
Extracorporeal Shock Wave Therapy Combined with Platelet-Rich Plasma during Preventive and Therapeutic Stages of Intrauterine Adhesion in a Rat Model

 ,
, 
 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Animals
2.3. Establishment of the IUA Model
2.4. Preparation and Isolation of PRP
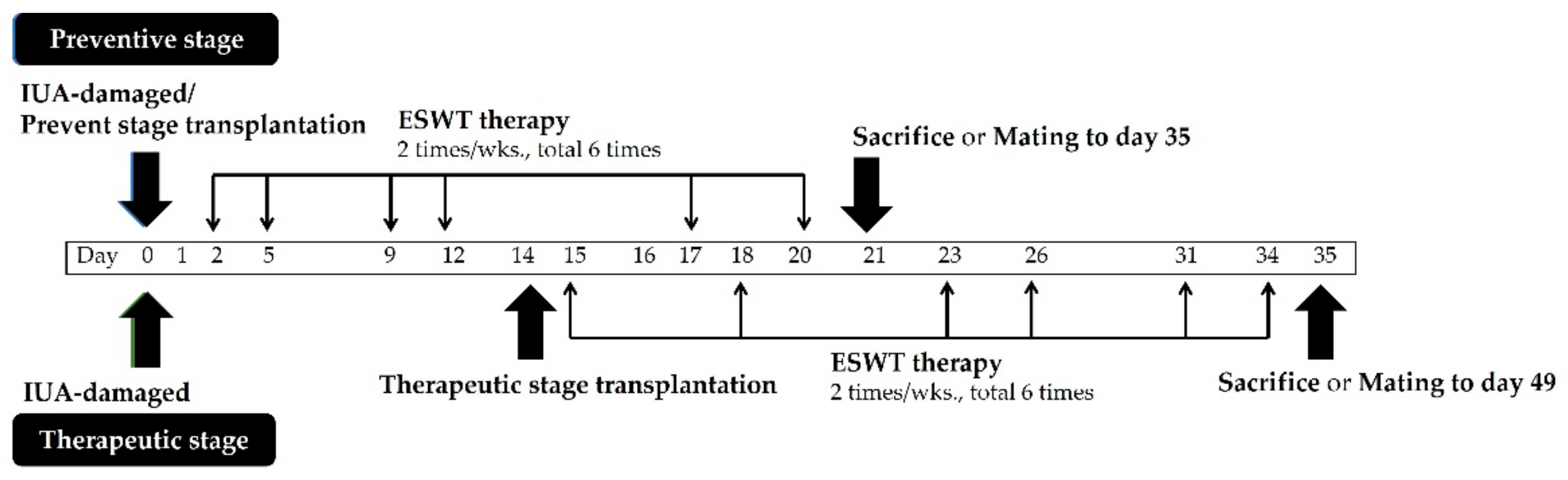
2.5. E2 and PRP Treatment during Preventive and Therapeutic Stages of the IUA Model
2.6. ESWT for IUA Model
2.7. Mating of Rats
2.8. Histological Analysis
2.9. Immunohistochemical Staining
2.10. RNA Extraction, Reverse Transcription, and Quantitative Real-Time Polymerase Chain Reaction
2.11. Statistical Analysis
3. Results
3.1. Effects of E2 or PRP Transplantation Combined with ESWT on Body Weight in IUA Female Rats
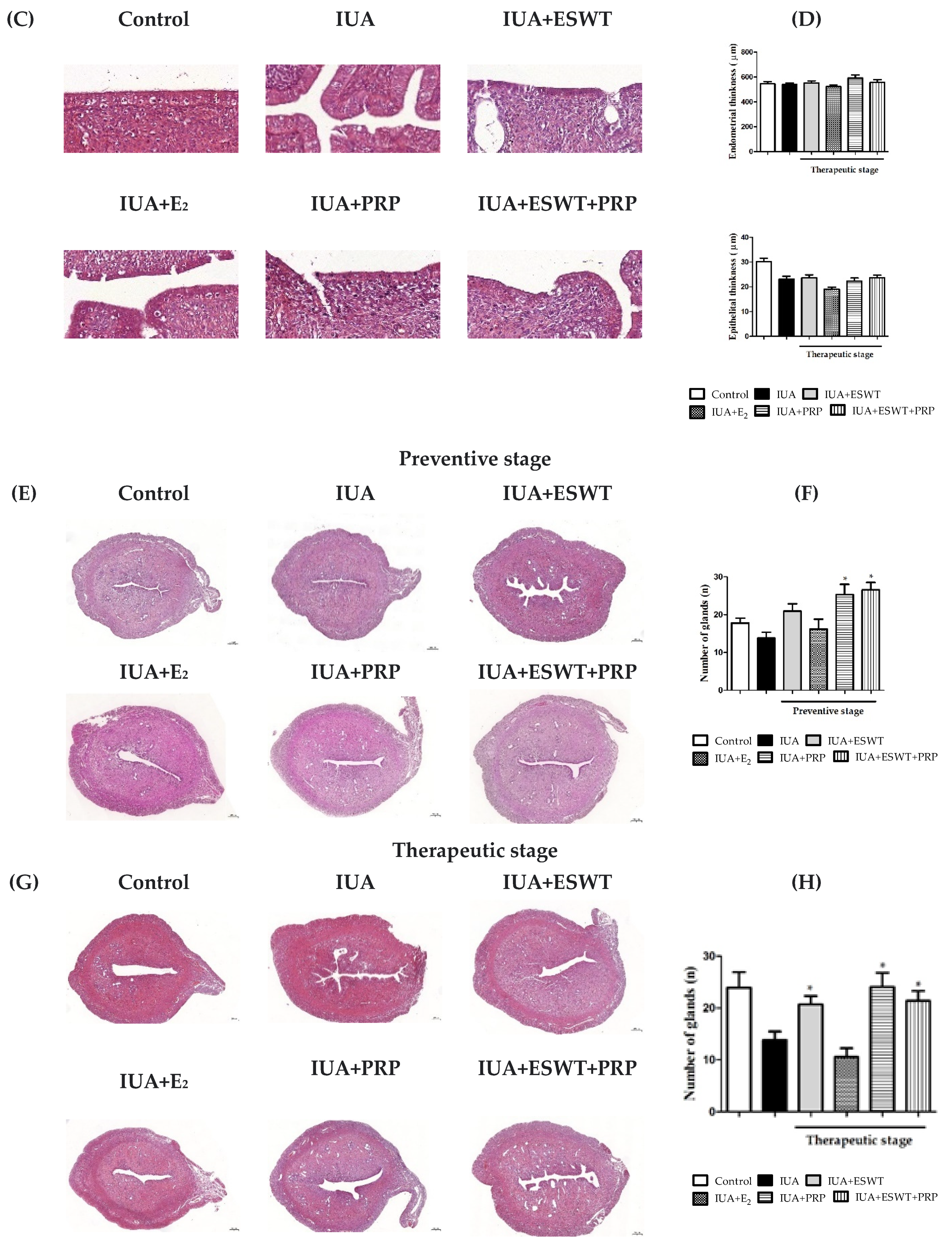
3.2. PRP and ESWT Combined with PRP Transplantation Restored Endometrial Morphology in an IUA Rat Model
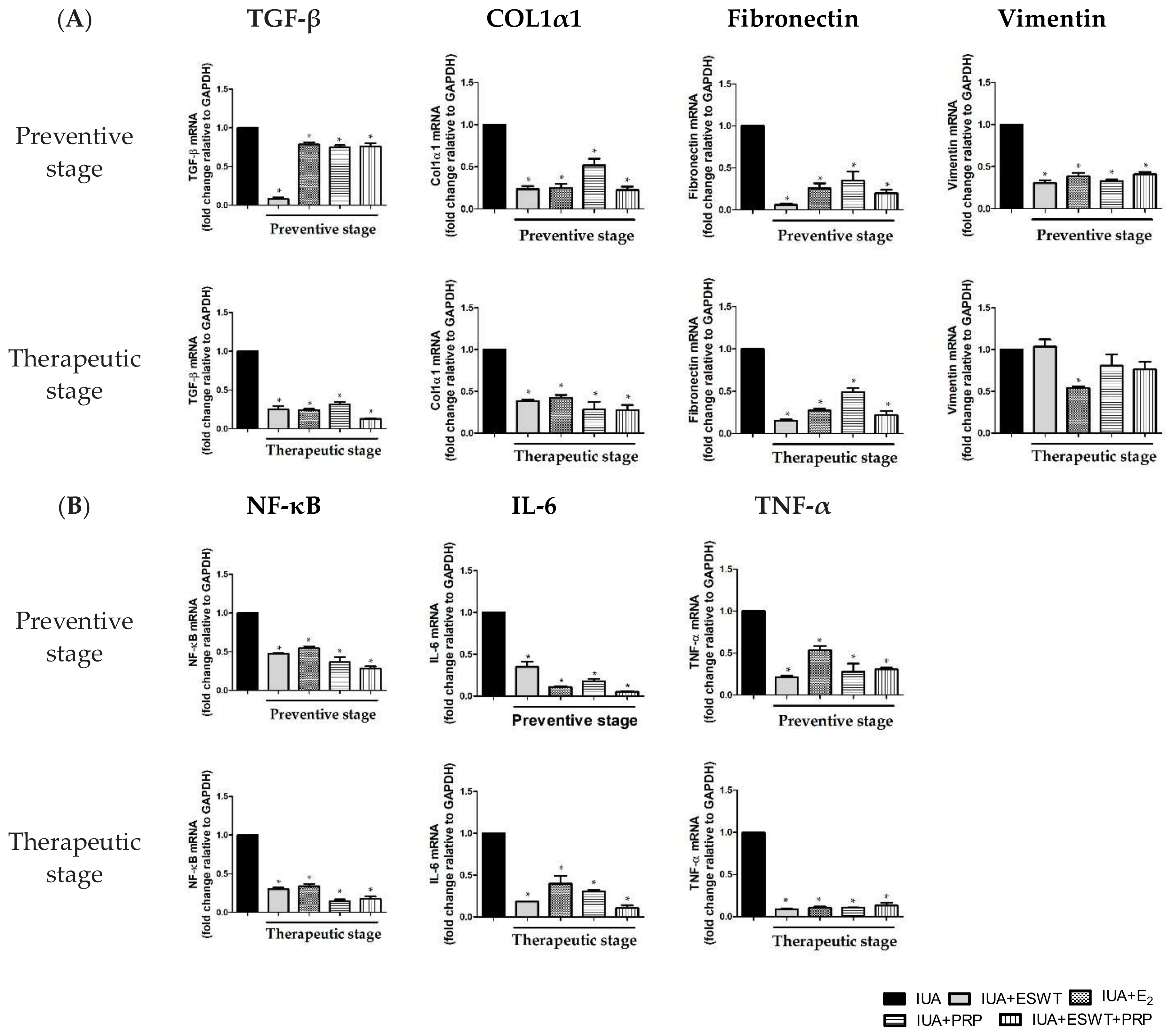
3.3. ESWT, E2, PRP, and ESWT Combined with PRP Transplantation Improved Fibrosis in an IUA Rat Model
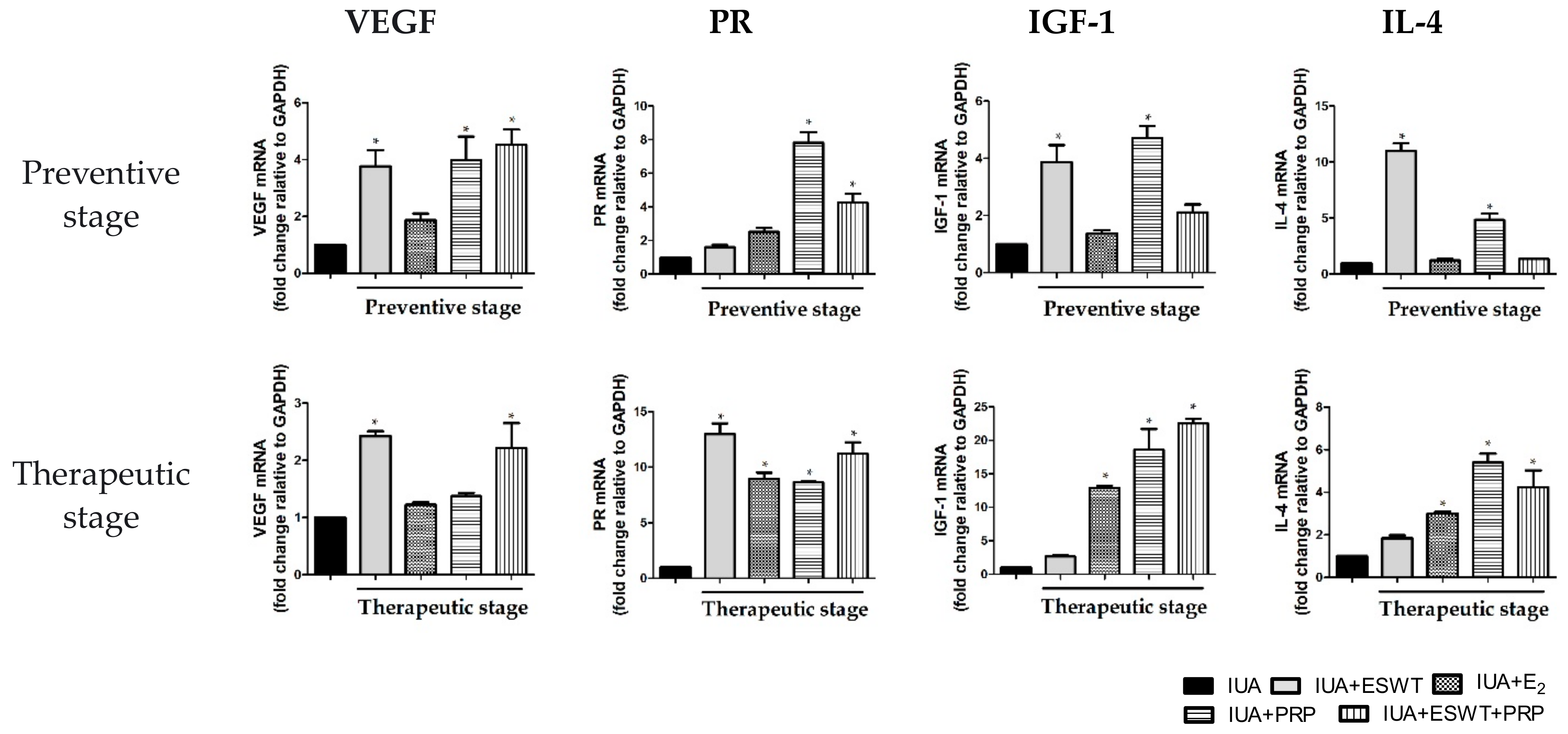
3.4. ESWT Treatment, E2 Transplantation, or ESWT Combined with PRP Regulated Vascular, Fibrosis, Inflammation, and Antiinflammation-Associated Genes in IUA Rats
3.5. ESWT Treatment, PRP Transplantation, or ESWT Combined with PRP Mainly Promoted VEGF and Vimentin Expression at the Therapeutic Stage in IUA Rats
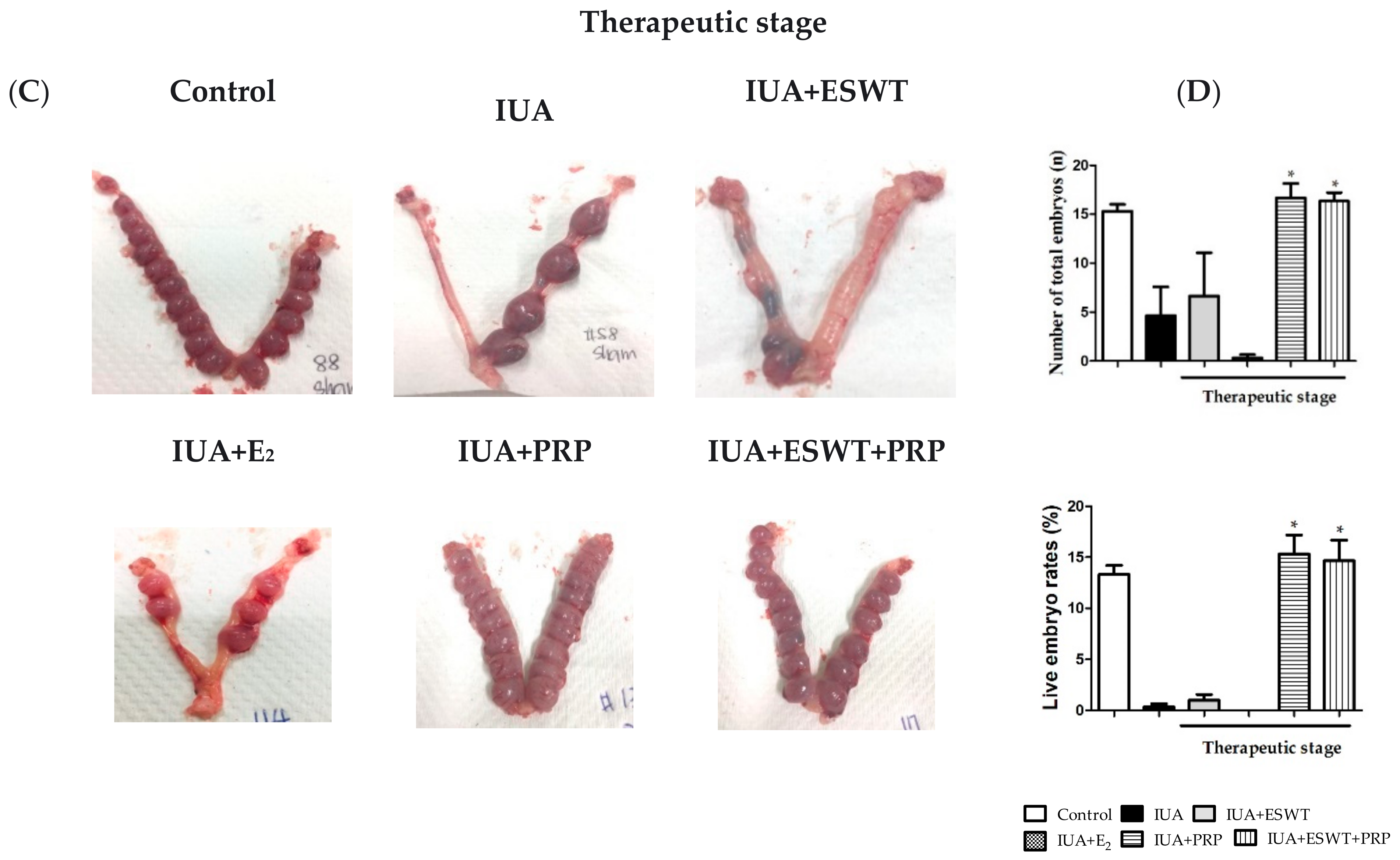
3.6. Pregnancy Outcomes in Rats with IUA-Damaged Endometrium after ESWT Treatment, E2 and PRP Transplantation, or ESWT Combined with PRP Transplantation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warembourg, S.; Huberlant, S.; Garric, X.; Leprince, S.; de Tayrac, R.; Letouzey, V. Prevention and treatment of intra-uterine synechiae: Review of the literature. J. Gynecol. Obstet. Biol. Reprod. 2015, 44, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Hooker, A.B.; de Leeuw, R.; van de Ven, P.M.; Bakkum, E.A.; Thurkow, A.L.; Vogel, N.E.A.; van Vliet, H.; Bongers, M.Y.; Emanuel, M.H.; Verdonkschot, A.E.M.; et al. Prevalence of intrauterine adhesions after the application of hyaluronic acid gel after dilatation and curettage in women with at least one previous curettage: Short-term outcomes of a multicenter, prospective randomized controlled trial. Fertil. Steril. 2017, 107, 1223–1231. [Google Scholar] [CrossRef]
- Hooker, A.B.; Lemmers, M.; Thurkow, A.L.; Heymans, M.W.; Opmeer, B.C.; Brolmann, H.A.; Mol, B.W.; Huirne, J.A. Systematic review and meta-analysis of intrauterine adhesions after miscarriage: Prevalence, risk factors and long-term reproductive outcome. Hum. Reprod. Update 2014, 20, 262–278. [Google Scholar] [CrossRef] [PubMed]
- Dmowski, W.P.; Greenblatt, R.B. Asherman’s syndrome and risk of placenta accreta. Obstet. Gynecol. 1969, 34, 288–299. [Google Scholar] [PubMed]
- March, C.M. Management of Asherman’s syndrome. Reprod. Biomed. Online 2011, 23, 63–76. [Google Scholar] [CrossRef]
- Capmas, P.; Mihalache, A.; Duminil, L.; Hor, L.S.; Pourcelot, A.G.; Fernandez, H. Intrauterine adhesions: What is the pregnancy rate after hysteroscopic management? J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101797. [Google Scholar] [CrossRef]
- Turocy, J.M.; Rackow, B.W. Uterine factor in recurrent pregnancy loss. Semin. Perinatol. 2019, 43, 74–79. [Google Scholar] [CrossRef]
- Gan, L.; Duan, H.; Xu, Q.; Tang, Y.Q.; Li, J.J.; Sun, F.Q.; Wang, S. Human amniotic mesenchymal stromal cell transplantation improves endometrial regeneration in rodent models of intrauterine adhesions. Cytotherapy 2017, 19, 603–616. [Google Scholar] [CrossRef]
- Zupi, E.; Centini, G.; Lazzeri, L. Asherman syndrome: An unsolved clinical definition and management. Fertil. Steril. 2015, 104, 1380–1381. [Google Scholar] [CrossRef]
- Seyedoshohadaei, F.; Tangestani, L.; Zandvakili, F.; Rashadmanesh, N. Comparison of the Effect of Clomiphene—Estradiol Valerate vs. Letrozole on Endometrial Thickness, Abortion and Pregnancy Rate in Infertile Women with Polycystic Ovarian Syndrome. J. Clin. Diagn. Res. 2016, 10, QC10–QC13. [Google Scholar] [CrossRef]
- Etulain, J.; Mena, H.A.; Meiss, R.P.; Frechtel, G.; Gutt, S.; Negrotto, S.; Schattner, M. An optimised protocol for platelet-rich plasma preparation to improve its angiogenic and regenerative properties. Sci. Rep. 2018, 8, 1513. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.S.; Xia, W.T.; Xu, J.; Xu, H.L.; Lu, C.T.; Zhao, Y.Z.; Wu, X.Q. Three-dimensional structure micelles of heparin-poloxamer improve the therapeutic effect of 17beta-estradiol on endometrial regeneration for intrauterine adhesions in a rat model. Int. J. Nanomed. 2017, 12, 5643–5657. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.S.; Xu, X.X.; Xiang, W.W.; Zhang, H.H.; Lin, H.L.; Shen, L.E.; Lin, Q.; Lin, F.; Zhou, Z.Y. Using 17beta-estradiol heparin-poloxamer thermosensitive hydrogel to enhance the endometrial regeneration and functional recovery of intrauterine adhesions in a rat model. FASEB J. 2020, 34, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, R.S.; Schwarz, E.M.; Maloney, M.D. Platelet-rich plasma therapy—Future or trend? Arthritis Res. Ther. 2012, 14, 219. [Google Scholar] [CrossRef]
- Barile, A.; La Marra, A.; Arrigoni, F.; Mariani, S.; Zugaro, L.; Splendiani, A.; Di Cesare, E.; Reginelli, A.; Zappia, M.; Brunese, L.; et al. Anaesthetics, steroids and platelet-rich plasma (PRP) in ultrasound-guided musculoskeletal procedures. Br. J. Radiol. 2016, 89, 20150355. [Google Scholar] [CrossRef]
- Bashir, J.; Panero, A.J.; Sherman, A.L. The emerging use of platelet-rich plasma in musculoskeletal medicine. J. Osteopath. Med. 2015, 115, 24–31. [Google Scholar] [CrossRef][Green Version]
- Rinaldi, F.; Marzani, B.; Pinto, D.; Sorbellini, E. Randomized controlled trial on a PRP-like cosmetic, biomimetic peptides based, for the treatment of alopecia areata. J. Dermatol. Treat. 2019, 30, 588–593. [Google Scholar] [CrossRef]
- Lin, M.-Y.; Lin, C.-S.; Hu, S.; Chung, W.-H. Progress in the use of platelet-rich plasma in aesthetic and medical dermatology. J. Clin. Aesthetic Dermatol. 2020, 13, 28. [Google Scholar]
- Puri, N. Platelet rich plasma in dermatology and aesthetic medicine. Our Dermatol. Online 2015, 6, 207. [Google Scholar] [CrossRef]
- Carroll, R.C.; Worthington, R.E.; Craft, R.M.; Snider, C.C.; Dakin, P.A.; Wortham, D.C.; Scott, J.; Jarrett, A. Post interventional cardiology urinary thromboxane correlates with PlateletMapping detected aspirin resistance. Thromb. Res. 2010, 125, e118–e122. [Google Scholar] [CrossRef]
- Spartalis, E.; Tomos, P.; Moris, D.; Athanasiou, A.; Markakis, C.; Spartalis, M.D.; Troupis, T.; Dimitroulis, D.; Perrea, D. Role of platelet-rich plasma in ischemic heart disease: An update on the latest evidence. World J. Cardiol. 2015, 7, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Biswas, D.; So, K.H.; Hwang, S.U.; Yoon, J.D.; Kim, M.; Kim, D.Y.; Hyun, S.H. Embryotropic effects of vascular endothelial growth factor on porcine embryos produced by in vitro fertilization. Theriogenology 2018, 120, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kwon, O.H.; Kim, T.K.; Cho, Y.K.; Choi, K.Y.; Chung, H.Y.; Cho, B.C.; Yang, J.D.; Shin, J.H. Platelet-rich plasma: Quantitative assessment of growth factor levels and comparative analysis of activated and inactivated groups. Arch. Plast. Surg. 2013, 40, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Zadehmodarres, S.; Salehpour, S.; Saharkhiz, N.; Nazari, L. Treatment of thin endometrium with autologous platelet-rich plasma: A pilot study. JBRA Assist. Reprod. 2017, 21, 54–56. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, M.R.; Sommese, L.; Casamassimi, A.; Napoli, C. Platelet derivatives in regenerative medicine: An update. Transfus. Med. Rev. 2015, 29, 52–61. [Google Scholar] [CrossRef]
- Qian, Y.; Han, Q.; Chen, W.; Song, J.; Zhao, X.; Ouyang, Y.; Yuan, W.; Fan, C. Platelet-Rich Plasma Derived Growth Factors Contribute to Stem Cell Differentiation in Musculoskeletal Regeneration. Front. Chem. 2017, 5, 89. [Google Scholar] [CrossRef]
- Jo, C.H.; Kim, J.E.; Yoon, K.S.; Shin, S. Platelet-rich plasma stimulates cell proliferation and enhances matrix gene expression and synthesis in tenocytes from human rotator cuff tendons with degenerative tears. Am. J. Sports Med. 2012, 40, 1035–1045. [Google Scholar] [CrossRef]
- Xu, Q.; Li, B.; Yuan, L.; Dong, Z.; Zhang, H.; Wang, H.; Sun, J.; Ge, S.; Jin, Y. Combination of platelet-rich plasma within periodontal ligament stem cell sheets enhances cell differentiation and matrix production. J. Tissue Eng. Regen. Med. 2017, 11, 627–636. [Google Scholar] [CrossRef]
- Goncalves, N.J.N.; Frantz, N.; de Oliveira, R.M. Platelet-rich plasma (PRP) therapy: An approach in reproductive medicine based on successful animal models. Anim. Reprod. 2020, 16, 93–98. [Google Scholar] [CrossRef]
- Zhang, S.; Li, P.; Yuan, Z.; Tan, J. Platelet-rich plasma improves therapeutic effects of menstrual blood-derived stromal cells in rat model of intrauterine adhesion. Stem Cell Res. Ther. 2019, 10, 61. [Google Scholar] [CrossRef]
- Chaussy, C.; Schmiedt, E.; Jocham, D.; Brendel, W.; Forssmann, B.; Walther, V. First clinical experience with extracorporeally induced destruction of kidney stones by shock waves. J. Urol. 1982, 127, 417–420. [Google Scholar] [CrossRef]
- Buch, M.; Knorr, U.; Fleming, L.; Theodore, G.; Amendola, A.; Bachmann, C.; Zingas, C.; Siebert, W.E. Extracorporeal shockwave therapy in symptomatic heel spurs. An overview. Orthopade 2002, 31, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Wilner, J.M.; Strash, W.W. Extracorporeal shockwave therapy for plantar fasciitis and other musculoskeletal conditions utilizing the Ossatron—An update. Clin. Podiatr. Med. Surg. 2004, 21, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.E.; Crawford, F.; Murray, G.D. The effectiveness of extra corporeal shock wave therapy for plantar heel pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2005, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Roehrig, G.J.; Baumhauer, J.; DiGiovanni, B.F.; Flemister, A.S. The role of extracorporeal shock wave on plantar fasciitis. Foot Ankle Clin. 2005, 10, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; Green, S.E.; Youd, J.M.; Assendelft, W.J.; Barnsley, L.; Smidt, N. Systematic review of the efficacy and safety of shock wave therapy for lateral elbow pain. J. Rheumatol. 2006, 33, 1351–1363. [Google Scholar]
- Stasinopoulos, D.; Johnson, M.I. Effectiveness of extracorporeal shock wave therapy for tennis elbow (lateral epicondylitis). Br. J. Sports Med. 2005, 39, 132–136. [Google Scholar] [CrossRef]
- Rompe, J.D.; Theis, C.; Maffulli, N. Shock wave treatment for tennis elbow. Orthopade 2005, 34, 567–570. [Google Scholar] [CrossRef]
- Erturk, E.; Ptak, A.M.; Monaghan, J. Fertility measures in women after extracorporeal shockwave lithotripsy of distal ureteral stones. J. Endourol. 1997, 11, 315–317. [Google Scholar] [CrossRef]
- Vieweg, J.; Weber, H.M.; Miller, K.; Hautmann, R. Female fertility following extracorporeal shock wave lithotripsy of distal ureteral calculi. J. Urol. 1992, 148, 1007–1010. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, T.; Cai, H.Y.; Ma, T.K.; Tao, S.M.; Sun, S.; Chen, M.Q.; Gu, Y.; Pang, J.H.; Xiao, J.M.; et al. Cardiac shock wave therapy reduces angina and improves myocardial function in patients with refractory coronary artery disease. Clin. Cardiol. 2010, 33, 693–699. [Google Scholar] [CrossRef]
- Ito, Y.; Ito, K.; Shiroto, T.; Tsuburaya, R.; Yi, G.J.; Takeda, M.; Fukumoto, Y.; Yasuda, S.; Shimokawa, H. Cardiac shock wave therapy ameliorates left ventricular remodeling after myocardial ischemia-reperfusion injury in pigs in vivo. Coron. Artery Dis. 2010, 21, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Sung, P.-H.; Lee, M.S.; Chai, H.-T.; Chiang, J.Y.; Li, Y.-C.; Chu, Y.-C.; Huang, C.-R.; Yip, H.-K. Extracorporeal Shock Wave Enhanced Exogenous Mitochondria into Adipose-Derived Mesenchymal Stem Cells and Further Preserved Heart Function in Rat Dilated Cardiomyopathy. Biomedicines 2021, 9, 1362. [Google Scholar] [CrossRef] [PubMed]
- Rassweiler, J.J.; Knoll, T.; Kohrmann, K.U.; McAteer, J.A.; Lingeman, J.E.; Cleveland, R.O.; Bailey, M.R.; Chaussy, C. Shock wave technology and application: An update. Eur. Urol. 2011, 59, 784–796. [Google Scholar] [CrossRef] [PubMed]
- Khrouf, M.; Morel, O.; Hafiz, A.; Chavatte-Palmer, P. Evaluation of the rabbit as an experimental model for human uterine synechia. J. Hum. Reprod. Sci. 2012, 5, 175. [Google Scholar]
- Zhang, X.; Yan, X.; Wang, C.; Tang, T.; Chai, Y. The dose-effect relationship in extracorporeal shock wave therapy: The optimal parameter for extracorporeal shock wave therapy. J. Surg. Res. 2014, 186, 484–492. [Google Scholar] [CrossRef]
- Reinehr, S.; Reinhard, J.; Gandej, M.; Gottschalk, I.; Stute, G.; Faissner, A.; Dick, H.B.; Joachim, S.C. S100B immunization triggers NFkappaB and complement activation in an autoimmune glaucoma model. Sci. Rep. 2018, 8, 9821. [Google Scholar] [CrossRef]
- Sanchez, R.N.; Chan, C.K.; Garg, S.; Kwong, J.M.; Wong, M.J.; Sadun, A.A.; Lam, T.T. Interleukin-6 in retinal ischemia reperfusion injury in rats. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4006–4011. [Google Scholar] [CrossRef]
- Li, M.; O’Sullivan, K.M.; Jones, L.K.; Lo, C.; Semple, T.; Kumanogoh, A.; Kikutani, H.; Holdsworth, S.R.; Kitching, R. Endogenous CD100 promotes glomerular injury and macrophage recruitment in experimental crescentic glomerulonephritis. Immunology 2009, 128, 114–122. [Google Scholar] [CrossRef]
- Spittau, B.; Rilka, J.; Steinfath, E.; Zoller, T.; Krieglstein, K. TGFbeta1 increases microglia-mediated engulfment of apoptotic cells via upregulation of the milk fat globule-EGF factor 8. Glia 2014, 63, 142–153. [Google Scholar] [CrossRef]
- Du, M.; Chen, B.; Meng, Q.; Liu, S.; Zheng, X.; Zhang, C.; Wang, H.; Li, H.; Wang, N.; Dai, J. 3D bioprinting of BMSC-laden methacrylamide gelatin scaffolds with CBD-BMP2-collagen microfibers. Biofabrication 2015, 7, 044104. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Chen, J.M.; Xiao, T.G.; Shu, X.B.; Xu, H.C.; Yang, L.L.; Xing, L.J.; Zheng, P.Y.; Ji, G. Qinggan Huoxue Recipe suppresses epithelial-to-mesenchymal transition in alcoholic liver fibrosis through TGF-beta1/Smad signaling pathway. World J. Gastroenterol. 2016, 22, 4695–4706. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; He, X.; Tao, X.; Hou, T.; Chen, M.; He, M.; Liao, H. The CD200/CD200R signaling pathway contributes to spontaneous functional recovery by enhancing synaptic plasticity after stroke. J. Neuroinflamm. 2020, 17, 171. [Google Scholar] [CrossRef] [PubMed]
- Imberti, B.; Corna, D.; Rizzo, P.; Xinaris, C.; Abbate, M.; Longaretti, L.; Cassis, P.; Benedetti, V.; Benigni, A.; Zoja, C.; et al. Renal primordia activate kidney regenerative events in a rat model of progressive renal disease. PLoS ONE 2015, 10, e0120235. [Google Scholar] [CrossRef]
- Lee, S.W.; Lee, J.E.; Yoo, C.Y.; Ko, M.S.; Park, C.S.; Yang, S.-H. NRP-1 expression is strongly associated with the progression of pituitary adenomas. Oncol. Rep. 2014, 32, 1537–1542. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, M.; Mizutani, T.; Yamada, K.; Yazawa, T.; Ogata-Kawata, H.; Sekiguchi, T.; Kajitani, T.; Miyamoto, K. Co-activator p120 is increased by gonadotropins in the rat ovary and enhances progesterone receptor activity. Reprod. Biol. Endocrinol. 2006, 4, 50. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhang, X.; Wang, X.; Liu, T.; Mo, M.; Ao, L.; Liu, J.; Cao, J.; Cui, Z. Smad2/3 Upregulates the Expression of Vimentin and Affects Its Distribution in DBP-Exposed Sertoli Cells. PPAR Res. 2015, 2015, 489314. [Google Scholar] [CrossRef]
- Xu, L.; Tong, R.; Li, X.; Liang, L.; Huang, H. Effects of CASZI on bronchopulmonary development of neonatal rats. Exp. Ther. Med. 2017, 14, 6243–6246. [Google Scholar] [CrossRef]
- Melki, E. Endometriosis treatment with shock waves: A novel approach. Med. Hypotheses 2019, 124, 114–117. [Google Scholar] [CrossRef]
- Martinez Portillo, F.J.; Heidenreich, A.; Schwarzer, U.; Michel, M.S.; Alken, P.; Engelmann, U. Microscopic and biochemical fertility characteristics of semen after shockwave lithotripsy of distal ureteral calculi. J. Endourol. 2001, 15, 781–784, discussion 784–785. [Google Scholar] [CrossRef]
- Zang, Z.J.; Liu, Q.; Hu, J.; Feng, J.; Zhu, Y.Q.; Ma, G.; Jiang, M.H. The impact of low-intensity extracorporeal shock wave therapy on testicular function in adult rats. Andrology 2018, 6, 936–942. [Google Scholar] [CrossRef]
- Wang, H.J.; Tyagi, P.; Lin, T.K.; Huang, C.C.; Lee, W.C.; Chancellor, M.B.; Chuang, Y.C. Low Energy Shock Wave Therapy Attenuates Mitochondrial Dysfunction and Improves Bladder Function in HCl induced Cystitis in Rats. Biomed. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, M.; Zhang, Q.; Zhao, W.; Yang, B.; Shang, H.; Shang, X.; Ma, Y.; Wang, B.; Feng, L. Estrogen therapy before hysteroscopic adhesiolysis improves the fertility outcome in patients with intrauterine adhesions. Arch. Gynecol. Obstet. 2019, 300, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Li, S.; Deng, J.; Yang, S.; Xiang, Z.; Guo, H.; Xi, H.; Sang, M.; Zhang, W. Aspirin inhibits endometrial fibrosis by suppressing the TGFbeta1Smad2/Smad3 pathway in intrauterine adhesions. Int. J. Mol. Med. 2020, 45, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Liu, J.; Yuan, W.; Liu, Y.; Li, W.; Cao, S.; Yu, L.; Wang, L. Therapeutic Effect of Human Amniotic Epithelial Cells in Rat Models of Intrauterine Adhesions. Cell Transplant. 2020, 29, 963689720908495. [Google Scholar] [CrossRef]
- Rochwerger, L.; Dho, S.; Parker, L.; Foskett, J.K.; Buchwald, M. Estrogen-dependent expression of the cystic fibrosis transmembrane regulator gene in a novel uterine epithelial cell line. J. Cell Sci. 1994, 107, 2439–2448. [Google Scholar] [CrossRef]
- Tonguc, E.A.; Var, T.; Yilmaz, N.; Batioglu, S. Intrauterine device or estrogen treatment after hysteroscopic uterine septum resection. Int. J. Gynaecol. Obstet. 2010, 109, 226–229. [Google Scholar] [CrossRef]
- Cai, H.; Li, H.; He, Y. Interceed and Estrogen Reduce Uterine Adhesions and Fibrosis and Improve Endometrial Receptivity in a Rabbit Model of Intrauterine Adhesions. Reprod. Sci. 2016, 23, 1208–1216. [Google Scholar] [CrossRef]
- Chen, Y.; Chang, Y.; Yao, S. Role of angiogenesis in endometrial repair of patients with severe intrauterine adhesion. Int. J. Clin. Exp. Pathol. 2013, 6, 1343–1350. [Google Scholar]
- Magos, A. Hysteroscopic treatment of Asherman’s syndrome. Reprod. Biomed. Online 2002, 4 (Suppl. 3), 46–51. [Google Scholar] [CrossRef]
- Johary, J.; Xue, M.; Zhu, X.; Xu, D.; Velu, P.P. Efficacy of estrogen therapy in patients with intrauterine adhesions: Systematic review. J. Minim. Invasive Gynecol. 2014, 21, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Di Spiezio Sardo, A.; Calagna, G.; Scognamiglio, M.; O’Donovan, P.; Campo, R.; De Wilde, R.L. Prevention of intrauterine post-surgical adhesions in hysteroscopy. A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Deans, R.; Vancaillie, T.; Ledger, W.; Liu, J.; Abbott, J.A. Live birth rate and obstetric complications following the hysteroscopic management of intrauterine adhesions including Asherman syndrome. Hum. Reprod. 2018, 33, 1847–1853. [Google Scholar] [CrossRef] [PubMed]
- Salma, U.; Xue, M.; Sayed, A.S.M.; Xu, D. Efficacy of intrauterine device in the treatment of intrauterine adhesions. Biomed. Res. Int. 2014, 2014, 589296. [Google Scholar] [CrossRef]
- Tafti, S.Z.G.; Javaheri, A.; Firoozabadi, R.D.; Ashkezar, S.K.; Abarghouei, H.F. Role of hyaluronic acid intrauterine injection in the prevention of Asherman’s syndrome in women undergoing uterine septum resection: An RCT. Int. J. Reprod. Biomed. 2021, 19, 339–346. [Google Scholar] [CrossRef]
- Azizi, R.; Aghebati-Maleki, L.; Nouri, M.; Marofi, F.; Negargar, S.; Yousefi, M. Stem cell therapy in Asherman syndrome and thin endometrium: Stem cell-based therapy. Biomed. Pharmacother. 2018, 102, 333–343. [Google Scholar] [CrossRef]
- Bai, X.; Liu, J.; Cao, S.; Wang, L. Mechanisms of endometrial fibrosis and the potential application of stem cell therapy. Discov. Med. 2019, 27, 267–279. [Google Scholar]
- Ebrahim, N.; Mostafa, O.; El Dosoky, R.E.; Ahmed, I.A.; Saad, A.S.; Mostafa, A.; Sabry, D.; Ibrahim, K.A.; Farid, A.S. Human mesenchymal stem cell-derived extracellular vesicles/estrogen combined therapy safely ameliorates experimentally induced intrauterine adhesions in a female rat model. Stem Cell Res. Ther. 2018, 9, 175. [Google Scholar] [CrossRef]
- Kilic, S.; Yuksel, B.; Pinarli, F.; Albayrak, A.; Boztok, B.; Delibasi, T. Effect of stem cell application on Asherman syndrome, an experimental rat model. J. Assist. Reprod. Genet. 2014, 31, 975–982. [Google Scholar] [CrossRef]
- Liu, Y.; Cai, J.; Luo, X.; Wen, H.; Luo, Y. Collagen Scaffold with Human Umbilical Cord Mesenchymal Stem Cells Remarkably Improves Intrauterine Adhesions in a Rat Model. Gynecol. Obstet. Investig. 2020, 85, 267–276. [Google Scholar] [CrossRef]
- Santamaria, X.; Cabanillas, S.; Cervello, I.; Arbona, C.; Raga, F.; Ferro, J.; Palmero, J.; Remohi, J.; Pellicer, A.; Simon, C. Autologous cell therapy with CD133+ bone marrow-derived stem cells for refractory Asherman’s syndrome and endometrial atrophy: A pilot cohort study. Hum. Reprod. 2016, 31, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhang, H.; Wang, Q.; Xie, F.; Gao, S.; Song, Y.; Dong, J.; Feng, H.; Xie, K.; Sui, L. Reproductive Outcomes in Patients with Intrauterine Adhesions Following Hysteroscopic Adhesiolysis: Experience from the Largest Women’s Hospital in China. J. Minim. Invasive Gynecol. 2017, 24, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Hamerlynck, T.W.; Meyers, D.; Van der Veken, H.; Bosteels, J.; Weyers, S. Fertility outcome after treatment of retained products of conception: A systematic review. Gynecol. Surg. 2018, 15, 12. [Google Scholar] [CrossRef]
- Li, H.-J.; He, Y.-L.; Hu, H.-Y.; Li, J.-X.; Xian, W.; Chen, S.-P.; Zhang, D.-M. Effects of Interceed on endometrial receptivity in rabbits with intrauterine adhesion. Med. J. Chin. People. Lib. Army 2015, 40, 344–348. [Google Scholar]
- Xue, X.; Chen, Q.; Zhao, G.; Zhao, J.Y.; Duan, Z.; Zheng, P.S. The Overexpression of TGF-beta and CCN2 in Intrauterine Adhesions Involves the NF-kappaB Signaling Pathway. PLoS ONE 2015, 10, e0146159. [Google Scholar] [CrossRef]
- Mouhayar, Y.; Sharara, F.I. G-CSF and stem cell therapy for the treatment of refractory thin lining in assisted reproductive technology. J. Assist. Reprod. Genet. 2017, 34, 831–837. [Google Scholar] [CrossRef]
- Hu, S.; Ogle, B.M.; Cheng, K. Body builder: From synthetic cells to engineered tissues. Curr. Opin. Cell Biol. 2018, 54, 37–42. [Google Scholar] [CrossRef]
- Niu, H.; Miao, X.; Zhan, X.; Zhou, X.; Li, X.; Jiang, L. Tiaoshen Tongluo Attenuates Fibrosis by Modulating the TGF-beta1/Smad Pathway in Endometrial Stromal Cells and a Rat Model of Intrauterine Adhesion. Evid. Based Complement. Altern. Med. 2021, 2021, 6675329. [Google Scholar] [CrossRef]
- Chen, X.; Sun, J.; Li, X.; Mao, L.; Zhou, Y.; Cui, L.; Bai, W. Antifibrotic Effects of Decellularized and Lyophilized Human Amniotic Membrane Transplant on the Formation of Intrauterine Adhesion. Exp. Clin. Transplant. 2019, 17, 236–242. [Google Scholar] [CrossRef]
- Ning, J.; Zhang, H.; Yang, H. MicroRNA326 inhibits endometrial fibrosis by regulating TGFbeta1/Smad3 pathway in intrauterine adhesions. Mol. Med. Rep. 2018, 18, 2286–2292. [Google Scholar] [CrossRef]
- Liu, X.; Xu, Q.; Chen, C.; Duan, H. miR-543 Inhibits the Occurrence and Development of Intrauterine Adhesion by Inhibiting the Proliferation, Migration, and Invasion of Endometrial Cells. BioMed Res. Int. 2021, 2021, 5559102. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.C. NF-kappaB signaling in inflammation. Signal Transduct. Target. Ther. 2017, 2, 17023. [Google Scholar] [CrossRef]
- Salama, N.M.; Zaghlol, S.S.; Mohamed, H.H.; Kamar, S.S. Suppression of the inflammation and fibrosis in Asherman syndrome rat model by mesenchymal stem cells: Histological and immunohistochemical studies. Folia Histochem. Cytobiol. 2020, 58, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ma, N.; Sun, Q.; Huang, C.; Liu, Y.; Luo, X. Elevated NF-kappaB signaling in Asherman syndrome patients and animal models. Oncotarget 2017, 8, 15399–15406. [Google Scholar] [CrossRef]
- Peng, Y.Z.; Zheng, K.; Yang, P.; Wang, Y.; Li, R.J.; Li, L.; Pan, J.H.; Guo, T. Shock wave treatment enhances endothelial proliferation via autocrine vascular endothelial growth factor. Genet. Mol. Res. 2015, 14, 19203–19210. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Zhang, Q.; Sun, J.; Lai, D. Human amniotic epithelial cells improve fertility in an intrauterine adhesion mouse model. Stem Cell Res. Ther. 2019, 10, 257. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Li, J.; Chen, Y.; Wei, L.; Yang, X.; Shi, Y.; Liang, X. Autologous platelet-rich plasma promotes endometrial growth and improves pregnancy outcome during in vitro fertilization. Int. J. Clin. Exp. Med. 2015, 8, 1286–1290. [Google Scholar] [PubMed]
- Ito, K.; Fukumoto, Y.; Shimokawa, H. Extracorporeal shock wave therapy for ischemic cardiovascular disorders. Am. J. Cardiovasc. Drugs 2011, 11, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Yeh, K.H.; Sheu, J.J.; Lin, Y.C.; Sun, C.K.; Chang, L.T.; Kao, Y.H.; Yen, C.H.; Shao, P.L.; Tsai, T.H.; Chen, Y.L.; et al. Benefit of combined extracorporeal shock wave and bone marrow-derived endothelial progenitor cells in protection against critical limb ischemia in rats. Crit. Care Med. 2012, 40, 169–177. [Google Scholar] [CrossRef]
- Sheu, J.J.; Lee, F.Y.; Yuen, C.M.; Chen, Y.L.; Huang, T.H.; Chua, S.; Chen, Y.L.; Chen, C.H.; Chai, H.T.; Sung, P.H.; et al. Combined therapy with shock wave and autologous bone marrow-derived mesenchymal stem cells alleviates left ventricular dysfunction and remodeling through inhibiting inflammatory stimuli, oxidative stress & enhancing angiogenesis in a swine myocardial infarction model. Int. J. Cardiol. 2015, 193, 69–83. [Google Scholar] [CrossRef]
- Huang, T.-H.; Sun, C.-K.; Chen, Y.-L.; Wang, C.-J.; Yin, T.-C.; Lee, M.S.; Yip, H.-K. Shock wave therapy enhances angiogenesis through VEGFR2 activation and recycling. Mol. Med. 2016, 22, 850–862. [Google Scholar] [CrossRef]
- Andersson, A.; Bernardi, A.I.; Nurkkala-Karlsson, M.; Stubelius, A.; Grahnemo, L.; Ohlsson, C.; Carlsten, H.; Islander, U. Suppression of Experimental Arthritis and Associated Bone Loss by a Tissue-Selective Estrogen Complex. Endocrinology 2016, 157, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Su, R.W.; Strug, M.R.; Jeong, J.W.; Miele, L.; Fazleabas, A.T. Aberrant activation of canonical Notch1 signaling in the mouse uterus decreases progesterone receptor by hypermethylation and leads to infertility. Proc. Natl. Acad. Sci. USA 2016, 113, 2300–2305. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ju, B.; Pan, C.; Gu, Y.; Zhang, Y.; Sun, L.; Zhang, B.; Zhang, Y. Application of Bone Marrow-Derived Mesenchymal Stem Cells in the Treatment of Intrauterine Adhesions in Rats. Cell. Physiol. Biochem. 2016, 39, 1553–1560. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Forward Primer (5′–3′) | Reverse Primer (5′–3′) |
|---|---|---|
| NF-κB [47] | CTGGCAGCTCTTCTCAAAGC | CCAGGTCATAGAGAGGCTCAA |
| IL-6 [48] | TCAACTCCATCTGCCCTTCAG | AAGGCAACTGGCTGGAAGTCT |
| TNF-α [49] | GCCTCTTCTCATTCCTGCTT | CACTTGGTGGTTTGCTACGA |
| TGF-β [50] | TAATGGTGGACCGCAACAACG | GGCACTGCTTCCCGAATGTCT |
| COL1α1 [51] | CATGTTCAGCTTTGTGGACCT | GCAGCTGACTTCAGGGATGT |
| Fibronectin [52] | GACTCGCTTTGACTTCACCAC | GCTGAGACCCAGGAGACCAC |
| IL-4 [53] | CAGGGTGCTTCGCAAATTTTAC | ACCGAGAACCCCAGACTTGTT |
| IGF-1 [54] | GCTTTTACTTCAACAAGCCCACA | TCAGCGGAGCACAGTACATC |
| VEGF [55] | TATCTTCAAGCCGTCCTGTG | GATCCGCATGATCTGCATAG |
| PR [56] | TCAAGGCAATTGGCTTAAGACA | GAGCTGTTTCACAAGATCATGCA |
| Vimentin [57] | GCACCCTGCAGTCATTCAGA | GCAAGGATTCCACTTTACGTTCA |
| GAPDH [58] | TGGTGAAGGTCGGTGTGAAC | GACTGTGCCGTTGAACTTGC |
| Control | IUA | IUA+ESWT | IUA+E2 | IUA+PRP | IUA+ESWT+PRP | |
|---|---|---|---|---|---|---|
| Bodyweight (g) of preventive stage | ||||||
| Day 0 | 212.1 ± 7.8 | 210.3 ± 14.1 | 205.4 ± 10.3 | 215.8 ± 8.9 | 201.8 ± 7.0 | 201.5 ± 6.0 |
| Day 21 | 253.5 ± 15.7 | 244.2 ± 19.0 | 243.9 ± 23.0 | 247.8 ± 12.9 | 243.0 ± 14.9 | 235.4 ± 13.9 |
| Bodyweight (g) of therapeutic stage | ||||||
| Day 0 | 206.1 ± 8.3 | 212.3 ± 12.2 | 209.3 ± 6.9 | 211.6 ± 10.6 | 221.8 ± 15.1 | 224.9 ± 13.9 |
| Day 35 | 262.7 ± 28.3 | 266.3 ± 20.4 | 261.6 ± 10.9 | 265.5 ± 22.6 | 279.4 ± 16.3 | 274.9 ± 20.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Y.-H.; Tsai, N.-C.; Chen, Y.-J.; Weng, P.-L.; Chang, Y.-C.; Cheng, J.-H.; Ko, J.-Y.; Kang, H.-Y.; Lan, K.-C. Extracorporeal Shock Wave Therapy Combined with Platelet-Rich Plasma during Preventive and Therapeutic Stages of Intrauterine Adhesion in a Rat Model. Biomedicines 2022, 10, 476. https://doi.org/10.3390/biomedicines10020476
Cheng Y-H, Tsai N-C, Chen Y-J, Weng P-L, Chang Y-C, Cheng J-H, Ko J-Y, Kang H-Y, Lan K-C. Extracorporeal Shock Wave Therapy Combined with Platelet-Rich Plasma during Preventive and Therapeutic Stages of Intrauterine Adhesion in a Rat Model. Biomedicines. 2022; 10(2):476. https://doi.org/10.3390/biomedicines10020476
Chicago/Turabian StyleCheng, Yin-Hua, Ni-Chin Tsai, Yun-Ju Chen, Pei-Ling Weng, Yun-Chiao Chang, Jai-Hong Cheng, Jih-Yang Ko, Hong-Yo Kang, and Kuo-Chung Lan. 2022. "Extracorporeal Shock Wave Therapy Combined with Platelet-Rich Plasma during Preventive and Therapeutic Stages of Intrauterine Adhesion in a Rat Model" Biomedicines 10, no. 2: 476. https://doi.org/10.3390/biomedicines10020476
APA StyleCheng, Y.-H., Tsai, N.-C., Chen, Y.-J., Weng, P.-L., Chang, Y.-C., Cheng, J.-H., Ko, J.-Y., Kang, H.-Y., & Lan, K.-C. (2022). Extracorporeal Shock Wave Therapy Combined with Platelet-Rich Plasma during Preventive and Therapeutic Stages of Intrauterine Adhesion in a Rat Model. Biomedicines, 10(2), 476. https://doi.org/10.3390/biomedicines10020476