
Multimarker Approach as More Reliable Method Than Single Vitamin D in Relationship with Type 2 Diabetes Mellitus in Montenegrin Postmenopausal Women


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Biochemical Analyses
2.3. Statistical Analysis
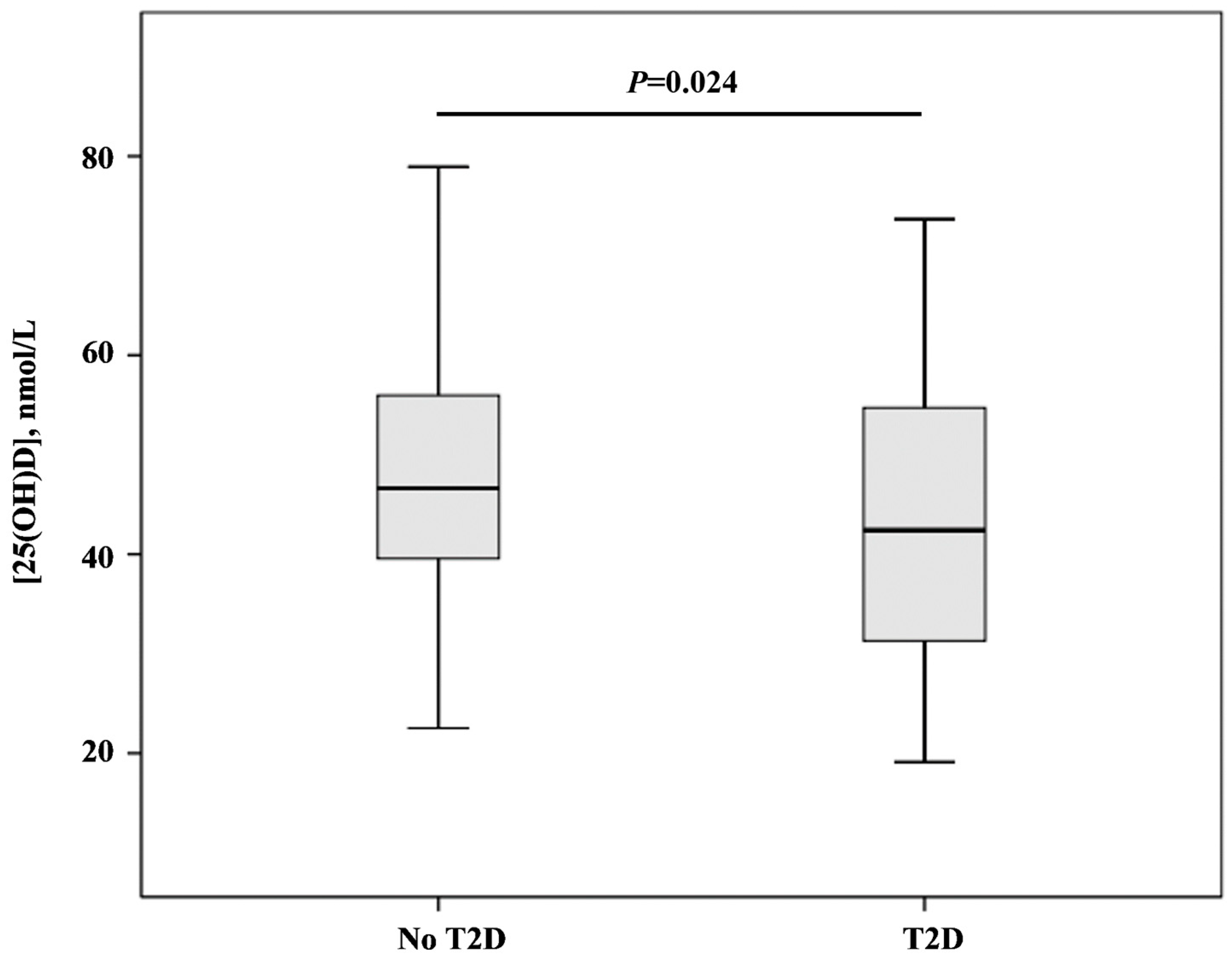
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crescioli, C. The Role of Estrogens and Vitamin D in Cardiomyocyte Protection: A Female Perspective. Biomolecules 2021, 11, 1815. [Google Scholar] [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.H.; Jung, Y. Energy Metabolism Changes and Dysregulated Lipid Metabolism in Postmenopausal Women. Nutrients 2021, 13, 4556. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Chedraui, P.; Lambrinoudaki, I.; Simoncini, T. Menopause: A cardiometabolic transition. Lancet. Diabetes Endocrinol. 2022, 10, 442–456. [Google Scholar] [CrossRef]
- Opoku, A.A.; Abushama, M.; Konje, J.C. Obesity and menopause. Best. Pract. Res. Clin. Obstet. Gynaecol. 2023, 88, 102348. [Google Scholar] [CrossRef]
- Liu, W.; Wu, Z.; Zhu, D.; Chen, G.; Yan, G.; Zhang, S.; Chen, F.; Khan, B.A.; Hou, K. Vitamin D and Lipid Profiles in Postmenopausal Women: A Meta-Analysis and Systematic Review of Randomized Controlled Trials. Front. Mol. Biosci. 2021, 8, 799934. [Google Scholar] [CrossRef]
- Cojic, M.; Kocic, R.; Klisic, A.; Cvejanov-Kezunovic, L.j.; Kavaric, N.; Kocic, G. A novel mechanism of vitamin D anti-inflammatory/antioxidative potential in type 2 diabetic patients on metformin therapy. Arch. Med. Sci. 2020, 16, 1004–1012. [Google Scholar] [CrossRef] [PubMed]
- Cojic, M.; Kocic, R.; Klisic, A.; Kocic, G. The effects of vitamin D supplementation on metabolic and oxidative stress markers in patients with type 2 diabetes: A 6-Month follow up randomized controlled study. Front. Endocrinol. 2021, 12, 610893. [Google Scholar] [CrossRef]
- Chen, X.; Chu, C.; Doebis, C.; von Baehr, V.; Hocher, B. Sex-Dependent Association of Vitamin D with Insulin Resistance in Humans. J. Clin. Endocrinol. Metab. 2021, 106, e3739–e3747. [Google Scholar] [CrossRef]
- Wang, W.; Ye, S.; Qian, L.; Xing, X. Sex-Specific Association of Serum 25-Hydroxyvitamin D3 with Insulin Resistance in Chinese Han Patients with Newly Diagnosed Type 2 Diabetes Mellitus. J. Nutr. Sci. Vitaminol. 2018, 64, 173–178. [Google Scholar] [CrossRef]
- Ganji, V.; Sukik, A.; Alaayesh, H.; Rasoulinejad, H.; Shraim, M. Serum vitamin D concentrations are inversely related to prevalence of metabolic syndrome in Qatari women. Biofactors 2020, 46, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.; Mikhail, M.; Dhaliwal, R.; Shieh, A.; Usera, G.; Stolberg, A.; Ragolia, L.; Islam, S. Free 25(OH)D and the Vitamin D Paradox in African Americans. J. Clin. Endocrinol. Metab. 2015, 100, 3356–3363. [Google Scholar] [CrossRef]
- Alharazy, S.; Alissa, E.; Lanham-New, S.; Naseer, M.I.; Chaudhary, A.G.; Robertson, M.D. Association between vitamin D and glycaemic parameters in a multi-ethnic cohort of postmenopausal women with type 2 diabetes in Saudi Arabia. BMC. Endocr. Disord. 2021, 21, 162. [Google Scholar] [CrossRef]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, diabetes, and ethnicity in the Third National Health and Nutrition Examination Survey. Diabetes Care 2004, 27, 2813–2818. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Somma, C.D.; Laudisio, D.; Salzano, C.; Pugliese, G.; de Alteriis, G.; Colao, A.; Savastano, S. Sex Differences of Vitamin D Status across BMI Classes: An Observational Prospective Cohort Study. Nutrients 2019, 11, 3034. [Google Scholar] [CrossRef]
- Kabadi, S.M.; Lee, B.K.; Liu, L. Joint effects of obesity and vitamin D insufficiency on insulin resistance and type 2 diabetes: Results from the NHANES 2001–2006. Diabetes Care 2012, 35, 2048–2054. [Google Scholar] [CrossRef] [PubMed]
- Tzotzas, T.; Papadopoulou, F.G.; Tziomalos, K.; Karras, S.; Gastaris, K.; Perros, P.; Krassas, G.E. Rising serum 25-hydroxy-vitamin D levels after weight loss in obese women correlate with improvement in insulin resistance. J Clin Endocrinol Metab. 2010, 95, 4251–4257. [Google Scholar] [CrossRef]
- Seferović, P.; Farmakis, D.; Bayes-Genis, A.; Ben Gal, T.; Böhm, M.; Chioncel, O.; Ferrari, R.; Filippatos, G.; Hill, L.; Jankowska, E.; et al. Biomarkers for the prediction of heart failure and cardiovascular events in patients with type 2 diabetes: A position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2022, 24, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef]
- Klisic, A.; Radoman Vujačić, I.; Kostadinovic, J.; Ninic, A. The correlation of metabolic and renal biomarkers with vitamin D status in postmenopausal women. J. Med. Biochem. 2023, 42, 1–9. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Drzewoski, J.; Śliwińska, A. The Molecular Mechanisms by Which Vitamin D Prevents Insulin Resistance and Associated Disorders. Int. J. Mol. Sci. 2020, 21, 6644. [Google Scholar] [CrossRef] [PubMed]
- Guillot, X.; Semerano, L.; Saidenberg-Kermanac'h, N.; Falgarone, G.; Boissier, M.C. Vitamin D and inflammation. Joint. Bone. Spine. 2010, 77, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Yang, Z.; Wang, L.; Han, Y.; Peng, C.; Yan, C.; Yan, D. Metabolite biomarkers of type 2 diabetes mellitus and pre-diabetes: A systematic review and meta-analysis. BMC. Endocr. Disord. 2020, 20, 174. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | No T2D | T2D | p |
|---|---|---|---|
| Postmenopausal women, N | 116 | 48 | |
| Age, years | 57.22 ± 4.66 | 63.15 ± 7.46 | <0.001 |
| BMI, kg/m2 * | 25.55 (22.85–28.25) | 29.43 (26.35–32.79) | <0.001 |
| WC, cm * | 86.5 (78.0–95.0) | 99.5 (94.0–105.5) | <0.001 |
| SBP, mmHg * | 129 (110–147) | 133 (121–143) | 0.142 |
| DBP, mmHg * | 84 (70–95) | 79 (73–83) | 0.191 |
| Hypertension, N (%) | 45 (38.8) | 48 (100) | <0.001 |
| Smoking status, N (%) | 0 (0) | 16 (33.3) | <0.001 |
| Menopause duration, years | 5 (2–10) | 14 (8–19) | <0.001 |
| MetS, N (%) | 31 (26.7) | 48 (100) | <0.001 |
| Diabetes duration, years | - | 6 (3–8) | - |
| TC, mmol/L | 6.48 ± 1.06 | 5.66 ± 1.27 | <0.001 |
| HDL-c, mmol/L | 1.72 (1.40–2.00) | 1.37 (1.15–1.55) | <0.001 |
| LDL-c, mmol/L | 4.11 (3.60–4.80) | 3.35 (2.78–4.19) | <0.001 |
| TG, mmol/L * | 1.19 (0.90–1.68) | 1.78 (1.31–2.26) | <0.001 |
| Glucose, mmol/L * | 5.2 (5.0–5.55) | 7.5 (6.60–8.35) | <0.001 |
| Insulin, μIU/L * | 5.89 (4.28–7.98) | 11.72 (8.56–16.53) | <0.001 |
| HsCRP, mg/L * | 0.93 (0.43–1.97) | 1.65 (0.69–3.03) | 0.001 |
| Variable | Glucose, mmol/L | HbA1c, % | ||
|---|---|---|---|---|
| ρ | p | ρ | p | |
| Age, years | 0.415 | <0.001 | 0.404 | <0.001 |
| BMI, kg/m2 | 0.427 | <0.001 | 0.642 | <0.001 |
| Waist circumference, cm | 0.497 | <0.001 | 0.682 | <0.001 |
| SBP, mmHg | 0.299 | <0.001 | 0.390 | <0.001 |
| DBP, mmHg | 0.116 | 0.147 | 0.229 | 0.004 |
| Menopause duration, years | 0.076 | 0.416 | 0.098 | 0.298 |
| TC, mmol/L | −0.201 | 0.010 | −0.130 | 0.097 |
| HDL-c, mmol/L | −0.379 | <0.001 | −0.337 | <0.001 |
| LDL-c, mmol/L | −0.168 | 0.031 | −0.111 | 0.156 |
| TG, mmol/L | 0.383 | <0.001 | 0.332 | <0.001 |
| HsCRP, mg/L | 0.257 | 0.001 | 0.401 | <0.001 |
| [25(OH)D], nmol/L | −0.175 | 0.025 | −0.302 | <0.001 |
| Factors | Variables (Loadings) | Factor Variability |
|---|---|---|
| Age-glycometabolic-related factor | Age (0.846) Glucose (0.767) Insulin (0.658) | 25% |
| Obesity-inflammation-related factor | HsCRP (0.801) WC (0.746) [25(OH)D] (−0.623) | 22% |
| Lipid-related factor | TG (0.826) HDL-c (−0.698) LDL-c (0.634) | 19% |
| Factors | p for the Difference between No T2D and T2D |
|---|---|
| Age-glycometabolic-related factor | <0.001 |
| Obesity-inflammation-related factor | 0.002 |
| Lipid-related factor | 0.050 |
| Predictors | Unadjusted OR (95%CI) | p | Nagelkerke R2 |
|---|---|---|---|
| Age-glycometabolic-related factor | 11.321 (5.369–23.874) | <0.001 | 0.608 |
| Obesity-inflammation-related factor | 2.079 (1.377–3.137) | <0.001 | 0.130 |
| Lipid-related factor | 1.423 (1.010–2.005) | 0.044 | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klisic, A.; Cojic, M.; Patoulias, D.; Ninic, A. Multimarker Approach as More Reliable Method Than Single Vitamin D in Relationship with Type 2 Diabetes Mellitus in Montenegrin Postmenopausal Women. Biomedicines 2023, 11, 2610. https://doi.org/10.3390/biomedicines11102610
Klisic A, Cojic M, Patoulias D, Ninic A. Multimarker Approach as More Reliable Method Than Single Vitamin D in Relationship with Type 2 Diabetes Mellitus in Montenegrin Postmenopausal Women. Biomedicines. 2023; 11(10):2610. https://doi.org/10.3390/biomedicines11102610
Chicago/Turabian StyleKlisic, Aleksandra, Milena Cojic, Dimitrios Patoulias, and Ana Ninic. 2023. "Multimarker Approach as More Reliable Method Than Single Vitamin D in Relationship with Type 2 Diabetes Mellitus in Montenegrin Postmenopausal Women" Biomedicines 11, no. 10: 2610. https://doi.org/10.3390/biomedicines11102610
APA StyleKlisic, A., Cojic, M., Patoulias, D., & Ninic, A. (2023). Multimarker Approach as More Reliable Method Than Single Vitamin D in Relationship with Type 2 Diabetes Mellitus in Montenegrin Postmenopausal Women. Biomedicines, 11(10), 2610. https://doi.org/10.3390/biomedicines11102610