
An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Tissue-Engineered Model Generation
2.3. Drug Treatment
2.4. Freezing Protocol
2.4.1. Cell Culture Freeze Procedure
2.4.2. TEM Freeze Procedure
2.5. Cell Viability and Data Analysis
2.5.1. Two-Dimensional Viability Assessment and Analysis
2.5.2. TEM Viability Assessment and Analysis
2.6. Immunofluorescent Analysis of Cleaved Caspase-3 Activity
3. Results
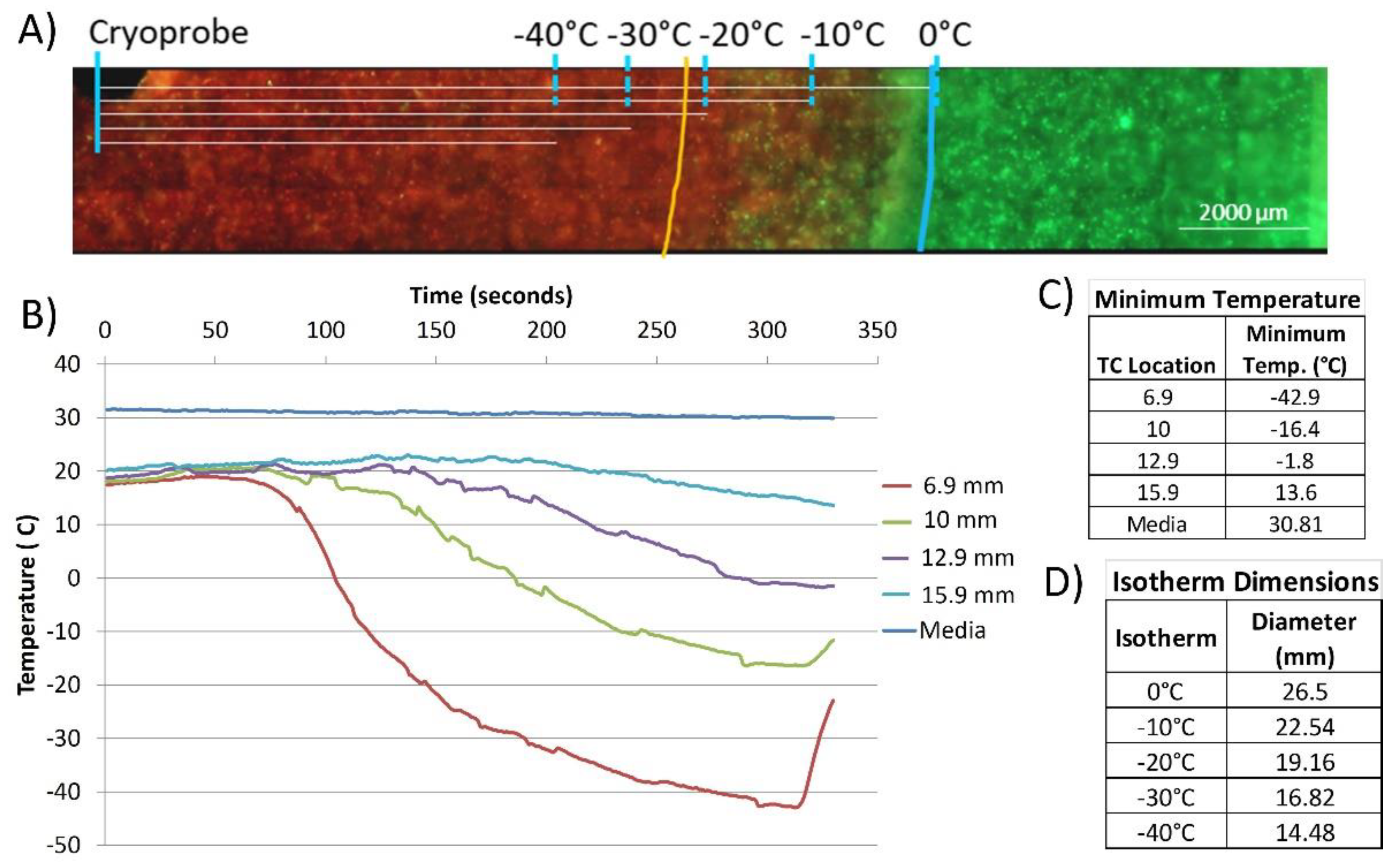
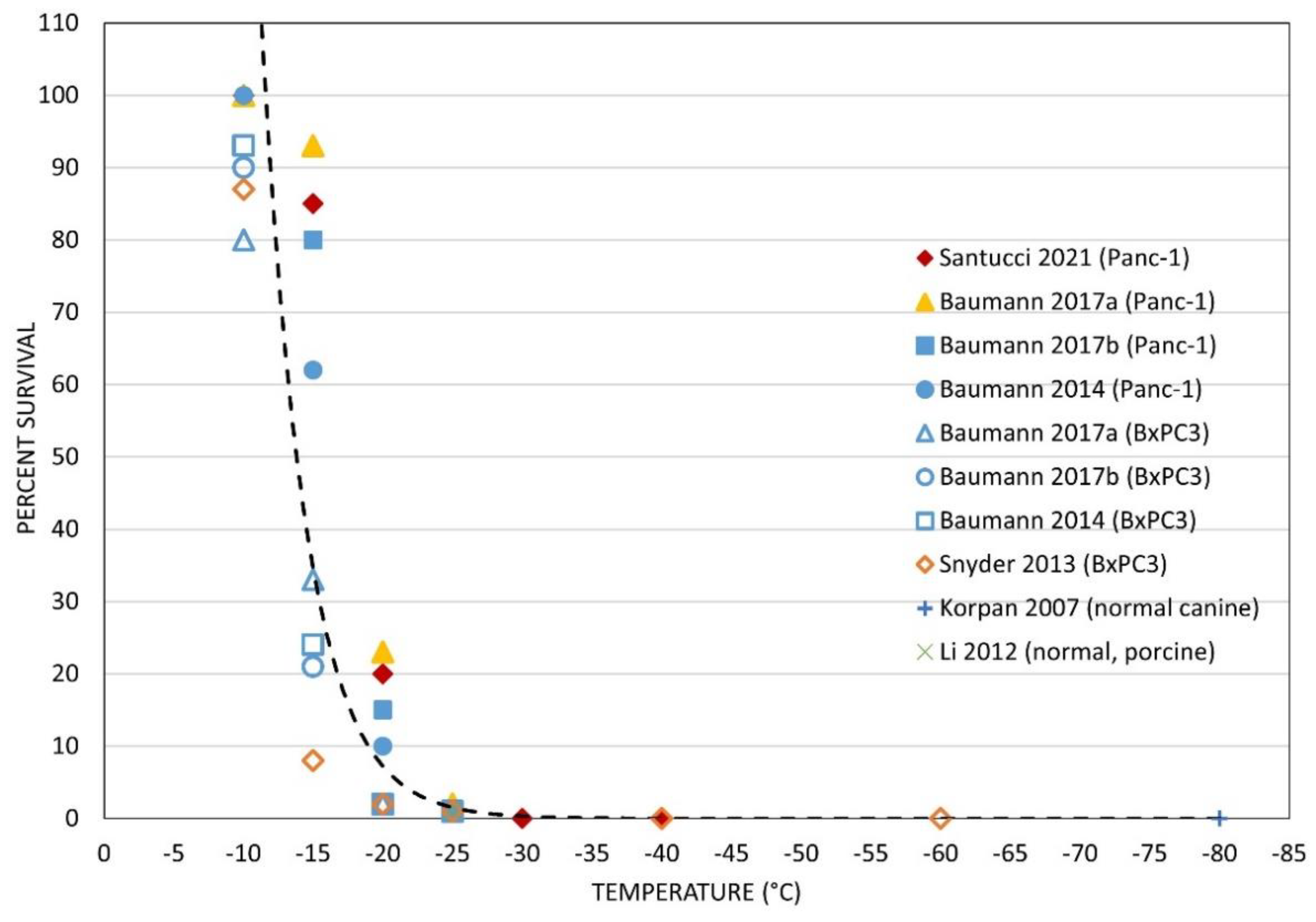
3.1. Pancreatic Cancer Cell Response to Cryoablation
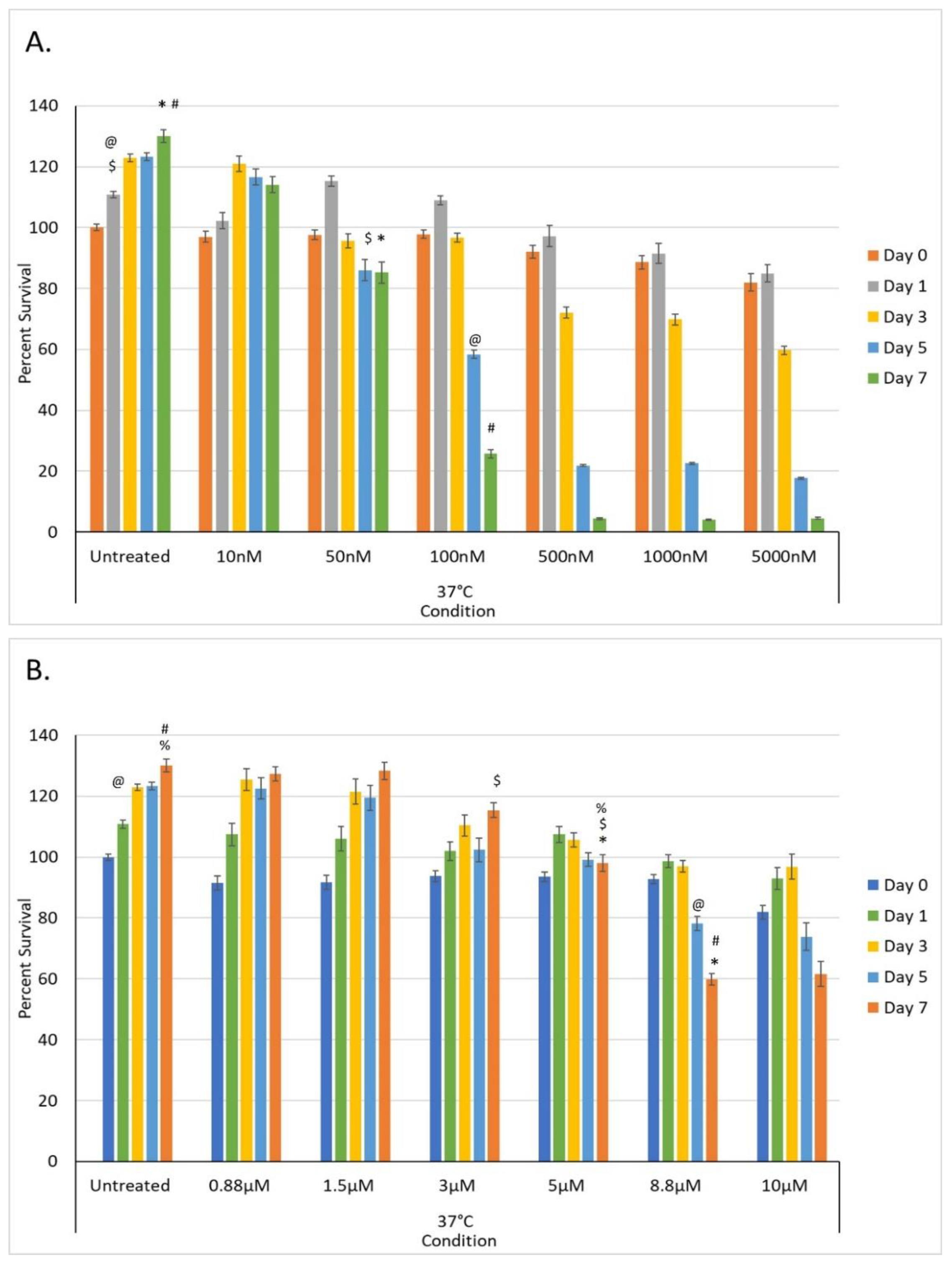
3.2. Drug Exposure Dose Response of Pancreatic Cancer Cells In Vitro
3.2.1. Dose Response of PANC-1 Cells to Gemcitabine In Vitro
3.2.2. Dose Response of PANC-1 Cells to Oxaliplatin In Vitro
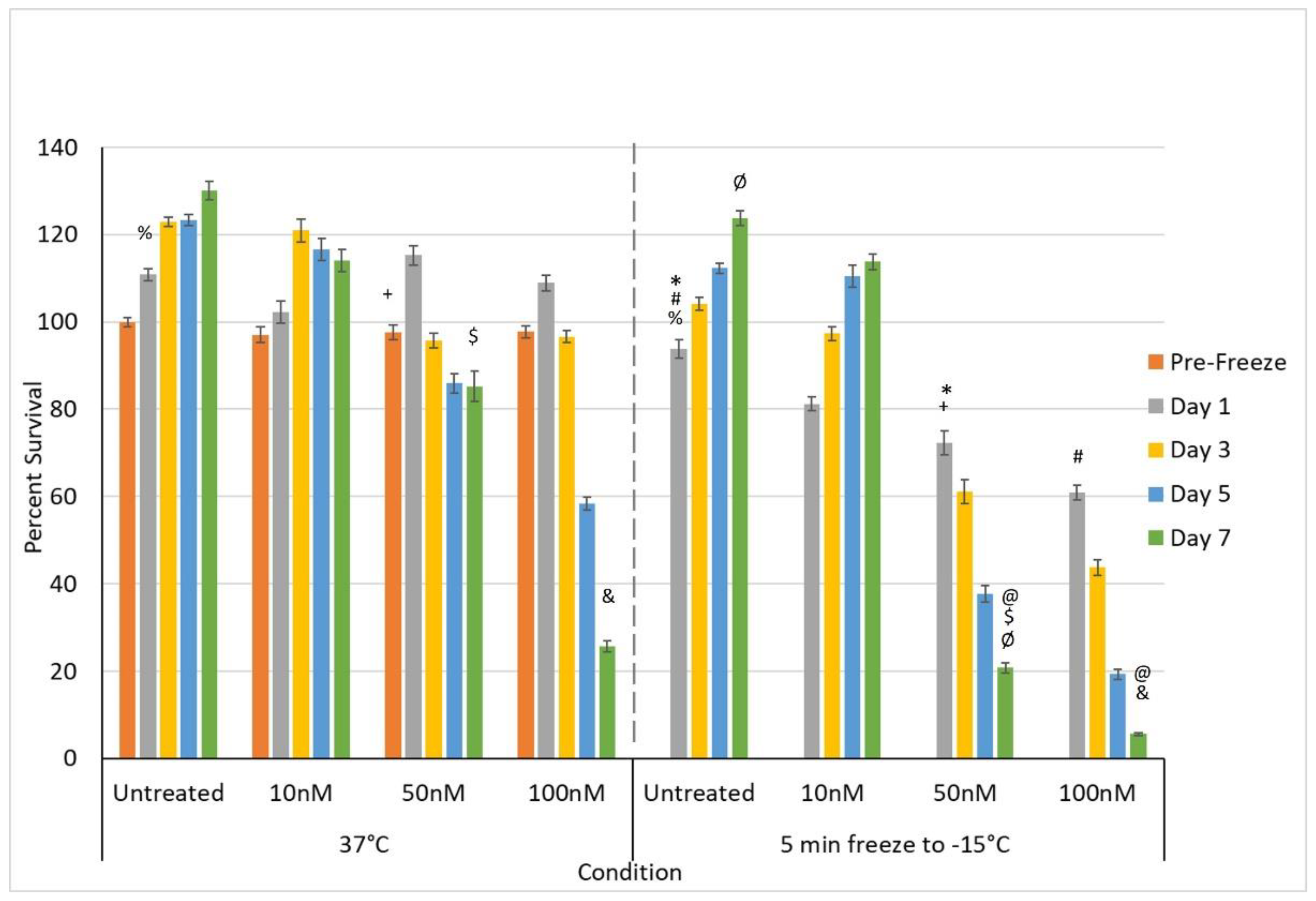
3.3. Impact of Adjunctive Chemo Pretreatment and Freezing on Pancreatic Cancer Cells
3.3.1. Impact of Adjunctive Gemcitabine Pretreatment and Mild Freezing
3.3.2. Impact of Adjunctive Oxaliplatin Pretreatment and Mild Freezing
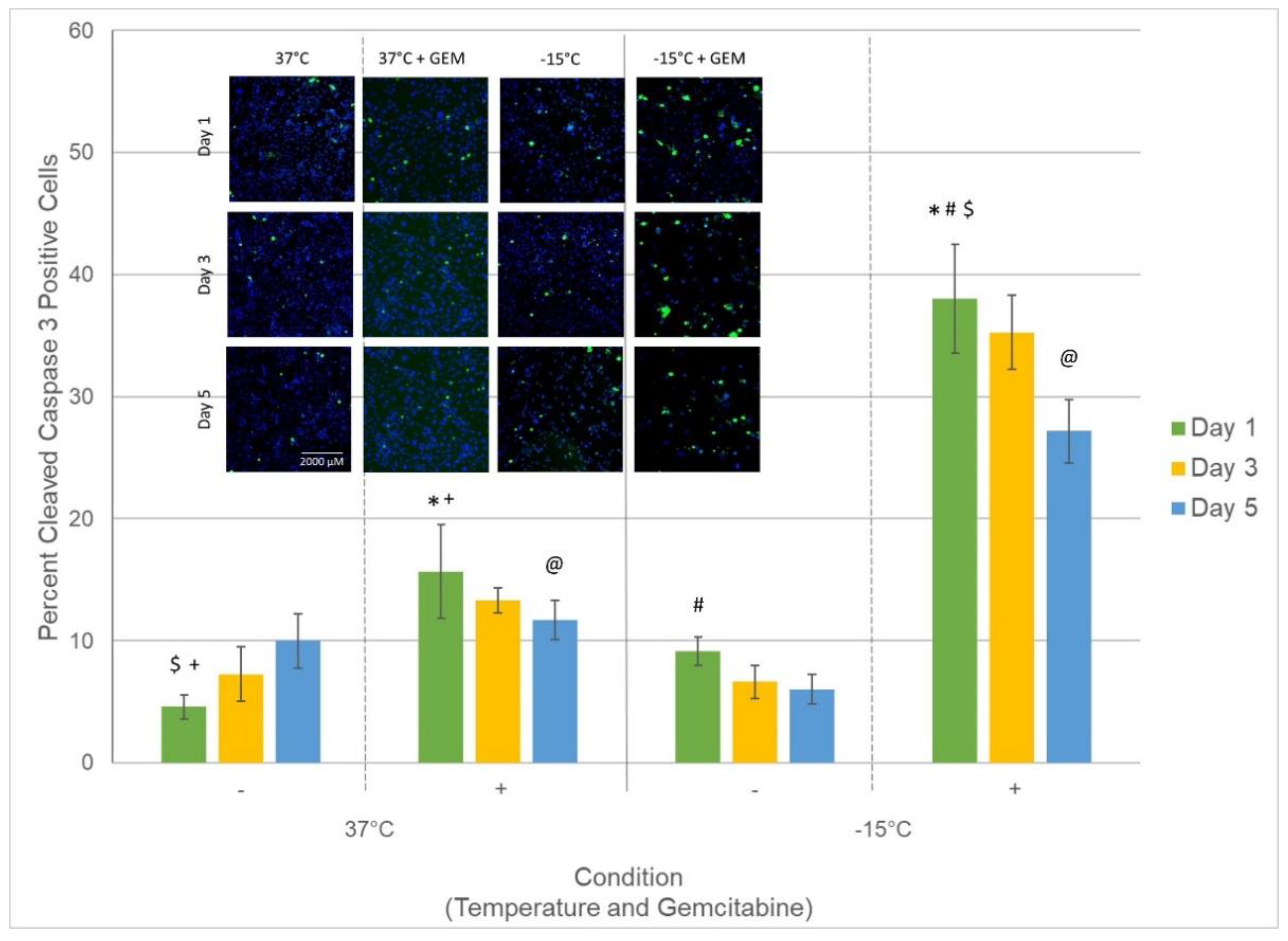
3.4. Assessment of Caspase Activity following Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Institute. SEER Cancer Statistics Review, 1975–2018; National Cancer Institute: Bethesda, MD, USA, 2021.
- Pancreatic Cancer. Available online: https://www.cancer.gov/types/pancreatic/patient/pancreatic-treatment-pdq (accessed on 15 November 2021).
- Pancreas Cancer: Statistics. Available online: https://www.cancer.net/cancer-types/pancreatic-cancer/types-treatment (accessed on 15 November 2021).
- Girelli, R.; Frigerio, I.; Salvia, R.; Barbi, E.; Tinazzi Martini, P.; Bassi, C. Feasibility and safety of radiofrequency ablation for locally advanced pancreatic cancer. Br. J. Surg. 2010, 97, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; El-Rayes, B.F. Small molecule tyrosine kinase inhibitors in pancreatic cancer. Biologics 2008, 2, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Lakkakula, B.; Farran, B.; Lakkakula, S.; Peela, S.; Yarla, N.S.; Bramhachari, P.V.; Kamal, M.A.; Saddala, M.S.; Nagaraju, G.P. Small molecule tyrosine kinase inhibitors and pancreatic cancer-Trials and troubles. Semin. Cancer Biol. 2019, 56, 149–167. [Google Scholar] [CrossRef]
- Bhullar, K.S.; Lagaron, N.O.; McGowan, E.M.; Parmar, I.; Jha, A.; Hubbard, B.P.; Rupasinghe, H.P.V. Kinase-targeted cancer therapies: Progress, challenges and future directions. Mol. Cancer 2018, 17, 48. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, C.; Faggion, B.; Balboni, B.; Carbone, D.; Peters, G.J.; Diana, P.; Assaraf, Y.G.; Giovannetti, E. GSK3beta as a novel promising target to overcome chemoresistance in pancreatic cancer. Drug Resist. Updates 2021, 58, 100779. [Google Scholar] [CrossRef]
- Baust, J.G.; Gage, A.A. The molecular basis of cryosurgery. BJU Int. 2005, 95, 1187–1191. [Google Scholar] [CrossRef]
- Gage, A.A.; Baust, J.M.; Baust, J.G. Experimental cryosurgery investigations in vivo. Cryobiology 2009, 59, 229–243. [Google Scholar] [CrossRef]
- Bang, H.J.; Littrup, P.J.; Currier, B.P.; Goodrich, D.J.; Aoun, H.D.; Klein, L.C.; Kuo, J.C.; Heilbrun, L.K.; Gadgeel, S.; Goodman, A.C. Percutaneous Cryoablation of Metastatic Lesions from Non–Small-Cell Lung Carcinoma: Initial Survival, Local Control, and Cost Observations. J. Vasc. Interv. Radiol. 2012, 23, 761–769. [Google Scholar] [CrossRef][Green Version]
- Mahnken, A.H.; Konig, A.M.; Figiel, J.H. Current Technique and Application of Percutaneous Cryotherapy. Rofo 2018, 190, 836–846. [Google Scholar] [CrossRef]
- Babaian, R.J.; Donnelly, B.; Bahn, D.; Baust, J.G.; Dineen, M.; Ellis, D.; Katz, A.; Pisters, L.; Rukstalis, D.; Shinohara, K.; et al. Best practice statement on cryosurgery for the treatment of localized prostate cancer. J. Urol. 2008, 180, 1993–2004. [Google Scholar] [CrossRef]
- Seager, M.; Kumar, S.; Lim, E.; Munneke, G.; Bandula, S.; Walkden, M. Renal cryoablation—A practical guide for interventional radiologists. Br. J. Radiol. 2021, 94, 20200854. [Google Scholar] [CrossRef]
- Pusceddu, C.; Paliogiannis, P.; Nigri, G.; Fancellu, A. Cryoablation in the Management Of Breast Cancer: Evidence To Date. Breast Cancer 2019, 11, 283–292. [Google Scholar] [CrossRef]
- Korpan, N.N. Cryosurgery: Early ultrastructural changes in liver tissue in vivo. J. Surg. Res. 2009, 153, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Liu, C.; Wang, X.M.; Chen, J.; Wang, D.; Merges, R. Functional CT in a rabbit model: Evaluation of the perfusion characteristics before and after Ar-He cryoablation therapy. J. Med. Imaging Radiat. Oncol. 2008, 52, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Edd, J.F.; Ivorra, A.; Horowitz, L.; Rubinsky, B. Imaging cryosurgery with EIT: Tracking the ice front and post-thaw tissue viability. Physiol. Meas. 2008, 29, 899–912. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nair, R.T.; Silverman, S.G.; Tuncali, K.; Obuchowski, N.A.; van Sonnenberg, E.; Shankar, S. Biochemical and hematologic alterations following percutaneous cryoablation of liver tumors: Experience in 48 procedures. Radiology 2008, 248, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.G.; Gage, A.A.; Ma, H.; Zhang, C.M. Minimally invasive cryosurgery-technological advances. Cryobiology 1997, 34, 373–384. [Google Scholar] [CrossRef]
- Gage, A.A.; Baust, J.G. Cryosurgery for tumors. J. Am. Coll. Surg. 2007, 205, 342–356. [Google Scholar] [CrossRef]
- Baust, J.G.; Bischof, J.C.; Jiang-Hughes, S.; Polascik, T.J.; Rukstalis, D.B.; Gage, A.A.; Baust, J.M. Re-purposing cryoablation: A combinatorial ‘therapy’ for the destruction of tissue. Prostate Cancer Prostatic Dis. 2015, 18, 87–95. [Google Scholar] [CrossRef]
- Baust, J.G.; Snyder, K.K.; Santucci, K.L.; Robilotto, A.T.; van Buskirk, R.G.; Baust, J.M. Cryoablation: Physical and molecular basis with putative immunological consequences. Int. J. Hyperth. 2019, 36, 10–16. [Google Scholar] [CrossRef]
- Baust, J.G.; Gage, A.A.; Bjerklund Johansen, T.E.; Baust, J.M. Mechanisms of cryoablation: Clinical consequences on malignant tumors. Cryobiology 2014, 68, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.M.; Rabin, Y.; Polascik, T.J.; Santucci, K.L.; Snyder, K.K.; Buskirk, R.G.V.; Baust, J.G. Defeating Cancers’ Adaptive Defensive Strategies Using Thermal Therapies: Examining Cancer’s Therapeutic Resistance, Ablative, and Computational Modeling Strategies as a means for Improving Therapeutic Outcome. Technol. Cancer Res. Treat. 2018, 17, 1533033818762207. [Google Scholar] [CrossRef] [PubMed]
- Klossner, D.P.; Robilotto, A.T.; Clarke, D.M.; VanBuskirk, R.G.; Baust, J.M.; Gage, A.A.; Baust, J.G. Cryosurgical technique: Assessment of the fundamental variables using human prostate cancer model systems. Cryobiology 2007, 55, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.M.; Robilotto, A.; Snyder, K.K.; Santucci, K.; Stewart, J.; van Buskirk, R.; Baust, J.G. Assessment of Cryosurgical Device Performance Using a 3D Tissue-Engineered Cancer Model. Technol. Cancer Res. Treat. 2017, 16, 900–909. [Google Scholar] [CrossRef]
- Niu, L.; Chen, J.; He, L.; Liao, M.; Yuan, Y.; Zeng, J.; Li, J.; Zuo, J.; Xu, K. Combination treatment with comprehensive cryoablation and immunotherapy in metastatic pancreatic cancer. Pancreas 2013, 42, 1143–1149. [Google Scholar] [CrossRef]
- Luo, X.M.; Niu, L.Z.; Chen, J.B.; Xu, K.C. Advances in cryoablation for pancreatic cancer. World J. Gastroenterol. 2016, 22, 790–800. [Google Scholar] [CrossRef]
- Pai, M.; Habib, N.; Senturk, H.; Lakhtakia, S.; Reddy, N.; Cicinnati, V.R.; Kaba, I.; Beckebaum, S.; Drymousis, P.; Kahaleh, M.; et al. Endoscopic ultrasound guided radiofrequency ablation, for pancreatic cystic neoplasms and neuroendocrine tumors. World J. Gastrointest. Surg. 2015, 7, 52–59. [Google Scholar] [CrossRef]
- Testoni, S.G.G.; Healey, A.J.; Dietrich, C.F.; Arcidiacono, P.G. Systematic review of endoscopy ultrasound-guided thermal ablation treatment for pancreatic cancer. Endosc. Ultrasound 2020, 9, 83–100. [Google Scholar] [CrossRef]
- Robilitto, A.T.; Baust, J.M.; Stewart, J.F.; van Buskirk, R.G.; Baust, J.G. Cryosurgical ablation in the gastrointestinal tract: Development of a novel cryosurgical platform. In Proceedings of the Cryo2016—Cool Developments in Cryomedicine—New Devices and Strategies, Ottawa, ON, Canada, 23–27 July 2016. [Google Scholar]
- Kuck, K.H.; Furnkranz, A.; Chun, K.R.; Metzner, A.; Ouyang, F.; Schluter, M.; Elvan, A.; Lim, H.W.; Kueffer, F.J.; Arentz, T.; et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: Reintervention, rehospitalization, and quality-of-life outcomes in the FIRE AND ICE trial. Eur. Heart J. 2016, 37, 2858–2865. [Google Scholar] [CrossRef]
- Hachem, A.H.; Marine, J.E.; Tahboub, H.A.; Kamdar, S.; Kanjwal, S.; Soni, R.; Kanjwal, K. Radiofrequency Ablation versus Cryoablation in the Treatment of Paroxysmal Atrial Fibrillation: A Meta-Analysis. Cardiol. Res. Pract. 2018, 2018, 6276241. [Google Scholar] [CrossRef]
- Kim, K.M.; Chung, S.; Kim, S.Y.; Kim, D.J.; Kim, J.S.; Lim, C.; Park, K.H. Comparison of Radiofrequency Ablation and Cryoablation for the Recovery of Atrial Contractility and Survival. Korean J. Thorac. Cardiovasc. Surg. 2018, 51, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, P.; Huemer, M.; Shokor Parwani, A.; Boldt, L.H.; Mugge, A.; Haverkamp, W.; Wutzler, A. Pain Reactions during Pulmonary Vein Isolation under Deep Sedation: Cryothermal versus Radiofrequency Ablation. Pacing Clin. Electrophysiol. 2016, 39, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Chiu, D.; Niu, L.; Mu, F.; Peng, X.; Zhou, L.; Li, H.; Li, R.; Ni, J.; Jiang, N.; Hu, Y.; et al. The experimental study for efficacy and safety of pancreatic cryosurgery. Cryobiology 2010, 60, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Kovach, S.J.; Hendrickson, R.J.; Cappadona, C.R.; Schmidt, C.M.; Groen, K.; Koniaris, L.G.; Sitzmann, J.V. Cryoablation of unresectable pancreatic cancer. Surgery 2002, 131, 463–464. [Google Scholar] [CrossRef]
- Saccomandi, P.; Lapergola, A.; Longo, F.; Schena, E.; Quero, G. Thermal ablation of pancreatic cancer: A systematic literature review of clinical practice and pre-clinical studies. Int. J. Hyperth. 2018, 35, 398–418. [Google Scholar] [CrossRef]
- Santucci, K.L.; Snyder, K.K.; Baust, J.G.; van Buskirk, R.G.; Baust, J.M. Investigation of Liver Cancer Cell Response to Cryoablation and Adjunctive Based Cryo/Chemotherapy. Br. J. Cancer Res. 2020, 3, 407–414. [Google Scholar] [CrossRef]
- Santucci, K.L.; Baust, J.M.; Snyder, K.K.; van Buskirk, R.G.; Katz, A.; Corcoran, A.; Baust, J.G. Investigation of Bladder Cancer Cell Response to Cryoablation and Adjunctive Cisplatin Based Cryo/Chemotherapy. Clin. Res. Open Access 2020, 6, 1–11. [Google Scholar] [CrossRef]
- Santucci, K.L.; Baust, J.M.; Snyder, K.K.; van Buskirk, R.G.; Baust, J.G. Dose Escalation of Vitamin D3 Yields Similar Cryosurgical Outcome to Single Dose Exposure in a Prostate Cancer Model. Cancer Control. 2018, 25, 1073274818757418. [Google Scholar] [CrossRef]
- Baust, J.M.; Klossner, D.P.; Robilotto, A.T.; van Buskirk, R.G.; Gage, A.A.; Polascik, T.J.; Baust, J.G. Vitamin D3 therapy increases cryoablation efficacy: A novel strategy for the treatment of prostate cancer. Cryobiology 2014, 69, 198. [Google Scholar]
- Santucci, K.L.; Snyder, K.K.; Baust, J.M.; van Buskirk, R.G.; Mouraviev, V.; Polascik, T.J.; Gage, A.A.; Baust, J.G. Use of 1,25alpha dihydroxyvitamin D3 as a cryosensitizing agent in a murine prostate cancer model. Prostate Cancer Prostatic Dis. 2011, 14, 97–104. [Google Scholar] [CrossRef]
- Clarke, D.M.; Robilotto, A.T.; van Buskirk, R.G.; Baust, J.G.; Gage, A.A.; Baust, J.M. Targeted induction of apoptosis via TRAIL and cryoablation: A novel strategy for the treatment of prostate cancer. Prostate Cancer Prostatic Dis. 2007, 10, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Robilotto, A.T.; Rhee, E.; VanBuskirk, R.G.; Baust, J.G.; Gage, A.A.; Baust, J.M. Cryoablation of renal cancer: Variables involved in freezing-induced cell death. Technol Cancer Res. Treat. 2007, 6, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Baust, J.M.; van Buskirk, R.G.; Baust, J.G. Addition of anticancer agents enhances freezing-induced prostate cancer cell death: Implications of mitochondrial involvement. Cryobiology 2004, 49, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Baust, J.M.; van Buskirk, R.G.; Baust, J.G. Chemo-cryo combination therapy: An adjunctive model for the treatment of prostate cancer. Cryobiology 2001, 42, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Anderson, K.; Slaton, J.; Schmidlin, F.; Vercellotti, G.; Belcher, J.; Bischof, J.C. Adjuvant approaches to enhance cryosurgery. J. Biomech. Eng. 2009, 131, 074003. [Google Scholar] [CrossRef]
- Han, B.; Iftekhar, A.; Bischof, J.C. Improved cryosurgery by use of thermophysical and inflammatory adjuvants. Technol. Cancer Res. Treat. 2004, 3, 103–111. [Google Scholar] [CrossRef]
- Le Pivert, P.; Haddad, R.S.; Aller, A.; Titus, K.; Doulat, J.; Renard, M.; Morrison, D.R. Ultrasound guided combined cryoablation and microencapsulated 5-Fluorouracil inhibits growth of human prostate tumors in xenogenic mouse model assessed by luminescence imaging. Technol. Cancer Res. Treat. 2004, 3, 135–142. [Google Scholar] [CrossRef]
- Forest, V.; Peoch, M.; Ardiet, C.; Campos, L.; Guyotat, D.; Vergnon, J.M. In vivo cryochemotherapy of a human lung cancer model. Cryobiology 2005, 51, 92–101. [Google Scholar] [CrossRef]
- Yuan, F.; Zhou, W.; Zhang, J.; Zhang, Z.; Zou, C.; Huang, L.; Zhang, Y.; Dai, Z. Anticancer drugs are synergistic with freezing in induction of apoptosis in HCC cells. Cryobiology 2008, 57, 60–65. [Google Scholar] [CrossRef]
- Jiang, J.; Goel, R.; Iftekhar, M.A.; Visaria, R.; Belcher, J.D.; Vercellotti, G.M.; Bischof, J.C. Tumor necrosis factor-alpha-induced accentuation in cryoinjury: Mechanisms in vitro and in vivo. Mol. Cancer Ther. 2008, 7, 2547–2555. [Google Scholar] [CrossRef]
- Klossner, D.P.; Baust, J.M.; van Buskirk, R.G.; Gage, A.A.; Baust, J.G. Cryoablative response of prostate cancer cells is influenced by androgen receptor expression. BJU Int. 2008, 101, 1310–1316. [Google Scholar] [CrossRef] [PubMed]
- Gradiz, R.; Silva, H.C.; Carvalho, L.; Botelho, M.F.; Mota-Pinto, A. MIA PaCa-2 and PANC-1—Pancreas ductal adenocarcinoma cell lines with neuroendocrine differentiation and somatostatin receptors. Sci. Rep. 2016, 6, 21648. [Google Scholar] [CrossRef] [PubMed]
- Deer, E.L.; Gonzalez-Hernandez, J.; Coursen, J.D.; Shea, J.E.; Ngatia, J.; Scaife, C.L.; Firpo, M.A.; Mulvihill, S.J. Phenotype and genotype of pancreatic cancer cell lines. Pancreas 2010, 39, 425–435. [Google Scholar] [CrossRef]
- Fukasawa, M.; Korc, M. Vascular endothelial growth factor-trap suppresses tumorigenicity of multiple pancreatic cancer cell lines. Clin. Cancer Res. 2004, 10, 3327–3332. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Jiao, X.; Jiang, Y.; Sun, S. ERK1/2 activity contributes to gemcitabine resistance in pancreatic cancer cells. J. Int. Med. Res. 2013, 41, 300–306. [Google Scholar] [CrossRef]
- Baumann, K.W.; Baust, J.M.; Snyder, K.K.; Baust, J.G.; van Buskirk, R.G. Characterization of Pancreatic Cancer Cell Thermal Response to Heat Ablation or Cryoablation. Technol. Cancer Res. Treat. 2017, 16, 393–405. [Google Scholar] [CrossRef]
- Baumann, K.W.; Baust, J.M.; Snyder, K.K.; Baust, J.G.; van Buskirk, R.G. Dual thermal ablation of pancreatic cancer cells as an improved combinatorial treatment stragegy. Liver Pancreat. Sci. 2017, 2, 1–10. [Google Scholar] [CrossRef]
- Snyder, K.K.; van Buskirk, R.G.; Baumann, K.W.; Baust, J.M.; Baust, J.G. Responses of pancreatic cancer cells under cryoablative conditions. Cryobiology 2013, 67, 428. [Google Scholar] [CrossRef]
- Fryer, R.A.; Barlett, B.; Galustian, C.; Dalgleish, A.G. Mechanisms underlying gemcitabine resistance in pancreatic cancer and sensitisation by the iMiD lenalidomide. Anticancer Res. 2011, 31, 3747–3756. [Google Scholar]
- Clarke, D.M.; Hollister, W.R.; Baust, J.G.; van Buskirk, R.G. Cryosurgical Modeling: Sequence of Freezing and Cytotoxic Agent Application Affects Cell Death. Mol. Urol. 1999, 3, 25–31. [Google Scholar]
- Santucci, K.L.; Snyder, K.K.; Baust, J.M.; van Buskirk, R.G.; Mouraviev, V.; Polascik, T.J.; Baust, J.G. The use of 1,25[alpha] dihydryoxyvitamin D3 as a cryosensitizing agent in a murine prostate cancer model. Cryobiology 2010, 61, 395. [Google Scholar] [CrossRef]
- Baust, J.M.; Klossner, D.P.; Robilotto, A.T.; Vanbuskirk, R.G.; Gage, A.A.; Mouraviev, V.; Polascik, T.J.; Baust, J.G. Vitamin D(3) cryosensitization increases prostate cancer susceptibility to cryoablation via mitochondrial-mediated apoptosis and necrosis. BJU Int. 2012, 109, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Forest, V.; Peoc’h, M.; Campos, L.; Guyotat, D.; Vergnon, J.M. Benefit of a combined treatment of cryotherapy and chemotherapy on tumour growth and late cryo-induced angiogenesis in a non-small-cell lung cancer model. Lung Cancer 2006, 54, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Ikekawa, S.; Ishihara, K.; Tanaka, S.; Ikeda, S. Basic studies of cryochemotherapy in a murine tumor system. Cryobiology 1985, 22, 477–483. [Google Scholar] [CrossRef]
- Mir, L.M.; Rubinsky, B. Treatment of cancer with cryochemotherapy. Br. J. Cancer 2002, 86, 1658–1660. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pham, L.; Dahiya, R.; Rubinsky, B. An in vivo study of antifreeze protein adjuvant cryosurgery. Cryobiology 1999, 38, 169–175. [Google Scholar] [CrossRef]
- Wang, C.L.; Teo, K.Y.; Han, B. An amino acidic adjuvant to augment cryoinjury of MCF-7 breast cancer cells. Cryobiology 2008, 57, 52–59. [Google Scholar] [CrossRef]
- Kimura, M.; Rabbani, Z.; Mouraviev, V.; Tsivian, M.; Caso, J.; Satoh, T.; Baba, S.; Vujaskovic, Z.; Baust, J.M.; Baust, J.G.; et al. Role of vitamin D(3) as a sensitizer to cryoablation in a murine prostate cancer model: Preliminary in vivo study. Urology 2010, 76, 764.E14–764.E20. [Google Scholar] [CrossRef]
- GEMZAR Prescribing Information. Available online: https://pi.lilly.com/us/gemzar.pdf (accessed on 22 November 2021).
- Xiong, H.Q.; Varadhachary, G.R.; Blais, J.C.; Hess, K.R.; Abbruzzese, J.L.; Wolff, R.A. Phase 2 trial of oxaliplatin plus capecitabine (XELOX) as second-line therapy for patients with advanced pancreatic cancer. Cancer 2008, 113, 2046–2052. [Google Scholar] [CrossRef]
- Bullock, A.; Stuart, K.; Jacobus, S.; Abrams, T.; Wadlow, R.; Goldstein, M.; Miksad, R. Capecitabine and oxaliplatin as first and second line treatment for locally advanced and metastatic pancreatic ductal adenocarcinoma. J. Gastrointest. Oncol. 2017, 8, 945–952. [Google Scholar] [CrossRef]
- Robilotto, A.T.; Baust, J.M.; van Buskirk, R.G.; Gage, A.A.; Baust, J.G. Temperature-dependent activation of differential apoptotic pathways during cryoablation in a human prostate cancer model. Prostate Cancer Prostatic Dis. 2013, 16, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Robilotto, A.T.; Clarke, D.; Baust, J.M.; van Buskirk, R.G.; Gage, A.A.; Baust, J.G. Development of a tissue engineered human prostate tumor equivalent for use in the evaluation of cryoablative techniques. Technol. Cancer Res. Treat. 2007, 6, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.G.; Smith, J.T.; Santucci, K.L.; Snyder, K.K.; Robilotto, A.T.; Van Buskirk, R.G.; Baust, J.M.; Corwin, W.L.; McKain, J.F. Tissue Engineered Model and Method of Use. USPTO Patent 9,213,0259,213,025, 15 December 2015. [Google Scholar]
- Baust, J.G.; Smith, J.T.; Santucci, K.L.; Snyder, K.K.; Roilotto, A.T.; van Buskirk, R.G.; Baust, J.M.; Corwin, W.L.; McKain, J.F. Evaluation of a Novel Cystoscopic Compatible Cryocatheter for the Treatment of Bladder Cancer. Bladder Cancer 2020, 6, 303–318. [Google Scholar] [CrossRef]
- Robilotto, A.T.; Baust, J.M.; Santucci, K.L.; Snyder, K.K.; van Buskirk, R.G. Assessment of a novel supercritical nitrogen cryosurgical device using prostate and renal cancer tissue engineered models. Med. Devices Diagn. Eng. 2020, 5, 1–8. [Google Scholar] [CrossRef]
- Robilotto, A.T.; Baust, J.M.; van Buskirk, R.G.; Gage, A.A.; Baust, J.G. Rapid induction of apoptosis at ultra low temperatures enhances the efficacy of prostate cancer cryoablation. Cryobiology 2013, 66, 354. [Google Scholar] [CrossRef]
- Baust, J.M.; Snyder, K.K.; Santucci, K.L.; Robilitto, A.T.; Smith, J.T.; McKain, J.F. Assessment of SCN and argon cryoablation devices in an in vivo like 3-D tissue engineered prostate and renal cancer model. In Proceedings of the Advances in Thermal Ablative Therapy and Biopreservation, Annual Meeting of the American College of Cryosurgery 2014, Key Largo, FL, USA, 15–19 January 2014. [Google Scholar]
- Baumann, K.W.; Snyder, K.K.; Baust, J.M.; van Buskirk, R.G.; Baust, J.G. Monitoring the effects of dual thermal ablation on pancreatic cancer cell line PANC-1. Cryobiology 2014, 69, 504–505. [Google Scholar] [CrossRef]
- Korpan, N.N. Cryosurgery: Ultrastructural changes in pancreas tissue after low temperature exposure. Technol. Cancer Res. Treat. 2007, 6, 59–67. [Google Scholar] [CrossRef]
- Li, J.; Zhou, L.; Chen, J.; Wu, B.; Zeng, J.; Fang, G.; Deng, C.; Huang, S.; Yao, F.; Chen, Z.; et al. Pancreatic head cryosurgery: Safety and efficiency in vivo—A pilot study. Pancreas 2012, 41, 1285–1291. [Google Scholar] [CrossRef]
- De Sousa Cavalcante, L.; Monteiro, G. Gemcitabine: Metabolism and molecular mechanisms of action, sensitivity and chemoresistance in pancreatic cancer. Eur. J. Pharmacol. 2014, 741, 8–16. [Google Scholar] [CrossRef]
- Fegrachi, S.; Molenaar, I.Q.; Klaessens, J.H.; Besselink, M.G.; Offerhaus, J.A.; van Hillegersberg, R. Radiofrequency ablation of the pancreas: Two-week follow-up in a porcine model. Eur. J. Surg. Oncol. 2014, 40, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Fegrachi, S.; Molenaar, I.Q.; Klaessens, J.H.; Besselink, M.G.; Offerhaus, J.A.; van Hillegersberg, R. Radiofrequency ablation of the pancreas with and without intraluminal duodenal cooling in a porcine model. J. Surg. Res. 2013, 184, 867–872. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics. CA Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Littrup, P.J.; Jallad, B.; Vorugu, V.; Littrup, G.; Currier, B.; George, M.; Herring, D. Lethal isotherms of cryoablation in a phantom study: Effects of heat load, probe size, and number. J. Vasc. Interv. Radiol. 2009, 20, 1343–1351. [Google Scholar] [CrossRef]
- Shah, T.T.; Arbel, U.; Foss, S.; Zachman, A.; Rodney, S.; Ahmed, H.U.; Arya, M. Modeling Cryotherapy Ice Ball Dimensions and Isotherms in a Novel Gel-based Model to Determine Optimal Cryo-needle Configurations and Settings for Potential Use in Clinical Practice. Urology 2016, 91, 234–240. [Google Scholar] [CrossRef]
- Alcindor, T.; Beauger, N. Oxaliplatin: A review in the era of molecularly targeted therapy. Curr. Oncol. 2011, 18, 18–25. [Google Scholar] [CrossRef]
- Kim, M.P.; Gallick, G.E. Gemcitabine resistance in pancreatic cancer: Picking the key players. Clin. Cancer Res. 2008, 14, 1284–1285. [Google Scholar] [CrossRef]
- Amrutkar, M.; Gladhaug, I.P. Pancreatic Cancer Chemoresistance to Gemcitabine. Cancers 2017, 9, 157. [Google Scholar] [CrossRef]
- Oldfield, L.E.; Connor, A.A.; Gallinger, S. Molecular Events in the Natural History of Pancreatic Cancer. Trends Cancer 2017, 3, 336–346. [Google Scholar] [CrossRef]
- Isayama, H.; Nakai, Y.; Yamamoto, K.; Sasaki, T.; Mizuno, S.; Yagioka, H.; Yashima, Y.; Kawakubo, K.; Kogure, H.; Arizumi, T.; et al. Gemcitabine and oxaliplatin combination chemotherapy for patients with refractory pancreatic cancer. Oncology 2011, 80, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Santucci, K.L.; Baust, J.M.; Snyder, K.K.; van Buskirk, R.G.; Baust, J.G. Investigation of the Impact of Cell Cycle Stage on Freeze Response Sensitivity of Androgen-Insensitive Prostate Cancer. Technol. Cancer Res. Treat. 2016, 15, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Sabel, M.S.; Su, G.; Griffith, K.A.; Chang, A.E. Rate of freeze alters the immunologic response after cryoablation of breast cancer. Ann. Surg. Oncol. 2010, 17, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.F.; Liu, P.; Xu, L.X. Recent advances in thermal treatment techniques and thermally induced immune responses against cancer. IEEE Trans. Biomed. Eng. 2014, 61, 1497–1505. [Google Scholar] [CrossRef]
- Takahashi, Y.; Izumi, Y.; Matsutani, N.; Dejima, H.; Nakayama, T.; Okamura, R.; Uehara, H.; Kawamura, M. Optimized magnitude of cryosurgery facilitating anti-tumor immunoreaction in a mouse model of Lewis lung cancer. Cancer Immunol. Immunother. 2016, 65, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Xu, K.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L. Prospective study of percutaneous cryoablation combined with allogenic NK cell immunotherapy for advanced renal cell cancer. Immunol. Lett. 2017, 184, 98–104. [Google Scholar] [CrossRef]
- Bang, H.J.; Littrup, P.J.; Currier, B.P.; Goodrich, D.J.; Choi, M.; Heilbrun, L.K.; Goodman, A.C. Percutaneous Cryoablation of Metastatic Lesions from Colorectal Cancer: Efficacy and Feasibility with Survival and Cost-Effectiveness Observations. ISRN Minim. Invasive Surg. 2012, 2012, 942364. [Google Scholar] [CrossRef][Green Version]
- Redondo, P.; del Olmo, J.; Lopez-Diaz de Cerio, A.; Inoges, S.; Marquina, M.; Melero, I.; Bendandi, M. Imiquimod enhances the systemic immunity attained by local cryosurgery destruction of melanoma lesions. J. Investig. Dermatol. 2007, 127, 1673–1680. [Google Scholar] [CrossRef]
- Baust, J.M.; Robilotto, A.T.; Gage, A.A.; Baust, J.G. Enhanced cryoablative methodologies. In Multiscale Technologies for Cryomedicine; Bischof, J.C., Xi, Y., Eds.; World Scientific Publishing Co.: Singapore, 2016; p. 388. [Google Scholar]
- Baust, J.G.; Gage, A.A.; Baust, J.M. Cryoablation: An emergent combinatorial therapy. In Proceedings of the 20th World Congress of the International Society of Cryosurgery, Haifa, Israel, 4–5 September 2019. [Google Scholar]
- Xu, H.; Wang, Q.; Lin, C.; Yin, Z.; He, X.; Pan, J.; Lu, G.; Zhang, S. Synergism between cryoablation and GM-CSF: Enhanced immune function of splenic dendritic cells in mice with glioma. Neuroreport 2015, 26, 346–353. [Google Scholar] [CrossRef]
- Shao, Q.; O’Flanagan, S.; Lam, T.; Roy, P.; Pelaez, F.; Burbach, B.J.; Azarin, S.M.; Shimizu, Y.; Bischof, J.C. Engineering T cell response to cancer antigens by choice of focal therapeutic conditions. Int. J. Hyperth. 2019, 36, 130–138. [Google Scholar] [CrossRef]
- Wu, F. Heat-Based Tumor Ablation: Role of the Immune Response. Adv. Exp. Med. Biol. 2016, 880, 131–153. [Google Scholar] [CrossRef] [PubMed]
- Korpan, N.N.; Goltsev, A.N.; Dronov, O.I.; Bondarovych, M.O. Cryoimmunology: Opportunities and challenges in biomedical science and practice. Cryobiology 2021, 100, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Abdo, J.; Cornell, D.L.; Mittal, S.K.; Agrawal, D.K. Immunotherapy Plus Cryotherapy: Potential Augmented Abscopal Effect for Advanced Cancers. Front. Oncol. 2018, 8, 85. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.R.; Lee, J.H.; Ponnazhagan, S. Revisiting Immunotherapy: A Focus on Prostate Cancer. Cancer Res. 2020, 80, 1615–1623. [Google Scholar] [CrossRef]
- Cerqueira, M.A.; Ferrari, K.L.; de Mattos, A.C.; Monti, C.R.; Reis, L.O. T cells CD4+/CD8+ local immune modulation by prostate cancer hemi-cryoablation. World J. Urol. 2020, 38, 673–680. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Average Ice Ball Size | Average Zone of Lethality | ||||
|---|---|---|---|---|---|
| Diameter (cm) | Volume (cm3) | Diameter (cm) | Volume (cm3) | % of Ice Ball | |
| Day 1 | 2.56 (±0.12) | 13.55 | 2.01 (±0.18) | 7.11 | 52.4 |
| Day 3 | 2.56 (±0.18) | 13.05 | 1.19 (±0.18) | 7.01 | 53.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baust, J.M.; Santucci, K.L.; Van Buskirk, R.G.; Raijman, I.; Fisher, W.E.; Baust, J.G.; Snyder, K.K. An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines 2022, 10, 450. https://doi.org/10.3390/biomedicines10020450
Baust JM, Santucci KL, Van Buskirk RG, Raijman I, Fisher WE, Baust JG, Snyder KK. An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines. 2022; 10(2):450. https://doi.org/10.3390/biomedicines10020450
Chicago/Turabian StyleBaust, John M., Kimberly L. Santucci, Robert G. Van Buskirk, Isaac Raijman, William E. Fisher, John G. Baust, and Kristi K. Snyder. 2022. "An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line" Biomedicines 10, no. 2: 450. https://doi.org/10.3390/biomedicines10020450
APA StyleBaust, J. M., Santucci, K. L., Van Buskirk, R. G., Raijman, I., Fisher, W. E., Baust, J. G., & Snyder, K. K. (2022). An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines, 10(2), 450. https://doi.org/10.3390/biomedicines10020450