
Needle-Probe Optical Coherence Tomography for Real-Time Visualization of Veress Peritoneal Needle Placement in a Porcine Model: A New Safety Concept for Pneumoperitoneum Establishment in Laparoscopic Surgery

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
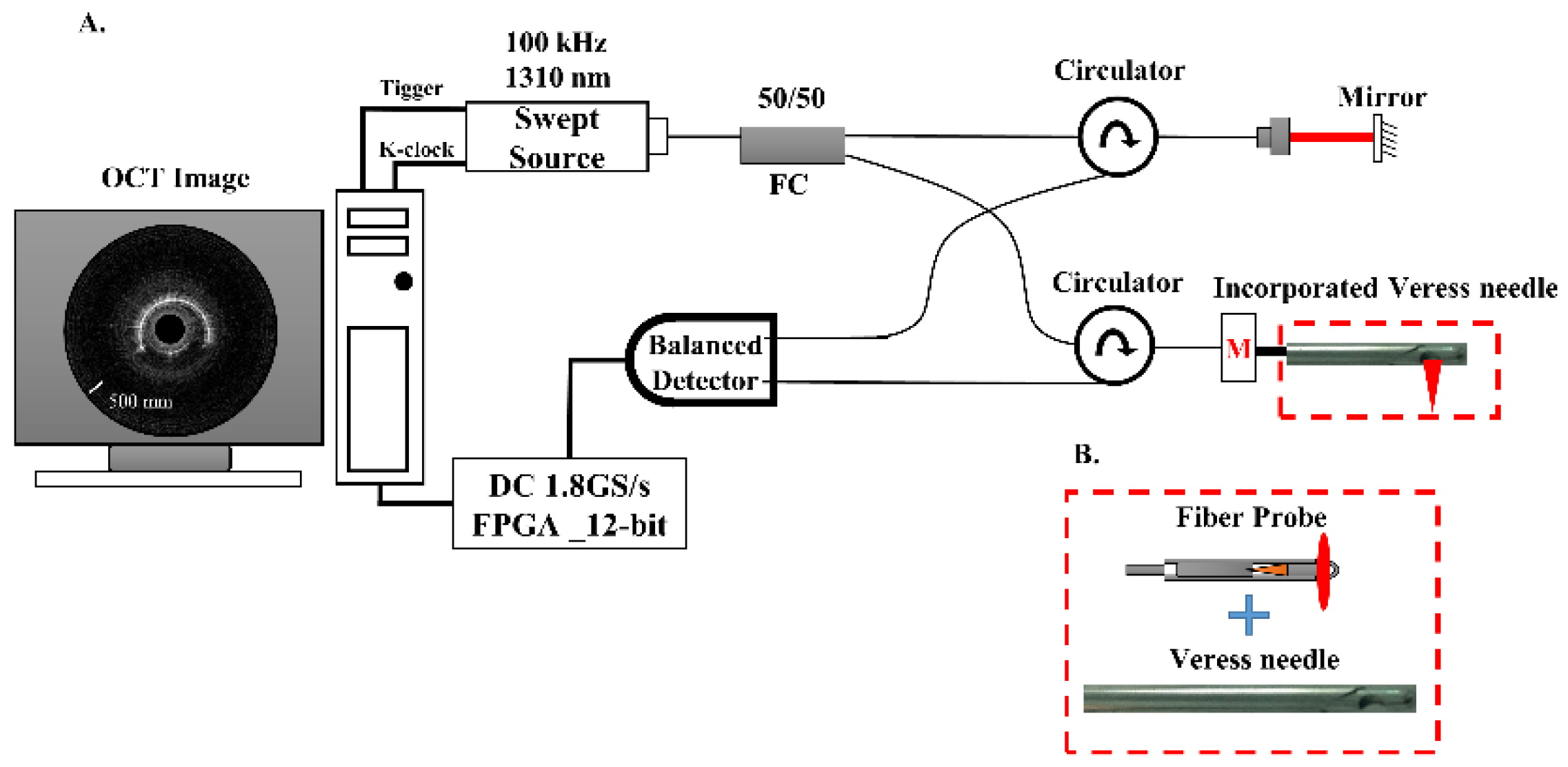
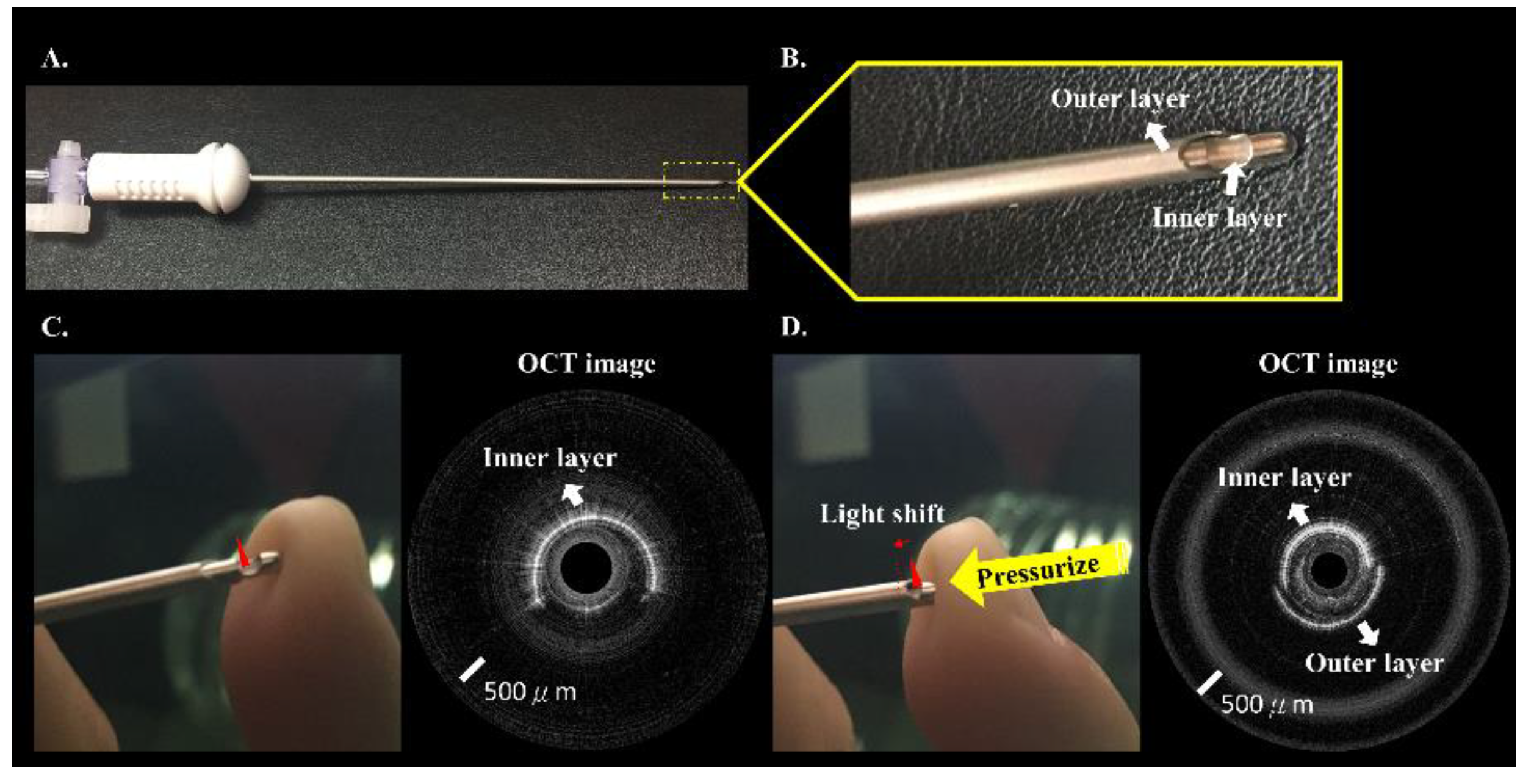
2.2. Incorporated Veress Needle and Fiber-Probe SSOCT System
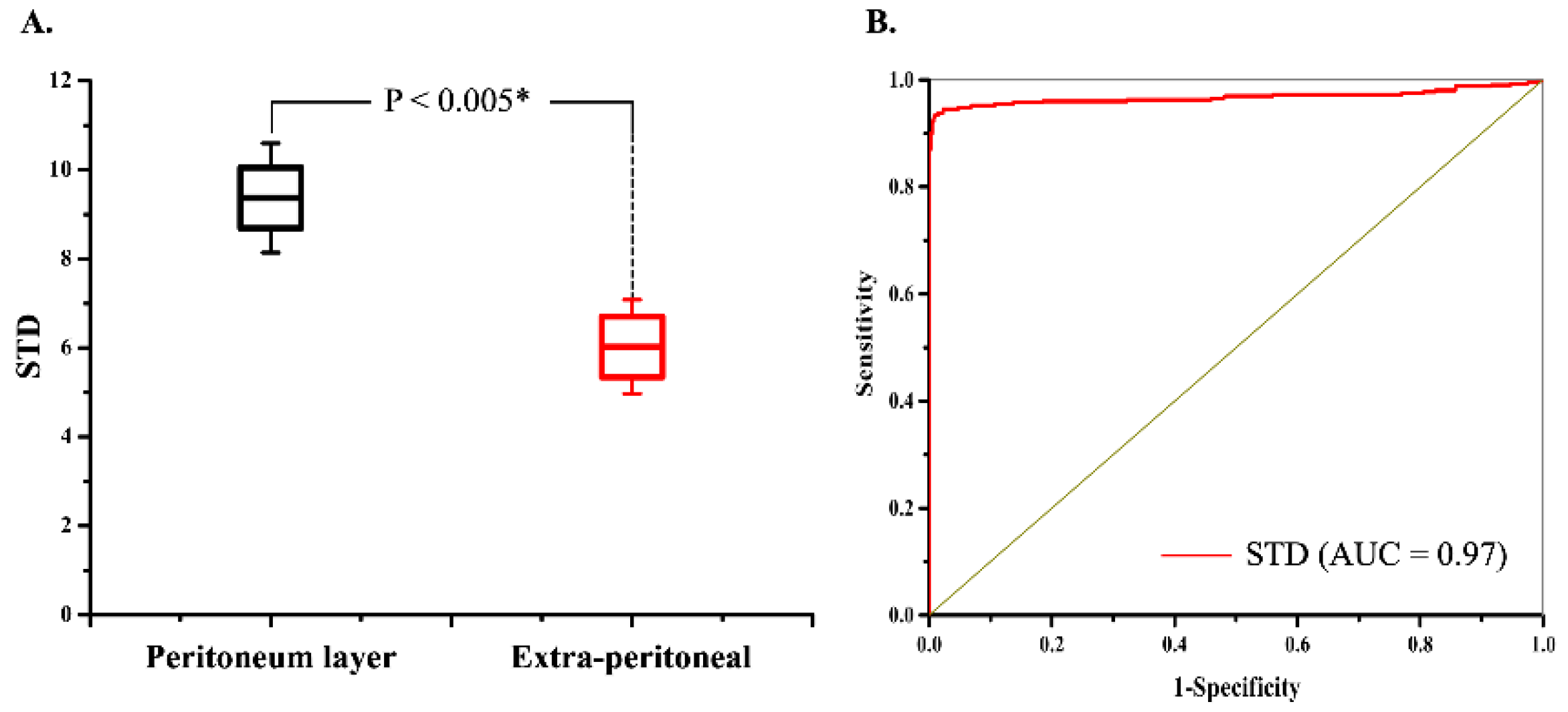
2.3. Quantitative Parameter Measurement and Statistical Analysis
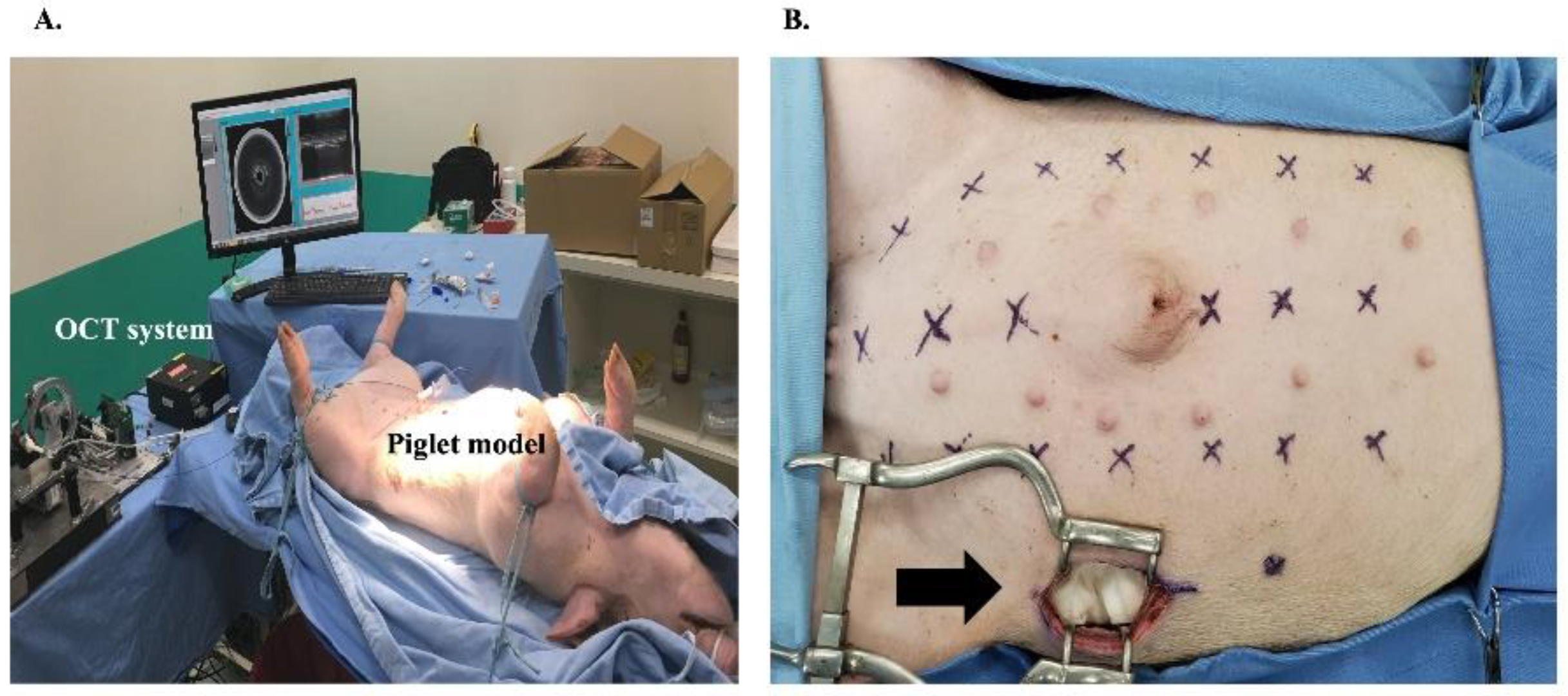
2.4. Porcine Model
2.5. Experimental Conditions
2.6. Primary and Secondary Outcomes
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Moberg, A.C.; Montgomery, A. Primary access related complications with laparoscopy: Comparison of blind and open techniques. Surg. Endosc. 2005, 19, 1196–1199. [Google Scholar] [CrossRef] [PubMed]
- Molloy, D.; Kaloo, P.D.; Cooper, M.; Nguyen, T.V. Laparoscopic entry: A literature review and analysis of techniques and complications of primary port entry. Aust. N. Z. J. Obstet. Gynaecol. 2002, 2, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.W.; Kapiteyn, K.; Trimpos, T.; Herman, J. Complication of laparoscopy: A prospective multicentre observational study. Br. J. Obstet. Gynaecol. 1997, 104, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.W.; Kolkman, W.; Bakkum, E.A.; de Kroon, C.D.; Trimbos-Kemper, T.C.M.; Trimbos, J.B. Complications of laparoscopy: An inquiry about closed versus open-entry technique. Am. J. Obstet. Gynecol. 2004, 190, 634–638. [Google Scholar] [CrossRef]
- Schafer, M.; Lauper, M.; Krahenbuhl, L. Trocar and Veress needle injuries during laparoscopy. Surg. Endosc. 2001, 15, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, J.L.; Azevedo, O.C.; Miyahira, S.A.; Miguel, G.P.; Becker, O.M., Jr.; Hypólito, O.H.M.; Machado, A.C.C.G.; Cardia, W.; Yamaguchi, G.A.; Godinho, L.; et al. Injuries caused by Veress needle insertion for creation of pneumoperitoneum: A systematic literature review. Surg. Endosc. 2009, 23, 1428–1432. [Google Scholar] [CrossRef]
- Wherry, D.C.; Marohn, M.R.; Malanoski, M.P.; Hetz, S.P.; Rieh, N.M. An external audit of laparoscopic cholecystectomy in the steady state performed in medical treatment facilities of the Department of Defense. Ann. Surg. 1996, 224, 145–154. [Google Scholar] [CrossRef]
- Jamil, M.; Niaz, K.; Tahir, F. Closed vs. open method of pneumoperitonium at infra-umbilical site in laparoscopic surgery—A comparative study. J. Pak. Med. Assoc. 2018, 68, 1478–1482. [Google Scholar]
- Mikhail, E.; Tamhane, N.; Sarkar, P.; Sappenfield, E.; Tanner, J.P.; Imudia, A.N. Laparoscopic entry technique using a Veress needle insertion with and without concomitant CO2 insufflation: A randomized controlled trial. J. Minim. Invasive Gynecol. 2019, 26, 1383–1388. [Google Scholar] [CrossRef]
- Pini Prato, A.; Palo, F.; Faticato, M.G.; Carlini, C.; Mattioli, G. Safety of Veress needle for laparoscopic entry in children: Myth or reality? J. Pediatr. Surg. 2021, 56, 569–572. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Zelić, A.; Jukić, M.; Llorente Muñoz, C.M. The safety and effectiveness of laparoscopic pyloromyotomy using 3-mm electrocautery hook versus open surgery for treatment of hypertrophic pyloric stenosis in infants. Children 2021, 8, 701. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Beara, V.; Jukić, M.; Rashwan, H.; Šušnjar, T. A new approach to laparoscopic appendectomy in children-clipless/sutureless Harmonic scalpel laparoscopic appendectomy. Langenbeck’s Arch. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Krishnakumar, S.; Tambe, P. Entry complications in laparoscopic surgery. J. Gynecol. Endosc. Surg. 2009, 1, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Riek, S.; Bachmann, K.H.; Gaiselmann, T.; Hoernstein, F.; Marzusch, K. A new insufflation needle with a special optical system for use in laparoscopic procedures. Obstet. Gynecol. 1994, 84, 476–478. [Google Scholar] [PubMed]
- Riek, S.; Bachmann, K.H.; Gaiselmann, T.; Fischer, S.C.; Raestrup, H.; Buess, G.F.; Bartzke, G. Veress needle with optical protective shield and step system: A new safety concept in minimally invasive surgery. Minim. Invasive Ther. Allied Technol. 1999, 8, 245–254. [Google Scholar] [CrossRef]
- Wojtkowski, M. High-speed optical coherence tomography: Basics and applications. Appl. Opt. 2010, 49, D30–D61. [Google Scholar] [CrossRef]
- Teng, W.N.; Kao, M.C.; Ting, C.K.; Kuo, W.C. Fibre-needle Swept-source Optical Coherence Tomography for the Real-time Visualization of the Fascia Plane Block Procedure in a Swine Model. Anesth. Analg. 2021, 133, 526–534. [Google Scholar] [CrossRef]
- Kuo, W.C.; Kao, M.C.; Ting, C.K.; Teng, W.N. Optical coherence tomography needle probe in neuraxial block application. IEEE J. Sel. Top. Quantum Electron. 2021, 27, 1–6. [Google Scholar] [CrossRef]
- Hasson, H.M. A modified instrument and method for laparoscopy. Am. J. Obstet. Gynecol. 1971, 110, 886–887. [Google Scholar] [CrossRef]
- Larobina, M.; Nottle, P. Complete evidence regarding major vascular injuries during laparoscopic access. Surg. Laparosc. Endosc. Percutan. Tech. 2005, 15, 119–123. [Google Scholar] [CrossRef]
- Nevler, A.; Har-Zahav, G.; Rosin, D.; Gutman, M. Safer trocar insertion for closed laparoscopic access: Ex vivo assessment of an improved Veress needle. Surg. Endosc. 2016, 30, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Postema, R.R.; Cefai, D.; van Straten, B.; Miedema, R.; Hardjo, L.L.; Dankelman, J.; Nickel, F.; Horeman-Franse, T. A novel Veress needle mechanism that reduces overshooting after puncturing the abdominal wall. Surg. Endosc. 2021, 35, 5857–5866. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
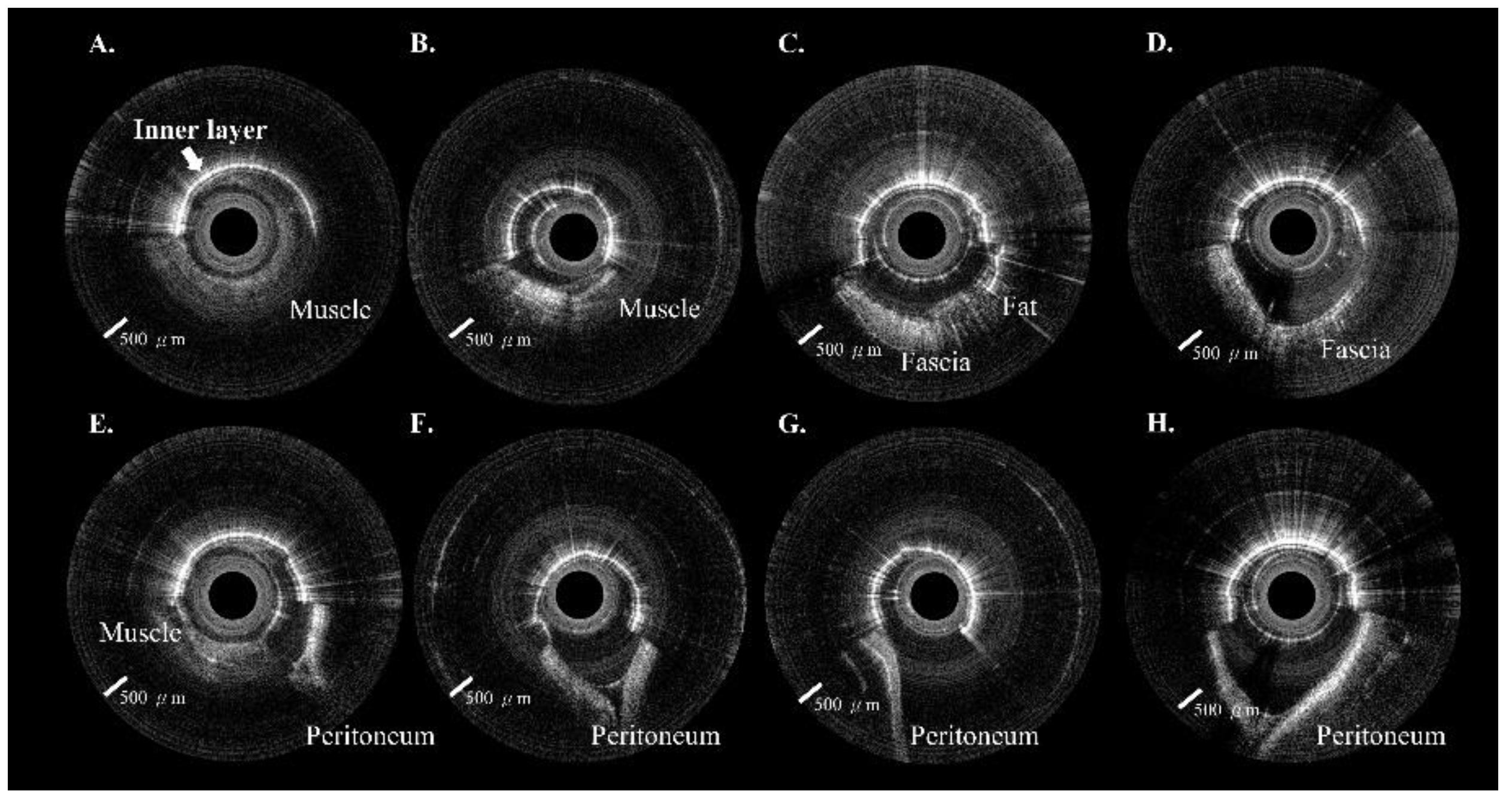
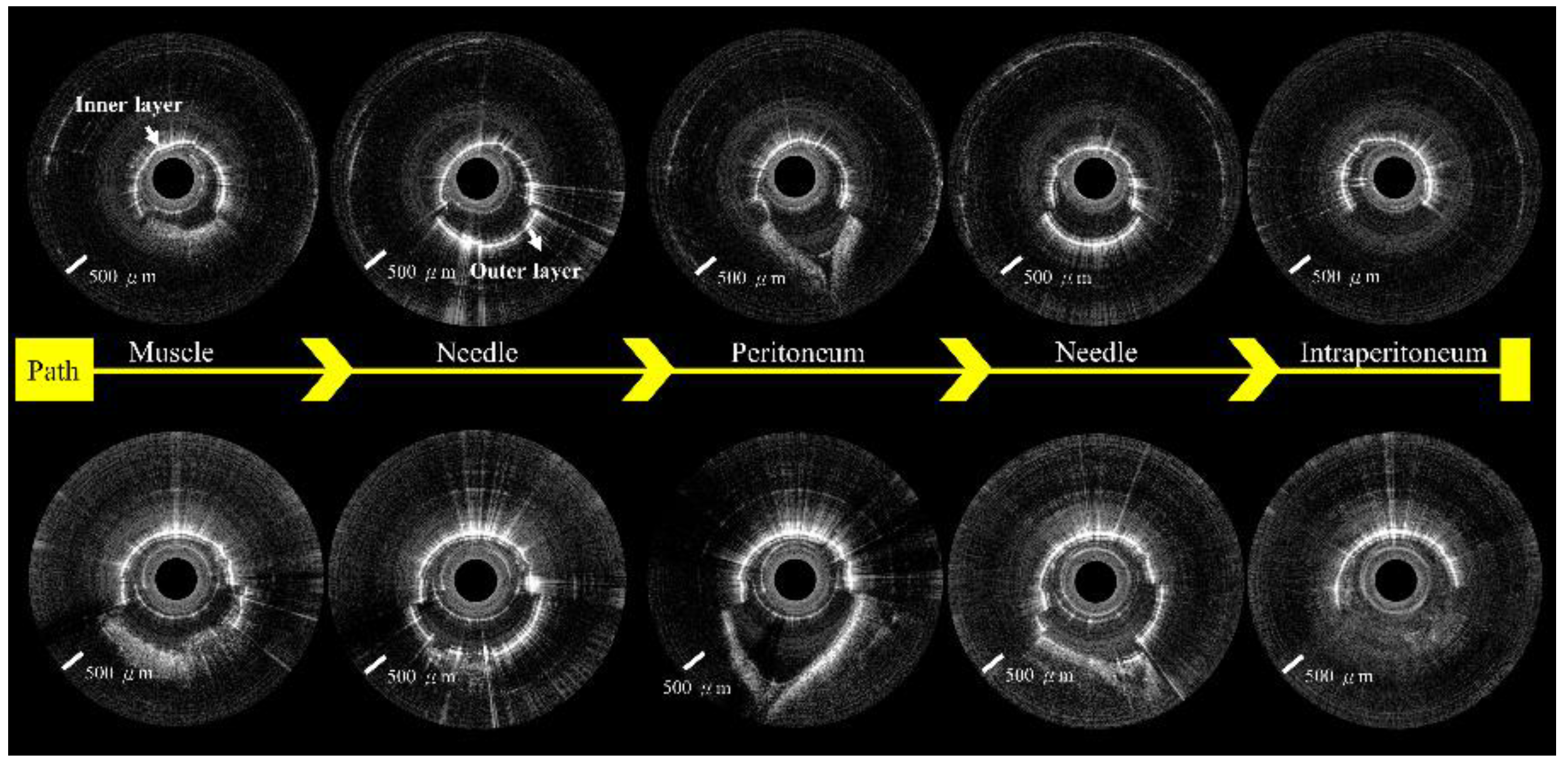
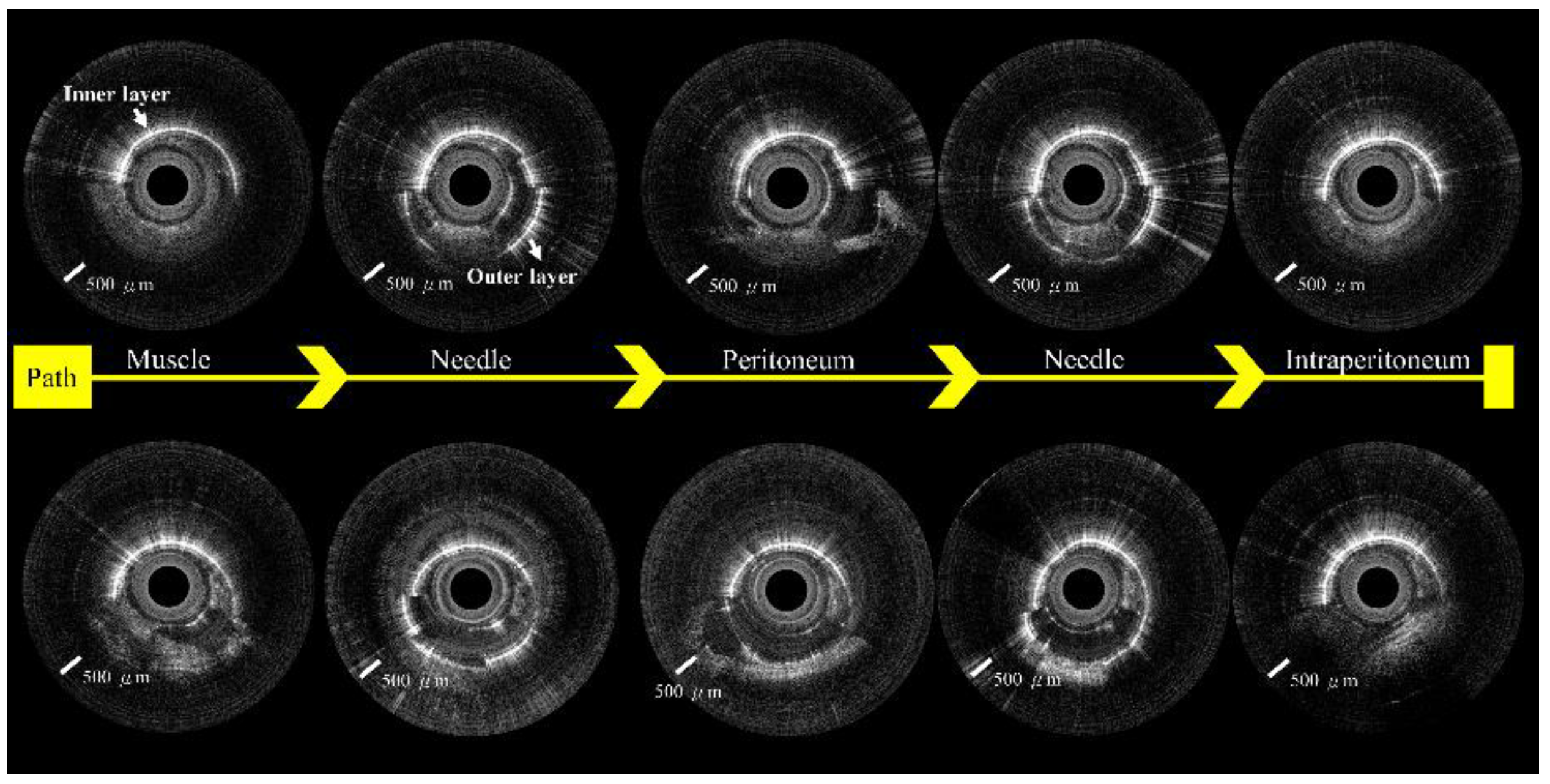
| Tissue Type | Characteristic Features Visible on OCT Images | |
|---|---|---|
| Extra-peritoneal tissue | Muscle | Non-uniform signal distribution, presence of layered structures |
| Fascia | Speckled bright reflections indicating adipose tissue, less imaging penetration depth than muscle tissue, V-shaped concave pattern | |
| Peritoneum | Strong and homogeneous laminar layer, deep V-shaped concave pattern | |
| Intraperitoneal tissue | Appearance of numerous empty spaces, no reflective signal, or homogeneous laminar layer tissue |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, E.Y.-H.; Kao, M.-C.; Ting, C.-K.; Huang, W.J.S.; Yeh, Y.-T.; Ke, H.-H.; Kuo, W.-C. Needle-Probe Optical Coherence Tomography for Real-Time Visualization of Veress Peritoneal Needle Placement in a Porcine Model: A New Safety Concept for Pneumoperitoneum Establishment in Laparoscopic Surgery. Biomedicines 2022, 10, 485. https://doi.org/10.3390/biomedicines10020485
Huang EY-H, Kao M-C, Ting C-K, Huang WJS, Yeh Y-T, Ke H-H, Kuo W-C. Needle-Probe Optical Coherence Tomography for Real-Time Visualization of Veress Peritoneal Needle Placement in a Porcine Model: A New Safety Concept for Pneumoperitoneum Establishment in Laparoscopic Surgery. Biomedicines. 2022; 10(2):485. https://doi.org/10.3390/biomedicines10020485
Chicago/Turabian StyleHuang, Eric Yi-Hsiu, Meng-Chun Kao, Chien-Kun Ting, William J. S. Huang, Yi-Ting Yeh, Hui-Hsuan Ke, and Wen-Chuan Kuo. 2022. "Needle-Probe Optical Coherence Tomography for Real-Time Visualization of Veress Peritoneal Needle Placement in a Porcine Model: A New Safety Concept for Pneumoperitoneum Establishment in Laparoscopic Surgery" Biomedicines 10, no. 2: 485. https://doi.org/10.3390/biomedicines10020485
APA StyleHuang, E. Y.-H., Kao, M.-C., Ting, C.-K., Huang, W. J. S., Yeh, Y.-T., Ke, H.-H., & Kuo, W.-C. (2022). Needle-Probe Optical Coherence Tomography for Real-Time Visualization of Veress Peritoneal Needle Placement in a Porcine Model: A New Safety Concept for Pneumoperitoneum Establishment in Laparoscopic Surgery. Biomedicines, 10(2), 485. https://doi.org/10.3390/biomedicines10020485