
Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness

 ,
,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Adiponectin and Interleukin-6 (IL-6) ELISAs
2.3. Statistical Analysis
3. Results
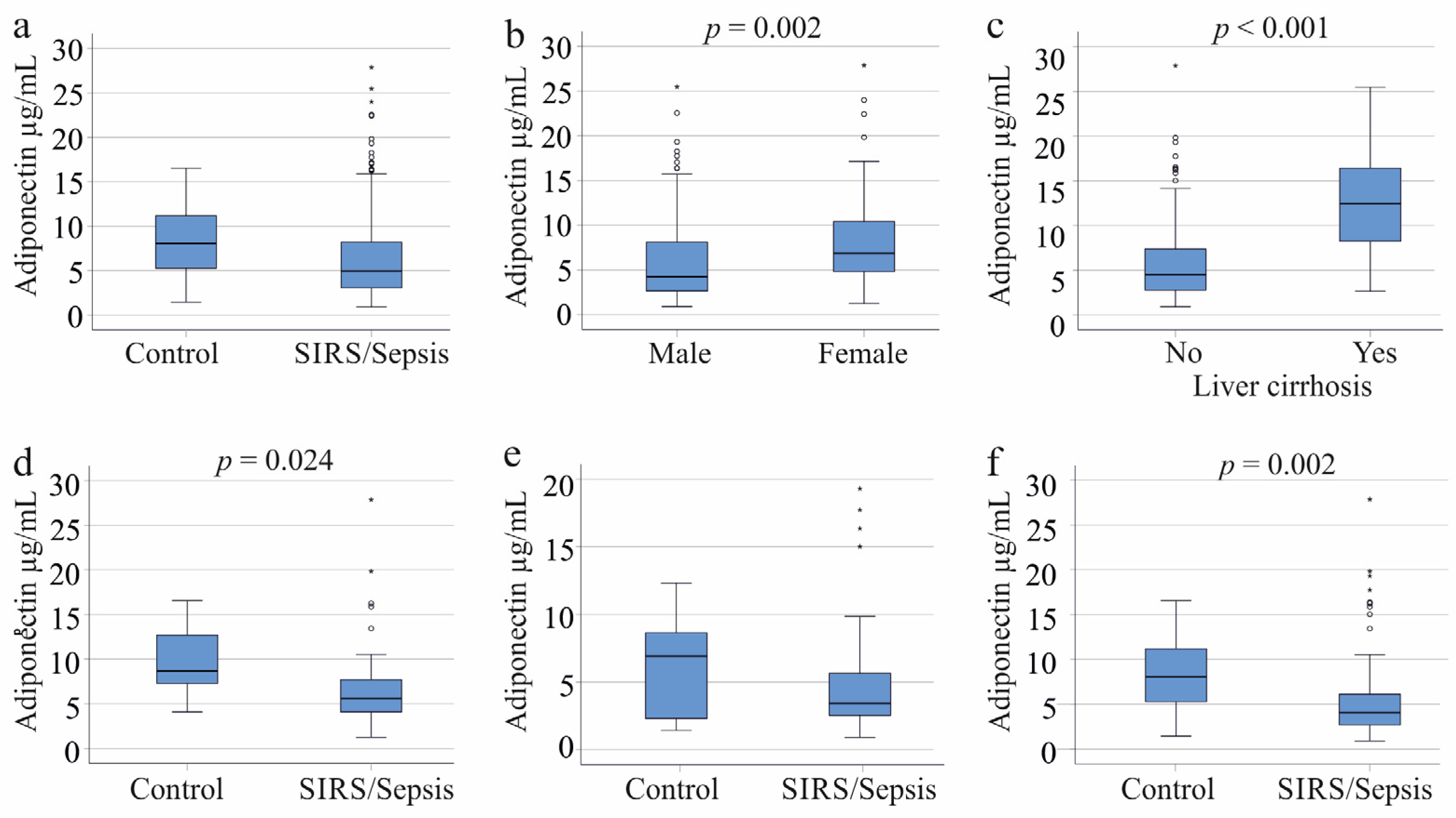
3.1. Adiponectin in the Plasma of Systemic Inflammatory Response Syndrome/Sepsis Patients with and without Liver Cirrhosis
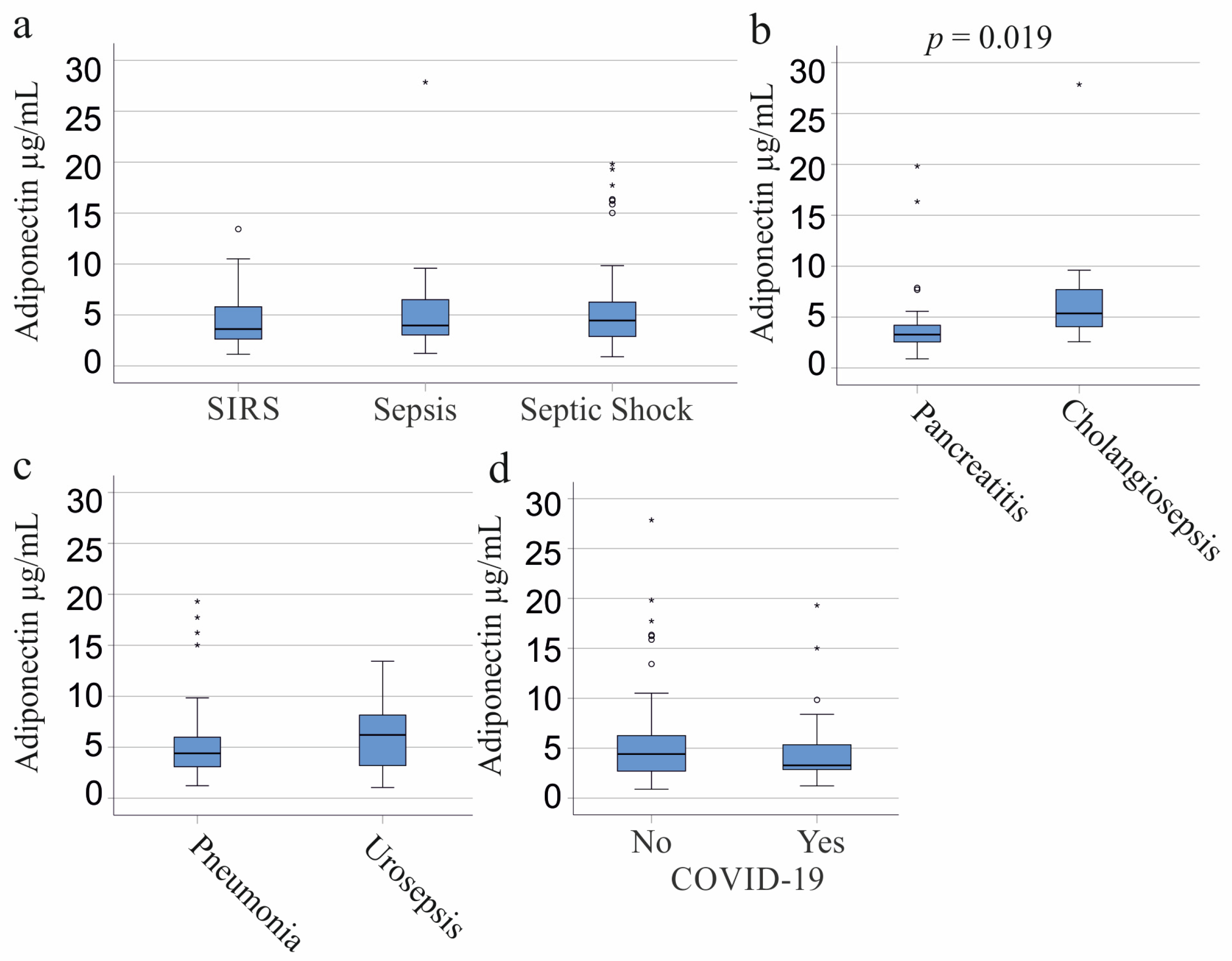
3.2. Plasma Adiponectin of SIRS/Sepsis Patients Stratified for SIRS, Sepsis, and Septic Shock and Underlying Diseases
3.3. Plasma Adiponectin of SIRS/Sepsis Patients Stratified for Infectious Diseases, SARS-CoV-2, and Bacterial Infections
3.4. Plasma Adiponectin Levels in Relation to Vasopressor Therapy and Interventions
3.5. Plasma Adiponectin Levels in Relation to Inflammation Markers
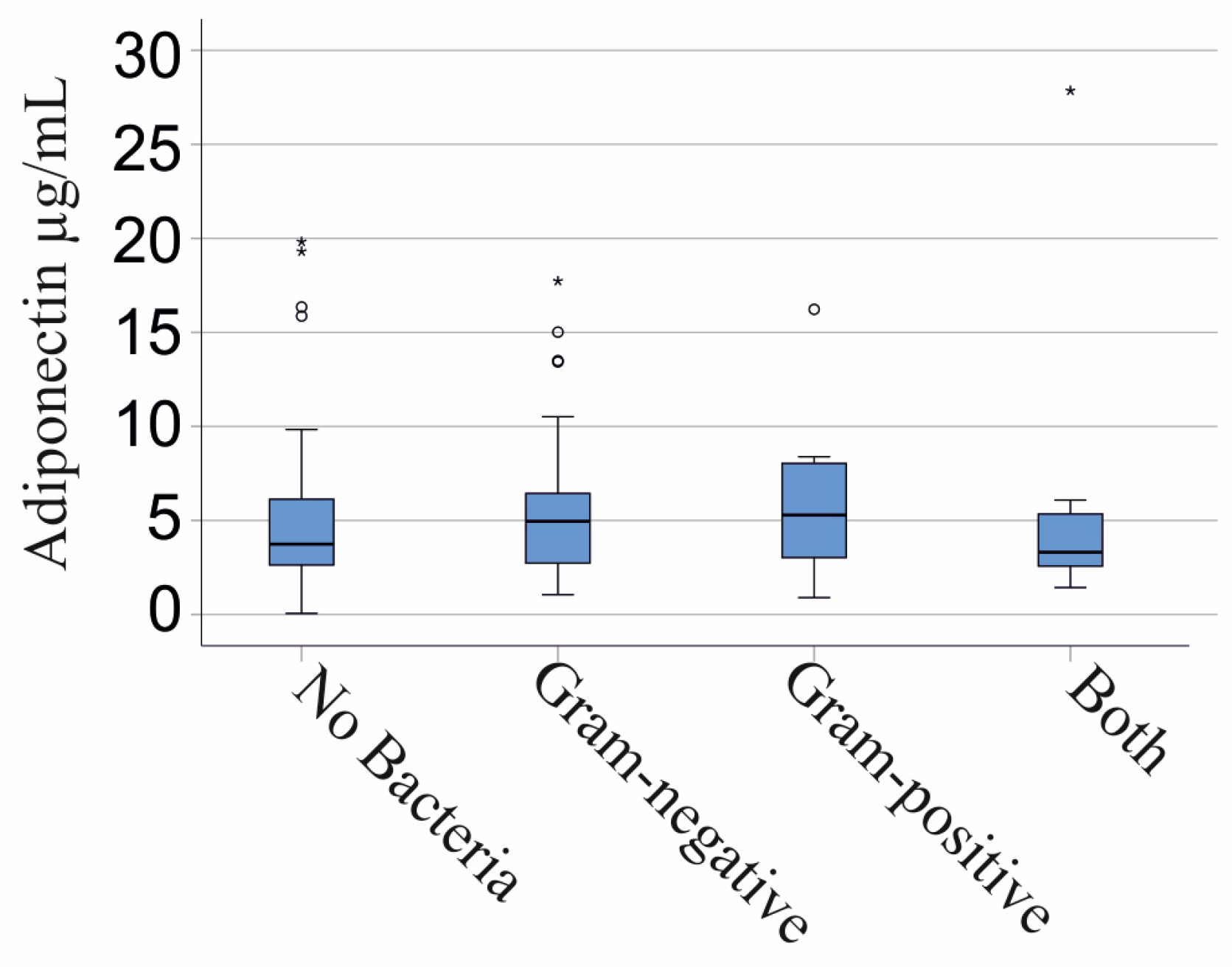
3.6. Plasma Adiponectin Levels in Gram-Negative and Gram-Positive Infection
3.7. Multiple Regression Analysis
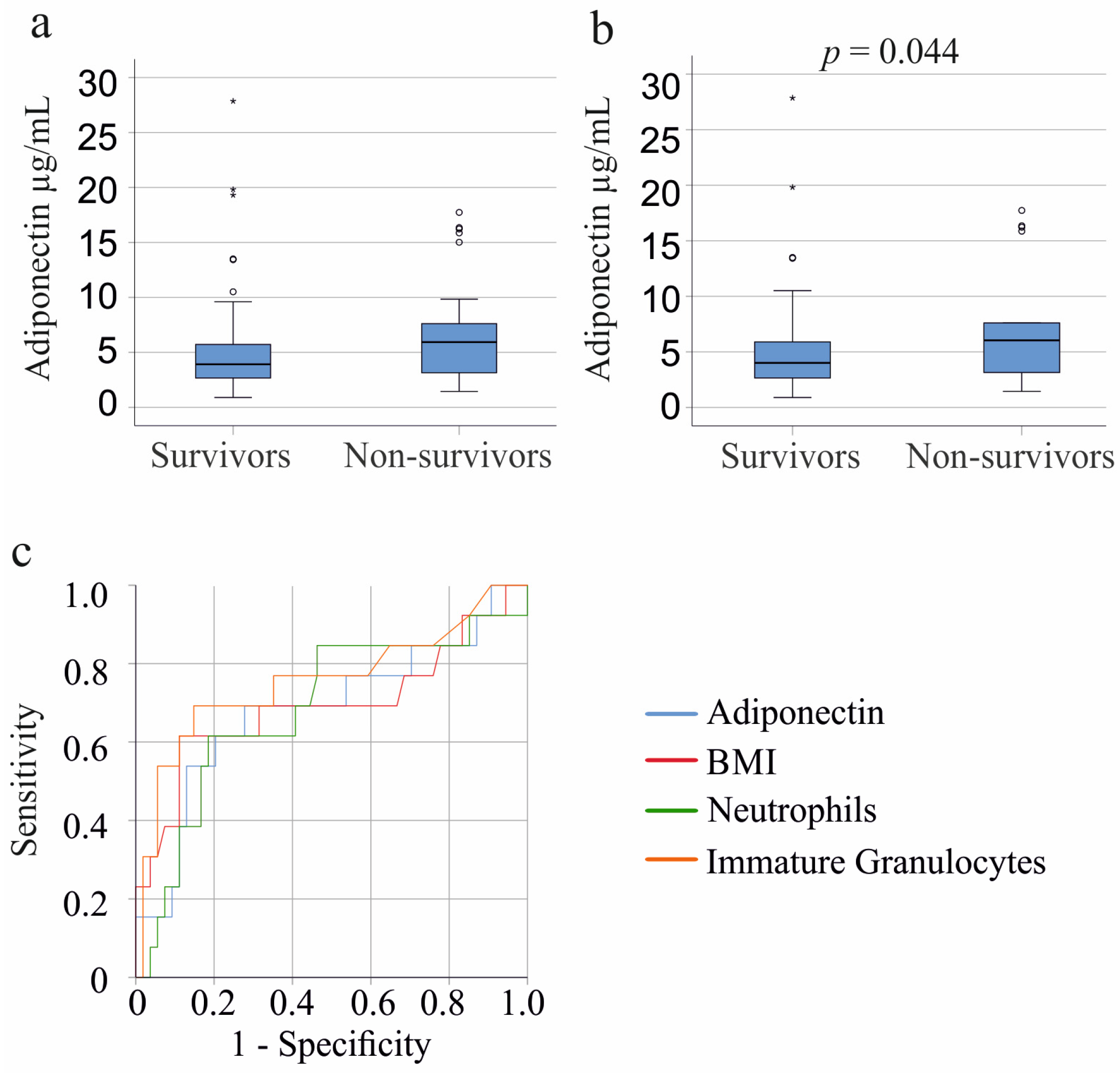
3.8. Plasma Adiponectin Levels and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jarczak, D.; Kluge, S.; Nierhaus, A. Sepsis-Pathophysiology and Therapeutic Concepts. Front. Med. 2021, 8, 628302. [Google Scholar] [CrossRef]
- Nedeva, C.; Menassa, J.; Puthalakath, H. Sepsis: Inflammation Is a Necessary Evil. Front. Cell Dev. Biol. 2019, 7, 108. [Google Scholar] [CrossRef]
- Grewal, T.; Buechler, C. Adipokines as Diagnostic and Prognostic Markers for the Severity of COVID-19. Biomedicines 2023, 11, 1302. [Google Scholar] [CrossRef] [PubMed]
- Ikeagwulonu, R.C.; Ugwu, N.I.; Ezeonu, C.T.; Ikeagwulonu, Z.C.; Uro-Chukwu, H.C.; Asiegbu, U.V.; Obu, D.C.; Briggs, D.C. C-Reactive Protein and COVID-19 Severity: A Systematic Review. West. Afr. J. Med. 2021, 38, 1011–1023. [Google Scholar]
- Becker, K.L.; Snider, R.; Nylen, E.S. Procalcitonin assay in systemic inflammation, infection, and sepsis: Clinical utility and limitations. Crit. Care Med. 2008, 36, 941–952. [Google Scholar] [CrossRef]
- Plebani, M. Why C-reactive protein is one of the most requested tests in clinical laboratories? Clin. Chem. Lab. Med. 2023, 61, 1540–1545. [Google Scholar] [CrossRef] [PubMed]
- Foreman, M.G.; Mannino, D.M.; Moss, M. Cirrhosis as a risk factor for sepsis and death: Analysis of the National Hospital Discharge Survey. Chest 2003, 124, 1016–1020. [Google Scholar] [CrossRef]
- Rannikko, J.; Syrjanen, J.; Seiskari, T.; Aittoniemi, J.; Huttunen, R. Sepsis-related mortality in 497 cases with blood culture-positive sepsis in an emergency department. Int. J. Infect. Dis. 2017, 58, 52–57. [Google Scholar] [CrossRef]
- Pieri, G.; Agarwal, B.; Burroughs, A.K. C-reactive protein and bacterial infection in cirrhosis. Ann. Gastroenterol. 2014, 27, 113–120. [Google Scholar]
- Dong, R.; Wan, B.; Lin, S.; Wang, M.; Huang, J.; Wu, Y.; Wu, Y.; Zhang, N.; Zhu, Y. Procalcitonin and Liver Disease: A Literature Review. J. Clin. Transl. Hepatol. 2019, 7, 51–55. [Google Scholar] [CrossRef]
- Buechler, C.; Wanninger, J.; Neumeier, M. Adiponectin, a key adipokine in obesity related liver diseases. World J. Gastroenterol. 2011, 17, 2801–2811. [Google Scholar] [PubMed]
- Ouchi, N.; Walsh, K. Adiponectin as an anti-inflammatory factor. Clin. Chim. Acta 2007, 380, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Turer, A.T.; Scherer, P.E. Adiponectin: Mechanistic insights and clinical implications. Diabetologia 2012, 55, 2319–2326. [Google Scholar] [CrossRef]
- Ouchi, N.; Kihara, S.; Funahashi, T.; Matsuzawa, Y.; Walsh, K. Obesity, adiponectin and vascular inflammatory disease. Curr. Opin. Lipidol. 2003, 14, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Wulster-Radcliffe, M.C.; Ajuwon, K.M.; Wang, J.; Christian, J.A.; Spurlock, M.E. Adiponectin differentially regulates cytokines in porcine macrophages. Biochem. Biophys. Res. Commun. 2004, 316, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Kumada, M.; Kihara, S.; Ouchi, N.; Kobayashi, H.; Okamoto, Y.; Ohashi, K.; Maeda, K.; Nagaretani, H.; Kishida, K.; Maeda, N.; et al. Adiponectin specifically increased tissue inhibitor of metalloproteinase-1 through interleukin-10 expression in human macrophages. Circulation 2004, 109, 2046–2049. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, K.; Parker, J.L.; Ouchi, N.; Higuchi, A.; Vita, J.A.; Gokce, N.; Pedersen, A.A.; Kalthoff, C.; Tullin, S.; Sams, A.; et al. Adiponectin promotes macrophage polarization toward an anti-inflammatory phenotype. J. Biol. Chem. 2010, 285, 6153–6160. [Google Scholar] [CrossRef]
- Ouchi, N.; Kihara, S.; Funahashi, T.; Nakamura, T.; Nishida, M.; Kumada, M.; Okamoto, Y.; Ohashi, K.; Nagaretani, H.; Kishida, K.; et al. Reciprocal association of C-reactive protein with adiponectin in blood stream and adipose tissue. Circulation 2003, 107, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Fantuzzi, G. Adiponectin in inflammatory and immune-mediated diseases. Cytokine 2013, 64, 1–10. [Google Scholar] [CrossRef]
- Abke, S.; Neumeier, M.; Weigert, J.; Wehrwein, G.; Eggenhofer, E.; Schaffler, A.; Maier, K.; Aslanidis, C.; Scholmerich, J.; Buechler, C. Adiponectin-induced secretion of interleukin-6 (IL-6), monocyte chemotactic protein-1 (MCP-1, CCL2) and interleukin-8 (IL-8, CXCL8) is impaired in monocytes from patients with type I diabetes. Cardiovasc. Diabetol. 2006, 5, 17. [Google Scholar] [CrossRef]
- Weigert, J.; Obermeier, F.; Neumeier, M.; Wanninger, J.; Filarsky, M.; Bauer, S.; Aslanidis, C.; Rogler, G.; Ott, C.; Schaffler, A.; et al. Circulating levels of chemerin and adiponectin are higher in ulcerative colitis and chemerin is elevated in Crohn’s disease. Inflamm. Bowel Dis. 2010, 16, 630–637. [Google Scholar] [CrossRef]
- Luo, L.; Liu, M. Adiponectin: Friend or foe in obesity and inflammation. Med. Rev. 2022, 2, 349–362. [Google Scholar] [CrossRef]
- Loosen, S.H.; Koch, A.; Tacke, F.; Roderburg, C.; Luedde, T. The Role of Adipokines as Circulating Biomarkers in Critical Illness and Sepsis. Int. J. Mol. Sci. 2019, 20, 4820. [Google Scholar] [CrossRef]
- Koch, A.; Sanson, E.; Voigt, S.; Helm, A.; Trautwein, C.; Tacke, F. Serum adiponectin upon admission to the intensive care unit may predict mortality in critically ill patients. J. Crit. Care 2011, 26, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Vassiliadi, D.A.; Tzanela, M.; Kotanidou, A.; Orfanos, S.E.; Nikitas, N.; Armaganidis, A.; Koutsilieris, M.; Roussos, C.; Tsagarakis, S.; Dimopoulou, I. Serial changes in adiponectin and resistin in critically ill patients with sepsis: Associations with sepsis phase, severity, and circulating cytokine levels. J. Crit. Care 2012, 27, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Langouche, L.; Vander Perre, S.; Frystyk, J.; Flyvbjerg, A.; Hansen, T.K.; Van den Berghe, G. Adiponectin, retinol-binding protein 4, and leptin in protracted critical illness of pulmonary origin. Crit. Care 2009, 13, R112. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, B.; Hickman, I.; Nisbet, J.; Cohen, J.; Prins, J. Changes in serum adiponectin concentrations in critical illness: A preliminary investigation. Crit. Care 2009, 13, R105. [Google Scholar] [CrossRef] [PubMed]
- Hillenbrand, A.; Xu, P.; Zhou, S.; Blatz, A.; Weiss, M.; Hafner, S.; Henne-Bruns, D.; Knippschild, U. Circulating adipokine levels and prognostic value in septic patients. J. Inflamm. 2016, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Walkey, A.J.; Rice, T.W.; Konter, J.; Ouchi, N.; Shibata, R.; Walsh, K.; deBoisblanc, B.P.; Summer, R. Plasma adiponectin and mortality in critically ill subjects with acute respiratory failure. Crit. Care Med. 2010, 38, 2329–2334. [Google Scholar] [CrossRef]
- Flikweert, A.W.; Kobold, A.C.M.; van der Sar-van der Brugge, S.; Heeringa, P.; Rodenhuis-Zybert, I.A.; Bijzet, J.; Tami, A.; van der Gun, B.T.F.; Wold, K.I.; Huckriede, A.; et al. Circulating adipokine levels and COVID-19 severity in hospitalized patients. Int. J. Obes. 2023, 47, 126–137. [Google Scholar] [CrossRef]
- Spirina, L.V.; Masunov, V.N.; Dyakov, D.A.; Akbasheva, O.E.; Kebekbayeva, A.Y.; Shuvalov, I.Y.; Masunova, N.V.; Kovaleva, I.V.; Dagbaeva, Y. Sars-Cov2 Induced Biochemical Mechanisms in Liver Damage and Intestinal Lesions. Indian. J. Clin. Biochem. 2022, 38, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Ryrso, C.K.; Dungu, A.M.; Hegelund, M.H.; Jensen, A.V.; Sejdic, A.; Faurholt-Jepsen, D.; Krogh-Madsen, R.; Lindegaard, B. Body composition, physical capacity, and immuno-metabolic profile in community-acquired pneumonia caused by COVID-19, influenza, and bacteria: A prospective cohort study. Int. J. Obes. 2022, 46, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; Sciorati, C.; Capobianco, A.; Lore, N.I.; Giustina, A.; Manfredi, A.A.; Rovere-Querini, P.; Conte, C. Adiponectin to leptin ratio reflects inflammatory burden and survival in COVID-19. Diabetes Metab. 2021, 47, 101268. [Google Scholar] [CrossRef] [PubMed]
- Caterino, M.; Gelzo, M.; Sol, S.; Fedele, R.; Annunziata, A.; Calabrese, C.; Fiorentino, G.; D’Abbraccio, M.; Dell’Isola, C.; Fusco, F.M.; et al. Dysregulation of lipid metabolism and pathological inflammation in patients with COVID-19. Sci. Rep. 2021, 11, 2941. [Google Scholar] [CrossRef] [PubMed]
- de Nooijer, A.H.; Kooistra, E.J.; Grondman, I.; Janssen, N.A.F.; Joosten, L.A.B.; van de Veerdonk, F.L.; Kox, M.; Pickkers, P.; Netea, M.G.; RCI-COVID-19 Study Group. Adipocytokine plasma concentrations reflect influence of inflammation but not body mass index (BMI) on clinical outcomes of COVID-19 patients: A prospective observational study from the Netherlands. Clin. Obes. 2022, 13, e12568. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C. Sepsis, sepsis syndrome, and the systemic inflammatory response syndrome (SIRS). Gulliver in Laputa. JAMA 1995, 273, 155–156. [Google Scholar] [CrossRef] [PubMed]
- Buechler, C.; Haberl, E.M.; Rein-Fischboeck, L.; Aslanidis, C. Adipokines in Liver Cirrhosis. Int. J. Mol. Sci. 2017, 18, 1392. [Google Scholar] [CrossRef]
- Shappell, C.N.; Klompas, M.; Kanjilal, S.; Chan, C.; Rhee, C. Prevalence, Clinical Characteristics, and Outcomes of Sepsis Caused by Severe Acute Respiratory Syndrome Coronavirus 2 Versus Other Pathogens in Hospitalized Patients With COVID-19. Crit. Care Explor. 2022, 4, e0703. [Google Scholar] [CrossRef]
- Sieurin, J.; Branden, G.; Magnusson, C.; Hergens, M.P.; Kosidou, K. A population-based cohort study of sex and risk of severe outcomes in COVID-19. Eur. J. Epidemiol. 2022, 37, 1159–1169. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 1988. [Google Scholar]
- Lancaster, A.; Zwijacz, M. Acute Pancreatitis and Fluid-Filled Collections: Etiology and Endoscopic Management. Gastroenterol. Nurs. 2019, 42, 417–419. [Google Scholar] [CrossRef]
- Ruan, H.; Dong, L.Q. Adiponectin signaling and function in insulin target tissues. J. Mol. Cell Biol. 2016, 8, 101–109. [Google Scholar] [CrossRef]
- Gu, W.; Hortlik, H.; Erasmus, H.P.; Schaaf, L.; Zeleke, Y.; Uschner, F.E.; Ferstl, P.; Schulz, M.; Peiffer, K.H.; Queck, A.; et al. Trends and the course of liver cirrhosis and its complications in Germany: Nationwide population-based study (2005 to 2018). Lancet Reg. Health Eur. 2022, 12, 100240. [Google Scholar] [CrossRef]
- Drake, M.; Dodwad, S.J.; Davis, J.; Kao, L.S.; Cao, Y.; Ko, T.C. Sex-Related Differences of Acute and Chronic Pancreatitis in Adults. J. Clin. Med. 2021, 10, 300. [Google Scholar] [CrossRef]
- Lammert, F.; Gurusamy, K.; Ko, C.W.; Miquel, J.F.; Mendez-Sanchez, N.; Portincasa, P.; van Erpecum, K.J.; van Laarhoven, C.J.; Wang, D.Q. Gallstones. Nat. Rev. Dis. Primers 2016, 2, 16024. [Google Scholar] [CrossRef]
- Dreger, N.M.; Degener, S.; Ahmad-Nejad, P.; Wobker, G.; Roth, S. Urosepsis--Etiology, Diagnosis, and Treatment. Dtsch. Arztebl. Int. 2015, 112, 837–847; quiz 848. [Google Scholar] [CrossRef]
- Corica, B.; Tartaglia, F.; D’Amico, T.; Romiti, G.F.; Cangemi, R. Sex and gender differences in community-acquired pneumonia. Intern. Emerg. Med. 2022, 17, 1575–1588. [Google Scholar] [CrossRef]
- Lakbar, I.; Einav, S.; Lalevee, N.; Martin-Loeches, I.; Pastene, B.; Leone, M. Interactions between Gender and Sepsis-Implications for the Future. Microorganisms 2023, 11, 746. [Google Scholar] [CrossRef]
- Al Duhailib, Z.; Farooqi, M.; Piticaru, J.; Alhazzani, W.; Nair, P. The role of eosinophils in sepsis and acute respiratory distress syndrome: A scoping review. Can. J. Anaesth. 2021, 68, 715–726. [Google Scholar] [CrossRef]
- Davido, B.; Partouche, B.; Jaffal, K.; de Truchis, P.; Herr, M.; Pepin, M. Eosinopenia in COVID-19: What we missed so far? J. Microbiol. Immunol. Infect. 2021, 54, 1006–1007. [Google Scholar] [CrossRef]
- Yu, J.; Wang, Y.Q.; Lin, S.L.; Jiang, L.; Sang, L.; Zheng, X.; Zhong, M. Severe COVID-19 has a distinct phenotype from bacterial sepsis: A retrospective cohort study in deceased patients. Ann. Transl. Med. 2021, 9, 1054. [Google Scholar] [CrossRef]
- de Roquetaillade, C.; Mansouri, S.; Brumpt, C.; Neuwirth, M.; Voicu, S.; Le Dorze, M.; Fontaine, C.; Barthélémy, R.; Gayat, E.; Megarbane, B.; et al. Comparison of Circulating Immune Cells Profiles and Kinetics Between Coronavirus Disease 2019 and Bacterial Sepsis*. Crit. Care Med. 2021, 49, 1717–1725. [Google Scholar] [CrossRef]
- Cnop, M.; Havel, P.J.; Utzschneider, K.M.; Carr, D.B.; Sinha, M.K.; Boyko, E.J.; Retzlaff, B.M.; Knopp, R.H.; Brunzell, J.D.; Kahn, S.E. Relationship of adiponectin to body fat distribution, insulin sensitivity and plasma lipoproteins: Evidence for independent roles of age and sex. Diabetologia 2003, 46, 459–469. [Google Scholar] [CrossRef]
- de Nooijer, A.H.; Antonakos, N.; Markopoulou, D.; Grondman, I.; Kox, M.; Pickkers, P.; Giamarellos-Bourboulis, E.J.; Netea, M.G. The Role of Obesity and Plasma Adipocytokines in Immune Dysregulation in Sepsis Patients. Shock 2023, 59, 344–351. [Google Scholar] [CrossRef]
- Bai, L.; Huang, J.; Wang, D.; Zhu, D.; Zhao, Q.; Li, T.; Zhou, X.; Xu, Y. Association of body mass index with mortality of sepsis or septic shock: An updated meta-analysis. J. Intensive Care 2023, 11, 27. [Google Scholar] [CrossRef]
- Umemura, Y.; Ogura, H.; Takuma, K.; Fujishima, S.; Abe, T.; Kushimoto, S.; Hifumi, T.; Hagiwara, A.; Shiraishi, A.; Otomo, Y.; et al. Current spectrum of causative pathogens in sepsis: A prospective nationwide cohort study in Japan. Int. J. Infect. Dis. 2021, 103, 343–351. [Google Scholar] [CrossRef]
- Taira, R.; Yamaguchi, S.; Shimizu, K.; Nakamura, K.; Ayabe, T.; Taira, T. Bacterial cell wall components regulate adipokine secretion from visceral adipocytes. J. Clin. Biochem. Nutr. 2015, 56, 149–154. [Google Scholar] [CrossRef]
- Agnello, L.; Giglio, R.V.; Bivona, G.; Scazzone, C.; Gambino, C.M.; Iacona, A.; Ciaccio, A.M.; Lo Sasso, B.; Ciaccio, M. The Value of a Complete Blood Count (CBC) for Sepsis Diagnosis and Prognosis. Diagnostics 2021, 11, 1881. [Google Scholar] [CrossRef]
- Wang, H.; Gao, Y.X.; Wu, Y.N.; Li, C.; Duan, J. Association between plasma adiponectin levels and left ventricular systolic dysfunction in sepsis patients. J. Crit. Care 2020, 60, 195–201. [Google Scholar] [CrossRef]
- Alay, G.H.; Tatlisuluoglu, D.; Bulut, K.; Fikri, B.I.; Oztas, A.; Turan, G. The Relationship between Immature Granulocyte Count and Mortality in ARDS Due to COVID-19. Niger. J. Clin. Pract. 2022, 25, 1301–1307. [Google Scholar] [CrossRef]
- Urrechaga, E. Reviewing the value of leukocytes cell population data (CPD) in the management of sepsis. Ann. Transl. Med. 2020, 8, 953. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All Patients | Patients with Liver Cirrhosis Excluded | Controls |
|---|---|---|---|
| Males/Females | 109/47 | 86/38 | 11/11 |
| Age (years) | 59 (21–93) | 57 (21–88) | 58 (40–67) |
| Body Mass Index (kg/m2) | 26.2 (15.4–55.6) | 26.2 (15.4–55.6) | not defined |
| SIRS/Sepsis/Septic Shock | 37/40/79 | 27/33/64 | not defined |
| C-reactive protein mg/L | 157 (12–697) *** | 183 (35–597) *** | not defined |
| Procalcitonin ng/mL | 1.15 (0.05–270.00) | 1.17 (0.06–270.00) | not defined |
| IL-6 pg/mL | 89 (0–5702)150 %%% | 75 (0–5702)121 %%% | 7 (0–48)21 %%% |
| Leukocytes n/nL | 10.31 (0.06–1586.00) | 10.35 (2.16–37.38) | not defined |
| Neutrophils n/nL | 7.55 (0–70.20) | 7.34 (0–70.20) | not defined |
| Basophils n/nL | 0.04 (0–0.90) | 0.04 (0–0.90) | not defined |
| Eosinophils n/nL | 0.13 (0–8.80) | 0.12 (0–8.80) | not defined |
| Monocytes n/nL | 0.78 (0–45.00) | 0.75 (0–45.00) | not defined |
| Lymphocytes n/nL | 0.95 (0.08–28.60) | 1.04 (0.08–28.60) | not defined |
| Immature Granulocytes n/nL | 0.12 (0–6.19) | 0.12 (0–6.19) | not defined |
| Intervention/Drug | Patients without Liver Cirrhosis (124) | Females without Liver Cirrhosis (38) | Males without Liver Cirrhosis (86) | |||
|---|---|---|---|---|---|---|
| N | p-Value | N | p-Value | N | p-Value | |
| Dialysis | 38 | 0.160 | 9 | 0.325 | 29 | 0.185 |
| Ventilation | 75 | 0.994 | 23 | 0.137 | 52 | 0.500 |
| Vasopressor therapy | 74 | 0.530 | 19 | 0.298 | 55 | 0.140 |
| Biomarker of Inflammation | Patients without Liver Cirrhosis (124) | Females without Liver Cirrhosis (38) | Males without Liver Cirrhosis (86) | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Leukocytes | −0.028 | 0.759 | −0.085 | 0.612 | 0.055 | 0.616 |
| Neutrophils | −0.003 | 0.977 | −0.114 | 0.502 | 0.149 | 0.177 |
| Basophils | 0.020 | 0.825 | 0.227 | 0.171 | −0.001 | 0.994 |
| Eosinophils | −0.131 | 0.151 | 0.236 | 0.154 | −0.195 | 0.077 |
| Monocytes | −0.023 | 0.804 | −0.171 | 0.306 | 0.114 | 0.304 |
| Lymphocytes | −0.114 | 0.215 | 0.041 | 0.805 | −0.142 | 0.202 |
| Immature Granulocytes | −0.083 | 0.372 | −0.197 | 0.250 | 0.022 | 0.846 |
| Procalcitonin | −0.020 | 0.825 | 0.310 | 0.058 | −0.141 | 0.204 |
| C-reactive protein | −0.199 | 0.027 | −0.067 | 0.688 | −0.299 | 0.005 |
| Interleukin-6 | −0.022 | 0.807 | 0.159 | 0.341 | −0.098 | 0.379 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, P.; Räth, U.; Schmid, S.; Müller, M.; Buechler, C.; Pavel, V. Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness. Biomedicines 2023, 11, 3287. https://doi.org/10.3390/biomedicines11123287
Mester P, Räth U, Schmid S, Müller M, Buechler C, Pavel V. Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness. Biomedicines. 2023; 11(12):3287. https://doi.org/10.3390/biomedicines11123287
Chicago/Turabian StyleMester, Patricia, Ulrich Räth, Stephan Schmid, Martina Müller, Christa Buechler, and Vlad Pavel. 2023. "Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness" Biomedicines 11, no. 12: 3287. https://doi.org/10.3390/biomedicines11123287
APA StyleMester, P., Räth, U., Schmid, S., Müller, M., Buechler, C., & Pavel, V. (2023). Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness. Biomedicines, 11(12), 3287. https://doi.org/10.3390/biomedicines11123287