

Allopurinol versus Febuxostat: A New Approach for the Management of Hepatic Steatosis in Metabolic Dysfunction-Associated Steatotic Liver Disease

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Eligibility (Inclusion and Exclusion Criteria)
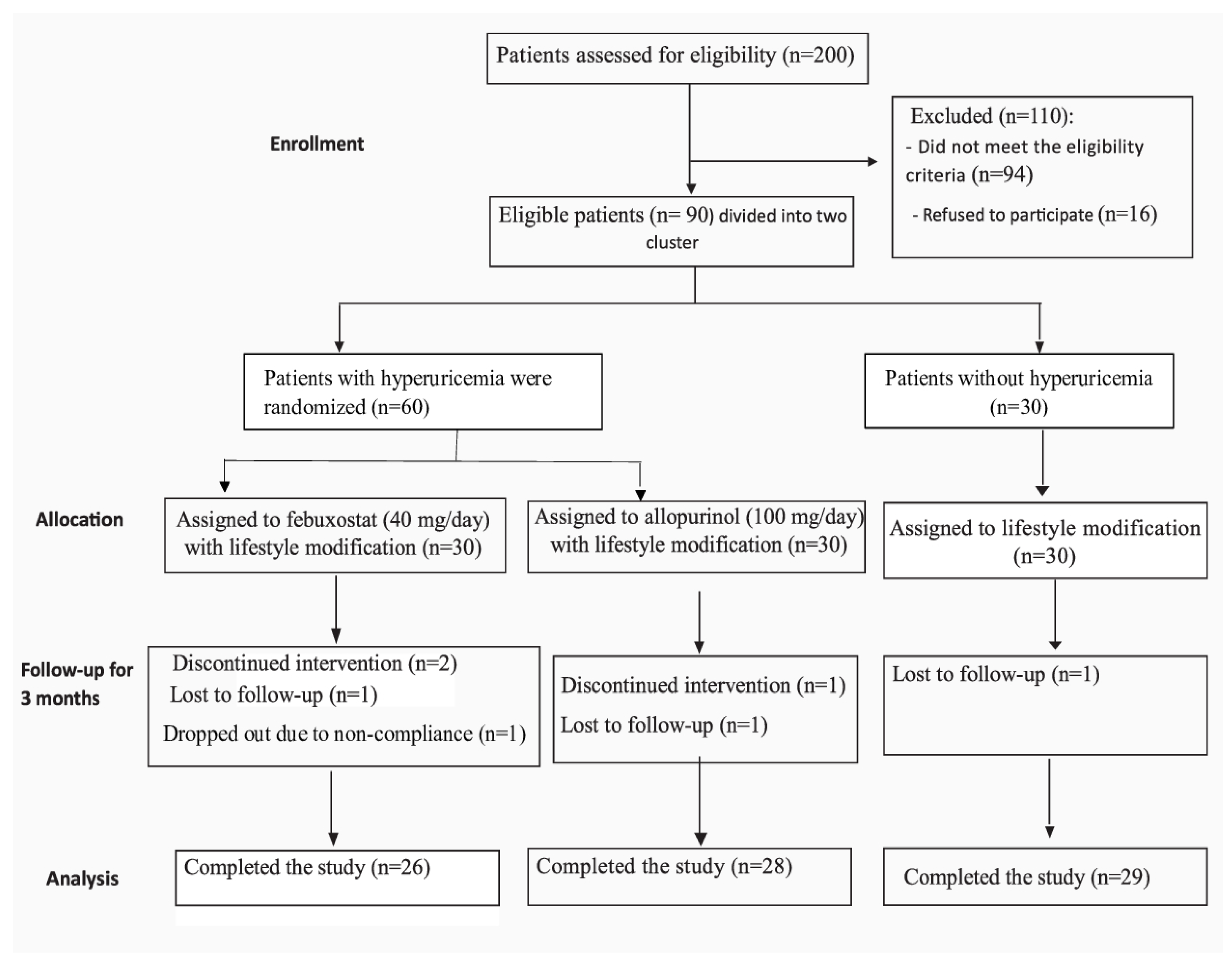
2.3. Enrollment and Allocation
2.4. Treatment Intervention
2.5. Clinical and Laboratory Data
2.6. Follow Up
2.7. Safety and Tolerability
2.8. Sample Size Calculations
2.9. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Liver Steatosis (CAP Score)
3.3. Adverse Events
3.4. Hepatotoxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of liver disease: 2023 update. J. Hepatol. 2023, 79, 516–537. [Google Scholar] [CrossRef] [PubMed]
- Roeb, E. Excess Body Weight and Metabolic (Dysfunction)-Associated Fatty Liver Disease (MAFLD). Visc. Med. 2021, 37, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Paul, J. Recent advances in non-invasive diagnosis and medical management of non-alcoholic fatty liver disease in adult. Egypt. Liver J. 2020, 10, 37. [Google Scholar] [CrossRef]
- Tsai, E.; Lee, T.P. Diagnosis and Evaluation of Nonalcoholic Fatty Liver Disease/Nonalcoholic Steatohepatitis, Including Noninvasive Biomarkers and Transient Elastography. Clin. Liver Dis. 2018, 22, 73–92. [Google Scholar] [CrossRef]
- Shrestha, R.; Kc, S.; Thapa, P.; Pokharel, A.; Karki, N.; Jaishi, B. Estimation of Liver Fat by FibroScan in Patients with Nonalcoholic Fatty Liver Disease. Cureus 2021, 13, e16414. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Ahuja, W.; Wirunsawanya, K.; Wijarnpreecha, K.; Ungprasert, P. Hyperuricemia is associated with nonalcoholic fatty liver disease activity score in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1031–1035. [Google Scholar] [CrossRef]
- Yang, C.; He, Q.; Chen, Z.; Qin, J.-J.; Lei, F.; Liu, Y.-M.; Liu, W.; Chen, M.-M.; Sun, T.; Zhu, Q.; et al. A Bidirectional Relationship Between Hyperuricemia and Metabolic Dysfunction-Associated Fatty Liver Disease. Front. Endocrinol. 2022, 13, 821689. [Google Scholar] [CrossRef]
- Timsans, J.; Kauppi, J.E.; Kerola, A.M.; Lehto, T.M.; Kautiainen, H.; Kauppi, M.J. Hyperuricaemia: Prevalence and association with mortality in an elderly Finnish population. BMJ Open 2023, 13, 72110. [Google Scholar] [CrossRef]
- Liu, N.; Xu, H.; Sun, Q.; Yu, X.; Chen, W.; Wei, H.; Jiang, J.; Xu, Y.; Lu, W. The Role of Oxidative Stress in Hyperuricemia and Xanthine Oxidoreductase (XOR) Inhibitors. Oxid. Med. Cell. Longev. 2021, 2021, 1470380. [Google Scholar] [CrossRef]
- Abou-Rjeileh, U.; Contreras, G.A. Redox Regulation of Lipid Mobilization in Adipose Tissues. Antioxidants 2021, 10, 1090. [Google Scholar] [CrossRef]
- Guo, X.; Yin, X.; Liu, Z.; Wang, J. Non-Alcoholic Fatty Liver Disease (NAFLD) Pathogenesis and Natural Products for Prevention and Treatment. Int. J. Mol. Sci. 2022, 23, 15489. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Xu, C.; Lin, Y.; Lu, C.; Li, D.; Sang, J.; He, H.; Liu, X.; Li, Y.; Yu, C. Uric acid regulates hepatic steatosis and insulin resistance through the NLRP3 inflammasome-dependent mechanism. J. Hepatol. 2016, 64, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Mu, J.; Chen, Q.I.; Li, X.; Liu, H. The involvement and mechanism of febuxostat in non-alcoholic fatty liver disease cells. J. Biol. Regul. Homeost. Agents 2018, 32, 545–551. [Google Scholar] [PubMed]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Leoni, S.; Tovoli, F.; Napoli, L.; Serio, I.; Ferri, S.; Bolondi, L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J. Gastroenterol. 2018, 24, 3361. [Google Scholar] [CrossRef] [PubMed]
- Kwak, M.-S.; Kim, D. Non-alcoholic fatty liver disease and lifestyle modifications, focusing on physical activity. Korean J. Intern Med. 2018, 33, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, K.; Adams, L.A. Lifestyle modification in NAFLD/NASH: Facts and figures. JHEP Rep. 2019, 1, 468–479. [Google Scholar] [CrossRef]
- Horder, M.; Elser, R.C.; Gerhardt, W.; Mathieu, M.; Sampson, E.J. IFCC methods for the measurement of catalytic concentrations of enzymes: Part 3. IFCC method for alanine aminotransferase (L-alanine: 2-oxoglutarate aminotransferase, EC 2.6.1.2). Clin. Chim. Acta 1980, 105, 147–154. [Google Scholar] [CrossRef]
- Chehrehgosha, H.; Sohrabi, M.R.; Ismail-Beigi, F.; Malek, M.; Babaei, M.R.; Zamani, F.; Ajdarkosh, H.; Khoonsari, M.; Fallah, A.E.; Khamseh, M.E. Empagliflozin Improves Liver Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Diabetes Ther. 2021, 12, 843–861. [Google Scholar] [CrossRef]
- Zenovia, S.; Stanciu, C.; Sfarti, C.; Singeap, A.-M.; Cojocariu, C.; Girleanu, I.; Dimache, M.; Chiriac, S.; Muzica, C.M.; Nastasa, R.; et al. Vibration-Controlled Transient Elastography and Controlled Attenuation Parameter for the Diagnosis of Liver Steatosis and Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Diagnostics 2021, 11, 787. [Google Scholar] [CrossRef]
- Lomonaco, R.; Leiva, E.G.; Bril, F.; Shrestha, S.; Mansour, L.; Budd, J.; Romero, J.P.; Schmidt, S.; Chang, K.-L.; Samraj, G.; et al. Advanced Liver Fibrosis Is Common in Patients with Type 2 Diabetes Followed in the Outpatient Setting: The Need for Systematic Screening. Diabetes Care 2021, 44, 399. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Won, J.; Kwon, O.C.; Lee, S.S.; Oh, J.S.; Kim, Y.-G.; Lee, C.-K.; Yoo, B.; Hong, S. Hepatic safety of febuxostat compared with allopurinol in gout patients with fatty liver disease. J. Rheumatol. 2019, 46, 527–531. [Google Scholar] [CrossRef]
- Abhishek, A.; Roddy, E.; Doherty, M. Gout—A guide for the general and acute physicians. Clin. Med. 2017, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wan, X.; Xu, L.; Weng, H.; Yan, M.; Miao, M.; Sun, Y.; Xu, G.; Dooley, S.; Li, Y.; et al. Xanthine oxidase in non-alcoholic fatty liver disease and hyperuricemia: One stone hits two birds. J. Hepatol. 2015, 62, 1412–1419. [Google Scholar] [CrossRef]
- Allameh, A.; Niayesh-Mehr, R.; Aliarab, A.; Sebastiani, G.; Pantopoulos, K. Oxidative Stress in Liver Pathophysiology and Disease. Antioxidants 2023, 12, 1653. [Google Scholar] [CrossRef] [PubMed]
- Vega, S.; Neira, J.L.; Marcuello, C.; Lostao, A.; Abian, O.; Velazquez-Campoy, A. NS3 protease from hepatitis C virus: Biophysical studies on an intrinsically disordered protein domain. Int. J. Mol. Sci. 2013, 14, 13282–13306. [Google Scholar] [CrossRef] [PubMed]
- Nakatsu, Y.; Seno, Y.; Kushiyama, A.; Sakoda, H.; Fujishiro, M.; Katasako, A.; Mori, K.; Matsunaga, Y.; Fukushima, T.; Kanaoka, R.; et al. The xanthine oxidase inhibitor febuxostat suppresses development of nonalcoholic steatohepatitis in a rodent model. Am. J. Physiol. Gastrointest. Liver Physiol. 2015, 309, G42–G51. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, T.; Nagata, N.; Shimakami, T.; Shirakura, T.; Matsui, C.; Ni, Y.; Zhuge, F.; Xu, L.; Chen, G.; Nagashimada, M.; et al. Xanthine oxidase inhibition attenuates insulin resistance and diet-induced steatohepatitis in mice. Sci. Rep. 2020, 10, 815. [Google Scholar] [CrossRef]
- Shimizu, M.; Suzuki, K.; Kato, K.; Jojima, T.; Iijima, T.; Murohisa, T.; Iijima, M.; Takekawa, H.; Usui, I.; Hiraishi, H.; et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes. Metab. 2019, 21, 285–292. [Google Scholar] [CrossRef]
- Feng, Y.; Zheng, S.; Liu, L.; Yang, Y. Association of serum uric acid with hepatic steatosis detected by controlled attenuation parameter in the United States population. Lipids Health Dis. 2023, 22, 76. [Google Scholar] [CrossRef]
- LiverTox: Clinical and Research Information on Drug—Induced Liver Injury; Bookshelf ID: NBK547852; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. Available online: https://pubmed.ncbi.nlm.nih.gov/31643176/ (accessed on 27 May 2023).




{kind=link}
{kind=link}
{kind=link}
| Variable | Lifestyle, (N = 29) | Allopurinol, 100 mg/Day (N = 28) | Febuxostat, 40 mg/Day (N = 26) | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | p-Value * | Before | After | p-Value * | Before | After | p-Value * | Before | After | |
| Age—years. | 46.0 ± 10.3 | 48.1 ± 11.0 | 47.3 ± 11.6 | 0.764 a | |||||||
| Female sex (%) | (89.7) | (67.9) | (76.9) | 0.133 b | |||||||
| Weight (kg) | 94.2 ± 10.3 | 92.75 ± 15.34 | 0.029 d | 98.0 ± 18.6 | 96.0 ± 18.1 | 0.001 d | 100.7 ± 16.5 | 98.69 ± 14.95 | 0.039 d | 0.356 a | 0.401 a |
| BMI (kg/m2) | 36.3 ± 5.1 | 35.8 ± 5.3 | 0.033 d | 36.1 ± 6.6 | 35.4 ± 6.5 | 0.001 d | 37.8 ± 6.2 | 37.1 ± 5.8 | 0.044 d | 0.538 a | 0.554 a |
| WC (cm) | 104.5 ± 9.1 | 103.6 ± 8.7 | 0.034 d | 106.2 ± 10.2 | 105.6 ± 09.2 | 0.038 d | 105.7 ± 9.7 | 104.7 ± 8.9 | 0.032 d | 0.267 a | 0.397 a |
| SCR (mg/dL) | 0.83 ± 0.17 | 0.81 ± 0.13 | 0.387 d | 0.89 ± 0.23 | 0.90 ± 0.14 | 0.789 d | 0.87 ± 0.22 | 0.91 ± 0.18 | 0.289 d | 0.541 a | 0.252 a |
| AST (u/L) | 28.1 ± 11.2 | 25.2 ± 9.8 | 0.056 k | 31.8 ± 15.9 | 30.7 ± 10.3 | 0.289 k | 27.3 ± 11.1 | 30.7 ± 12.1 | 0.162 k | 0.557 | 0.459 c |
| ALT (u/L) | 27.9 ± 10.6 | 26.5 ± 14.0 | 0.153 k | 38.6 ± 25.6 | 33.3 ± 16.1 | 0.858 k | 28.7 ± 13.3 | 26.0 ± 11.0 | 0.545 k | 0.274 | 0.494 c |
| AST/ALT | 1.05 ± 0.33 | 1.05 ± 0.40 | 0.452 k | 0.93 ± 0.32 | 0.98 ± 0.26 | 0.135 k | 1.03 ± 0.38 | 1.22 ± 0.28 | 0.234 k | 0.289 | 0.099 c |
| SUA (mg/dL) | 3.87 ± 0.59 | 4.1 ± 0.90 | 0.090 d | 6.70 ± 0.90 | 4.1 ± 1.10 | <0.001 d | 6.40 ± 0.80 | 3.9 ± 0.80 | <0.001 d | <0.001 a | 0.711 a |
| HbAIc % | 6.4 ± 1.2 | 6.6 ± 1.4 | 6.3 ± 1.02 | 0.253 a | |||||||
| SBP | 119.1 ± 22.6 | 112.3 ± 11.3 | 113.7 ± 14.8 | 0.287 a | |||||||
| DBP | 84.2 ± 4.4 | 85.4 ± 3.5 | 85.3 ± 4.1 | 0.487 a | |||||||
| TC (mg/dL) | 186.9 ± 29.8 | 222.9 ± 63.0 | 199.7 ± 64.2 | 0.065 c | |||||||
| TG (mg/dL) | 180.1 ± 99.4 | 214.0 ± 105.3 | 171.1 ± 63.3 | 0.146 c | |||||||
| HDL (mg/dL) | 43.3 ± 8.4 | 42.9 ± 12.5 | 46.7 ± 14.2 | 0.417 c | |||||||
| LDL (mg/dL) | 111.0 ± 32.0 | 115.2 ± 21.9 | 109.5 ± 32.3 | 0.221 c | |||||||
| CAP Scores | Lifestyle | Allopurinol, 100 mg/Day | Febuxostat, 40 mg/Day | ||||
|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | ||
| S0 | Patient count | 0 | 6 | 0 | 2 | 0 | 5 |
| % within the group | 0.0% | 20.7% | 0.0% | 7.1% | 0.0% | 19.2% | |
| S1 | Patient count | 3 | 2 | 0 | 1 | 4 | 2 |
| % within the group | 10.3% | 6.9% | 0.0% | 3.6% | 15.4% | 7.7% | |
| S2 | Patient count: | 5 | 6 | 3 | 9 | 8 | 8 |
| % within the group | 17.2% | 20.7% | 10.7% | 32.1% | 30.8% | 30.8% | |
| S3 | Patient count: | 21 | 15 | 25 | 16 | 14 | 11 |
| % within the group | 72.4% | 51.7% | 89.3% | 57.1% | 53.8% | 42.3% | |
| Lifestyle (N = 29) | Allopurinol (N = 28) | Febuxostat (N = 26) | Whole Group (N = 83) | |
|---|---|---|---|---|
| BMI change | −0.78 (−3.81–2.22) | −0.73 (−2.94–1.56) | −0.75 (−4.57–5.27) | −0.76 (−4.57–5.27) |
| CAP change | −24.0 (−139.0–87.0) | −38.0 (−113.0–60.0) | −23.0 (−104.0–73.0) | −24.00 (−139.00–87.00) |
| Correlations in each group between CAP change and BMI change. | ||||
| (r) | 0.111 | 0.253 | 0.455 | 0.243 |
| p-value | 0.568 | 0.194 | 0.019 | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Shargi, A.; El Kholy, A.A.; Adel, A.; Hassany, M.; Shaheen, S.M. Allopurinol versus Febuxostat: A New Approach for the Management of Hepatic Steatosis in Metabolic Dysfunction-Associated Steatotic Liver Disease. Biomedicines 2023, 11, 3074. https://doi.org/10.3390/biomedicines11113074
Al-Shargi A, El Kholy AA, Adel A, Hassany M, Shaheen SM. Allopurinol versus Febuxostat: A New Approach for the Management of Hepatic Steatosis in Metabolic Dysfunction-Associated Steatotic Liver Disease. Biomedicines. 2023; 11(11):3074. https://doi.org/10.3390/biomedicines11113074
Chicago/Turabian StyleAl-Shargi, Amani, Amal A. El Kholy, Abdulmoneim Adel, Mohamed Hassany, and Sara M. Shaheen. 2023. "Allopurinol versus Febuxostat: A New Approach for the Management of Hepatic Steatosis in Metabolic Dysfunction-Associated Steatotic Liver Disease" Biomedicines 11, no. 11: 3074. https://doi.org/10.3390/biomedicines11113074
APA StyleAl-Shargi, A., El Kholy, A. A., Adel, A., Hassany, M., & Shaheen, S. M. (2023). Allopurinol versus Febuxostat: A New Approach for the Management of Hepatic Steatosis in Metabolic Dysfunction-Associated Steatotic Liver Disease. Biomedicines, 11(11), 3074. https://doi.org/10.3390/biomedicines11113074