
Blast-Derived Small Extracellular Vesicles in the Plasma of Patients with Acute Myeloid Leukemia Predict Responses to Chemotherapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Donors
2.2. sEV Isolation
2.3. Western Blots
2.4. Microarray Printing
2.5. Microarray: Antibodies
2.6. Microarray: Visualization and Data Analysis
2.7. Microarray: Optimization for Immunocapture of LAA+ and Total Plasma sEV
2.8. Statistical Analyses
3. Results
3.1. Patient Characteristics
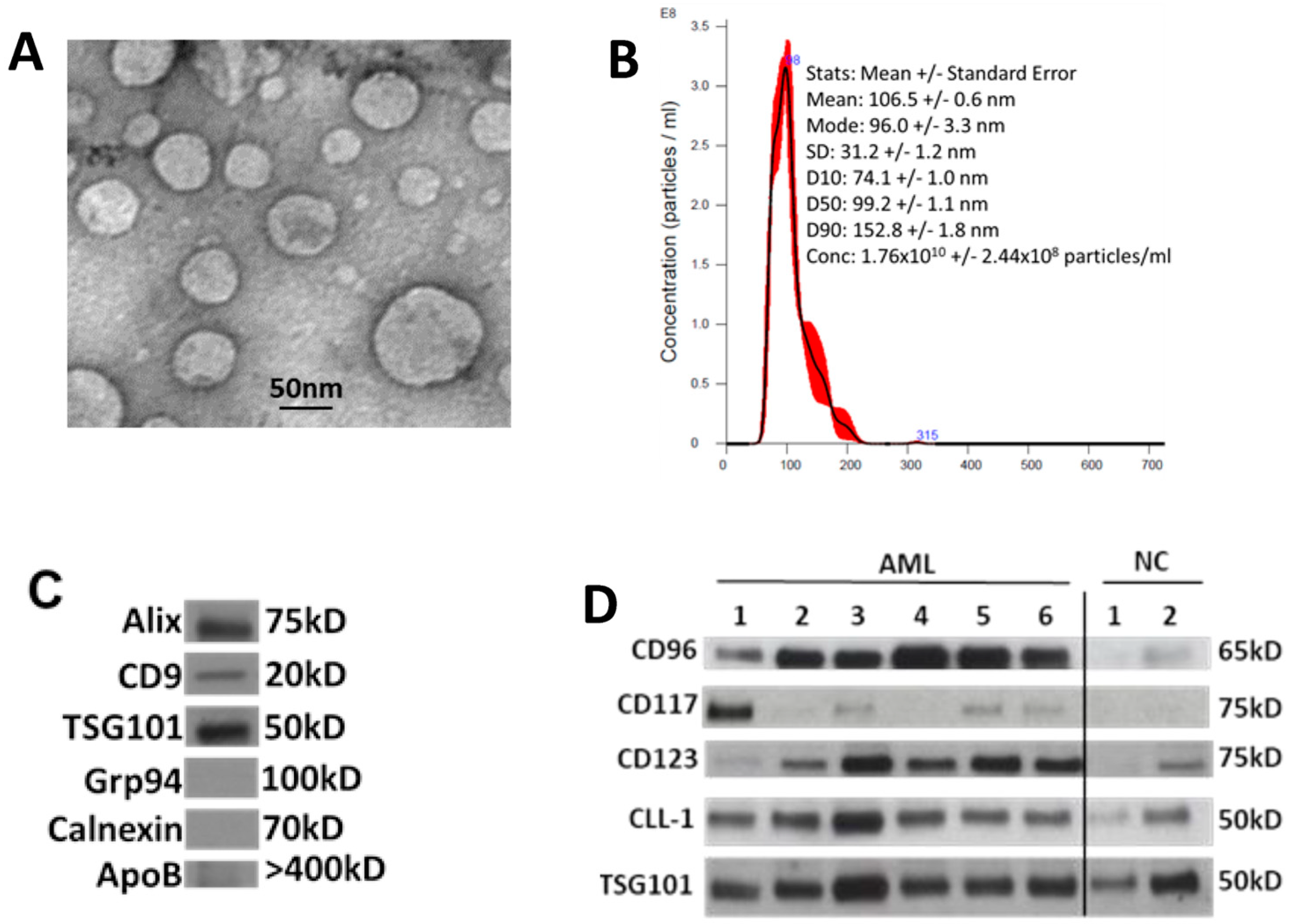
3.2. Characterization of sEV Isolated from AML Patients’ Plasma
3.3. Total sEV Protein (TEP) Levels in AML Patients’ Plasma
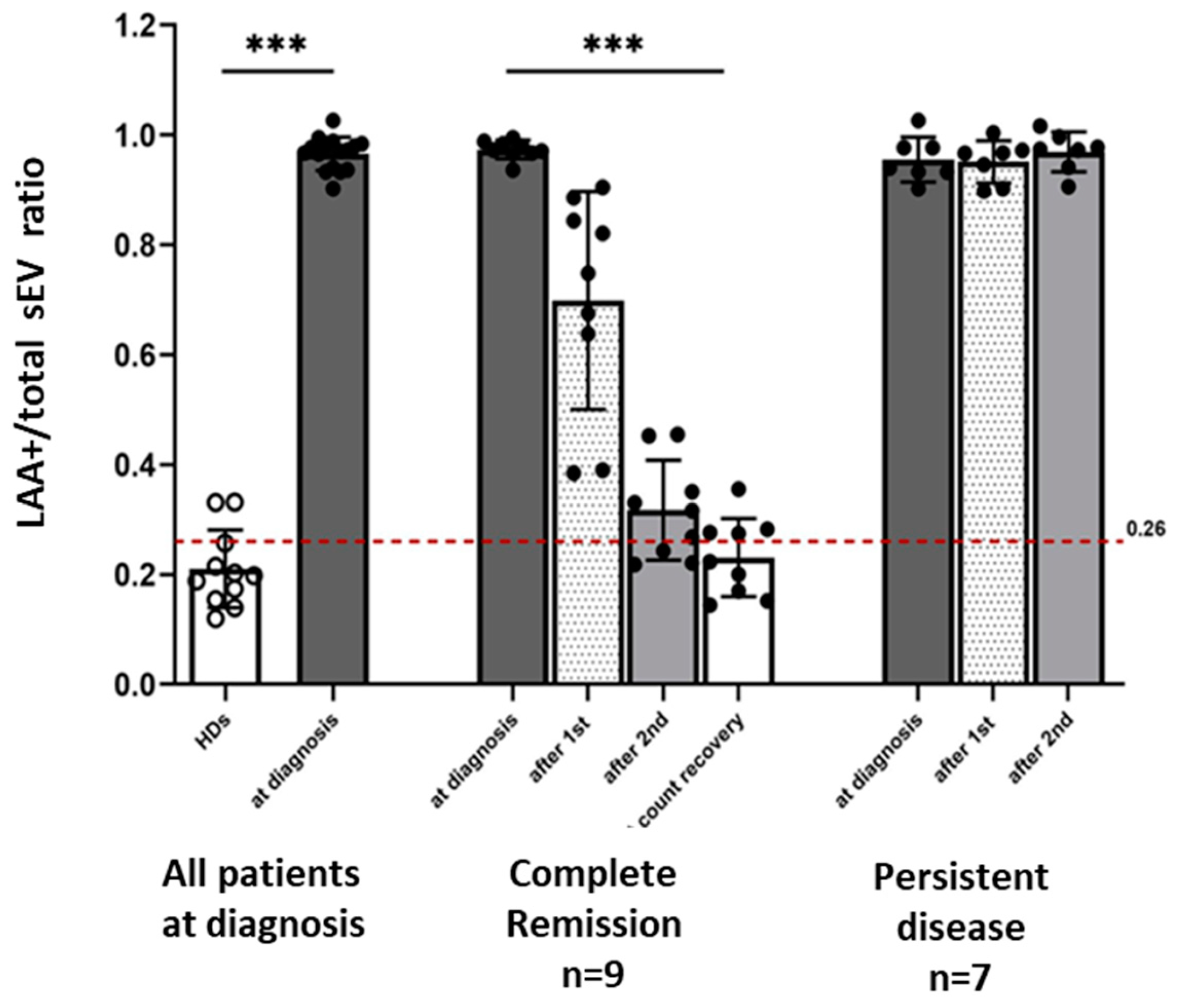
3.4. LAA+ sEV in AML Patients’ Plasma Measured by Microarrays
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, R.; Patel, T.; Freedman, J.E. Circulating Extracellular Vesicles in Human Disease. N. Engl. J. Med. 2018, 379, 2180–2181. [Google Scholar] [CrossRef]
- Xu, R.; Rai, A.; Chen, M.; Suwakulsiri, W.; Greening, D.W.; Simpson, R.J. Extracellular vesicles in cancer—Implications for future improvements in cancer care. Nat. Rev. Clin. Oncol. 2018, 15, 617–638. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, D.K.; Zhang, Q.; Franklin, J.L.; Coffey, R.J. Extracellular vesicles and nanoparticles: Emerging complexities. Trends Cell Biol. 2023, 33, 667–681. [Google Scholar] [CrossRef] [PubMed]
- Moller, A.; Lobb, R.J. The evolving translational potential of small extracellular vesicles in cancer. Nat. Rev. Cancer 2020, 20, 697–709. [Google Scholar] [CrossRef] [PubMed]
- Szczepanski, M.J.; Szajnik, M.; Welsh, A.; Whiteside, T.L.; Boyiadzis, M. Blast-derived microvesicles in sera from patients with acute myeloid leukemia suppress natural killer cell function via membrane-associated transforming growth factor-beta1. Haematologica 2011, 96, 1302–1309. [Google Scholar] [CrossRef]
- Hong, C.S.; Muller, L.; Boyiadzis, M.; Whiteside, T.L. Isolation and characterization of CD34+ blast-derived exosomes in acute myeloid leukemia. PLoS ONE 2014, 9, e103310. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.S.; Muller, L.; Whiteside, T.L.; Boyiadzis, M. Plasma exosomes as markers of therapeutic response in patients with acute myeloid leukemia. Front. Immunol. 2014, 5, 160. [Google Scholar] [CrossRef]
- Boyiadzis, M.; Hong, C.S.; Whiteside, T.L. Evidence for the Role of Biologically Active Exosomes in Acute Myeloid Leukemia Relapse. Blood 2015, 126, 2607. [Google Scholar] [CrossRef]
- Namburi, S.; Broxmeyer, H.E.; Hong, C.S.; Whiteside, T.L.; Boyiadzis, M. DPP4(+) exosomes in AML patients’ plasma suppress proliferation of hematopoietic progenitor cells. Leukemia 2020, 35, 1925–1932. [Google Scholar] [CrossRef]
- Im, A.; Hou, J.Z.; Raptis, A.; Agha, M.; Farah, R.; Redner, R.L.; Sehgal, A.R.; Dorritie, K.A.; Welsh, A.; Johnson, D.E.; et al. Epigenetic priming using decitabine followed by cytarabine as an induction regimen in older patients with newly diagnosed acute myeloid leukemia. Blood 2014, 124, 2265. [Google Scholar] [CrossRef]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Buchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef] [PubMed]
- Dohner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Buchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.S.; Funk, S.; Muller, L.; Boyiadzis, M.; Whiteside, T.L. Isolation of biologically active and morphologically intact exosomes from plasma of patients with cancer. J. Extracell. Vesicles 2016, 5, 29289. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.S.; Sharma, P.; Yerneni, S.S.; Simms, P.; Jackson, E.K.; Whiteside, T.L.; Boyiadzis, M. Circulating exosomes carrying an immunosuppressive cargo interfere with cellular immunotherapy in acute myeloid leukemia. Sci. Rep. 2017, 7, 14684. [Google Scholar] [CrossRef] [PubMed]
- Yerneni, S.S.; Whiteside, T.L.; Weiss, L.E.; Campbell, P.G. Bioprinting exosome-like extracellular vesicle microenvironments. Bioprinting 2019, 2019, e00041. [Google Scholar] [CrossRef]
- Thery, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef]
- Vetsika, E.K.; Sharma, P.; Samaras, I.; Markou, A.; Georgoulias, V.; Whiteside, T.L.; Kotsakis, A. Small Extracellular Vesicles in Pre-Therapy Plasma Predict Clinical Outcome in Non-Small-Cell Lung Cancer Patients. Cancers 2021, 13, 2041. [Google Scholar] [CrossRef]
- Munoz, L.; Nomdedeu, J.F.; Lopez, O.; Carnicer, M.J.; Bellido, M.; Aventin, A.; Brunet, S.; Sierra, J. Interleukin-3 receptor alpha chain (CD123) is widely expressed in hematologic malignancies. Haematologica 2001, 86, 1261–1269. [Google Scholar]
- Testa, U.; Riccioni, R.; Militi, S.; Coccia, E.; Stellacci, E.; Samoggia, P.; Latagliata, R.; Mariani, G.; Rossini, A.; Battistini, A.; et al. Elevated expression of IL-3Ralpha in acute myelogenous leukemia is associated with enhanced blast proliferation, increased cellularity, and poor prognosis. Blood 2002, 100, 2980–2988. [Google Scholar] [CrossRef]
- Testa, U.; Riccioni, R.; Diverio, D.; Rossini, A.; Lo Coco, F.; Peschle, C. Interleukin-3 receptor in acute leukemia. Leukemia 2004, 18, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Cascavilla, N.; Musto, P.; D’Arena, G.; Melillo, L.; Carella, A.M.; Petrilli, M.P.; Sanpaolo, G.; Carotenuto, M. CD117 (c-kit) is a restricted antigen of acute myeloid leukemia and characterizes early differentiative levels of M5 FAB subtype. Haematologica 1998, 83, 392–397. [Google Scholar] [PubMed]
- Muroi, K.; Nakamura, M.; Amemiya, Y.; Suda, T.; Miura, Y. Expression of c-kit receptor (CD117) and CD34 in leukemic cells. Leuk. Lymphoma 1995, 16, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Valverde, L.R.; Matutes, E.; Farahat, N.; Heffernan, A.; Owusu-Ankomah, K.; Morilla, R.; Catovsky, D. C-kit receptor (CD117) expression in acute leukemia. Ann. Hematol. 1996, 72, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; van den Oudenrijn, S.; Bakker, A.Q.; Feller, N.; van Meijer, M.; Bia, J.A.; Jongeneelen, M.A.; Visser, T.J.; Bijl, N.; Geuijen, C.A.; et al. C-type lectin-like molecule-1: A novel myeloid cell surface marker associated with acute myeloid leukemia. Cancer Res. 2004, 64, 8443–8450. [Google Scholar] [CrossRef] [PubMed]
- van Rhenen, A.; van Dongen, G.A.; Kelder, A.; Rombouts, E.J.; Feller, N.; Moshaver, B.; Stigter-van Walsum, M.; Zweegman, S.; Ossenkoppele, G.J.; Jan Schuurhuis, G. The novel AML stem cell associated antigen CLL-1 aids in discrimination between normal and leukemic stem cells. Blood 2007, 110, 2659–2666. [Google Scholar] [CrossRef]
- Hosen, N.; Park, C.Y.; Tatsumi, N.; Oji, Y.; Sugiyama, H.; Gramatzki, M.; Krensky, A.M.; Weissman, I.L. CD96 is a leukemic stem cell-specific marker in human acute myeloid leukemia. Proc. Natl. Acad. Sci. USA 2007, 104, 11008–11013. [Google Scholar] [CrossRef] [PubMed]
- Dohner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef] [PubMed]
- Draganski, E.; Deason, T.; Craig, F.E. Bone Marrow Aspiration and Biopsy Performed by RNs: A Review of Clinical Practice. Am. J. Nurs. 2019, 119, 47–53. [Google Scholar] [CrossRef]
- Stensby, J.D.; Long, J.R.; Hillen, T.J.; Jennings, J.W. Safety of bone marrow aspiration and biopsy in severely thrombocytopenic patients. Skeletal Radiol. 2021, 50, 915–920. [Google Scholar] [CrossRef]
- Bucher, C.M.; Lehmann, T.; Tichelli, A.; Tzankov, A.; Dirnhofer, S.; Passweg, J.; Rovo, A. Comparison of a powered bone marrow biopsy device with a manual system: Results of a prospective randomised controlled trial. J. Clin. Pathol. 2013, 66, 24–28. [Google Scholar] [CrossRef]
- Hjortholm, N.; Jaddini, E.; Halaburda, K.; Snarski, E. Strategies of pain reduction during the bone marrow biopsy. Ann. Hematol. 2013, 92, 145–149. [Google Scholar] [CrossRef]
- Degen, C.; Christen, S.; Rovo, A.; Gratwohl, A. Bone marrow examination: A prospective survey on factors associated with pain. Ann. Hematol. 2010, 89, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Gendron, N.; Zia Chahabi, S.; Poenou, G.; Rivet, N.; Belleville-Rolland, T.; Lemaire, P.; Escuret, A.; Ciaudo, M.; Curis, E.; Gaussem, P.; et al. Pain assessment and factors influencing pain during bone marrow aspiration: A prospective study. PLoS ONE 2019, 14, e0221534. [Google Scholar] [CrossRef] [PubMed]
- Bain, B.J. Morbidity associated with bone marrow aspiration and trephine biopsy—A review of UK data for 2004. Haematologica 2006, 91, 1293–1294. [Google Scholar] [PubMed]
- Tsai, C.S.; Yu, S.C. Inadvertent arterial & venous injury by bone marrow biopsy needle: Case report on rescue embolization techniques. CVIR Endovasc. 2020, 3, 80. [Google Scholar] [CrossRef]
- Wojciechowski, A.; Duckert, M.; Hartmann, J.; Bullinger, L.; Matzdorff, A. Retroperitoneal Hematoma after Bone Marrow Biopsy: The First Cut Should Not Be the Deepest. Oncol. Res. Treat. 2019, 42, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Zarnegar-Lumley, S.; Lange, K.R.; Mathias, M.D.; Nakajima-Hatano, M.; Offer, K.M.; Ogu, U.O.; Ortiz, M.V.; Tan, K.S.; Kellick, M.; Modak, S.; et al. Local Anesthesia With General Anesthesia for Pediatric Bone Marrow Procedures. Pediatrics 2019, 144, e20183829. [Google Scholar] [CrossRef]
- Abdolkarimi, B.; Zareifar, S.; Golestani Eraghi, M.; Saleh, F. Comparison Effect of Intravenous Ketamine with Pethidine for Analgesia and Sedation during Bone Marrow Procedures in Oncologic Children: A Randomized, Double-Blinded, Crossover Trial. Int. J. Hematol. Oncol. Stem Cell Res. 2016, 10, 206–211. [Google Scholar]
- Iannalfi, A.; Bernini, G.; Caprilli, S.; Lippi, A.; Tucci, F.; Messeri, A. Painful procedures in children with cancer: Comparison of moderate sedation and general anesthesia for lumbar puncture and bone marrow aspiration. Pediatr. Blood Cancer 2005, 45, 933–938. [Google Scholar] [CrossRef]
- Short, N.J.; Patel, K.P.; Albitar, M.; Franquiz, M.; Luthra, R.; Kanagal-Shamanna, R.; Wang, F.; Assi, R.; Montalban-Bravo, G.; Matthews, J.; et al. Targeted next-generation sequencing of circulating cell-free DNA vs bone marrow in patients with acute myeloid leukemia. Blood Adv. 2020, 4, 1670–1677. [Google Scholar] [CrossRef]
- Yeh, P.; Dickinson, M.; Ftouni, S.; Hunter, T.; Sinha, D.; Wong, S.Q.; Agarwal, R.; Vedururu, R.; Doig, K.; Fong, C.Y.; et al. Molecular disease monitoring using circulating tumor DNA in myelodysplastic syndromes. Blood 2017, 129, 1685–1690. [Google Scholar] [CrossRef]
- Nakamura, S.; Yokoyama, K.; Shimizu, E.; Yusa, N.; Kondoh, K.; Ogawa, M.; Takei, T.; Kobayashi, A.; Ito, M.; Isobe, M.; et al. Prognostic impact of circulating tumor DNA status post-allogeneic hematopoietic stem cell transplantation in AML and MDS. Blood 2019, 133, 2682–2695. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 28 |
|---|---|
| Age in years, mean (range) | 75.5 (68–83) |
| Sex, N (%) female | 9 (32.1) |
| Cytogenetic risk category, N (%) | |
| Favorable | 1 (3.6) |
| Intermediate | 12 (42.9) |
| Unfavorable | 14 (50.0) |
| Unknown | 1 (3.6) |
| WBC a count (×109/L), mean (range) | 11.4 (0.8–54.8) |
| Platelet count (×109/L), mean (range) | 77.5 (16–354) |
| % blasts in bone marrow, mean (range) | 47.2 (8–94) |
| % blasts in peripheral blood, mean (range) | 18.6 (0–81) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyiadzis, M.; Hong, C.-S.; Yerneni, S.; Im, A.; Diergaarde, B.; Whiteside, T.L. Blast-Derived Small Extracellular Vesicles in the Plasma of Patients with Acute Myeloid Leukemia Predict Responses to Chemotherapy. Biomedicines 2023, 11, 3236. https://doi.org/10.3390/biomedicines11123236
Boyiadzis M, Hong C-S, Yerneni S, Im A, Diergaarde B, Whiteside TL. Blast-Derived Small Extracellular Vesicles in the Plasma of Patients with Acute Myeloid Leukemia Predict Responses to Chemotherapy. Biomedicines. 2023; 11(12):3236. https://doi.org/10.3390/biomedicines11123236
Chicago/Turabian StyleBoyiadzis, Michael, Chang-Sook Hong, Saigopalakrishna Yerneni, Annie Im, Brenda Diergaarde, and Theresa L. Whiteside. 2023. "Blast-Derived Small Extracellular Vesicles in the Plasma of Patients with Acute Myeloid Leukemia Predict Responses to Chemotherapy" Biomedicines 11, no. 12: 3236. https://doi.org/10.3390/biomedicines11123236
APA StyleBoyiadzis, M., Hong, C.-S., Yerneni, S., Im, A., Diergaarde, B., & Whiteside, T. L. (2023). Blast-Derived Small Extracellular Vesicles in the Plasma of Patients with Acute Myeloid Leukemia Predict Responses to Chemotherapy. Biomedicines, 11(12), 3236. https://doi.org/10.3390/biomedicines11123236