|---|---|---|---|---|
| (n = 396) | (n = 213) | (n = 183) | ||
| Homocysteine (µmol/L) | 13.60 ± 4.90 | 12.97 ± 4.64 | 14.34 ± 5.10 | <0.001 |
| FPG (mg/dL) | 109.79 ± 35.65 | 99.27 ± 30.97 | 122.02 ± 36.90 | <0.001 |
| ALT (U/L) | 27.16 ± 22.82 | 25.06 ± 20.85 | 29.60 ± 24.76 | <0.001 |
| Creatinine (mg/dL) | 0.87 ± 0.43 | 0.85 ± 0.54 | 0.89 ± 0.26 | <0.001 |
| HDL-C(mg/dL) | 53.65 ± 14.66 | 58.77 ± 14.09 | 47.49 ± 12.54 | <0.001 |
| LDL-C (mg/dL) | 109.69 ± 33.99 | 113.36 ± 33.55 | 105.42 ± 34.10 | <0.001 |
| Triglycerides (mg/dL) | 141.07 ± 110.00 | 101.75 ± 41.20 | 186.85 ± 142.72 | 0.006 |
| Uric acid (mg/dL) | 5.63 ± 1.52 | 5.32 ± 1.34 | 6.00 ± 1.63 | 0.006 |
| Waist circumference (cm) | 85.36 ± 10.83 | 81.12 ± 10.01 | 90.28 ± 9.62 | 0.048 |
| SBP (mmHg) | 137.30 ± 17.49 | 134.07 ± 17.62 | 141.07 ± 16.61 | 0.051 |
| DBP (mmHg) | 85.19 ± 10.98 | 83.37 ± 10.91 | 87.31 ± 10.70 | 0.371 |
| Age (year) | 64.80 ± 8.77 | 63.23 ± 9.38 | 64.28 ± 7.96 | 0.349 |
| BMI (kg/m2) | 25.59 ± 3.84 | 24.00 ± 3.10 | 27.45 ± 3.79 | 0.001 |
| Smoking, n (%) | 50 (12.6) | 21 (9.9) | 29 (15.8) | 0.074 |
| Alcohol consumption, n (%) | 28 (7.1) | 10 (4.7) | 18 (9.8) | 0.047 |
| Hypertension, n (%) | 201 (50.8) | 71 (33.3) | 130 (71.0) | <0.001 |
| Diabetes mellitus, n (%) | 133 (33.6) | 40 (18.8) | 93 (50.8) | <0.001 |
| Dyslipidemia, n (%) | 153 (38.6) | 57 (26.8) | 96 (52.5) | <0.001 |
| Gender (men), n (%) | 164 (41.4) | 83 (39.0) | 81 (44.3) | 0.287 |
| Variable | Nonmetabolic Syndrome (n = 213) | Metabolic Syndrome (n = 183) | p-Value |
|---|---|---|---|
| High waist circumference, n (%) | 67 (31.5%) | 146 (79.8%) | <0.001 |
| High triglyceride, n (%) | 19 (8.9%) | 108 (59.0%) | <0.001 |
| Low HDL-C, n (%) | 10 (4.7%) | 91 (49.7%) | <0.001 |
| High BP, n (%) | 149 (70.0%) | 179 (97.8%) | <0.001 |
| High FPG, n (%) | 54 (25.4%) | 142 (77.6%) | <0.001 |
| Homocysteine | |||||
|---|---|---|---|---|---|
| Variable | Total | First Group | Second Group | Third Group | p-Value |
| (<11.1) | (11.1~14.3) | (≥14.4) | |||
| (n = 396) | (n = 132) | (n = 130) | (n = 134) | ||
| Homocysteine (µmol/L) | 13.60 ± 4.90 | 9.37 ± 1.26 | 12.66 ± 0.90 | 18.69 ± 4.92 | <0.001 |
| FPG (mg/dL) | 109.79 ± 35.65 | 102.89 ± 20.65 | 111.74 ± 41.87 | 114.68 ± 39.74 | 0.007 |
| ALT (U/L) | 27.16 ± 22.82 | 26.06 ± 25.70 | 28.15 ± 21.44 | 27.28 ± 21.18 | 0.665 |
| Creatinine (mg/dL) | 0.87 ± 0.43 | 0.73 ± 0.14 | 0.80 ± 0.19 | 1.07 ± 0.66 | <0.001 |
| HDL-C(mg/dL) | 53.65 ± 14.66 | 56.74 ± 13.89 | 54.42 ± 14.28 | 49.40 ± 14.28 | <0.001 |
| LDL-C (mg/dL) | 109.69 ± 33.99 | 113.27 ± 32.46 | 108.09 ± 35.97 | 107.71 ± 33.46 | 0.183 |
| TG (mg/dL) | 141.07 ± 110.00 | 137.95 ± 105.33 | 141.65 ± 130.97 | 143.59 ± 91.41 | 0.677 |
| Uric acid (mg/dL) | 5.63 ± 1.52 | 5.13 ± 1.27 | 5.53 ± 1.35 | 6.23 ± 1.70 | <0.001 |
| Waist circumference (cm) | 85.36 ± 10.83 | 81.01 ± 10.06 | 86.01 ± 10.55 | 89.00 ± 10.40 | <0.001 |
| SBP (mmHg) | 137.30 ± 17.49 | 134.28 ± 16.60 | 137.29 ± 18.17 | 140.29 ± 17.29 | 0.005 |
| DBP (mmHg) | 85.19 ± 10.98 | 83.61 ± 10.62 | 84.04 ± 10.35 | 87.86 ± 11.49 | 0.001 |
| Age (year) | 64.80 ± 8.77 | 64.19 ± 8.50 | 65.34 ± 9.36 | 64.88 ± 8.47 | 0.521 |
| BMI (kg/m2) | 25.59 ± 3.84 | 24.53 ± 3.38 | 25.49 ± 3.54 | 26.74 ± 4.23 | 0.524 |
| Smoking, n (%) | 50 (12.6) | 7 (5.3) | 14 (10.8) | 29 (21.6) | <0.001 |
| Alcohol consumption, n (%) | 28 (7.1) | 8 (6.1) | 9 (6.9) | 11 (8.2) | 0.495 |
| HTN, n (%) | 201 (50.8) | 55 (41.7) | 63 (48.5) | 83 (61.9) | <0.001 |
| DM, n (%) | 133 (33.6) | 29 (22.0) | 49 (37.7) | 55 (41.0) | <0.001 |
| Dyslipidemia, n (%) | 153 (38.6) | 49 (37.1) | 43 (33.1) | 61 (45.5) | 0.158 |
| Metabolic syndrome, n (%) | 183 (46.2) | 48 (36.4) | 60 (46.2) | 75 (56.0) | <0.001 |
| Gender (male), n (%) | 164 (41.4) | 24 (18.2) | 52 (40.0) | 88 (65.7) | <0.001 |
| Variables | Homocysteine | |
|---|---|---|
| Correlation Coefficient, r | p-Value | |
| FPG (mg/dL) | 0.091 | 0.069 |
| Waist circumference (cm) | 0.251 | <0.001 |
| SBP (mmHg) | 0.139 | 0.006 |
| DBP (mmHg) | 0.152 | 0.002 |
| Triglycerides (mg/dL) | 0.024 | 0.627 |
| HDL-C (mg/dL) | −0.198 | <0.001 |
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | (95% C.I.) | p Value | OR | (95% C.I.) | p Value | OR | (95% C.I.) | p Value | |
| First | 1.00 | 0.006 | 1.00 | 0.014 | 1.00 | 0.08 | |||
| Second | 1.50 | 0.91 to 2.46 | 0.108 | 1.48 | 0.89 to 2.46 | 0.126 | 1.52 | 0.79 to 2.93 | 0.21 |
| Third | 2.22 | 1.36 to 3.64 | 0.001 | 2.23 | 1.30 to 3.81 | 0.004 | 2.32 | 1.12 to 4.78 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, Y.-L.; Shih, C.-C.; Huang, T.-C.; Chen, J.-Y. The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan. Biomedicines 2023, 11, 378. https://doi.org/10.3390/biomedicines11020378
Shih Y-L, Shih C-C, Huang T-C, Chen J-Y. The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan. Biomedicines. 2023; 11(2):378. https://doi.org/10.3390/biomedicines11020378
Chicago/Turabian StyleShih, Yu-Lin, Chin-Chuan Shih, Tzu-Cheng Huang, and Jau-Yuan Chen. 2023. "The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan" Biomedicines 11, no. 2: 378. https://doi.org/10.3390/biomedicines11020378
APA StyleShih, Y.-L., Shih, C.-C., Huang, T.-C., & Chen, J.-Y. (2023). The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan. Biomedicines, 11(2), 378. https://doi.org/10.3390/biomedicines11020378