
Cardiac Amyloidosis with Normal Wall Thickness: Prevalence, Clinical Characteristics and Outcome in a Retrospective Analysis

 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
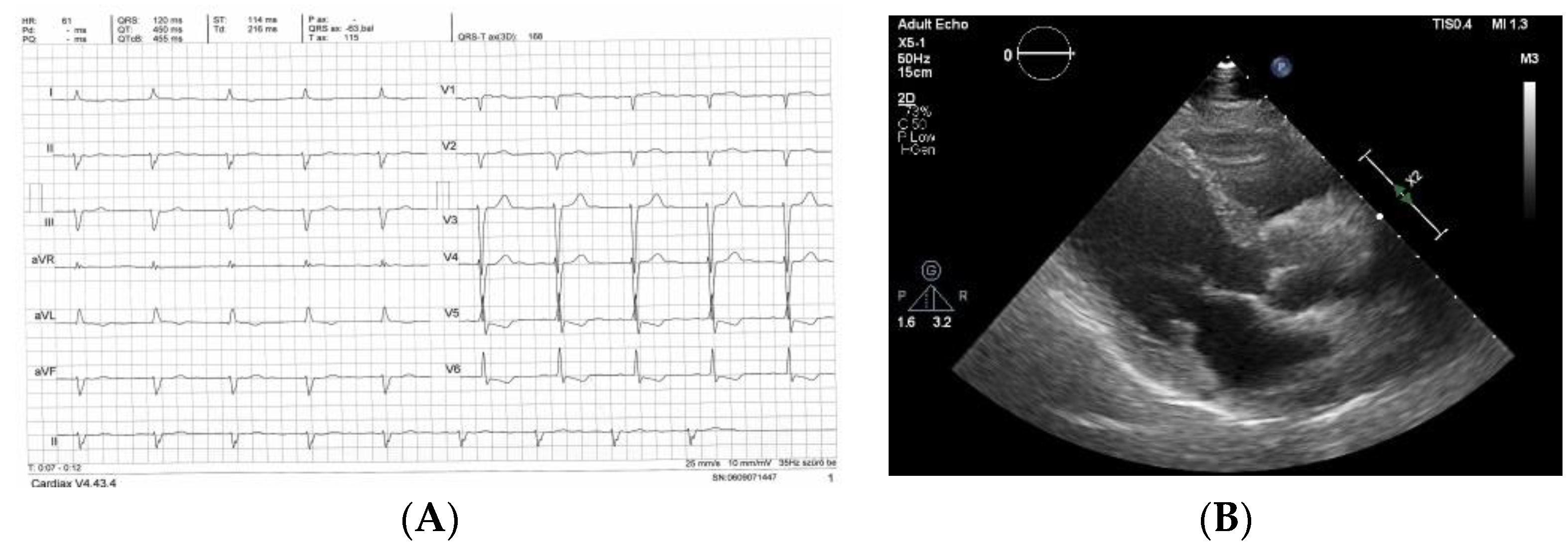
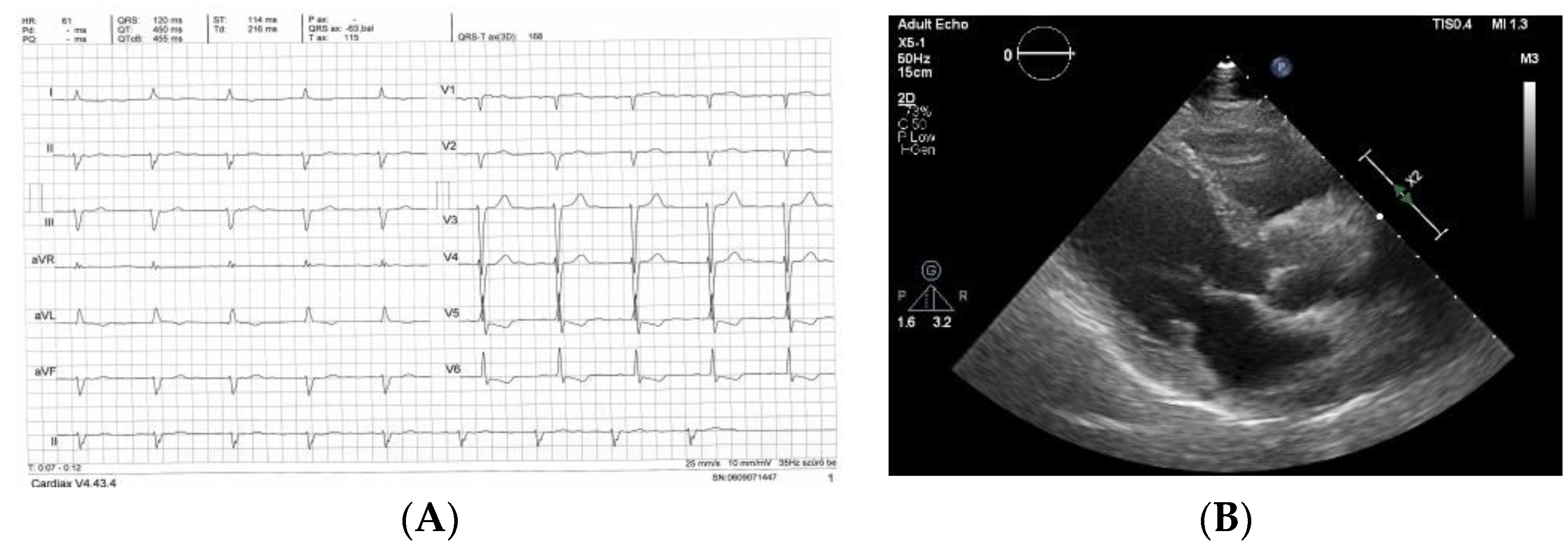
2.2. Echocardiography
2.3. Statistics
3. Results
3.1. Patient Population
3.2. Clinical Characteristics of Patients with and without IWT
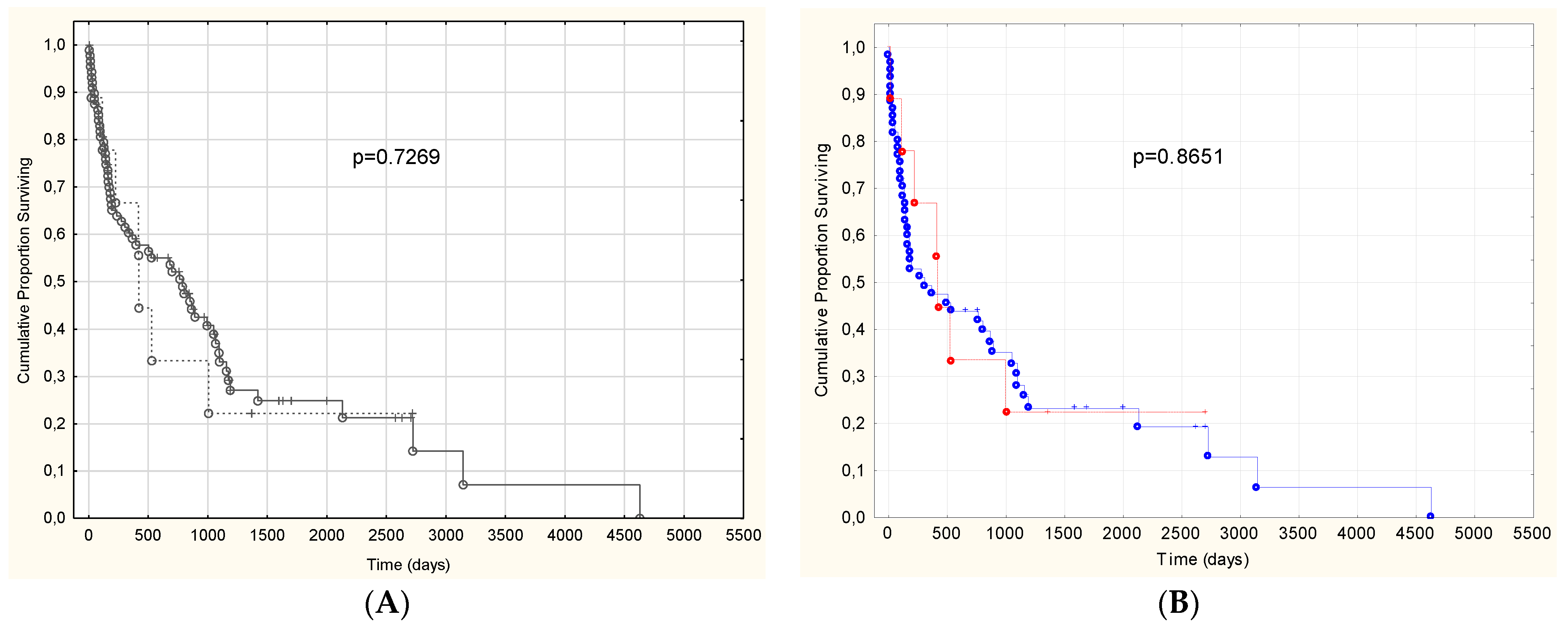
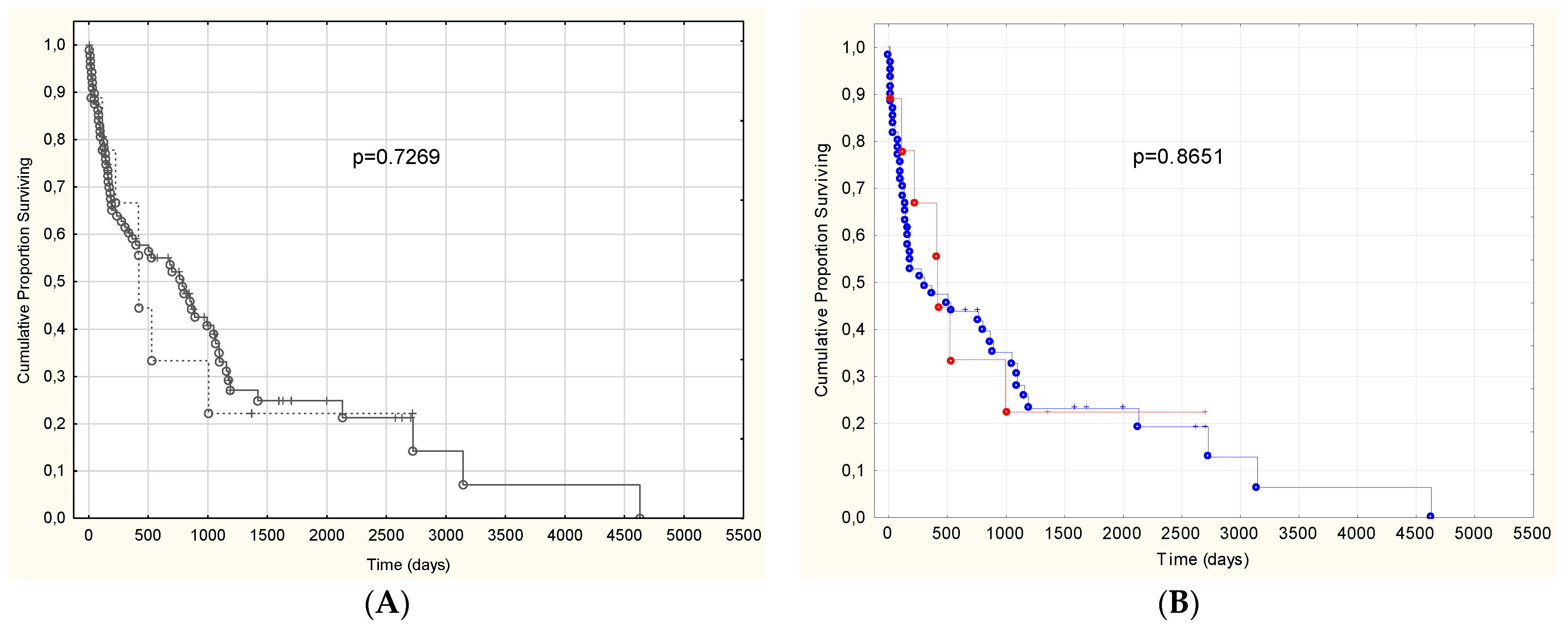
3.3. Prognosis of Patients with and without IWT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gertz, M.A.; Dispenzieri, A. Systemic Amyloidosis Recognition, Prognosis, and Therapy: A Systematic Review. JAMA J. Am. Med. Assoc. 2020, 324, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Buadi, F.K.; Dispenzieri, A.; Gertz, M.A. Immunoglobulin Light-Chain Amyloidosis: From Basics to New Developments in Diagnosis, Prognosis and Therapy. Acta Haematol. 2016, 135, 172–190. [Google Scholar] [CrossRef] [PubMed]
- Gertz, M.A.; Comenzo, R.; Falk, R.H.; Fermand, J.P.; Hazenberg, B.; Hawkins, P.N.; Merlini, G.; Moreau, P.; Ronco, P.; Sanchorawala, V.; et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): A consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18–22 April 2004. Am. J. Hematol. 2005, 79, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2—Evidence base and standardized methods of imaging. J. Nucl. Cardiol. 2019, 26, 2065–2123. [Google Scholar] [CrossRef] [PubMed]
- Dorbala, S.; Ando, Y.; Bokhari, S.; Dispenzieri, A.; Falk, R.H.; Ferrari, V.A.; Fontana, M.; Gheysens, O.; Gillmore, J.D.; Glaudemans, A.; et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 2 of 2—Diagnostic criteria and appropriate utilization. J. Nucl. Cardiol. 2020, 27, 659–673. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Phelan, D.; Collier, P.; Thavendiranathan, P.; Popovic, Z.; Hanna, M.; Plana, J.C.; Marwick, T.H.; Thomas, J.D. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart 2012, 98, 1442–1448. [Google Scholar] [CrossRef]
- Lee, G.Y.; Kim, K.; Choi, J.-O.; Kim, S.J.; Kim, J.-S.; Choe, Y.H.; Grogan, M.A.; Jeon, E.-S. Cardiac Amyloidosis Without Increased Left Ventricular Wall Thickness. Mayo Clin. Proc. 2014, 89, 781–789. [Google Scholar] [CrossRef]
- Cueto-Garcia, L.; Reeder, G.S.; Kyle, R.A.; Wood, D.L.; Seward, J.B.; Naessens, J.; Offord, K.P.; Greipp, P.R.; Edwards, W.D.; Tajik, A.J. Echocardiographic findings in systemic amyloidosis: Spectrum of cardiac involvement and relation to survival. J. Am. Coll. Cardiol. 1985, 6, 737–743. [Google Scholar] [CrossRef] [Green Version]
- Bellavia, D.; Pellikka, P.A.; Al-Zahrani, G.B.; Abraham, T.P.; Dispenzieri, A.; Miyazaki, C.; Lacy, M.; Scott, C.; Oh, J.K.; Miller, F.A., Jr. Independent Predictors of Survival in Primary Systemic (AL) Amyloidosis, Including Cardiac Biomarkers and Left Ventricular Strain Imaging: An Observational Cohort Study. J. Am. Soc. Echocardiogr. 2010, 23, 643–652. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Dispenzieri, A.; Lacy, M.Q.; Hayman, S.R.; Buadi, F.K.; Colby, C.; Laumann, K.; Zeldenrust, S.R.; Leung, N.; Dingli, D.; et al. Revised Prognostic Staging System for Light Chain Amyloidosis Incorporating Cardiac Biomarkers and Serum Free Light Chain Measurements. J. Clin. Oncol. 2012, 30, 989–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillmore, J.D.; Damy, T.; FontAna, M.; Hutchinson, M.; Lachmann, H.J.; Martinez-Naharro, A.; Quarta, C.C.; Rezk, T.; Whelan, C.J.; Gonzalez-Lopez, E.; et al. A new staging system for cardiac transthyretin amyloidosis. Eur. Heart J. 2018, 39, 2799–2806. [Google Scholar] [CrossRef] [PubMed]
- Devesa, A.; Blasco, A.C.; Lázaro, A.M.P.; Askari, E.; Lapeña, G.; Talavera, S.G.; Urquía, M.T.; Olleros, C.R.; Tuñón, J.; Ibáñez, B.; et al. Prevalence of transthyretin amyloidosis in patients with heart failure and no left ventricular hypertrophy. ESC Heart Fail. 2021, 8, 2856–2865. [Google Scholar] [CrossRef]
- Ryšavá, R. AL amyloidosis: Advances in diagnostics and treatment. Nephrol. Dial. Transplant. 2019, 34, 1460–1466. [Google Scholar] [CrossRef] [Green Version]
- Razvi, Y.; Patel, R.K.; Fontana, M.; Gillmore, J.D. Cardiac Amyloidosis: A Review of Current Imaging Techniques. Front. Cardiovasc. Med. 2021, 8, 751293. [Google Scholar] [CrossRef] [PubMed]
- Wechalekar, A.D.; Gillmore, J.D.; Hawkins, P.N. Systemic amyloidosis. Lancet 2016, 387, 2641–2654. [Google Scholar] [CrossRef]
- Joury, A.; Gupta, T.; Krim, S.R. Cardiac Amyloidosis: Presentations, Diagnostic Work-up and Collaborative Approach for Comprehensive Clinical Management. Curr. Probl. Cardiol. 2021, 46, 100910. [Google Scholar] [CrossRef]
- Boldrini, M.; Cappelli, F.; Chacko, L.; Restrepo-Cordoba, M.A.; Sainz, A.L.; Giannoni, A.; Aimo, A.; Baggiano, A.; Martinez-Naharro, A.; Whelan, C.; et al. Multiparametric Echocardiography Scores for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 909–920. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology W orking G roup on M yocardial and P ericardial D iseases. Eur. J. Heart Fail. 2021, 23, 512–526. [Google Scholar] [CrossRef]
- Vogelsberg, H.; Mahrholdt, H.; Deluigi, C.C.; Yilmaz, A.; Kispert, E.M.; Greulich, S.; Klingel, K.; Kandolf, R.; Sechtem, U. Cardiovascular Magnetic Resonance in Clinically Suspected Cardiac Amyloidosis: Noninvasive Imaging Compared to Endomyocardial Biopsy. J. Am. Coll. Cardiol. 2008, 51, 1022–1030. [Google Scholar] [CrossRef] [Green Version]
- Syed, I.S.; Glockner, J.F.; Feng, D.; Araoz, P.A.; Martinez, M.W.; Edwards, W.D.; Gertz, M.A.; Dispenzieri, A.; Oh, J.K.; Bellavia, D.; et al. Role of Cardiac Magnetic Resonance Imaging in the Detection of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2010, 3, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Maceira, A.M.; Joshi, J.; Prasad, S.K.; Moon, J.; Perugini, E.; Harding, I.; Sheppard, M.; Poole-Wilson, P.A.; Hawkins, P.N.; Pennell, D. Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation 2005, 111, 186–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 98) | Patients with IWT (n = 89) | Patients without IWT (n = 9) | p Value |
|---|---|---|---|---|
| Age (years) | 68 (59–76) | 68 (60–76) | 59 (58–72) | 0.281 |
| Male patients (n, %) | 54 (55) | 50 (56) | 4 (44.4) | 0.500 |
| NYHA III-IV (n, %) | 51 (52) | 47 (53) | 4 (44.4) | 0.574 |
| ATTRv (n, %) | 11 (11) | 11 (12) | 0 (0) | 0.263 |
| ATTRwt (n, %) | 16 (16) | 16 (18) | 0 (0) | 0.164 |
| AL (n, %) | 70 (71) | 61 (68.5) | 9 (100) | 0.046 |
| AA (n, %) | 1 (1) | 1 (1.1) | 0 (0) | 0.750 |
| Mean wall thickness (mm) | 16.5 (14–18) | 17 (14.5–18.5) | 10 (10–11) | <0.001 |
| Septum (mm) | 16 (14–19) | 17 (14–19) | 10 (10–11) | <0.001 |
| Posterior wall (mm) | 16 (14–18) | 16 (15–18) | 10 (10–11) | <0.001 |
| Relative wall thickness | 0.79 (0.65–1.02) | 0.84 (0.68–1.02) | 0.52 (0.43–0.55) | <0.001 |
| Left ventricular ejection fraction (%) | 54 (43–62) | 54 (44–62) | 56 (40–60) | 0.725 |
| E/e’(e’: average of lateral and septal e’) | 19.5 (15.11–23.8) | 20 (15.6–23.8) | 15.82 (11.47–26.09) | 0.298 |
| TAPSE (mm) | 15 (11–19.5) | 16 (11–19) | 19 (14–24) | 0.119 |
| NTproBNP (pg/mL) | 4289 (1537–8575) | 4819 (1713–8798) | 1821 (573–4311) | 0.172 |
| Troponin T (ng/L) | 73 (40–127) | 83 (40–131) | 50 (26–62) | 0.090 |
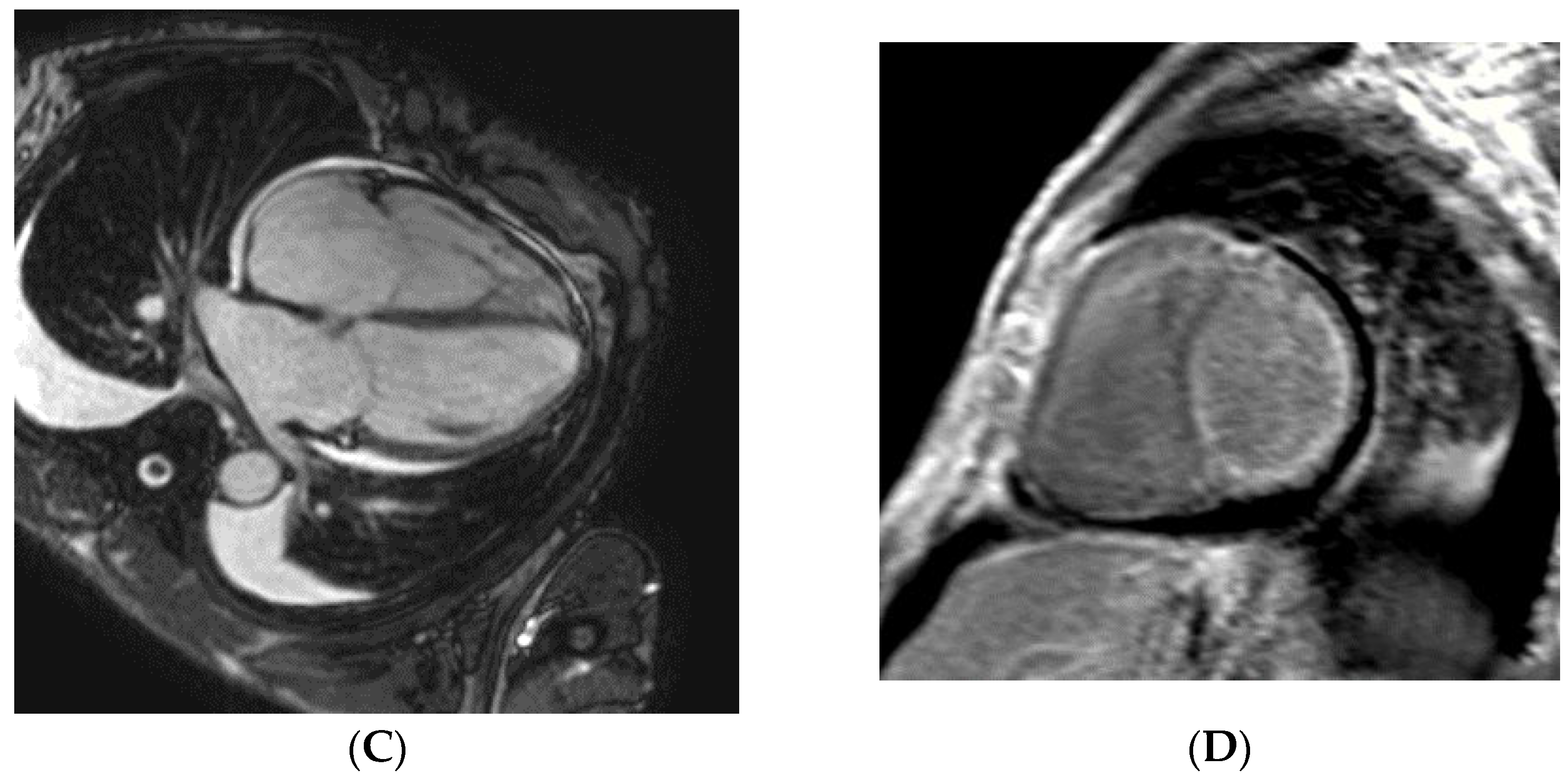
| Pt | Age at Diagnosis (Years) Sex of Patient | Left Ventricular Septal/Inferior/Average Wall Thickness (mm) EDV (mm)/ EF Measured with Echocardiography | E/e’ | Stage of Heart Failure According to NYHA at the Time of Diagnosis | NTproBNP (pg/mL) | Troponin T (ng/L) | GFR (mL/min/ 1.73 m2) | Organ from where the Biopsy Proved AL Amyloidosis | Result of CMR | Known PCD Before the Diagnosis of CA | Complaint, Symptom that Led to the Diagnosis of CA/Other Clinically Significant Organ Involvement |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 65 male | 10/10/10 | 33.5 | IV | 6492 | 50 | 23 | rectum | typical for CA | No | heart failure/ polyneuropathy |
| 54/22 | |||||||||||
| 2 | 59 male | 10/10/10 43/56 | 8.95 | II | 2106 | 55 | 108 | heart | typical for CA | Yes | heart failure/ polyneuropathy |
| 3 | 52 male | 11/11/11 | 16 | III | 1537 | 42 | 80 | heart | typical for CA | No | heart failure/CTS, polyneuropathy |
| 42/63 | |||||||||||
| 4 | 75 female | 12/11/11.5 43/35 | 18.6 | III | 4311 | 96 | 112 | skin of eyelid | NP | No | heart failure/- |
| 5 | 59 female | 10/10/10 36/63 | 14 | I | 1436 | 69 | 26 | kidney | NP | Yes | screening for CA/ nephrotic syndrome |
| 6 | 72 female | 11/12/11.5 41/40 | 35.8 | IV | 6925 | 50 | 85 | abdominal fat | typical for CA | No | heart failure |
| 7 | 56 male | 9/9/9 42/53 | 13.9 | II | 573 | 32.9 | 113 | skin of eyelid, capsular ligament | LGE in atrial walls | Yes | screening for CA/ joint pain/ CTS |
| 8 | 58 female | 10/10/10 36/60 | 8.9 | I | 486 | 10 | 51 | kidney | not typical for CA | Yes | screening for CA/ polyneuropathy/ nephrotic syndrome |
| 9 | 82 female | 11/11/11 51/60 | 15.6 | II | 1717 | 8 | 51 | abdominal fat | not typical for CA | Yes | heart failure |
| Characteristic | AL Patients (n = 70) | AL IWT (n = 61) | AL non IWT (n = 9) | p Value |
|---|---|---|---|---|
| Age (years) | 64 (58–73) | 64 (58–73) | 59 (58–72) | 0.605 |
| Male patients (n, %) | 26 (37) | 22 (36) | 4 (44.4) | 0.582 |
| NYHA (III-IV) (n, %) | 43 (30) | 39 (64) | 4 (44.4) | 0.205 |
| TroponinT (ng/L) | 85 (45–132) | 93 (46–141) | 50 (26–62) | 0.030 |
| NTproBNP (pg/mL) | 5063 (1909–11764) | 5927 (2678–14183) | 1821 (573–4311) | 0.060 |
| Mean left ventricular wall thickness (mm) | 15 (13–17) | 16 (14.5–17.5) | 10 (10–11) | <0.001 |
| Septum (mm) | 15 (14–18) | 16 (14–18) | 10 (10–11) | <0.001 |
| Posterior wall (mm) | 15.5 (15–17) | 16 (15–17) | 10 (10–11) | <0.001 |
| EF (%) | 58 (43–63) | 59 (45–63) | 56 (40–60) | 0.497 |
| TAPSE (mm) | 15 (11–19) | 14 (10–19) | 19 (14–24) | 0.079 |
| E/e’(e’: average of lateral and septal e’) | 19.2 (15.6–25.5) | 20 (17–25.5) | 15.6 (14–18.6) | 0.130 |
| Low voltage on ECG (n, %) | 39 (56) | 37 (61) | 2 (22) | 0.032 |
| Atrial fibrillation (n, %) | 12 (17) | 12 (20) | 0 (0) | 0.054 |
| FLC-diff (mg/L) | 227 (143–574) | 224 (146–547) | 376 (99–757) | 0.666 |
| GFR (mL/min/ 1.73 m2) | 65 (44–81) | 64 (44–79) | 80 (51–108) | 0.350 |
| CyBorDex as first line specific medical therapy | 33 (23) | 28 (46) | 5 (56) | 0.459 |
| ASCT | 7 (10) | 6 (10) | 1 (11) | 0.759 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, D.; Révész, K.; Peskó, G.; Varga, G.; Horváth, L.; Farkas, P.; Tóth, A.D.; Sepp, R.; Vágó, H.; Nagy, A.I.; et al. Cardiac Amyloidosis with Normal Wall Thickness: Prevalence, Clinical Characteristics and Outcome in a Retrospective Analysis. Biomedicines 2022, 10, 1765. https://doi.org/10.3390/biomedicines10071765
Nagy D, Révész K, Peskó G, Varga G, Horváth L, Farkas P, Tóth AD, Sepp R, Vágó H, Nagy AI, et al. Cardiac Amyloidosis with Normal Wall Thickness: Prevalence, Clinical Characteristics and Outcome in a Retrospective Analysis. Biomedicines. 2022; 10(7):1765. https://doi.org/10.3390/biomedicines10071765
Chicago/Turabian StyleNagy, Daniella, Katalin Révész, Gergely Peskó, Gergely Varga, Laura Horváth, Péter Farkas, András Dávid Tóth, Róbert Sepp, Hajnalka Vágó, Anikó Ilona Nagy, and et al. 2022. "Cardiac Amyloidosis with Normal Wall Thickness: Prevalence, Clinical Characteristics and Outcome in a Retrospective Analysis" Biomedicines 10, no. 7: 1765. https://doi.org/10.3390/biomedicines10071765
APA StyleNagy, D., Révész, K., Peskó, G., Varga, G., Horváth, L., Farkas, P., Tóth, A. D., Sepp, R., Vágó, H., Nagy, A. I., Masszi, T., & Pozsonyi, Z. (2022). Cardiac Amyloidosis with Normal Wall Thickness: Prevalence, Clinical Characteristics and Outcome in a Retrospective Analysis. Biomedicines, 10(7), 1765. https://doi.org/10.3390/biomedicines10071765