
Fatigue in Multiple Sclerosis Is Associated with Reduced Expression of Interleukin-10 and Worse Prospective Disease Activity

 , , , , , , ,
, , , , , , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. RR-MS Patients
2.2. MRI Examination
2.3. CSF Collection and Analysis
2.4. Blood Collection and Analysis of Peripheral Inflammatory Biomarkers
2.5. Statistical Analysis
3. Results
3.1. Fatigue and Clinical Characteristics at the Time of MS Diagnosis
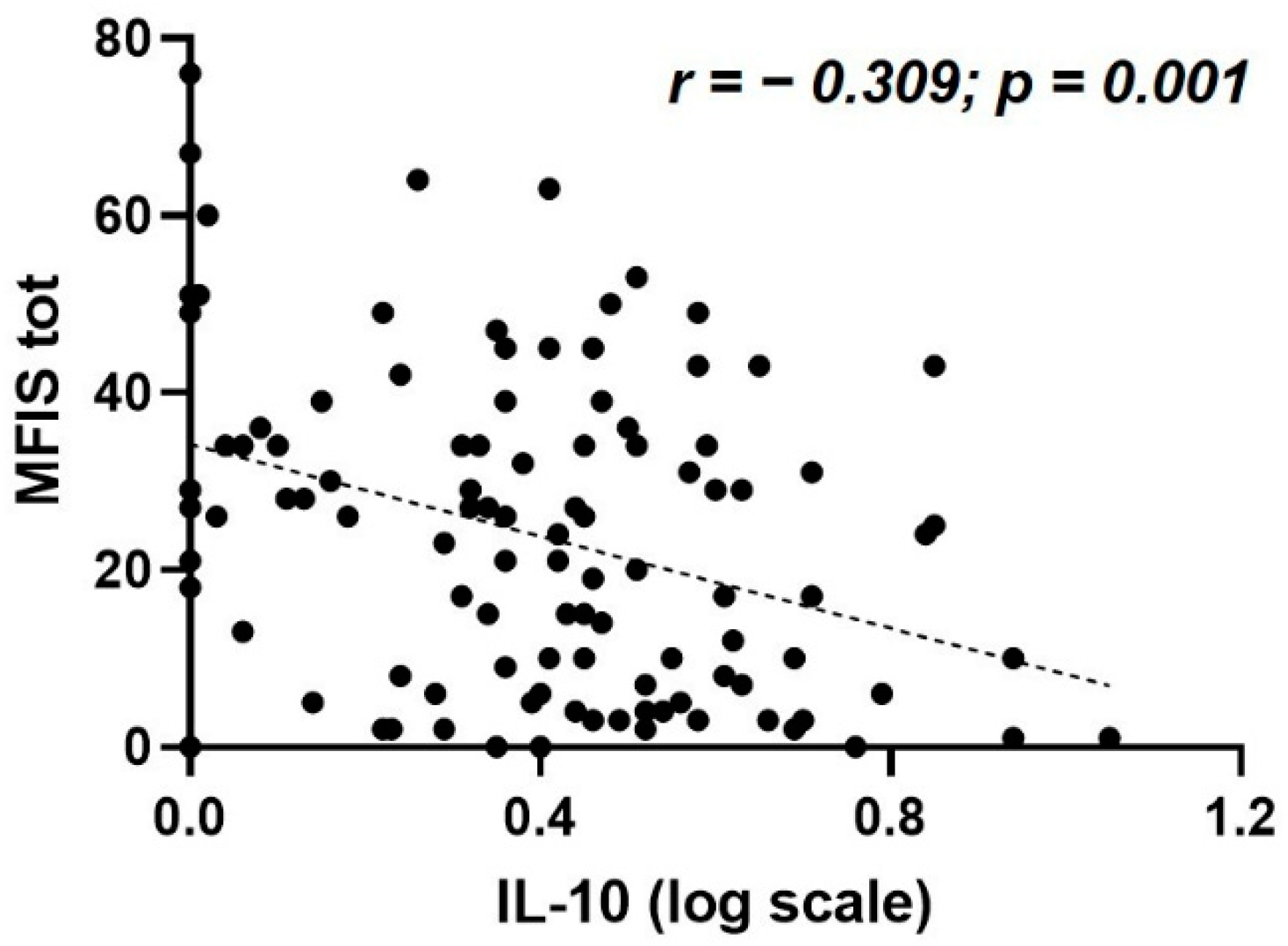
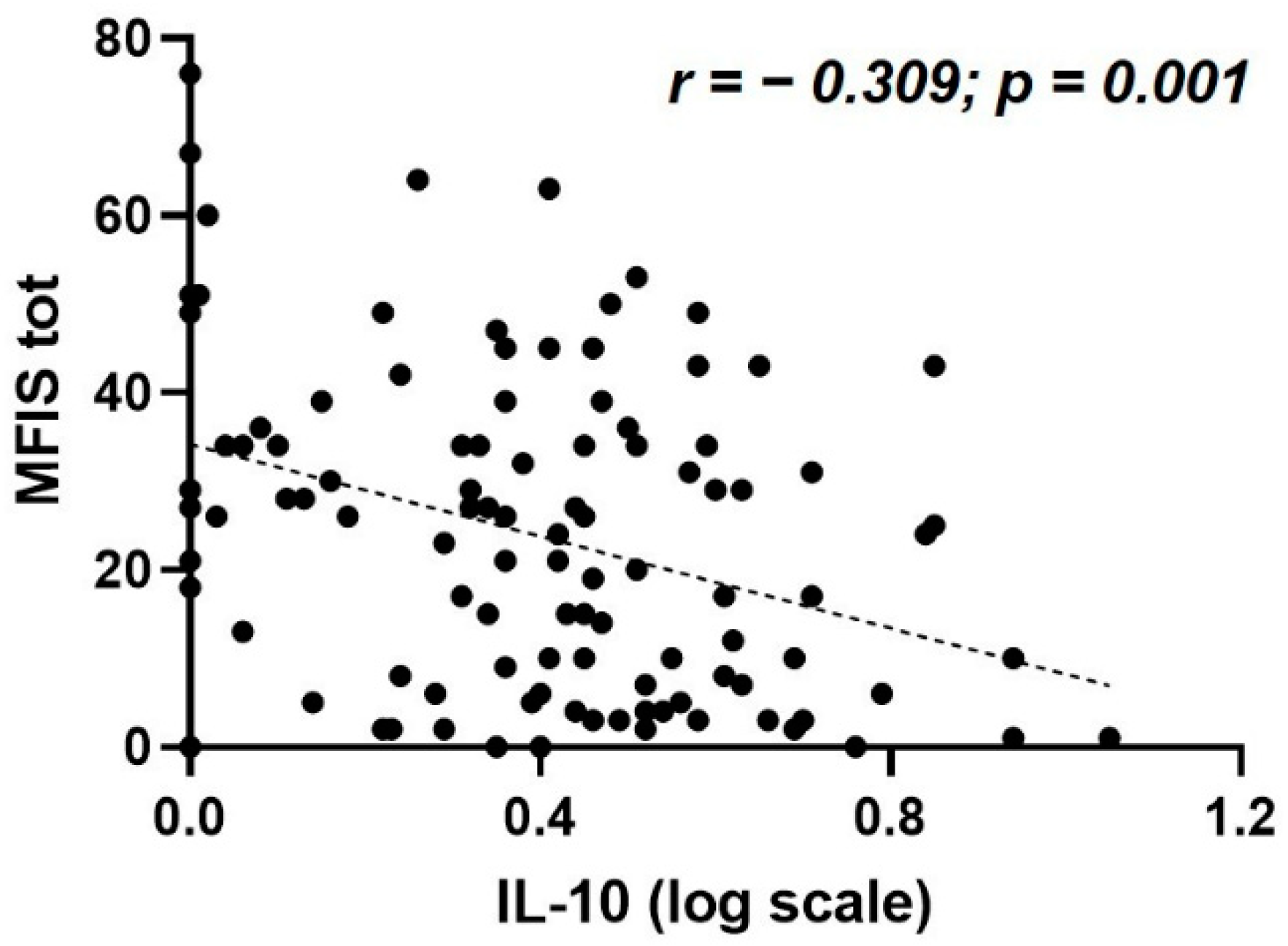
3.2. Fatigue Is Associated with Reduced IL-10 CSF Expression
3.3. Fatigue Is not Associated with Peripheral Inflammation
3.4. Baseline Fatigue Predicts NEDA-3 after One Year Follow-Up
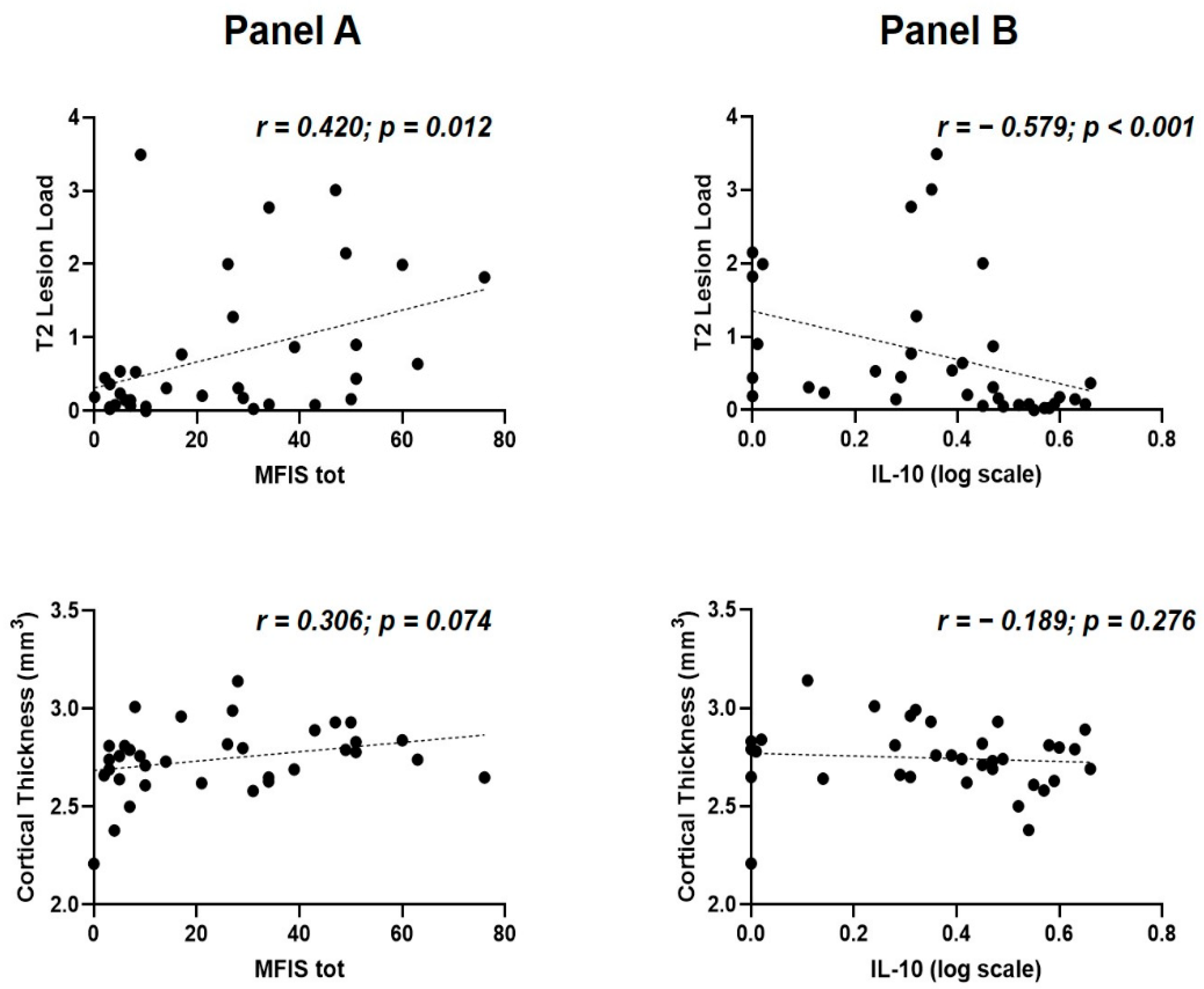
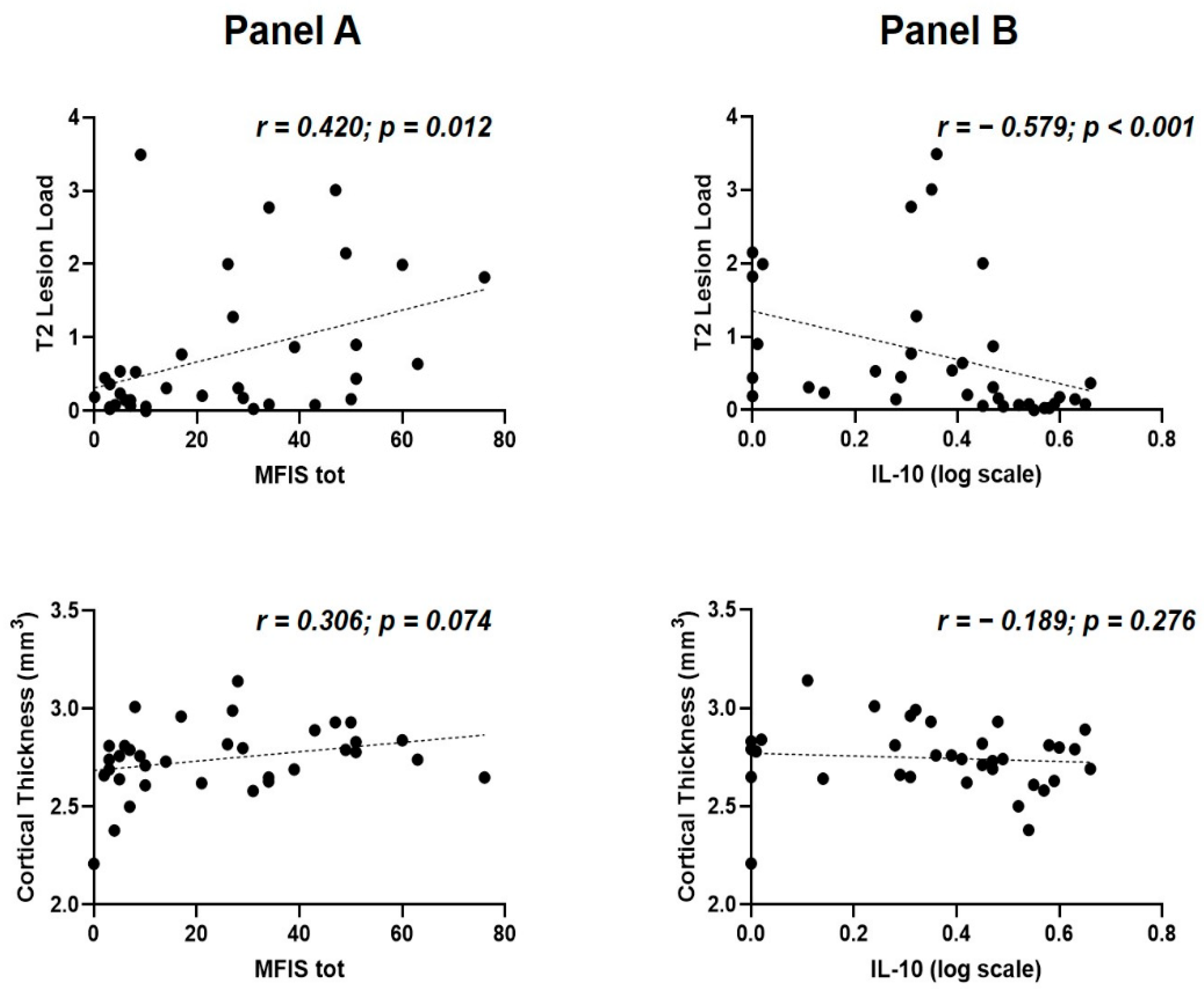
3.5. Correlations between Structural MRI Measures, Fatigue, and CSF IL-10 Levels at the Time of MS Diagnosis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lassmann, H.; Bradl, M. Multiple sclerosis: Experimental models and reality. Acta Neuropathol. 2017, 133, 223–244. [Google Scholar] [CrossRef] [PubMed]
- Herring, T.E.; Alschuler, K.N.; Knowles, L.M.; Phillips, K.M.; Morean, W.M.; Turner, A.P.; Ehde, D.M. Differences in correlates of fatigue between relapsing and progressive forms of multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 54, 103109. [Google Scholar] [CrossRef] [PubMed]
- Patrick, E.; Christodoulou, C.; Krupp, L.; New York State MS Consortium. Longitudinal correlates of fatigue in multiple sclerosis. Mult. Scler. 2009, 15, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Manjaly, Z.M.; Harrison, N.A.; Critchley, H.D.; Do, C.T.; Stefanics, G.; Wenderoth, N.; Lutterotti, A.; Müller, A.; Stephan, K.E. Pathophysiological and cognitive mechanisms of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2019, 90, 642–651. [Google Scholar] [CrossRef]
- Dantzer, R.; Heijnen, C.J.; Kavelaars, A.; Laye, S.; Capuron, L. The neuroimmune basis of fatigue. Trends Neurosci. 2014, 37, 39–46. [Google Scholar] [CrossRef]
- Ramsey-Goldman, R.; Rothrock, N. Fatigue in systemic lupus erythematosus and rheumatoid arthritis. PM R 2010, 2, 384–392. [Google Scholar] [CrossRef]
- Morris, G.; Maes, M. Mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome explained by activated immuno-inflammatory, oxidative and nitrosative stress pathways. Metab. Brain Dis. 2014, 29, 19–36. [Google Scholar] [CrossRef]
- Heesen, C.; Nawrath, L.; Reich, C.; Bauer, N.; Schulz, K.H.; Gold, S.M. Fatigue in multiple sclerosis: An example of cytokine mediated sickness behaviour? J. Neurol. Neurosurg. Psychiatry 2006, 77, 34–39. [Google Scholar] [CrossRef]
- Lee, Y.C.; Frits, M.L.; Iannaccone, C.K.; Weinblatt, M.E.; Shadick, N.A.; Williams, D.A.; Cui, J. Subgrouping of patients with rheumatoid arthritis based on pain, fatigue, inflammation, and psychosocial factors. Arthritis Rheumatol. 2014, 66, 2006–2014. [Google Scholar] [CrossRef]
- Flachenecker, P.; Bihler, I.; Weber, F.; Gottschalk, M.; Toyka, K.V.; Rieckmann, P. Cytokine mRNA expression in patients with multiple sclerosis and fatigue. Mult. Scler. 2004, 10, 165–169. [Google Scholar] [CrossRef]
- Alvarenga-Filho, H.; Salles, M.; Hygino, J.; Ferreira, T.B.; Sacramento, P.M.; Monteiro, C.; Vasconcelos, C.C.; Alvarenga, R.M.; Bento, C.A. Fatigue favors in vitro Th1 and Th17-like cell expansion and reduces corticoid sensitivity in MS patients. J. Neuroimmunol. 2017, 303, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, A.; Van de Geer-Peeters, W.; De Groot, V.; Teunissen, C.E.; Beckerman, H.; TREFAMS-ACE Study Group. Fatigue in patients with multiple sclerosis: Is it related to pro- and anti-inflammatory cytokines? Dis. Markers 2015, 2015, 758314. [Google Scholar] [CrossRef] [PubMed]
- Akcali, A.; Zengin, F.; Aksoy, S.N.; Zengin, O. Fatigue in Multiple Sclerosis: Is it related to cytokines and hypothalamic-pituitary-adrenal axis? Mult. Scler. Relat. Disord. 2017, 15, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Iriarte, J.; Subirá, M.L.; Castro, P. Modalities of fatigue in multiple sclerosis: Correlation with clinical and biological factors. Mult. Scler. 2000, 6, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Thompson, A.J.; Miller, D.H.; Thompson, E.J. Fatigue is not associated with raised inflammatory markers in multiple sclerosis. Neurology 2001, 57, 676–681. [Google Scholar] [CrossRef]
- Yaldizli, O.; Kumar, M.; Vago, S.; Kreuzfelder, E.; Limmroth, V.; Putzki, N. Fatigue is not associated with impaired function of regulatory T cells in untreated patients with multiple sclerosis. Eur. Neurol. 2009, 62, 321–326. [Google Scholar] [CrossRef]
- Patejdl, R.; Penner, I.K.; Noack, T.K.; Zettl, U. Multiple sclerosis and fatigue: A review on the contribution of inflammation and immune-mediated neurodegeneration. Autoimmun. Rev. 2016, 15, 210–220. [Google Scholar] [CrossRef]
- Stampanoni Bassi, M.; Iezzi, E.; Landi, D.; Monteleone, F.; Gilio, L.; Simonelli, I.; Musella, A.; Mandolesi, G.; De Vito, F.; Furlan, R.; et al. Delayed treatment of MS is associated with high CSF levels of IL-6 and IL-8 and worse future disease course. J. Neurol. 2018, 265, 2540–2547. [Google Scholar] [CrossRef]
- Runia, T.F.; Jafari, N.; Siepman, D.A.; Hintzen, R.Q. Fatigue at time of CIS is an independent predictor of a subsequent diagnosis of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 543–546. [Google Scholar] [CrossRef]
- Cavallari, M.; Palotai, M.; Glanz, B.I.; Egorova, S.; Prieto, J.C.; Healy, B.C.; Chitnis, T.; Guttmann, C.R. Fatigue predicts disease worsening in relapsing-remitting multiple sclerosis patients. Mult. Scler. 2016, 22, 1841–1849. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in four different European countries. Mult. Scler. 2005, 11, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. 2002, 8, 523–526. [Google Scholar] [CrossRef]
- Sica, C.; Ghisi, M. The Italian versions of the Beck Anxiety Inventory and the Beck Depression Inventory-II: Psychometric properties and discriminant power. In Leading-Edge Psychological Tests and Testing Research; Lange, M.A., Ed.; Nova Science Publishers: New York, NY, USA, 2007; pp. 27–50. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Manuale Dell’adattamento Italiano dello STAI di Spielberger, Forma Y; Organizzazioni Speciali: Firenze, Italy, 1989. [Google Scholar]
- Havrdova, E.; Galetta, S.; Hutchinson, M.; Stefoski, D.; Bates, D.; Polman, C.H.; O’Connor, P.W.; Giovannoni, G.; Phillips, J.T.; Lublin, F.D.; et al. Effect of natalizumab on clinical and radiological disease activity in multiple sclerosis: A retrospective analysis of the Natalizumab Safety and Efficacy in Relapsing-Remitting Multiple Sclerosis (AFFIRM) study. Lancet Neurol. 2009, 8, 254–260. [Google Scholar] [CrossRef]
- Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2019, 92, 112. [CrossRef]
- Hasselbalch, I.C.; Søndergaard, H.B.; Koch-Henriksen, N.; Olsson, A.; Ullum, H.; Sellebjerg, F.; Oturai, A.B. The neutrophil-to-lymphocyte ratio is associated with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2018, 4, 2055217318813183. [Google Scholar] [CrossRef]
- Biberacher, V.; Schmidt, P.; Selter, R.C.; Pernpeinter, V.; Kowarik, M.C.; Knier, B.; Buck, D.; Hoshi, M.M.; Korn, T.; Berthele, A.; et al. Fatigue in multiple sclerosis: Associations with clinical, MRI and CSF parameters. Mult. Scler. 2018, 24, 1115–1125. [Google Scholar] [CrossRef]
- Brenner, P.; Granqvist, M.; Königsson, J.; Al Nimer, F.; Piehl, F.; Jokinen, J. Depression and fatigue in multiple sclerosis: Relation to exposure to violence and cerebrospinal fluid immunomarkers. Psychoneuroendocrinology 2018, 89, 53–58. [Google Scholar] [CrossRef]
- Peterson, D.; Brenu, E.W.; Gottschalk, G.; Ramos, S.; Nguyen, T.; Staines, D.; Marshall-Gradisnik, S. Cytokines in the cerebrospinal fluids of patients with chronic fatigue syndrome/myalgic encephalomyelitis. Mediat. Inflamm. 2015, 2015, 929720. [Google Scholar] [CrossRef]
- Grace, P.M.; Loram, L.C.; Christianson, J.P.; Strand, K.A.; Flyer-Adams, J.G.; Penzkover, K.R.; Forsayeth, J.R.; van Dam, A.M.; Mahoney, M.J.; Maier, S.F. Behavioral assessment of neuropathic pain, fatigue, and anxiety in experimental autoimmune encephalomyelitis (EAE) and attenuation by interleukin-10 gene therapy. Brain Behav. Immun. 2017, 59, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Kwilasz, A.J.; Grace, P.M.; Serbedzija, P.; Maier, S.F.; Watkins, L.R. The therapeutic potential of interleukin-10 in neuroimmune diseases. Neuropharmacology 2015, 96, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Van Boxel-Dezaire, A.H.; Hoff, S.C.; van Oosten, B.W.; Verweij, C.L.; Dräger, A.M.; Adèr, H.J.; van Houwelingen, J.C.; Barkhof, F.; Polman, C.H.; Nagelkerken, L. Decreased interleukin-10 and increased interleukin-12p40 mRNA are associated with disease activity and characterize different disease stages in multiple sclerosis. Ann. Neurol. 1999, 45, 695–703. [Google Scholar] [CrossRef]
- Inogés, S.; Merino, J.; Bandrés, E.; De Castro, P.; Subirá, M.L.; Sánchez-Ibarrola, A. Cytokine flow cytometry differentiates the clinical status of multiple sclerosis (MS) patients. Clin. Exp. Immunol. 1999, 115, 521–525. [Google Scholar] [CrossRef]
- Waubant, E.; Gee, L.; Bacchetti, P.; Sloan, R.; Cotleur, A.; Rudick, R.; Goodkin, D. Relationship between serum levels of IL-10, MRI activity and interferon beta-1a therapy in patients with relapsing remitting MS. J. Neuroimmunol. 2001, 112, 139–145. [Google Scholar] [CrossRef]
- Petereit, H.F.; Pukrop, R.; Fazekas, F.; Bamborschke, S.U.; Röpele, S.; Kölmel, H.W.; Merkelbach, S.; Japp, G.; Jongen, P.J.; Hartung, H.P.; et al. Low interleukin-10 production is associated with higher disability and MRI lesion load in secondary progressive multiple sclerosis. J. Neurol. Sci. 2003, 206, 209–214. [Google Scholar] [CrossRef]
- Tedeschi, G.; Dinacci, D.; Lavorgna, L.; Prinster, A.; Savettieri, G.; Quattrone, A.; Livrea, P.; Messina, C.; Reggio, A.; Servillo, G.; et al. Correlation between fatigue and brain atrophy and lesion load in multiple sclerosis patients independent of disability. J. Neurol. Sci. 2007, 263, 15–19. [Google Scholar] [CrossRef]
- Sepulcre, J.; Masdeu, J.C.; Goñi, J.; Arrondo, G.; Vélez de Mendizábal, N.; Bejarano, B.; Villoslada, P. Fatigue in multiple sclerosis is associated with the disruption of frontal and parietal pathways. Mult. Scler. 2009, 15, 337–344. [Google Scholar] [CrossRef]
- Bakshi, R.; Miletich, R.S.; Henschel, K.; Shaikh, Z.A.; Janardhan, V.; Wasay, M.; Stengel, L.M.; Ekes, R.; Kinkel, P.R. Fatigue in multiple sclerosis: Cross-sectional correlation with brain MRI findings in 71 patients. Neurology 1999, 53, 1151–1153. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Müller-Lenke, N.; Naegelin, Y.; Kalt, G.; Bendfeldt, K.; Kuster, P.; Stoecklin, M.; Gass, A.; Sprenger, T.; Radue, E.W.; et al. Contribution of cortical and white matter lesions to cognitive impairment in multiple sclerosis. Mult. Scler. 2013, 19, 1290–1296. [Google Scholar] [CrossRef]
- Popescu, V.; Schoonheim, M.M.; Versteeg, A.; Chaturvedi, N.; Jonker, M.; Xavier de Menezes, R.; Gallindo Garre, F.; Uitdehaag, B.M.; Barkhof, F.; Vrenken, H. Grey Matter Atrophy in Multiple Sclerosis: Clinical Interpretation Depends on Choice of Analysis Method. PLoS ONE 2016, 11, e0143942. [Google Scholar] [CrossRef] [PubMed]
- Rocca, M.A.; Parisi, L.; Pagani, E.; Copetti, M.; Rodegher, M.; Colombo, B.; Comi, G.; Falini, A.; Filippi, M. Regional but not global brain damage contributes to fatigue in multiple sclerosis. Radiology 2014, 273, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Larson, R.D. Psychometric properties of the modified fatigue impact scale. Int. J. MS Care 2013, 15, 15–20. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| RR-MS | ||
|---|---|---|
| RR-MS patients | N | 106 |
| Age, years | Median [IQR] | 34.02 [25.44–45.23] |
| Sex, F | N (%) | 70/106 (66) |
| BMI | Median [IQR] | 25.04 [22.43–28.65] |
| Disease duration, months | Median [IQR] | 5.7 [1.9–24.5] |
| EDSS at diagnosis | Median [IQR] | 1.5 [1–2.125] |
| Radiological activity, presence | N (%) | 39/101 (38.6) |
| OCB, presence | N (%) | 89/104 (85.6) |
| CSF lactate mmol/L | Median [IQR] | 1.42 [1.3–1.6] |
| MFIS_total | Median [IQR] | 24 [6.75–34] |
| BDI-II | Median [IQR] | 7 [2.25–11.75] |
| STAI-Y state | Median [IQR] | 41 [33.25–49.75] |
| STAI-Y trait | Median [IQR] | 34 [30–45] |
| CSF Molecules | Spearman’s r | p | B-H Adjusted p |
|---|---|---|---|
| IL-1β | −0.159 | 0.103 | 0.515 |
| IL-2 | −0.041 | 0.674 | 0.949 |
| IL-4 | −0.006 | 0.952 | 0.952 |
| IL-5 | −0.027 | 0.786 | 0.949 |
| IL-6 | −0.012 | 0.902 | 0.949 |
| IL-7 | −0.058 | 0.556 | 0.927 |
| IL-8 | −0.113 | 0.248 | 0.792 |
| IL-9 | −0.179 | 0.066 | 0.440 |
| IL-10 | −0.309 | 0.001 | 0.020 |
| IL-12 | 0.026 | 0.791 | 0.949 |
| IL-13 | −0.088 | 0.370 | 0.792 |
| IL-17 | −0.083 | 0.396 | 0.792 |
| TNF | −0195 | 0.045 | 0.44 |
| IFNγ | −0.013 | 0.893 | 0.949 |
| IL1-ra | 0.098 | 0.318 | 0.792 |
| G-CSF | −0.016 | 0.868 | 0.949 |
| GM-CSF | −0.112 | 0.254 | 0.792 |
| MCP-1/CCL2 | 0.099 | 0.311 | 0.792 |
| MIP-1 α/CCL3 | 0.068 | 0.490 | 0.891 |
| MIP-1 β/CCL4 | −0.023 | 0.812 | 0.949 |
| Variable | OR | 95% CI | p |
|---|---|---|---|
| MFIS physical | 0.95 | 0.89–1.01 | 0.089 |
| Sex | 1.22 | 0.39–3.83 | 0.733 |
| Age at diagnosis | 1.01 | 0.96–1.06 | 0.708 |
| Disease duration | 0.99 | 0.97–1.01 | 0.298 |
| EDSS at diagnosis | 1.29 | 0.72–2.30 | 0.386 |
| Radiological disease activity | 2.68 | 0.86–8.40 | 0.090 |
| Total number of relapses at diagnosis | 0.80 | 0.35–1.84 | 0.602 |
| BDI–II | 1.03 | 0.91–1.15 | 0.663 |
| STAI-Y state | 1.01 | 0.94–1.07 | 0.847 |
| STAI-Y trait | 0.93 | 0.84–1.02 | 0.107 |
| BMI | 0.94 | 0.84–1.06 | 0.306 |
| DMTs | 0.32 | 0.09–1.10 | 0.070 |
| IL-10 | 0.18 | 0.02–1.98 | 0.162 |
| MFIS cognitive | 0.94 | 0.88–1.02 | 0.124 |
| Sex | 1.23 | 0.40–3.82 | 0.716 |
| Age at diagnosis | 1.00 | 0.95–1.06 | 0.888 |
| Disease duration | 0.99 | 0.97–1.01 | 0.336 |
| EDSS at diagnosis | 1.31 | 0.74–2.34 | 0.353 |
| Radiological disease activity | 2.54 | 0.82–7.88 | 0.106 |
| Total number of relapses at diagnosis | 0.73 | 0.32–1.65 | 0.445 |
| BDI-II | 1.03 | 0.92–1.15 | 0.627 |
| STAI-Y state | 0.99 | 0.94–1.06 | 0.971 |
| STAI-Y trait | 0.93 | 0.85–1.03 | 0.154 |
| BMI | 0.94 | 0.83–1.05 | 0.278 |
| DMTs | 0.30 | 0.08–1.05 | 0.059 |
| IL-10 | 0.25 | 0.02–2.48 | 0.235 |
| MFIS psychosocial | 0.67 | 0.49–0.90 | 0.009 |
| Sex | 0.93 | 0.28–3.13 | 0.912 |
| Age at diagnosis | 1.01 | 0.95–1.06 | 0.773 |
| Disease duration | 0.99 | 0.97–1.01 | 0.580 |
| EDSS at diagnosis | 1.20 | 0.67–2.17 | 0.536 |
| Radiological disease activity | 4.27 | 1.19–15.32 | 0.026 |
| Total number of relapses at diagnosis | 0.67 | 0.29–1.56 | 0.357 |
| BDI-II | 1.03 | 0.92–1.17 | 0.588 |
| STAI-Y state | 1.01 | 0.94–1.08 | 0.809 |
| STAI-Y trait | 0.93 | 0.84–1.02 | 0.138 |
| BMI | 0.94 | 0.83–1.06 | 0.283 |
| DMTs | 0.36 | 0.10–1.31 | 0.123 |
| IL-10 | 0.12 | 0.01–1.42 | 0.093 |
| MFIS total score | 0.96 | 0.92–0.99 | 0.039 |
| Sex | 1.10 | 0.34–0.35 | 0.876 |
| Age at diagnosis | 1.00 | 0.95–1.06 | 0.874 |
| Disease duration | 0.99 | 0.971.01 | 0.378 |
| EDSS at diagnosis | 1.33 | 0.73–2.39 | 0.348 |
| Radiological disease activity | 2.67 | 0.84–8.45 | 0.095 |
| Total number of relapses at diagnosis | 0.72 | 0.31–1.66 | 0.435 |
| BDI-II | 1.03 | 0.92–1.16 | 0.578 |
| STAI-Y state | 1.00 | 0.94–1.07 | 0.900 |
| STAI-Y trait | 0.94 | 0.85–1.03 | 0.182 |
| BMI | 0.93 | 0.83–1.05 | 0.259 |
| DMTs | 0.30 | 0.09–1.07 | 0.064 |
| IL-10 | 0.14 | 0.11–0.60 | 0.113 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilio, L.; Buttari, F.; Pavone, L.; Iezzi, E.; Galifi, G.; Dolcetti, E.; Azzolini, F.; Bruno, A.; Borrelli, A.; Storto, M.; et al. Fatigue in Multiple Sclerosis Is Associated with Reduced Expression of Interleukin-10 and Worse Prospective Disease Activity. Biomedicines 2022, 10, 2058. https://doi.org/10.3390/biomedicines10092058
Gilio L, Buttari F, Pavone L, Iezzi E, Galifi G, Dolcetti E, Azzolini F, Bruno A, Borrelli A, Storto M, et al. Fatigue in Multiple Sclerosis Is Associated with Reduced Expression of Interleukin-10 and Worse Prospective Disease Activity. Biomedicines. 2022; 10(9):2058. https://doi.org/10.3390/biomedicines10092058
Chicago/Turabian StyleGilio, Luana, Fabio Buttari, Luigi Pavone, Ennio Iezzi, Giovanni Galifi, Ettore Dolcetti, Federica Azzolini, Antonio Bruno, Angela Borrelli, Marianna Storto, and et al. 2022. "Fatigue in Multiple Sclerosis Is Associated with Reduced Expression of Interleukin-10 and Worse Prospective Disease Activity" Biomedicines 10, no. 9: 2058. https://doi.org/10.3390/biomedicines10092058
APA StyleGilio, L., Buttari, F., Pavone, L., Iezzi, E., Galifi, G., Dolcetti, E., Azzolini, F., Bruno, A., Borrelli, A., Storto, M., Furlan, R., Finardi, A., Pekmezovic, T., Drulovic, J., Mandolesi, G., Fresegna, D., Vanni, V., Centonze, D., & Stampanoni Bassi, M. (2022). Fatigue in Multiple Sclerosis Is Associated with Reduced Expression of Interleukin-10 and Worse Prospective Disease Activity. Biomedicines, 10(9), 2058. https://doi.org/10.3390/biomedicines10092058