
Combined Effects of Chronic Kidney Disease and Nonalcoholic Fatty Liver Disease on the Risk of Cardiovascular Disease in Patients with Diabetes

 , ,
, ,
Abstract
:1. Introduction
2. Research Design and Method
2.1. Data Source
2.2. Ethics Statement
2.3. Study Population
2.4. Measurements
2.5. Surrogate Measurement of NAFLD and Probability of Advanced Fibrosis
× BMI + 0.718 × ln GGT + 0.053 × WC − 15.745) × 100
2.6. Outcome Variable
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
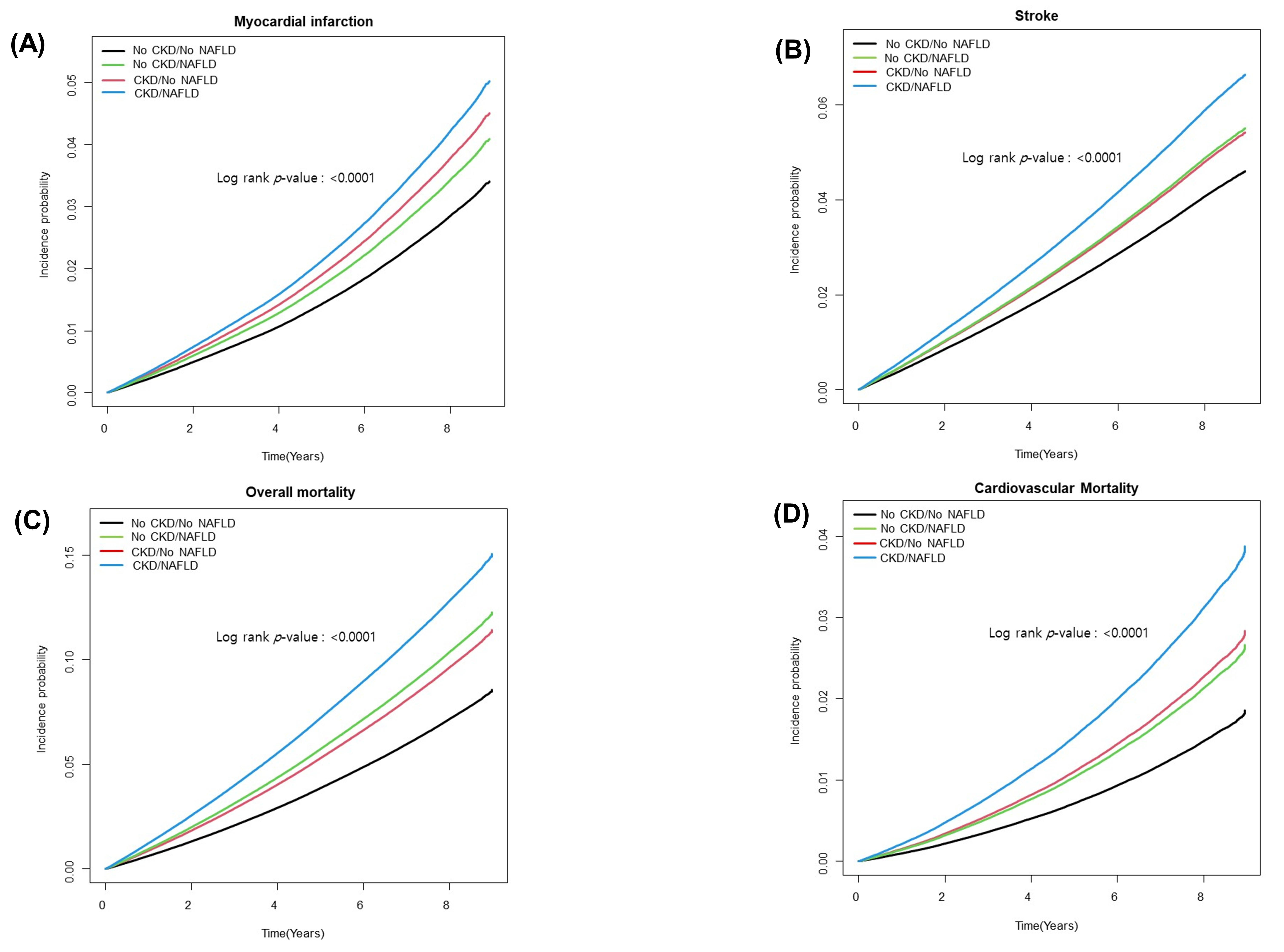
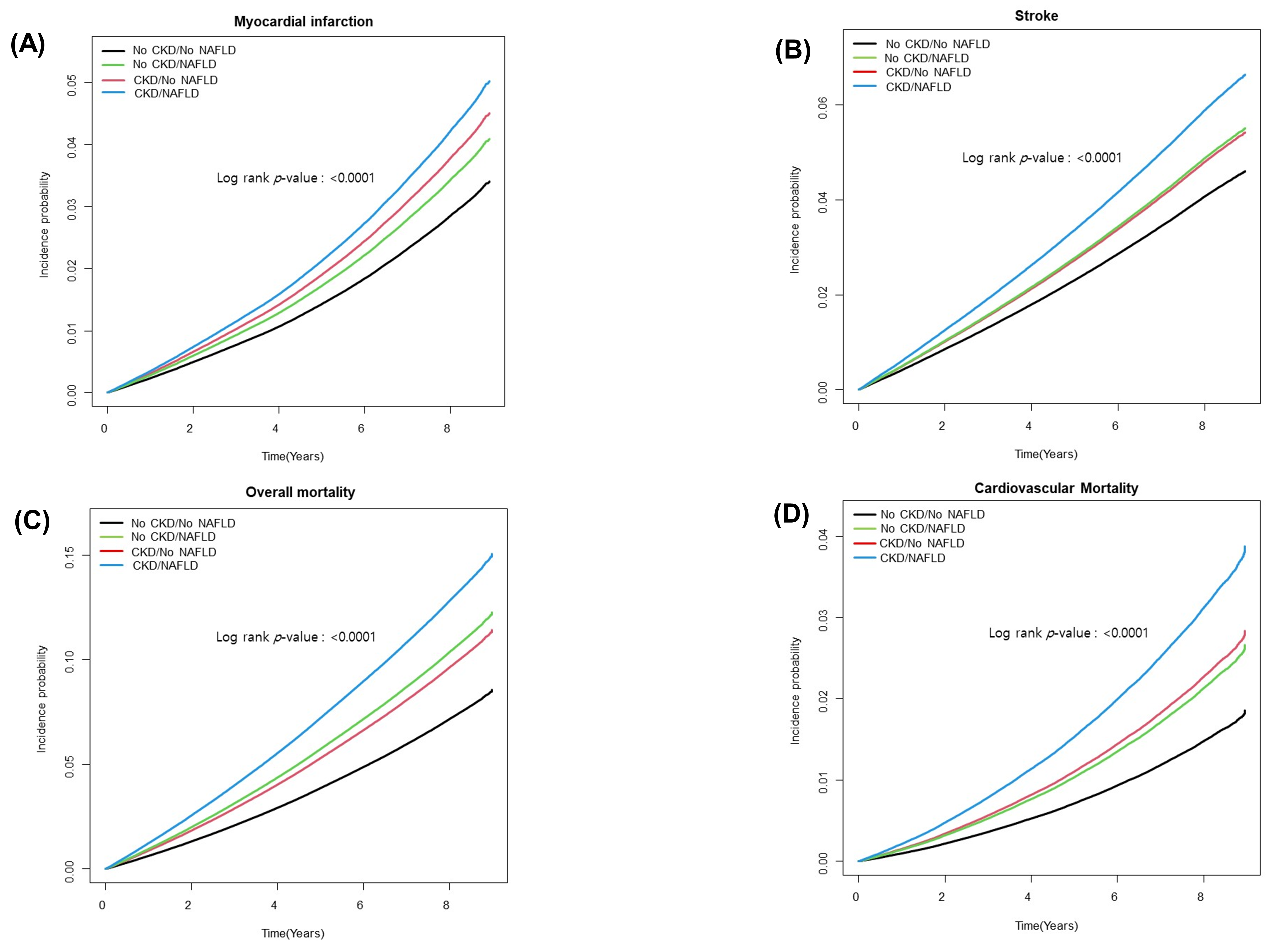
3.2. Risk of CVD According to NAFLD and CKD
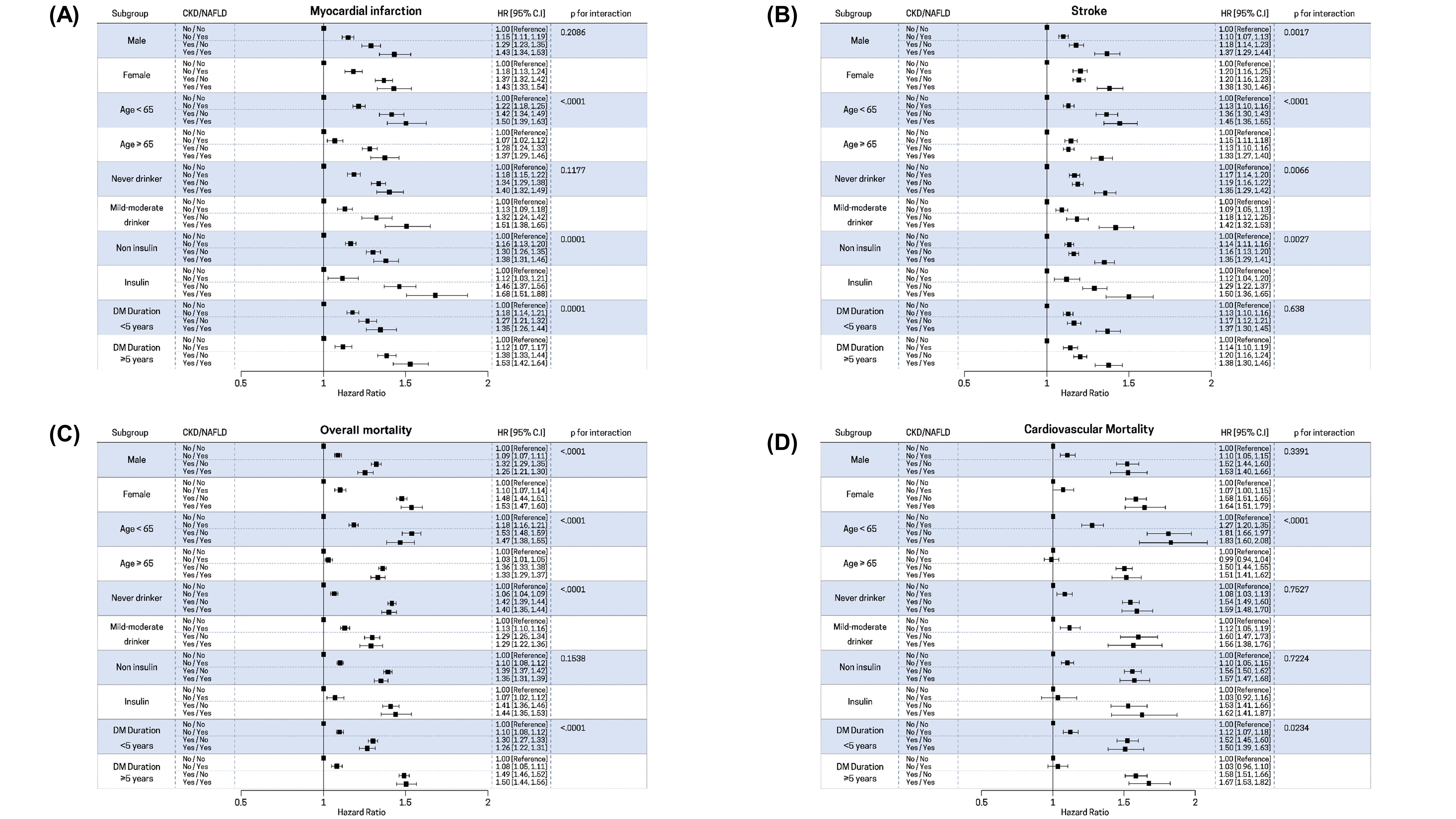
3.3. Stratified Analyses
3.4. Subgroup Analysis in Subjects with NAFLD
3.5. Subgroup Analysis in Subjects with CKD
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Ye, L.; Liu, A.; Wen, S.W.; Deng, J.; Wu, X.; Lai, Z. Prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: A meta-analysis. Medicine 2017, 96, e8179. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Bertolini, L.; Rodella, S.; Tessari, R.; Zenari, L.; Lippi, G.; Arcaro, G. Nonalcoholic fatty liver disease is independently associated with an increased incidence of cardiovascular events in type 2 diabetic patients. Diabetes Care 2007, 30, 2119–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.A.; Wang, Y.; Zhu, V.; Rupnow, M.F. Chronic kidney disease in US adults with type 2 diabetes: An updated national estimate of prevalence based on Kidney Disease: Improving Global Outcomes (KDIGO) staging. BMC Res. Notes 2014, 7, 415. [Google Scholar] [CrossRef] [Green Version]
- Zelnick, L.R.; Weiss, N.S.; Kestenbaum, B.R.; Robinson-Cohen, C.; Heagerty, P.J.; Tuttle, K.; Hall, Y.N.; Hirsch, I.B.; de Boer, I.H. Diabetes and CKD in the United States Population, 2009-2014. Clin. J. Am. Soc. Nephrol. 2017, 12, 1984–1990. [Google Scholar] [CrossRef] [Green Version]
- Fioretto, P. Diabetic kidney disease: The onset of a new era? J. Nephrol. 2020, 33, 899–900. [Google Scholar] [CrossRef]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef]
- Hahr, A.J.; Molitch, M.E. Management of Diabetes Mellitus in Patients With CKD: Core Curriculum 2022. Am. J. Kidney Dis. 2021, 79, 728–736. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD as a driver of chronic kidney disease. J. Hepatol. 2020, 72, 785–801. [Google Scholar] [CrossRef] [Green Version]
- Sinn, D.H.; Kang, D.; Jang, H.R.; Gu, S.; Cho, S.J.; Paik, S.W.; Ryu, S.; Chang, Y.; Lazo, M.; Guallar, E.; et al. Development of chronic kidney disease in patients with non-alcoholic fatty liver disease: A cohort study. J. Hepatol. 2017, 67, 1274–1280. [Google Scholar] [CrossRef]
- Alexander, M.; Loomis, A.K.; van der Lei, J.; Duarte-Salles, T.; Prieto-Alhambra, D.; Ansell, D.; Pasqua, A.; Lapi, F.; Rijnbeek, P.; Mosseveld, M.; et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: Findings from matched cohort study of 18 million European adults. BMJ 2019, 367, l5367. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Roelstraete, B.; Hagström, H.; Sundström, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2021, in press. [Google Scholar] [CrossRef]
- Kühn, A.; van der Giet, M.; Kuhlmann, M.K.; Martus, P.; Mielke, N.; Ebert, N.; Schaeffner, E.S. Kidney Function as Risk Factor and Predictor of Cardiovascular Outcomes and Mortality Among Older Adults. Am. J. Kidney Dis. 2021, 77, 386–396.e381. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Han, K.; Ko, S.H.; Ko, K.S.; Lee, K.U.; Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Data Analytic Process of a Nationwide Population-Based Study Using National Health Information Database Established by National Health Insurance Service. Diabetes Metab. J. 2016, 40, 79–82. [Google Scholar] [CrossRef]
- Lee, H.J.; Choi, E.K.; Han, K.D.; Kim, D.H.; Lee, E.; Lee, S.R.; Oh, S.; Lip, G.Y.H. High variability in bodyweight is associated with an increased risk of atrial fibrillation in patients with type 2 diabetes mellitus: A nationwide cohort study. Cardiovasc. Diabetol. 2020, 19, 78. [Google Scholar] [CrossRef]
- Choi, Y.J.; Han, K.D.; Choi, E.K.; Jung, J.H.; Lee, S.R.; Oh, S.; Lip, G.Y.H. Alcohol Abstinence and the Risk of Atrial Fibrillation in Patients With Newly Diagnosed Type 2 Diabetes Mellitus: A Nationwide Population-Based Study. Diabetes Care 2021, 44, 1393–1401. [Google Scholar] [CrossRef]
- Cho, E.J.; Han, K.; Lee, S.P.; Shin, D.W.; Yu, S.J. Liver enzyme variability and risk of heart disease and mortality: A nationwide population-based study. Liver Int. 2020, 40, 1292–1302. [Google Scholar] [CrossRef]
- Chung, G.E.; Chang, Y.; Cho, Y.; Cho, E.J.; Yoo, J.J.; Park, S.H.; Han, K.; Shin, D.W.; Yu, S.J.; Kim, Y.J.; et al. The Change in Metabolic Syndrome Status and the Risk of Nonviral Liver Cirrhosis. Biomedicines 2021, 9, 1948. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Han, K.; Hong, J.Y.; Park, Y.S.; Park, J.O. Association between alcohol consumption and pancreatic cancer risk differs by glycaemic status: A nationwide cohort study. Eur. J. Cancer 2022, 163, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Kim, J.; Park, S.; Park, S.Y.; Yu, J.H.; Seo, J.A.; Kim, N.H.; Yoo, H.J.; Kim, S.G.; Choi, K.M.; et al. Fasting Glucose Variability as a Risk Indicator for End-Stage Kidney Disease in Patients with Diabetes: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 5948. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Int. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Bae, E.H.; Kim, B.; Song, S.H.; Oh, T.R.; Suh, S.H.; Choi, H.S.; Kim, C.S.; Ma, S.K.; Han, K.D.; Kim, S.W. Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 2356. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J.; American Gastroenterological, A.; American Association for the Study of Liver, D.; et al. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Schouten, J.N.; Hansen, B.E.; Hofman, A.; Stricker, B.H.; Janssen, H.L. External validation of the fatty liver index for identifying nonalcoholic fatty liver disease in a population-based study. Clin. Gastroenterol. Hepatol. 2013, 11, 1201–1204. [Google Scholar] [CrossRef]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; Group, L.S. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef]
- Kim, J.H.; Kwon, S.Y.; Lee, S.W.; Lee, C.H. Validation of fatty liver index and lipid accumulation product for predicting fatty liver in Korean population. Liver Int. 2011, 31, 1600–1601. [Google Scholar] [CrossRef]
- Lee, Y.H.; Bang, H.; Park, Y.M.; Bae, J.C.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Lee, H.C.; Balkau, B.; Lee, W.Y.; et al. Non-laboratory-based self-assessment screening score for non-alcoholic fatty liver disease: Development, validation and comparison with other scores. PLoS ONE 2014, 9, e107584. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Muraca, E.; Perra, S.; Bianconi, E.; Zerbini, F.; Oltolini, A.; Cannistraci, R.; Parmeggiani, P.; Manzoni, G.; Gastaldelli, A.; et al. Screening for non-alcoholic fatty liver disease in type 2 diabetes using non-invasive scores and association with diabetic complications. BMJ Open Diabetes Res. Care 2020, 8, e000904. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Zhao, Z.; Qin, G.; Chen, L.; Lu, J.; Huo, Y.; Chen, L.; Zeng, T.; Xu, M.; Chen, Y.; et al. Non-alcoholic fatty liver disease, metabolic goal achievement with incident cardiovascular disease and eGFR-based chronic kidney disease in patients with prediabetes and diabetes. Metabolism 2021, 124, 154874. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Han, K.; Kim, H.S.; Park, Y.M.; Kwon, H.S.; Yoon, K.H.; Lee, S.H. Cholesterol variability and the risk of mortality, myocardial infarction, and stroke: A nationwide population-based study. Eur. Heart J. 2017, 38, 3560–3566. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.Y.; Zhou, X.D.; Wu, S.J.; Hu, X.Q.; Tang, B.; Poucke, S.V.; Pan, X.Y.; Wu, W.J.; Gu, X.M.; Fu, S.W.; et al. Synergistic increase in cardiovascular risk in diabetes mellitus with nonalcoholic fatty liver disease: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 631–636. [Google Scholar] [CrossRef]
- Targher, G.; Lonardo, A.; Byrne, C.D. Nonalcoholic fatty liver disease and chronic vascular complications of diabetes mellitus. Nat. Rev. Endocrinol. 2018, 14, 99–114. [Google Scholar] [CrossRef] [Green Version]
- Caussy, C.; Aubin, A.; Loomba, R. The Relationship Between Type 2 Diabetes, NAFLD, and Cardiovascular Risk. Curr. Diab. Rep. 2021, 21, 15. [Google Scholar] [CrossRef]
- Shen, Y.; Cai, R.; Sun, J.; Dong, X.; Huang, R.; Tian, S.; Wang, S. Diabetes mellitus as a risk factor for incident chronic kidney disease and end-stage renal disease in women compared with men: A systematic review and meta-analysis. Endocrine 2017, 55, 66–76. [Google Scholar] [CrossRef]
- Chang, Y.T.; Wu, J.L.; Hsu, C.C.; Wang, J.D.; Sung, J.M. Diabetes and end-stage renal disease synergistically contribute to increased incidence of cardiovascular events: A nationwide follow-up study during 1998-2009. Diabetes Care 2014, 37, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Nag, S.; Bilous, R.; Kelly, W.; Jones, S.; Roper, N.; Connolly, V. All-cause and cardiovascular mortality in diabetic subjects increases significantly with reduced estimated glomerular filtration rate (eGFR): 10 years’ data from the South Tees Diabetes Mortality study. Diabet. Med. 2007, 24, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, S.; Kim, Y.; Cho, S.; Kim, K.; Kim, Y.C.; Han, S.S.; Lee, H.; Lee, J.P.; Joo, K.W.; et al. Causal effects from non-alcoholic fatty liver disease on kidney function: A Mendelian randomization study. Liver Int. 2021, 42, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Forlani, G.; Giorda, C.; Manti, R.; Mazzella, N.; De Cosmo, S.; Rossi, M.C.; Nicolucci, A.; Di Bartolo, P.; Ceriello, A.; Guida, P.; et al. The Burden of NAFLD and Its Characteristics in a Nationwide Population with Type 2 Diabetes. J. Diabetes Res. 2016, 2016, 2931985. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Byrne, C.D. Non-alcoholic fatty liver disease: An emerging driving force in chronic kidney disease. Nat. Rev. Nephrol. 2017, 13, 297–310. [Google Scholar] [CrossRef] [Green Version]
- Francque, S.M.; van der Graaff, D.; Kwanten, W.J. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J. Hepatol. 2016, 65, 425–443. [Google Scholar] [CrossRef] [Green Version]
- Yeung, M.W.; Wong, G.L.; Choi, K.C.; Luk, A.O.; Kwok, R.; Shu, S.S.; Chan, A.W.; Lau, E.S.H.; Ma, R.C.W.; Chan, H.L.; et al. Advanced liver fibrosis but not steatosis is independently associated with albuminuria in Chinese patients with type 2 diabetes. J. Hepatol. 2017, 68, 147–156. [Google Scholar] [CrossRef]
- Williams, M.E. Diabetic nephropathy: The proteinuria hypothesis. Am. J. Nephrol. 2005, 25, 77–94. [Google Scholar] [CrossRef]
- de Zeeuw, D.; Remuzzi, G.; Parving, H.H.; Keane, W.F.; Zhang, Z.; Shahinfar, S.; Snapinn, S.; Cooper, M.E.; Mitch, W.E.; Brenner, B.M. Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation 2004, 110, 921–927. [Google Scholar] [CrossRef] [Green Version]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [Green Version]
- Alhinai, A.; Patel, K.; Fonseca, V.A.; Sebastiani, G. Non-invasive diagnosis of nonalcoholic fatty liver disease in patients with type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107978. [Google Scholar] [CrossRef] [PubMed]
- White, S.L.; Yu, R.; Craig, J.C.; Polkinghorne, K.R.; Atkins, R.C.; Chadban, S.J. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general community. Am. J. Kidney Dis. 2011, 58, 19–28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| No CKD /No NAFLD | No CKD/NAFLD | CKD/No NAFLD | CKD/NAFLD | p-Value | |
|---|---|---|---|---|---|
| Number of subjects | 1,065,190 | 379,638 | 124,507 | 37,879 | |
| Age, years | 56.5 ± 12.1 | 51.9 ± 11.5 | 65.3 ± 11.2 | 62.0 ± 11.5 | <0.0001 |
| Male (%) | 567,790 (53.3) | 283,075 (75.6) | 49,682 (39.9) | 21,439 (56.6) | <0.0001 |
| Smoking status | <0.0001 | ||||
| Never-smoker (%) | 657,597 (61.7) | 164,527 (43.3) | 90,663 (72.8) | 22,810 (60.2) | |
| Ex-smoker (%) | 170,467 (16.0) | 78,392 (20.7) | 18,091 (14.5) | 7351 (19.4) | |
| Current smoker (%) | 237,126 (22.3) | 136,719 (36.0) | 15,753 (12.7) | 7736 (20.4) | |
| Alcohol consumption | <0.0001 | ||||
| None (%) | 680,576 (63.9) | 168,735 (44.5) | 97,478 (78.3) | 24,336 (64.2) | |
| Mild-to-moderate (%) | 384,614 (36.1) | 210,903 (55.6) | 27,032 (21.7) | 13,561 (35.8) | |
| Regular physical activity (%) | 229,673 (21.6) | 66,218 (17.4) | 25,657 (20.6) | 6911 (18.2) | <0.0001 |
| BMI, kg/m2 | 23.9 ± 2.7 | 28.2 ± 3.4 | 24.1 ± 2.7 | 28.4 ± 3.5 | <0.0001 |
| Waist circumference (cm) | 82.0 ± 7.2 | 93.0 ± 8.6 | 83.0 ± 7.3 | 94.2 ± 8.3 | <0.0001 |
| SBP (mmHg) | 127.1 ± 15.5 | 132.1 ± 15.4 | 129.8 ± 16.6 | 132.9 ± 16.4 | <0.0001 |
| DBP (mmHg) | 77.9 ± 9.9 | 82.3 ± 10.3 | 77.6 ± 10.3 | 80.9 ± 10.5 | <0.0001 |
| Hypertension (%) | 498,952 (46.8) | 221,449 (58.3) | 86,834 (69.7) | 29,484 (77.8) | <0.0001 |
| Dyslipidemia (%) | 380,152 (35.7) | 173,055 (45.6) | 58,176 (46.7) | 21,034 (55.5) | <0.0001 |
| DM duration ≥ 5 years (%) | 306,461 (28.8) | 65,192 (17.2) | 55,941 (44.9) | 12,921 (34.1) | <0.0001 |
| Insulin use (%) | 71,954 (6.8) | 16,580 (4.4) | 16,953 (13.6) | 4135 (10.9) | <0.0001 |
| OHA ≥ 3 (%) | 143,862 (13.5) | 39,644 (10.4) | 23,172 (18.6) | 6274 (16.6) | <0.0001 |
| Statin use (%) | 277,520 (26.1) | 102,071 (26.9) | 44,274 (35.6) | 14,639 (38.6) | <0.0001 |
| Laboratory results | |||||
| Fasting glucose (mg/dL) | 144.1 ± 45.8 | 152.9 ± 47.1 | 138.9 ± 48.6 | 147.8 ± 52.3 | <0.0001 |
| Total cholesterol (mg/dL) | 195.3 ± 43.6 | 211.9 ± 47.4 | 194.8 ± 45.1 | 209.1 ± 50.8 | <0.0001 |
| Triglyceride (mg/dL) † | 122.2 (122.1, 122.3) | 232.7 (232.3, 233.0) | 131.6 (131.3, 132.0) | 231.7 (230.5, 233.0) | <0.0001 |
| HDL-cholesterol (mg/dL) | 53.1 ± 23.8 | 49.1 ± 32.1 | 53.1 ± 40.0 | 55.7 ± 62.4 | <0.0001 |
| Urine Protein | |||||
| Negative | 983,624 (92.3) | 335,195 (88.3) | 103,959 (83.5) | 30,280 (79.9) | <0.0001 |
| Trace | 32,872 (3.1) | 15,754 (4.2) | 5174 (4.2) | 1808 (4.8) | |
| 1+ | 30,976 (2.9) | 17,327 (4.6) | 7274 (5.8) | 2732 (7.2) | |
| 2+ | 13,212 (1.2) | 8457 (2.2) | 5212 (4.2) | 1985 (5.2) | |
| 3,4+ | 3728 (0.4) | 2432 (0.6) | 2354 (1.9) | 893 (2.4) |
| Number of Subjects | Number of Events | Incidence Rate (1000 p-y) | Model 1 | Model 2 | Model 3 | After IPTW | |
|---|---|---|---|---|---|---|---|
| Adjusted HR (95% CI) | |||||||
| Myocardial Infarction | |||||||
| No CKD/No NAFLD | 1,065,190 | 24,759 | 3.35 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| No CKD/NAFLD | 379,638 | 8617 | 3.28 | 1.18 (1.15–1.21) | 1.16 (1.13–1.19) | 1.21 (1.18–1.25) | 1.27 (1.24–1.31) |
| CKD/No NAFLD | 124,507 | 5752 | 6.85 | 1.45 (1.40–1.49) | 1.33 (1.29–1.37) | 1.33 (1.30–1.37) | 1.18 (1.24–1.31) |
| CKD/NAFLD | 37,897 | 1735 | 6.68 | 1.56 (1.49–1.64) | 1.43 (1.36–1.50) | 1.49 (1.42–1.57) | 1.58 (1.50–1.67) |
| Stroke | |||||||
| No CKD/No NAFLD | 1,065,190 | 36,027 | 4.90 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| No CKD/NAFLD | 379,638 | 11,468 | 4.39 | 1.18 (1.15–1.20) | 1.14 (1.11–1.16) | 1.21 (1.18–1.24) | 1.33 (1.30–1.11) |
| CKD/No NAFLD | 124,507 | 8340 | 10.04 | 1.28 (1.25–1.31) | 1.19 (1.16–1.22) | 1.19 (1.16–1.22) | 1.08 (1.05–1.11) |
| CKD/NAFLD | 37,897 | 2592 | 10.10 | 1.51 (1.45–1.57) | 1.37 (1.32-1.43) | 1.48 (1.41–1.54) | 1.54 (1.47–1.62) |
| Overall mortality | |||||||
| No CKD/No NAFLD | 1,065,190 | 70,966 | 9.51 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| No CKD/NAFLD | 379,638 | 19,468 | 7.35 | 1.09 (1.07–1.11) | 1.10 (1.08–1.11) | 1.54 (1.52–1.57) | 1.69 (1.66–1.72) |
| CKD/No NAFLD | 124,507 | 21,250 | 24.90 | 1.46 (1.44–1.48) | 1.39 (1.37–1.42) | 1.41 (1.39–1.43) | 1.17 (1.15–1.19) |
| CKD/NAFLD | 37,897 | 5293 | 20.04 | 1.41 (1.37–1.45) | 1.37 (1.33–1.40) | 2.00 (1.94–2.06) | 2.13 (2.06–2.21) |
| Cardiovascular mortality | |||||||
| No CKD/No NAFLD | 1,065,190 | 12,490 | 1.67 | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| No CKD/NAFLD | 379,638 | 3349 | 1.26 | 1.14 (1.10–1.19) | 1.09 (1.05–1.14) | 1.47 (1.41–1.54) | 1.57 (1.51–1.63) |
| CKD/No NAFLD | 124,507 | 4659 | 5.46 | 1.67 (1.62–1.73) | 1.55 (1.50–1.61) | 1.57 (1.51–1.62) | 1.34 (1.29–1.40) |
| CKD/NAFLD | 37,897 | 1190 | 4.50 | 1.75 (1.65–1.85) | 1.58 (1.49–1.68) | 2.20 (2.07–2.35) | 2.31 (2.15–2.49) |
| AAR | Number of Subjects | Number of Events | Incidence of Event (1000 Person-Years) | Model 1 | Model 2 | |
|---|---|---|---|---|---|---|
| Adjusted HR (95% CI) | ||||||
| Myocardial Infarction | ||||||
| Non-CKD | <0.8 | 180,271 | 3576 | 2.85 | 1 (reference) | 1 (reference) |
| <1.4 | 173,116 | 4266 | 3.56 | 0.96 (0.91,1.00) | 1.01 (0.96, 1.05) | |
| ≥1.4 | 26,251 | 775 | 4.42 | 1.08 (1.00, 1.17) | 1.13 (1.04, 1.23) | |
| CKD | <0.8 | 11,787 | 444 | 5.34 | 1.30 (1.18, 1.44) | 1.21 (1.09, 1.34) |
| <1.4 | 21,347 | 1047 | 7.18 | 1.41 (1.31, 1.51) | 1.35 (1.26, 1.46) | |
| ≥1.4 | 4763 | 244 | 7.93 | 1.43 (1.25,1.63) | 1.38 (1.21, 1.58) | |
| Stroke | ||||||
| Non-CKD | <0.8 | 180,271 | 3889 | 3.11 | 1 (reference) | 1 (reference) |
| <1.4 | 173,116 | 6332 | 5.32 | 1.13 (1.08, 1.17) | 1.14 (1.09, 1.19) | |
| ≥1.4 | 26,251 | 1247 | 7.18 | 1.30 (1.22, 1.39) | 1.29 (1.20, 1.37) | |
| CKD | <0.8 | 11,787 | 564 | 6.82 | 1.25 (1.14, 1.37) | 1.15 (1.05, 1.26) |
| <1.4 | 21,347 | 1600 | 11.13 | 1.45 (1.36, 1.54) | 1.38 (1.29, 1.46) | |
| ≥1.4 | 4763 | 428 | 14.14 | 1.57 (1.42, 1.74) | 1.50 (1.36, 1.67) | |
| Overall mortality | ||||||
| Non-CKD | <0.8 | 180,271 | 5452 | 4.32 | 1 (reference) | 1 (reference) |
| <1.4 | 173,116 | 10,646 | 8.81 | 1.24 (1.20, 1.29) | 1.26 (1.22, 1.31) | |
| ≥1.4 | 26,251 | 3370 | 19.02 | 2.22 (2.12, 2.32) | 2.16 (2.06, 2.25) | |
| CKD | <0.8 | 11,787 | 1015 | 12.03 | 1.40 (1.31,1.50) | 1.32 (1.23, 1.41) |
| <1.4 | 21,347 | 3185 | 21.46 | 1.75 (1.67, 1.84) | 1.71 (1.63, 1.79) | |
| ≥1.4 | 4763 | 1093 | 34.87 | 2.44 (2.28, 2.61) | 2.36 (2.20, 2.52) | |
| Cardiovascular mortality | ||||||
| Non-CKD | <0.8 | 180,271 | 949 | 0.75 | 1 (reference) | 1 (reference) |
| <1.4 | 173,116 | 1864 | 1.54 | 1.19 (1.10, 1.29) | 1.23 (1.14, 1.34) | |
| ≥1.4 | 26,251 | 536 | 3.02 | 1.92 (1.72,2.14) | 1.93 (1.73, 2.15) | |
| CKD | <0.8 | 11,787 | 226 | 2.68 | 1.70 (1.47, 1.97) | 1.56 (1.35, 1.81) |
| <1.4 | 21,347 | 729 | 4.91 | 2.08 (1.88, 2.31) | 2.00 (1.81, 2.22) | |
| ≥1.4 | 4763 | 235 | 7.50 | 2.65 (2.28, 3.07) | 2.57 (2.21, 2.98) | |
| Urine Protein | Number of Subjects | Number of Events | Incidence of Event (1000 p-y) | Multivariate Model HR (95% CI) | After IPTW HR (95% CI) | |
|---|---|---|---|---|---|---|
| Myocardial Infarction | ||||||
| Non-NAFLD | Negative | 103,959 | 4286 | 6.04 | 1 (reference) | 1 (reference) |
| Trace | 5174 | 258 | 7.45 | 1.17 (1.04–1.33) | 1.14 (1.00–1.29) | |
| 1+ | 7274 | 496 | 10.68 | 1.59 (1.44–1.75) | 1.50 (1.36–1.65) | |
| 2+ | 5212 | 438 | 13.64 | 2.01 (1.82–2.22) | 1.77 (1.60–1.96) | |
| 3,4+ | 2888 | 274 | 15.74 | 2.34 (2.06–2.65) | 1.93 (1.70–2.19) | |
| NAFLD | Negative | 30,280 | 1219 | 5.82 | 1.19 (1.11–1.28) | 1.23 (1.15–1.32) |
| Trace | 1808 | 81 | 6.51 | 1.29 (1.03–1.61) | 1.30 (1.05–1.61) | |
| 1+ | 2732 | 162 | 8.84 | 1.64 (1.40–1.93) | 1.55 (1.32–1.82) | |
| 2+ | 1985 | 169 | 13.20 | 2.43 (2.08–2.85) | 2.29 (1.96–2.68) | |
| 3,4+ | 1092 | 104 | 15.44 | 2.91 (2.38–3.55) | 2.57 (2.11–3.13) | |
| Stroke | ||||||
| Non-NAFLD | Negative | 103,959 | 6401 | 9.12 | 1 (reference) | 1 (reference) |
| Trace | 5174 | 406 | 11.88 | 1.25 (1.13–1.38) | 1.21 (1.09–1.34) | |
| 1+ | 7274 | 644 | 14.01 | 1.40 (1.29–1.52) | 1.30 (1.20–1.42) | |
| 2+ | 5212 | 521 | 16.37 | 1.66 (1.52–1.82) | 1.47 (1.34–1.61) | |
| 3,4+ | 2888 | 368 | 21.65 | 2.33 (2.09–2.59) | 1.92 (1.73–2.14) | |
| NAFLD | Negative | 30,280 | 18,979 | 9.16 | 1.25 (1.18–1.33) | 1.30 (1.22–1.37) |
| Trace | 1808 | 138 | 11.25 | 1.49 (1.25–1.77) | 1.57 (1.34–1.85) | |
| 1+ | 2732 | 239 | 13.25 | 1.66 (1.46–1.90) | 1.62 (1.42–1.85) | |
| 2+ | 1985 | 182 | 14.36 | 1.81 (1.56–2.11) | 1.68 (1.45–1.95) | |
| 3,4+ | 1092 | 136 | 20.59 | 2.74 (2.30–3.25) | 2.40 (2.04–2.84) | |
| Overall mortality | ||||||
| Non-NAFLD | Negative | 103,959 | 16,002 | 22.24 | 1 (reference) | 1 (reference) |
| Trace | 5174 | 1027 | 29.14 | 1.25 (1.29–1.34) | 1.20 (1.23–1.28) | |
| 1+ | 7274 | 1788 | 37.60 | 1.55 (1.48–1.63) | 1.41 (1.34–1.48) | |
| 2+ | 5212 | 1492 | 45.02 | 1.98 (1.87–2.09) | 1.63 (1.54–1.72) | |
| 3,4+ | 2888 | 941 | 52.43 | 2.59 (2.42–2.76) | 1.92 (1.80–2.05) | |
| NAFLD | Negative | 30,280 | 3783 | 17.79 | 1.38 (1.32–1.43) | 1.47 (1.41–1.53) |
| Trace | 1808 | 284 | 22.49 | 1.85 (1.68–2.03) | 1.84 (1.64–2.05) | |
| 1+ | 2732 | 482 | 25.74 | 1.33 (1.30–1.37) | 1.89 (1.73–2.07) | |
| 2+ | 1985 | 453 | 34.40 | 2.56 (2.32–2.81) | 2.45 (2.24–2.69) | |
| 3,4+ | 1092 | 291 | 41.76 | 3.53 (3.14–3.98) | 3.09 (2.77–3.45) | |
| Cardiovascular mortality | ||||||
| Non-NAFLD | Negative | 103,959 | 3469 | 4.82 | 1 (reference) | 1 (reference) |
| Trace | 5174 | 235 | 6.67 | 1.34 (1.17–1.53) | 1.28 (1.12–1.47) | |
| 1+ | 7274 | 429 | 9.02 | 1.77 (1.60–1.96) | 1.59 (1.43–1.76) | |
| 2+ | 5212 | 321 | 9.69 | 2.07 (1.84–2.33) | 1.69 (1.50–1.89) | |
| 3,4+ | 2888 | 205 | 11.42 | 2.81 (2.44–3.25) | 2.07 (1.80–2.38) | |
| NAFLD | Negative | 30,280 | 836 | 3.93 | 1.36 (1.24–1.48) | 1.41 (1.30–1.53) |
| Trace | 1808 | 69 | 5.46 | 1.86 (1.46–2.37) | 2.05 (1.65–2.54) | |
| 1+ | 2732 | 120 | 6.41 | 2.09 (1.73–2.52) | 2.04 (1.70–2.43) | |
| 2+ | 1985 | 99 | 7.52 | 2.60 (2.12–3.19) | 2.49 (2.06–3.00) | |
| 3,4+ | 1092 | 66 | 9.47 | 3.77 (2.94–4.83) | 3.30 (2.64–4.13) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, G.-E.; Han, K.; Lee, K.-N.; Cho, E.-J.; Bae, J.-H.; Yang, S.-Y.; Yu, S.-J.; Choi, S.-H.; Yim, J.-Y.; Heo, N.-J. Combined Effects of Chronic Kidney Disease and Nonalcoholic Fatty Liver Disease on the Risk of Cardiovascular Disease in Patients with Diabetes. Biomedicines 2022, 10, 1245. https://doi.org/10.3390/biomedicines10061245
Chung G-E, Han K, Lee K-N, Cho E-J, Bae J-H, Yang S-Y, Yu S-J, Choi S-H, Yim J-Y, Heo N-J. Combined Effects of Chronic Kidney Disease and Nonalcoholic Fatty Liver Disease on the Risk of Cardiovascular Disease in Patients with Diabetes. Biomedicines. 2022; 10(6):1245. https://doi.org/10.3390/biomedicines10061245
Chicago/Turabian StyleChung, Goh-Eun, Kyungdo Han, Kyu-Na Lee, Eun-Ju Cho, Jung-Ho Bae, Sun-Young Yang, Su-Jong Yu, Seung-Ho Choi, Jeong-Yoon Yim, and Nam-Ju Heo. 2022. "Combined Effects of Chronic Kidney Disease and Nonalcoholic Fatty Liver Disease on the Risk of Cardiovascular Disease in Patients with Diabetes" Biomedicines 10, no. 6: 1245. https://doi.org/10.3390/biomedicines10061245
APA StyleChung, G.-E., Han, K., Lee, K.-N., Cho, E.-J., Bae, J.-H., Yang, S.-Y., Yu, S.-J., Choi, S.-H., Yim, J.-Y., & Heo, N.-J. (2022). Combined Effects of Chronic Kidney Disease and Nonalcoholic Fatty Liver Disease on the Risk of Cardiovascular Disease in Patients with Diabetes. Biomedicines, 10(6), 1245. https://doi.org/10.3390/biomedicines10061245