
Inflammation Status and Body Composition Predict Two-Year Mortality of Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma under Provision of Recommended Energy Intake during Concurrent Chemoradiotherapy

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. CCRT Schedule
2.3. Provision of Recommended Daily Calorie during CCRT
2.4. Clinicopathological Data and Blood NIBs
2.5. Assessment of Body Composition Parameters
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Clinicopathological Variables, NIBs, Treatment Factors, Body Composition, and Prognosis in Patients Enrolled in Two Different Daily Calorie Supply Programs during CCRT
3.3. Factor Analysis
3.4. Correlation between Mean Daily Calorie Supply during CCRT Course and Treatment Interval Changes in the Blood NIBs and DXA-Derived Factors
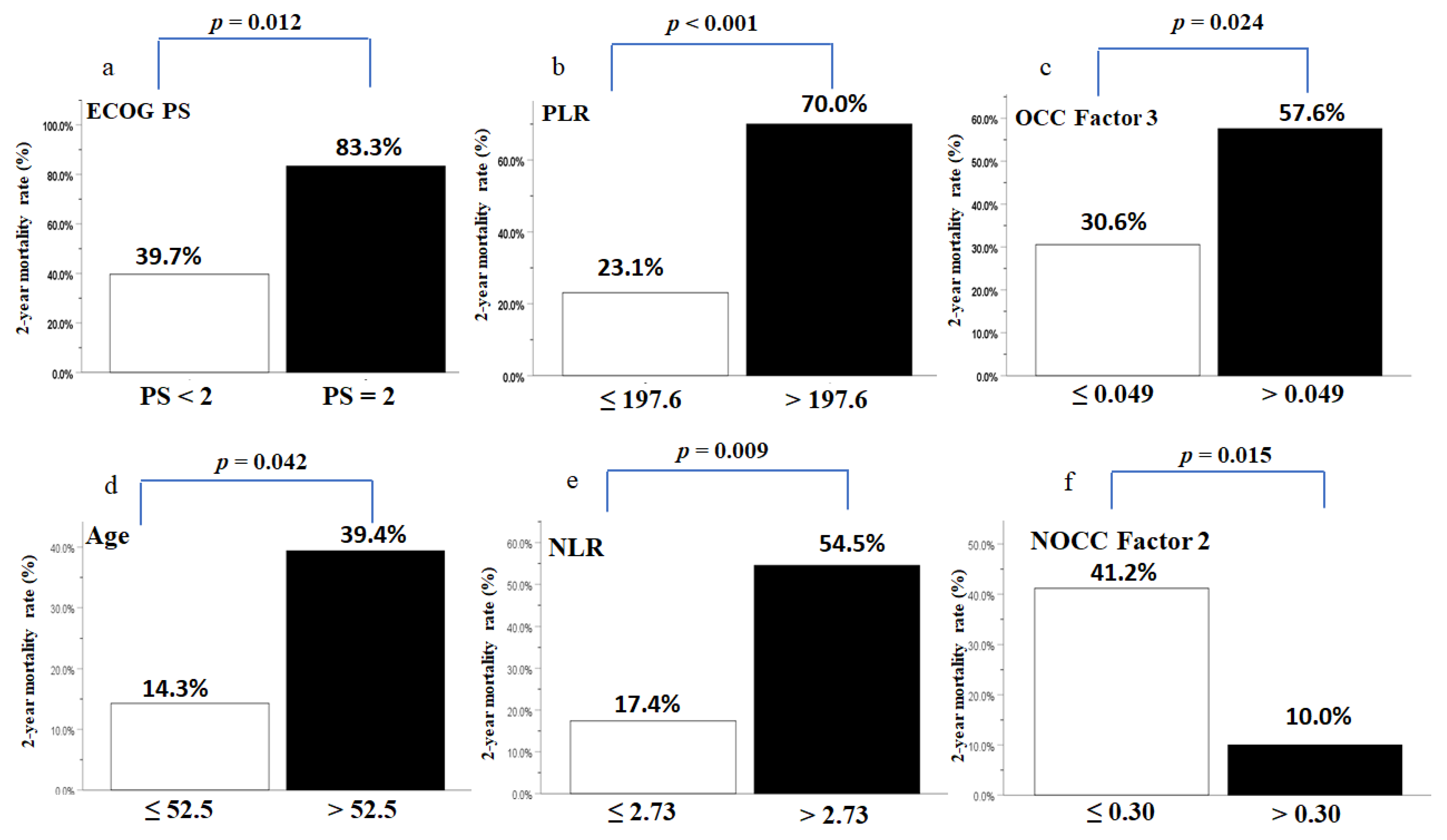
3.5. Factors Independently Contributing to the 2-Year Mortality Rate of Patients with LAHNSCC Receiving CCRT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adelstein, D.J.; Saxton, J.P.; Lavertu, P.; Tuason, L.; Wood, B.G.; Wanamaker, J.R.; Eliachar, I.; Strome, M.; Van Kirk, M.A. A phase III randomized trial comparing concurrent chemotherapy and radiotherapy with radiotherapy alone in resectable stage III and IV squamous cell head and neck cancer: Preliminary results. Head Neck 1997, 19, 567–575. [Google Scholar] [CrossRef]
- El-Sayed, S.; Nelson, N. Adjuvant and adjunctive chemotherapy in the management of squamous cell carcinoma of the head and neck region. A meta-analysis of prospective and randomized trials. J. Clin. Oncol. 1996, 14, 838–847. [Google Scholar] [CrossRef]
- Chasen, M.R.; Bhargava, R. A descriptive review of the factors contributing to nutritional compromise in patients with head and neck cancer. Support. Care Cancer 2009, 17, 1345–1351. [Google Scholar] [CrossRef]
- Gorenc, M.; Kozjek, N.R.; Strojan, P. Malnutrition and cachexia in patients with head and neck cancer treated with (chemo)radiotherapy. Rep. Pract. Oncol. Radiother. 2015, 20, 249–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, J.; Ishii, S.; Fukushima, T.; Natsuzako, A.; Sakamoto, F.; Natsuzako, A.; Sakamoto, J.; Okitaet, M. Factors affecting muscle strength in cancer patients receiving chemotherapy. J. Nov. Physiother. Rehabil. 2017, 1, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Orell-Kotikangas, H.; Osterlund, P.; Makitie, O.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Makitie, A.A. Cachexia at diagnosis is associated with poor survival in head and neck cancer patients. Acta Otolaryngol. 2017, 137, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Silver, H.J.; Dietrich, M.S.; Murphy, B.A. Changes in body mass, energy balance, physical function, and inflammatory state in patients with locally advanced head and neck cancer treated with concurrent chemoradiation after low-dose induction chemotherapy. Head Neck 2007, 29, 893–900. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Arends, J. The causes and consequences of cancer-associated malnutrition. Eur J. Oncol. Nurs. 2005, 9 (Suppl. 2), S51–S63. [Google Scholar] [CrossRef]
- Willemsen, A.C.H.; Hoeben, A.; Lalisang, R.I.; Van Helvoort, A.; Wesseling, F.W.R.; Hoebers, F.; Baijens, L.W.J.; Schols, A. Disease-induced and treatment-induced alterations in body composition in locally advanced head and neck squamous cell carcinoma. J. Cachexia Sarcopenia Muscle 2020, 11, 145–159. [Google Scholar] [CrossRef] [Green Version]
- Capuano, G.; Gentile, P.C.; Bianciardi, F.; Tosti, M.; Palladino, A.; Di Palma, M. Prevalence and influence of malnutrition on quality of life and performance status in patients with locally advanced head and neck cancer before treatment. Support. Care Cancer 2010, 18, 433–437. [Google Scholar] [CrossRef]
- Miyawaki, E.; Naito, T.; Nakashima, K.; Miyawaki, T.; Mamesaya, N.; Kawamura, T.; Shota, K.; Omori, H.; Wakuda, K.; Ono, A.; et al. Management of anorexia prevents skeletal muscle wasting during cisplatin-based chemotherapy for thoracic malignancies. JCSM Clin. Rep. 2020, 5, 8–15. [Google Scholar] [CrossRef]
- Lazzari, G.; De Cillis, M.A.; Buccoliero, G.; Silvano, G. Competing Morbidities In Advanced Head And Neck Squamous Cell Carcinoma Concurrent Chemoradiotherapy: A Strong Implication Of A Multidisciplinary Team Approach. Cancer Manag. Res. 2019, 11, 9771–9782. [Google Scholar] [CrossRef] [Green Version]
- Powrozek, T.; Dziwota, J.; Malecka-Massalska, T. Nutritional Deficiencies in Radiotherapy-Treated Head and Neck Cancer Patients. J. Clin. Med. 2021, 10, 574. [Google Scholar] [CrossRef] [PubMed]
- Seelaender, M.; Laviano, A.; Busquets, S.; Puschel, G.P.; Margaria, T.; Batista, M.L., Jr. Inflammation in Cachexia. Mediat. Inflamm. 2015, 2015, 536954. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hutterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Bardash, Y.; Olson, C.; Herman, W.; Khaymovich, J.; Costantino, P.; Tham, T. Platelet-Lymphocyte Ratio as a Predictor of Prognosis in Head and Neck Cancer: A Systematic Review and Meta-Analysis. Oncol. Res. Treat. 2019, 42, 665–677. [Google Scholar] [CrossRef]
- Chang, P.H.; Yeh, K.Y.; Huang, J.S.; Lai, C.H.; Wu, T.H.; Lan, Y.J.; Tsai, J.C.; Chen, E.Y.; Yang, S.W.; Wang, C.H. Pretreatment performance status and nutrition are associated with early mortality of locally advanced head and neck cancer patients undergoing concurrent chemoradiation. Eur. Arch. Otorhinolaryngol. 2013, 270, 1909–1915. [Google Scholar] [CrossRef]
- Dechaphunkul, T.; Martin, L.; Alberda, C.; Olson, K.; Baracos, V.; Gramlich, L. Malnutrition assessment in patients with cancers of the head and neck: A call to action and consensus. Crit. Rev. Oncol. Hematol. 2013, 88, 459–476. [Google Scholar] [CrossRef]
- Dixon, L.; Garcez, K.; Lee, L.W.; Sykes, A.; Slevin, N.; Thomson, D. Ninety Day Mortality After Radical Radiotherapy for Head and Neck Cancer. Clin. Oncol. R. Coll. Radiol. 2017, 29, 835–840. [Google Scholar] [CrossRef]
- Fanetti, G.; Polesel, J.; Fratta, E.; Muraro, E.; Lupato, V.; Alfieri, S.; Gobitti, C.; Minatel, E.; Matrone, F.; Caroli, A.; et al. Prognostic Nutritional Index Predicts Toxicity in Head and Neck Cancer Patients Treated with Definitive Radiotherapy in Association with Chemotherapy. Nutrients 2021, 13, 1277. [Google Scholar] [CrossRef]
- Ling, H.H.; Yeh, K.Y.; Ng, S.H.; Wang, C.H.; Lai, C.H.; Wu, T.H.; Chang, P.H.; Chou, W.C.; Chen, F.P.; Lin, Y.C. Determining Malnutrition Assessment Criteria to Predict One-Year Mortality for Locally Advanced Head and Neck Cancer Patients Undergoing Concurrent Chemoradiotherapy. Nutrients 2020, 12, 836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascarella, M.A.; Mannard, E.; Silva, S.D.; Zeitouni, A. Neutrophil-to-lymphocyte ratio in head and neck cancer prognosis: A systematic review and meta-analysis. Head Neck 2018, 40, 1091–1100. [Google Scholar] [CrossRef]
- Alshadwi, A.; Nadershah, M.; Carlson, E.R.; Young, L.S.; Burke, P.A.; Daley, B.J. Nutritional considerations for head and neck cancer patients: A review of the literature. J. Oral Maxillofac. Surg. 2013, 71, 1853–1860. [Google Scholar] [CrossRef] [PubMed]
- Baxi, S.S.; Schwitzer, E.; Jones, L.W. A review of weight loss and sarcopenia in patients with head and neck cancer treated with chemoradiation. Cancers Head Neck 2016, 1, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capozzi, L.C.; McNeely, M.L.; Lau, H.Y.; Reimer, R.A.; Giese-Davis, J.; Fung, T.S.; Culos-Reed, S.N. Patient-reported outcomes, body composition, and nutrition status in patients with head and neck cancer: Results from an exploratory randomized controlled exercise trial. Cancer 2016, 122, 1185–1200. [Google Scholar] [CrossRef] [Green Version]
- Couch, M.; Lai, V.; Cannon, T.; Guttridge, D.; Zanation, A.; George, J.; Hayes, D.N.; Zeisel, S.; Shores, C. Cancer cachexia syndrome in head and neck cancer patients: Part I. Diagnosis, impact on quality of life and survival, and treatment. Head Neck 2007, 29, 401–411. [Google Scholar] [CrossRef]
- Lango, M.N. Multimodal treatment for head and neck cancer. Surg. Clin. N. Am. 2009, 89, 43–52. [Google Scholar] [CrossRef]
- Almada-Correia, I.; Neves, P.M.; Makitie, A.; Ravasco, P. Body Composition Evaluation in Head and Neck Cancer Patients: A Review. Front. Oncol. 2019, 9, 1112. [Google Scholar] [CrossRef] [Green Version]
- Fouladiun, M.; Korner, U.; Bosaeus, I.; Daneryd, P.; Hyltander, A.; Lundholm, K.G. Body composition and time course changes in regional distribution of fat and lean tissue in unselected cancer patients on palliative care--correlations with food intake, metabolism, exercise capacity, and hormones. Cancer 2005, 103, 2189–2198. [Google Scholar] [CrossRef] [PubMed]
- Couch, M.E.; Dittus, K.; Toth, M.J.; Willis, M.S.; Guttridge, D.C.; George, J.R.; Chang, E.Y.; Gourin, C.G.; Der-Torossian, H. Cancer cachexia update in head and neck cancer: Pathophysiology and treatment. Head Neck 2015, 37, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.; Alexander, N.; Schipper, M.; Fig, L.; Feng, F.; Jolly, S. Characterization of changes in total body composition for patients with head and neck cancer undergoing chemoradiotherapy using dual-energy x-ray absorptiometry. Head Neck 2014, 36, 1356–1362. [Google Scholar] [CrossRef] [Green Version]
- Jager-Wittenaar, H.; Dijkstra, P.U.; Vissink, A.; Langendijk, J.A.; van der Laan, B.F.; Pruim, J.; Roodenburg, J.L. Changes in nutritional status and dietary intake during and after head and neck cancer treatment. Head Neck 2011, 33, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lonbro, S.; Dalgas, U.; Primdahl, H.; Johansen, J.; Nielsen, J.L.; Overgaard, J.; Overgaard, K. Lean body mass and muscle function in head and neck cancer patients and healthy individuals—Results from the DAHANCA 25 study. Acta Oncol. 2013, 52, 1543–1551. [Google Scholar] [CrossRef] [Green Version]
- Lonkvist, C.K.; Vinther, A.; Zerahn, B.; Rosenbom, E.; Deshmukh, A.S.; Hojman, P.; Gehl, J. Progressive resistance training in head and neck cancer patients undergoing concomitant chemoradiotherapy. Laryngoscope Investig. Otolaryngol. 2017, 2, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Ling, H.H.; Chang, P.H.; Pan, Y.P.; Wang, C.H.; Chou, W.C.; Chen, F.P.; Yeh, K.Y. Concurrent Chemoradiotherapy Induces Body Composition Changes in Locally Advanced Head and Neck Squamous Cell Carcinoma: Comparison between Oral Cavity and Non-Oral Cavity Cancer. Nutrients 2021, 13, 2969. [Google Scholar] [CrossRef]
- Yeh, K.Y.; Ling, H.H.; Ng, S.H.; Wang, C.H.; Chang, P.H.; Chou, W.C.; Chen, F.P.; Lin, Y.C. Role of the Appendicular Skeletal Muscle Index for Predicting the Recurrence-Free Survival of Head and Neck Cancer. Diagnostics 2021, 11, 309. [Google Scholar] [CrossRef] [PubMed]
- Wendrich, A.W.; Swartz, J.E.; Bril, S.I.; Wegner, I.; de Graeff, A.; Smid, E.J.; de Bree, R.; Pothen, A.J. Low skeletal muscle mass is a predictive factor for chemotherapy dose-limiting toxicity in patients with locally advanced head and neck cancer. Oral Oncol. 2017, 71, 26–33. [Google Scholar] [CrossRef]
- Boje, C.R.; Dalton, S.O.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. Evaluation of comorbidity in 9388 head and neck cancer patients: A national cohort study from the DAHANCA database. Radiother. Oncol. 2014, 110, 91–97. [Google Scholar] [CrossRef]
- Bruixola, G.; Caballero, J.; Papaccio, F.; Petrillo, A.; Iranzo, A.; Civera, M.; Moriana, M.; Bosch, N.; Maronas, M.; Gonzalez, I.; et al. Prognostic Nutritional Index as an independent prognostic factor in locoregionally advanced squamous cell head and neck cancer. ESMO Open 2018, 3, e000425. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef]
- Araki, K.; Ito, Y.; Fukada, I.; Kobayashi, K.; Miyagawa, Y.; Imamura, M.; Kira, A.; Takatsuka, Y.; Egawa, C.; Suwa, H.; et al. Predictive impact of absolute lymphocyte counts for progression-free survival in human epidermal growth factor receptor 2-positive advanced breast cancer treated with pertuzumab and trastuzumab plus eribulin or nab-paclitaxel. BMC Cancer 2018, 18, 982–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.P.; Chang, P.H.; Fan, C.W.; Tseng, W.K.; Huang, J.S.; Chen, C.H.; Chou, W.C.; Wang, C.H.; Yeh, K.Y. Relationship between pre-treatment nutritional status, serum glutamine, arginine levels and clinicopathological features in Taiwan colorectal cancer patients. Asia Pac. J. Clin. Nutr. 2015, 24, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Hangartner, T.N.; Warner, S.; Braillon, P.; Jankowski, L.; Shepherd, J. The Official Positions of the International Society for Clinical Densitometry: Acquisition of dual-energy X-ray absorptiometry body composition and considerations regarding analysis and repeatability of measures. J. Clin. Densitom 2013, 16, 520–536. [Google Scholar] [CrossRef]
- Bossola, M. Nutritional interventions in head and neck cancer patients undergoing chemoradiotherapy: A narrative review. Nutrients 2015, 7, 265–276. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, T.M.; Miguel Marin, D.; da Silva, C.A.; de Souza, A.L.; Talamoni, M.; Lima, C.S.; Monte Alegre, S. Evaluation of patients with head and neck cancer performing standard treatment in relation to body composition, resting metabolic rate, and inflammatory cytokines. Head Neck 2015, 37, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Peris, P.; Lozano, M.A.; Velasco, C.; de La Cuerda, C.; Iriondo, T.; Breton, I.; Camblor, M.; Navarro, C. Prospective study of resting energy expenditure changes in head and neck cancer patients treated with chemoradiotherapy measured by indirect calorimetry. Nutrition 2005, 21, 1107–1112. [Google Scholar] [CrossRef] [PubMed]
- Kubrak, C.; Olson, K.; Jha, N.; Scrimger, R.; Parliament, M.; McCargar, L.; Koski, S.; Baracos, V.E. Clinical determinants of weight loss in patients receiving radiation and chemoirradiation for head and neck cancer: A prospective longitudinal view. Head Neck 2013, 35, 695–703. [Google Scholar] [CrossRef]
- Langius, J.A.; Kruizenga, H.M.; Uitdehaag, B.M.; Langendijk, J.A.; Doornaert, P.; Leemans, C.R.; Weijs, P.J. Resting energy expenditure in head and neck cancer patients before and during radiotherapy. Clin. Nutr. 2012, 31, 549–554. [Google Scholar] [CrossRef]
- Ng, K.; Leung, S.F.; Johnson, P.J.; Woo, J. Nutritional consequences of radiotherapy in nasopharynx cancer patients. Nutr. Cancer 2004, 49, 156–161. [Google Scholar] [CrossRef]
- van den Berg, M.G.; Rasmussen-Conrad, E.L.; Gwasara, G.M.; Krabbe, P.F.; Naber, A.H.; Merkx, M.A. A prospective study on weight loss and energy intake in patients with head and neck cancer, during diagnosis, treatment and revalidation. Clin. Nutr. 2006, 25, 765–772. [Google Scholar] [CrossRef]
- Talwar, B.; Donnelly, R.; Skelly, R.; Donaldson, M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S32–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, K.H.; Kubrak, C.; Baracos, V.E.; Olson, K.; Mazurak, V.C. Recommended European Society of Parenteral and Enteral Nutrition protein and energy intakes and weight loss in patients with head and neck cancer. Head Neck 2016, 38, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- Jager-Wittenaar, H.; Dijkstra, P.U.; Vissink, A.; van der Laan, B.F.; van Oort, R.P.; Roodenburg, J.L. Critical weight loss in head and neck cancer--prevalence and risk factors at diagnosis: An explorative study. Support. Care Cancer 2007, 15, 1045–1050. [Google Scholar] [CrossRef] [Green Version]
- Kubrak, C.; Martin, L.; Gramlich, L.; Scrimger, R.; Jha, N.; Debenham, B.; Chua, N.; Walker, J.; Baracos, V.E. Prevalence and prognostic significance of malnutrition in patients with cancers of the head and neck. Clin. Nutr. 2020, 39, 901–909. [Google Scholar] [CrossRef]
- Mulasi, U.; Vock, D.M.; Kuchnia, A.J.; Jha, G.; Fujioka, N.; Rudrapatna, V.; Patel, M.R.; Teigen, L.; Earthman, C.P. Malnutrition Identified by the Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition Consensus Criteria and Other Bedside Tools Is Highly Prevalent in a Sample of Individuals Undergoing Treatment for Head and Neck Cancer. JPEN J. Parenter. Enter. Nutr. 2018, 42, 139–147. [Google Scholar] [CrossRef]
- Tayek, J.A.; Bistrian, B.R.; Hehir, D.J.; Martin, R.; Moldawer, L.L.; Blackburn, G.L. Improved protein kinetics and albumin synthesis by branched chain amino acid-enriched total parenteral nutrition in cancer cachexia. A prospective randomized crossover trial. Cancer 1986, 58, 147–157. [Google Scholar] [CrossRef]
- Daly, J.M.; Hearne, B.; Dunaj, J.; LePorte, B.; Vikram, B.; Strong, E.; Green, M.; Muggio, F.; Groshen, S.; DeCosse, J.J. Nutritional rehabilitation in patients with advanced head and neck cancer receiving radiation therapy. Am. J. Surg. 1984, 148, 514–520. [Google Scholar] [CrossRef]
- Lundholm, K.; Daneryd, P.; Bosaeus, I.; Korner, U.; Lindholm, E. Palliative nutritional intervention in addition to cyclooxygenase and erythropoietin treatment for patients with malignant disease: Effects on survival, metabolism, and function. Cancer 2004, 100, 1967–1977. [Google Scholar] [CrossRef]
- Mekhail, T.M.; Adelstein, D.J.; Rybicki, L.A.; Larto, M.A.; Saxton, J.P.; Lavertu, P. Enteral nutrition during the treatment of head and neck carcinoma: Is a percutaneous endoscopic gastrostomy tube preferable to a nasogastric tube? Cancer 2001, 91, 1785–1790. [Google Scholar] [CrossRef]
- Wang, J.; Liu, M.; Liu, C.; Ye, Y.; Huang, G. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for patients with head and neck cancer: A systematic review. J. Radiat. Res. 2014, 55, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argiles, J.M.; Olivan, M.; Busquets, S.; Lopez-Soriano, F.J. Optimal management of cancer anorexia-cachexia syndrome. Cancer Manag. Res. 2010, 2, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Tisdale, M.J. Mechanisms of cancer cachexia. Physiol. Rev. 2009, 89, 381–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, M.D.; Fearon, K.C.; Delmore, G.; Loprinzi, C.L. Should cancer patients with incurable disease receive parenteral or enteral nutritional support? Eur. J. Cancer 1998, 34, 279–285. [Google Scholar] [CrossRef]
- Yeh, K.Y.; Wang, H.M.; Chang, J.W.; Huang, J.S.; Lai, C.H.; Lan, Y.J.; Wu, T.H.; Chang, P.H.; Wang, H.; Wu, C.J.; et al. Omega-3 fatty acid-, micronutrient-, and probiotic-enriched nutrition helps body weight stabilization in head and neck cancer cachexia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 41–48. [Google Scholar] [CrossRef]
- McMillan, D.C. Systemic inflammation, nutritional status and survival in patients with cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Acharya, S.; Rai, P.; Hallikeri, K.; Anehosur, V.; Kale, J. Preoperative platelet lymphocyte ratio is superior to neutrophil lymphocyte ratio to be used as predictive marker for lymph node metastasis in oral squamous cell carcinoma. J. Investig. Clin. Dent. 2017, 8, e12219. [Google Scholar] [CrossRef]
- Malik, A.; Mishra, A.; Mair, M.; Chakrabarti, S.; Garg, A.; Singhvi, H.; Chopda, P.; Mathur, Y.; Shetty, R.; Nair, S.; et al. Role of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as prognostic markers in oral cavity cancers. Indian J. Med. Paediatr. Oncol. 2019, 40, 94–100. [Google Scholar] [CrossRef]
- Tham, T.; Bardash, Y.; Herman, S.W.; Costantino, P.D. Neutrophil-to-lymphocyte ratio as a prognostic indicator in head and neck cancer: A systematic review and meta-analysis. Head Neck 2018, 40, 2546–2557. [Google Scholar] [CrossRef] [PubMed]
- Park, H.C.; Kim, M.Y.; Kim, C.H. C-reactive protein/albumin ratio as prognostic score in oral squamous cell carcinoma. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.; Roh, J.L.; Lee, S.W.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Prognostic value of nutritional and hematologic markers in head and neck squamous cell carcinoma treated by chemoradiotherapy. Radiother. Oncol. 2016, 118, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Rosculet, N.; Zhou, X.C.; Ha, P.; Tang, M.; Levine, M.A.; Neuner, G.; Califano, J. Neutrophil-to-lymphocyte ratio: Prognostic indicator for head and neck squamous cell carcinoma. Head Neck 2017, 39, 662–667. [Google Scholar] [CrossRef]
- Sun, W.; Zhang, L.; Luo, M.; Hu, G.; Mei, Q.; Liu, D.; Long, G.; Hu, G. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Head Neck 2016, 38 (Suppl. 1), E1332–E1340. [Google Scholar] [CrossRef] [PubMed]
- Young, C.A.; Murray, L.J.; Karakaya, E.; Thygesen, H.H.; Sen, M.; Prestwich, R.J. The Prognostic Role of the Neutrophil-to-Lymphocyte Ratio in Oropharyngeal Carcinoma Treated with Chemoradiotherapy. Clin. Med. Insights Oncol. 2014, 8, 81–86. [Google Scholar] [CrossRef]
- Brown, D.J.; Milroy, R.; Preston, T.; McMillan, D.C. The relationship between an inflammation-based prognostic score (Glasgow Prognostic Score) and changes in serum biochemical variables in patients with advanced lung and gastrointestinal cancer. J. Clin. Pathol. 2007, 60, 705–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerem, M.; Ferahkose, Z.; Yilmaz, U.T.; Pasaoglu, H.; Ofluoglu, E.; Bedirli, A.; Salman, B.; Sahin, T.T.; Akin, M. Adipokines and ghrelin in gastric cancer cachexia. World J. Gastroenterol. 2008, 14, 3633–3641. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Matusiewicz, M.; Diakowska, D.; Grabowski, K.; Blachut, K.; Kustrzeba-Wojcicka, I.; Terlecki, G.; Gamian, A. Acute-phase response proteins are related to cachexia and accelerated angiogenesis in gastroesophageal cancers. Clin. Chem. Lab. Med. 2008, 46, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Costamagna, D.; Costelli, P.; Sampaolesi, M.; Penna, F. Role of Inflammation in Muscle Homeostasis and Myogenesis. Mediat. Inflamm. 2015, 2015, 805172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebadi, M.; Mazurak, V.C. Potential Biomarkers of Fat Loss as a Feature of Cancer Cachexia. Mediat. Inflamm. 2015, 2015, 820934. [Google Scholar] [CrossRef] [Green Version]
- Blauwhoff-Buskermolen, S.; Versteeg, K.S.; de van der Schueren, M.A.; den Braver, N.R.; Berkhof, J.; Langius, J.A.; Verheul, H.M. Loss of Muscle Mass During Chemotherapy Is Predictive for Poor Survival of Patients With Metastatic Colorectal Cancer. J. Clin. Oncol. 2016, 34, 1339–1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozzetti, F. Chemotherapy-Induced Sarcopenia. Curr. Treat. Options Oncol. 2020, 21, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F.; Cotogni, P. Nutritional Issues in Head and Neck Cancer Patients. Healthcare 2020, 8, 102. [Google Scholar] [CrossRef] [Green Version]
- Ghadjar, P.; Hayoz, S.; Zimmermann, F.; Bodis, S.; Kaul, D.; Badakhshi, H.; Bernier, J.; Studer, G.; Plasswilm, L.; Budach, V.; et al. Impact of weight loss on survival after chemoradiation for locally advanced head and neck cancer: Secondary results of a randomized phase III trial (SAKK 10/94). Radiat. Oncol. 2015, 10, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pin, F.; Couch, M.E.; Bonetto, A. Preservation of muscle mass as a strategy to reduce the toxic effects of cancer chemotherapy on body composition. Curr. Opin. Support. Palliat. Care 2018, 12, 420–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, R.A.; Al-Khalaf, M.; Megeney, L.A. The beneficial role of proteolysis in skeletal muscle growth and stress adaptation. Skelet. Muscle 2016, 6, 16–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanello, V.; Scalabrin, M.; Albiero, M.; Blaauw, B.; Scorrano, L.; Sandri, M. Inhibition of the Fission Machinery Mitigates OPA1 Impairment in Adult Skeletal Muscles. Cells 2019, 8, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, A.; Saraswat, M.; Joenvaara, S.; Agarwal, R.; Jyllikoski, D.; Wilkman, T.; Makitie, A.; Silen, S. Mass spectrometry-based lipidomics of oral squamous cell carcinoma tissue reveals aberrant cholesterol and glycerophospholipid metabolism—A Pilot study. Transl. Oncol. 2020, 13, 100807. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, G.; Jayaram, K.M.; Patil, R.V.; Malik, S. Alterations in serum lipid profile patterns in oral squamous cell carcinoma patients. J. Contemp. Dent. Pract. 2011, 12, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Halczy-Kowalik, L.; Drozd, A.; Stachowska, E.; Drozd, R.; Zabski, T.; Domagala, W. Fatty acids distribution and content in oral squamous cell carcinoma tissue and its adjacent microenvironment. PLoS ONE 2019, 14, e0218246. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Bresciani, E.; Rizzi, L.; Cappellari, O.; De Luca, A.; Torsello, A.; Liantonio, A. Cisplatin-Induced Skeletal Muscle Dysfunction: Mechanisms and Counteracting Therapeutic Strategies. Int. J. Mol. Sci. 2020, 21, 1242. [Google Scholar] [CrossRef] [Green Version]
- Garcia, J.M.; Scherer, T.; Chen, J.A.; Guillory, B.; Nassif, A.; Papusha, V.; Smiechowska, J.; Asnicar, M.; Buettner, C.; Smith, R.G. Inhibition of cisplatin-induced lipid catabolism and weight loss by ghrelin in male mice. Endocrinology 2013, 154, 3118–3129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pin, F.; Barreto, R.; Couch, M.E.; Bonetto, A.; O’Connell, T.M. Cachexia induced by cancer and chemotherapy yield distinct perturbations to energy metabolism. J. Cachexia Sarcopenia Muscle 2019, 10, 140–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gramignano, G.; Lusso, M.R.; Madeddu, C.; Massa, E.; Serpe, R.; Deiana, L.; Lamonica, G.; Dessi, M.; Spiga, C.; Astara, G.; et al. Efficacy of l-carnitine administration on fatigue, nutritional status, oxidative stress, and related quality of life in 12 advanced cancer patients undergoing anticancer therapy. Nutrition 2006, 22, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Pai, P.C.; Chuang, C.C.; Chuang, W.C.; Tsang, N.M.; Tseng, C.K.; Chen, K.H.; Yen, T.C.; Lin, C.Y.; Chang, K.P.; Lei, K.F. Pretreatment subcutaneous adipose tissue predicts the outcomes of patients with head and neck cancer receiving definitive radiation and chemoradiation in Taiwan. Cancer Med. 2018, 7, 1630–1641. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, D.; Paiar, F.; Saieva, C.; Bonomo, P.; Agresti, B.; Meattini, I.; Greto, D.; Mangoni, M.; Meacci, F.; Loi, M.; et al. Prognostic factors in patients with locally advanced head and neck cancer treated with concurrent radiochemotherapy. Radiol. Med. 2016, 121, 229–237. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| OCC with Postoperative Adjuvant CCRT | NOCC with Primary CCRT | ||
|---|---|---|---|
| Variables, Expressed as Numbers (%), Percentage (%), or Mean ± SD (Median) | p-Value * | ||
| Patient number | 69 (56.1) | 54 (43.9) | |
| Clinicopathologic variables | |||
| Sex | 0.203 | ||
| Male | 68 (98.6) | 51 (94.4) | |
| Female | 1 (1.4) | 3 (5.6) | |
| Age (years) (median) | 53.1 ± 8.4 (53.0) | 55.3 ± 8.5 (54.7) | 0.184 |
| <65 | 62 (89.9) | 46 (85.2) | 0.432 |
| ≥65 | 7 (10.1) | 8 (14.8) | |
| Tumor subsites (OCC/NOCC) | |||
| Buccal mucosa/Tonsil | 20 (29.0) | 13 (24.1) | |
| Tongue/Tongue base | 28 (40.6) | 6 (11.1) | |
| Gingiva/Soft palate | 13 (18.9) | 3 (5.6) | |
| Mouth floor/Hypopharynx | 3 (4.3) | 24 (44.4) | |
| Retromolar/Larynx | 2 (2.9) | 8 (14.8) | |
| Lip | 2 (2.9) | --- | |
| Hard palate | 1 (1.4) | --- | |
| TNM Stage | 0.613 | ||
| III | 4 (5.8) | 5 (9.3) | |
| IVA | 50 (72.5) | 35 (64.8) | |
| IVB | 15 (21.7) | 14 (25.9) | |
| T status (%) | 0.001 * | ||
| T0-2 | 11.6 | 37.0 | |
| T3-4 | 88.4 | 63.0 | |
| N status (%) | 0.007 * | ||
| N0-1 | 43.5 | 20.4 | |
| N2-3 | 56.5 | 79.6 | |
| Histological grade (%) | 0.023 * | ||
| Well differentiated | 11.6 | 3.7 | |
| Moderately differentiated | 73.9 | 63.0 | |
| Poorly differentiated | 14.5 | 33.3 | |
| Smoking user (%) | 91.3 | 90.7 | 0.913 |
| Alcohol user (%) | 73.9 | 75.9 | 0.799 |
| Betel nut user (%) | 76.8 | 50.0 | 0.002 * |
| HN-CCI (%) | 0.760 | ||
| 0 | 42.1 | 40.7 | |
| ≥1 | 57.9 | 59.3 | |
| ECOG performance status (%) | 0.046 * | ||
| 0 | 2.9 | 11.1 | |
| 1 | 86.4 | 87.0 | |
| 2 | 8.6 | 1.9 | |
| Tracheostomy (%) | 66.7 | 18.5 | <0.001 * |
| PG-SGA assessment before CCRT (%) | 0.328 | ||
| Stage A (well nourished) | 18.8 | 9.3 | |
| Stage B (moderately malnourished) | 55.1 | 61.1 | |
| Stage C (severely malnourished) | 26.1 | 29.6 | |
| Anthropometric data and blood NIB data | |||
| Before CCRT | |||
| BW (kg) (median) | 63.6 ± 12.6 (61.1) | 62.1 ± 12.1 (61.9) | 0.529 |
| BMI (kg/m2) (median) | 22.7 ± 4.3 (21.6) | 22.7 ± 4.0 (22.5) | 0.966 |
| <18.5 (%) | 20.3 | 20.4 | 0.991 |
| ≥18.5 (%) | 79.7 | 79.6 | |
| Hb (g/dL) (median) | 11.7 ± 1.5 (11.5) | 11.9 ± 1.7 (11.7) | 0.459 |
| WBC (×103 cells/mm3) (median) | 7.3 ± 2.5 (7.3) | 7.1 ± 2.9 (6.9) | 0.731 |
| Platelet count (×103/mm3) (median) | 341.1 ± 148.4 (327) | 251.4 ± 75.3 (241) | <0.001 * |
| TLC (×103 cells/mm3) (median) | 1.6 ± 0.6 (1.4) | 1.8 ± 0.7 (1.7) | 0.205 |
| <1.5 (%) | 46.4 | 33.3 | 0.144 |
| ≥1.5 (%) | 53.6 | 69.7 | |
| Albumin (g/dL) (median) | 3.8 ± 0.6 (3.8) | 3.8 ± 0.5 (3.7) | 0.720 |
| <3.5 (%) | 18.8 | 20.4 | 0.832 |
| ≥3.5 (%) | 81.2 | 79.6 | |
| CRP (mg/dL) (median) | 11.2 ± 1.8 (7.7) | 18.7 ± 6.6 (5.9) | 0.223 |
| NLR (median) | 3.7 ± 4.2 (3.0) | 2.9 ± 2.9 (2.3) | 0.241 |
| PLR (median) | 222.1 ± 70.3 (206.8) | 145.8 ± 99.2 (133.0) | 0.002 * |
| PNI (median) | 46.8 ± 6.2 (46.6) | 48.3 ± 5.4 (47.3) | 0.183 |
| Treatment interval change (%) | |||
| ΔBW% ** (median) | −4.1 ± 0.8 (−4.6) | −5.2 ± 1.1 (−6.3) | 0.426 |
| ΔBMI% ** (median) | −3.8 ± 0.8 (−4.7) | −5.4 ± 1.2 (−6.7) | 0.235 |
| ΔHb% ** (median) | −8.1 ± 1.8 (−9.5) | −11.1 ± 1.9 (−11.0) | 0.163 |
| ΔWBC% ** (median) | −21.7 ± 5.2 (−31.7) | −24.0 ± 5.9 (−34.6) | 0.768 |
| ΔPlatelet% ** (median) | −20.7 ± 3.7 (−30.1) | −13.9 ± 5.3 (−20.6) | 0.304 |
| ΔTLC% ** (median) | −39.2 ± 5.9 (−45.1) | −52.1 ± 4.7 (−51.7) | 0.103 |
| ΔAlbumin% ** (median) | 6.7 ± 2.8 (5.0) | 3.5 ± 2.5 (4.2) | 0.448 |
| ΔCRP% ** (median) | 58.2 ± 7.8 (55.5) | 47.6 ± 19.3 (68.6) | 0.174 |
| ΔNLR% ** (median) | 4.7 ± 1.8 (2.4) | 6.3 ± 1.4 (2.4) | 0.514 |
| ΔPLR% ** (median) | 206.5 ± 23.7 (72.3) | 218.6 ± 24.5 (129.9) | 0.074 |
| ΔPNI% ** (median) | −5.1 ± 1.9 (−4.9) | −10.5 ± 1.8 (−11.9) | 0.053 |
| DXA-related measurements | |||
| Before CCRT | |||
| LBM (kg) (median) | 43.7 ± 5.1 (43.2) | 43.6 ± 6.8 (43.4) | 0.846 |
| TFM (kg) (median) | 17.0 ± 8.8 (15.4) | 15.9 ± 6.0 (15.3) | 0.450 |
| ASM (kg) (median) | 18.4 ± 3.1 (18.4) | 18.7 ± 3.6 (19.0) | 0.636 |
| Android (%) (median) | 29.6 ± 13.4 (29.5) | 30.2 ± 10.5 (30.1) | 0.814 |
| Gynoid (%) (median) | 25.7 ± 5.3 (25.5) | 24.9 ± 6.1 (24.6) | 0.551 |
| Treatment interval change (%) | |||
| ΔLBM% ** (median) | −6.1 ± 5.7 (−6.0) | −5.6 ± 6.6 (−5.1) | 0.685 |
| ΔTFM% ** (median) | −2.6 ± 16.5 (−4.0) | −5.8 ± 18.5 (−6.9) | 0.308 |
| ΔASM% ** (median) | −7.8 ± 7.7 (−8.4) | −8.0 ± 9.8 (−6.6) | 0.901 |
| ΔAndroid% ** (median) | −0.3 ± 21.6(−0.6) | −2.2 ± 28.9 (−2.3) | 0.577 |
| ΔGynoid% ** (median) | 4.4 ± 14.6 (2.7) | 3.3 ± 20.7 (1.9) | 0.551 |
| Mean daily calorie intake during CCRT (kcal/kg/day, median) | 28.6 ± 8.6 (27.1) | 26.6 ± 7.4 (25.7) | 0.040 * |
| <30 (%) | 69.6 | 81.5 | 0.131 |
| ≥30 (%) | 30.4 | 18.5 | |
| Mean daily protein intake during CCRT (g/kg/day, median) | 1.1 ± 0.6 (1.2) | 1.0 ± 0.9 (1.1) | 0.324 |
| Feeding tube placement (%) | 68.1 | 37.3 | 0.022 * |
| Mean days of feeding tube placement during CCRT (median) | 34.5 ± 3.5 | 20.5 ± 3.7 | 0.017 * |
| CCRT data | |||
| Radiotherapy | |||
| Dose (Gy) (median) | 64.3 ± 4.5 (64.0) | 69.7 ± 3.1 (69.3) | <0.001 * |
| Fractions (median) | 31.9 ± 2.6 (32.0) | 33.4 ± 1.5 (32.9) | <0.001 * |
| Duration (days) (median) | 48.0 ± 4.8 (47) | 51.6 ± 8.1 (50) | 0.003 * |
| Cisplatin dose (mg/m2) (median) | 238.4 ± 45.5 (240) | 213.2 ± 66.0 (209) | 0.009 * |
| Grade 3/4 toxicity during CCRT | |||
| Non-hematologic | |||
| Dermatitis (%) | 4.3 | 3.7 | 0.858 |
| Pharyngitis (%) | 5.7 | 13.0 | 0.058 |
| Infection (%) | 14.4 | 31.5 | 0.024 * |
| Mucositis (%) | 26.0 | 25.9 | 0.870 |
| Emesis (%) | 8.7 | 7.4 | 0.795 |
| Hematologic | |||
| Anemia (%) | 7.2 | 11.0 | 0.289 |
| Neutropenia (%) | 33.3 | 38.9 | 0.524 |
| Thrombocytopenia | 5.7 | 13.0 | 0.167 |
| 2-year mortality rate (%) | 43.5 | 29.6 | 0.115 |
| OCC with Adjuvant CCRT | NOCC with Primary CCRT | |||||
|---|---|---|---|---|---|---|
| CCRT Completion | CCRT Completion | |||||
| Variables, Expressed as Numbers (%) or Mean ± SD | 25–30 kcal/kg/day | ≥30 kcal/kg/day | p-Value | 25–30 kcal/kg/day | ≥30 kcal/kg/day | p-Value * |
| Patient number | 48 (69.6) | 21 (30.4) | 43 (79.6) | 11 (20.4) | ||
| Clinicopathologic | ||||||
| Age (years) | 52.6 ± 8.7 | 54.5 ± 7.9 | 0.389 | 55.3 ± 8.5 | 55.2 ± 8.9 | 0.961 |
| Sex (male/female) | 47 (97.9): 1 (2.1) | 21 (100.0): 0 (0.0) | 0.505 | 41 (95.3): 2 (4.7) | 10 (90.9): 1 (9.1) | 0.566 |
| Tumor location (OCC/NOCC) | 0.353 | 0.441 | ||||
| Buccal mucosa/Tonsil | 17 (35.4) | 3 (14.2) | 10 (23.2) | 3 (27.2) | ||
| Tongue/Tongue base | 18 (37.5) | 10 (47.6) | 5 (11.6) | 1 (9.1) | ||
| Gingiva/Soft palate | 8 (16.6) | 5 (23.8) | 2 (4.7) | 1 (9.1) | ||
| Mouth floor/Hypopharynx | 2 (4.2) | 1 (4.8) | 19 (44.2) | 5 (45.5) | ||
| Retromolar/Larynx | 1 (2.1) | 1 (4.8) | 7 (16.3) | 1 (9.1) | ||
| Lip/Nasopharynx | 2 (4.2) | 0 (0.0) | -- | -- | ||
| Hard palate | 0 (0.0) | 1 (4.8) | -- | -- | ||
| TNM stage (III vs. IVA vs. IVB) | 2 (4.2): 34 (70.8): 12 (25.0) | 2 (9.5): 32 (76.2): 3 (14.3) | 0.460 | 4 (9.3): 28 (65.1): 11 (25.6) | 1 (9.1): 7 (63.6): 3 (27.3) | 0.993 |
| T status (T0-2 vs. T3-4) | 6 (12.5): 42 (87.5) | 2 (9.5): 15 (90.5) | 0.722 | 17 (39.5): 26 (60.5) | 3 (27.2): 8 (72.8) | 0.452 |
| N status (N0-1 vs. N2-3) | 22 (45.8): 26 (54.2) | 8 (38.1):13 (61.9) | 0.551 | 8 (18.6): 35 (81.4) | 3 (27.2): 8 (72.8) | 0.524 |
| ECOG performance status (0: 1: 2) | 2 (4.2): 43 (89.5): 3 (6.3) | 0 (0.0): 18 (85.7): 3 (14.3) | 0.371 | 6 (14.0): 37 (86.0): 0 (0.0) | 0 (0.0): 10 (90.9): 1 (9.1) | 0.065 |
| Histological grade (1: 2: 3) | 6 (12.5): 35 (72.9): 7 (14.6) | 2 (9.5): 16 (76.2): 3 (14.3) | 0.935 | 2 (4.4): 29 (63.0): 15 (32.6) | 1 (8.3): 6 (50.0): 5 (41.7) | 0.675 |
| Smoking (no/yes) | 5 (10.4): 43 (89.6) | 1 (4.5): 20 (90.2) | 0.443 | 4 (9.3): 39 (90.7) | 1 (9.1): 10 (90.9) | 0.983 |
| Alcohol (no/yes) | 13 (27.1): 351 (72.9) | 5 (23.8): 16 (76.2) | 0.776 | 12 (27.9): 31 (72.1) | 1 (9.1): 10 (90.9) | 0.193 |
| Betel nut (no/yes) | 11 (22.9): 37 (77.1) | 5 (23.8): 16 (76.2) | 0.936 | 20 (46.5): 23 (53.5) | 7 (68.6): 4 (31.4) | 0.311 |
| HN-CCI (0 vs. 1 vs. 2 vs. ≥3) | 19 (39.5): 13 (27.1): 2 (6.3): 13 (27.1) | 10 (47.6): 2 (9.5): 3 (14.3): 6 (28.1) | 0.478 | 16 (37.1): 12 (27.9): 6 (14.0): 9 (21.0) | 5 (45.5): 4 (36.4): 0 (0.0): 2 (18.1) | 0.715 |
| Tracheostomy (no/yes) | 19 (39.6): 29 (60.4) | 4 (19.0): 17 (81.0) | 0.096 | 22 (47.8): 24 (52.2) | 7 (68.6): 4 (31.4) | 0.088 |
| PG-SGA (stage A vs. stage B vs. stage C) before CCRT | 8 (16.7): 29 (60.4): 11 (22.9) | 5 (23.8): 9 (42.9): 7 (33.3) | 0.402 | 3 (8.7): 28 (63.0): 12 (28.3) | 2 (18.2): 5 (45.4): 4 (36.4) | 0.377 |
| Anthropometric and blood NIB data | ||||||
| Before CCRT | ||||||
| BW (kg) | 65.3 ± 12.5 | 54.9 ± 7.7 | <0.001 * | 65.1 ± 10.5 | 51.0 ± 11.7 | <0.001 * |
| BMI (kg/m2) | 23.9 ± 0.4 | 20.2 ± 0.7 | 0.001 * | 23.6 ± 3.5 | 19.1 ± 3.8 | 0.001 * |
| Hb (g/dL) | 11.7 ± 1.6 | 11.6 ± 1.0 | 0.780 | 11.9 ± 1.7 | 11.8 ± 1.6 | 0.820 |
| WBC (×103 cells/mm3) | 7.1 ± 2.4 | 7.6 ± 2.7 | 0.409 | 7.4 ± 3.2 | 5.9 ± 1.8 | 0.144 |
| Platelet count (×103/mm3) | 324.6 ± 126.4 | 378.9 ± 186.2 | 0.233 | 246.4 ± 71.6 | 270.0 ± 90.0 | 0.363 |
| TLC (×103 cells/mm3) | 1.0 ± 0.6 | 1.1 ± 0.7 | 0.905 | 1.9 ± 0.7 | 1.6 ± 0.4 | 0.115 |
| Albumin (g/dL) | 3.8 ± 0.5 | 3.8 ± 1.5 | 0.601 | 3.9 ± 0.4 | 3.6 ± 0.6 | 0.055 |
| CRP (mg/dL) | 10.5 ± 1.9 | 13.0 ± 4.0 | 0.521 | 18.1 ± 7.2 | 20.6 ± 12.6 | 0.879 |
| NLR | 3.4 ± 0.4 | 5.3 ± 2.5 | 0.307 | 2.9 ± 0.5 | 2.7 ± 0.4 | 0.809 |
| PLR | 216.4 ± 23.7 | 235.1 ± 31.4 | 0.678 | 137.1 ± 28.9 | 158.4 ± 23.0 | 0.643 |
| PNI | 47.1 ± 5.9 | 46.3 ± 6.8 | 0.661 | 48.9 ± 5.2 | 46.0 ± 5.7 | 0.073 |
| Treatment interval change (%) | ||||||
| ΔBW% ** | −5.3 ± 0.9 | −1.4 ± 1.1 | 0.019 * | −6.4 ± 1.2 | −0.2 ± 2.1 | 0.023 * |
| ΔBMI% ** | −4.9 ± 0.9 | −1.3 ± 1.2 | 0.040 * | −6.7 ± 1.2 | −0.4 ± 2.0 | 0.001 * |
| ΔHb% ** | −7.4 ± 2.2 | −9.7 ± 2.7 | 0.538 | −12.9 ± 2.0 | −7.2 ± 4.8 | 0.225 |
| ΔWBC% ** | −24.3 ± 4.6 | −15.5 ± 13.6 | 0.445 | −27.8 ± 6.2 | −13.0 ± 14.1 | 0.198 |
| ΔPlatelet% ** | −20.1 ± 4.4 | −21.9 ± 6.8 | 0.818 | −17.8 ± 6.1 | −29.3 ± 7.9 | 0.152 |
| ΔTLC% ** | −41.5 ± 4.9 | −33.7 ± 16.1 | 0.550 | −49.2 ± 5.5 | −63.2 ± 8.0 | 0.238 |
| ΔAlbumin% ** | 6.3 ± 2.7 | 7.6 ± 7.8 | 0.847 | 1.4 ± 2.8 | 1.9 ± 8.2 | 0.237 |
| ΔCRP% ** | 84.5 ± 10.8 | 98.0 ± 6.6 | 0.614 | 55.1 ± 22.3 | 80.5 ± 42.1 | 0.404 |
| ΔNLR% ** | 5.3 ± 2.5 | 3.4 ± 1.8 | 0.027 * | 4.8 ± 7.1 | 12.4 ± 23.6 | 0.292 |
| ΔPLR% ** | 113.9 ± 30.9 | 89.8 ± 33.1 | 0.684 | 137.1 ± 27.8 | 237.2 ± 78.8 | 0.185 |
| ΔPNI% ** | −4.8 ± 2.3 | −5.8 ± 3.3 | 0.807 | −9.9 ± 1.8 | −11.6 ± 4.5 | 0.692 |
| Body composition parameters | ||||||
| Before CCRT | ||||||
| LBM (kg) | 45.2 ± 5.1 | 40.4 ± 3.6 | <0.001 * | 44.8 ± 6.2 | 38.4 ± 7.2 | 0.004 * |
| TFM (kg) | 19.3 ± 9.1 | 11.8 ± 5.4 | 0.001 * | 17.4 ± 5.5 | 10.2 ± 4.8 | <0.001 * |
| ASM (kg) | 19.2 ± 2.9 | 16.6 ± 2.5 | 0.001 * | 19.6 ± 3.4 | 15.4 ± 3.8 | 0.001 * |
| Android (%) | 32.8 ± 12.9 | 22.3 ± 11.5 | 0.002 * | 32.7 ± 9.1 | 19.9 ± 9.6 | <0.001 * |
| Gynoid (%) | 27.4 ± 8.2 | 21.7 ± 7.2 | 0.007 * | 26.4 ± 9.7 | 19.4 ± 4.4 | <0.001 * |
| Treatment interval change (%) | ||||||
| ΔLBM% ** | −7.1 ± 5.8 | −3.9 ± 4.7 | 0.001 * | −5.7 ± 7.2 | −2.4 ± 4.0 | 0.021 * |
| ΔTFM% ** | −7.5 ± 13.9 | 8.1 ± 17.2 | <0.001 * | −8.9 ± 16.0 | 6.1 ± 6.3 | 0.015 * |
| ΔASM% ** | −8.4 ± 7.5 | −6.3 ± 8.0 | 0.280 | −8.7 ± 10.3 | −5.1 ± 7.1 | 0.276 |
| ΔAndroid% ** | −4.8 ± 19.2 | 11.9 ± 22.5 | 0.002 * | −7.8 ± 5.2 | 19.2 ± 12.8 | 0.005 * |
| ΔGynoid% ** | 2.6 ± 12.2 | 8.5 ± 18.7 | 0.126 | 1.0 ± 2.6 | 10.9 ± 8.5 | 0.109 |
| Mean daily calorie intake during CCRT | 25.2 ± 4.3 | 38.6 ± 7.0 | <0.001 * | 25.7 ± 3.8 | 36.6 ± 7.8 | <0.001 * |
| Mean protein intake during CCRT | 0.9 ± 0.9 | 1.3 ± 0.4 | 0.014 * | 0.8 ± 0.9 | 1.2 ± 0.8 | 0.021 * |
| Feeding tube placement (no/yes) | 18 (37.5): 30 (63.5) | 4 (19.0): 17 (81.0) | 0.130 | 21 (48.8): 22 (51.2) | 5 (45.5): 6 (54.5) | 0.841 |
| Mean days of feeding tube placement | 28.2 ± 4.1 | 48.8 ± 5.7 | 0.007 * | 20.6 ± 4.0 | 27.5 ± 9.5 | 0.451 |
| CCRT data | ||||||
| Radiotherapy | ||||||
| Dose (Gy) | 64.3 ± 4.5 | 64.3 ± 1.7 | 0.988 | 69.8 ± 2.9 | 69.7 ± 4.1 | 0.911 |
| Fractions | 31.8 ± 1.7 | 32.3 ± 1.6 | 0.299 | 33.3 ± 1.1 | 34.0 ± 2.3 | 0.164 |
| Duration (days) | 45.2 ± 5.4 | 47.7 ± 3.6 | 0.727 | 51.9 ± 8.5 | 50.3 ± 6.1 | 0.538 |
| Cisplatin dose (mg/m2) | 238.2 ± 23.3 | 239.1 ± 16.5 | 0.880 | 211.3 ± 10.2 | 220.9 ± 12.7 | 0.670 |
| Grade 3/4 toxicity during CCRT | ||||||
| Non-hematologic | ||||||
| Dermatitis (no/yes) | 46 (95.8): 2 (4.2) | 20 (95.2): 1 (4.8) | 0.911 | 41 (95.7): 2 (4.3) | 11 (100.0): 0 (0.0) | 0.466 |
| Pharyngitis (no/yes) | 45 (93.8): 3 (6.2) | 19 (90.5): 2 (9.5) | 0.629 | 36 (83.7): 7 (16.3) | 8 (72.8): 3 (27.2) | 0.402 |
| Infection (no/yes) | 42 (87.5): 6 (12.5) | 17 (81.0): 4 (19.0) | 0.477 | 32 (74.4): 11 (25.6) | 5 (45.5): 6 (54.5) | 0.065 |
| Mucositis (no/yes) | 35 (72.9): 13 (27.1) | 17 (81.0): 4 (19.0) | 0.476 | 32 (74.4): 11 (25.6) | 8 (72.8): 3 (27.2) | 0.909 |
| Emesis (no/yes) | 43 (89.6): 5 (10.4) | 20 (95.2): 1 (4.8) | 0.476 | 40 (93.0): 3 (7.0) | 10 (90.9): 1 (9.1) | 0.811 |
| Hematologic | ||||||
| Anemia (no/yes) | 44 (91.7): 4 (8.3) | 20 (95.2): 1 (4.8) | 0.599 | 37 (86.0): 6 (14.0) | 7 (90.9): 4 (9.1) | 0.668 |
| Neutropenia (no/yes) | 31 (64.6): 17 (35.4) | 15 (71.4): 6 (28.6) | 0.579 | 26 (60.5): 17 (39.5) | 8 (63.6): 4 (36.4) | 0.847 |
| Thrombocytopenia (no/yes) | 45 (93.8): 3 (6.2) | 20 (95.2): 1 (4.8) | 0.808 | 37 (86.0): 6 (14.0) | 10 (90.9): 1 (9.1) | 0.668 |
| 2-year mortality (%) | 18 (37.1) | 12 (57.1) | 0.045 * | 10 (23.3) | 6 (54.5) | 0.043 * |
| OCC with Postoperative Adjuvant CCRT | NOCC with Primary CCRT | |||||||
|---|---|---|---|---|---|---|---|---|
| Factor | Factor | |||||||
| Component | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 |
| BW | 0.766 | −0.103 | −0.092 | 0.614 | 0.834 | 0.500 | −0.195 | −0.054 |
| BMI | 0.804 | −0.115 | −0.082 | 0.508 | 0.656 | 0.656 | −0.268 | −0.016 |
| LBM | 0.265 | −0.110 | 0.102 | 0.931 | 0.965 | 0.127 | −0.193 | −0.007 |
| ASM | 0.287 | −0.121 | 0.867 | 0.897 | 0.956 | 0.180 | −0.175 | −0.048 |
| TFM | 0.930 | −0.084 | −0.337 | 0.302 | 0.514 | 0.827 | −0.162 | −0.056 |
| Android | 0.937 | −0.072 | −0.093 | 0.155 | 0.353 | 0.863 | −0.219 | −0.080 |
| Gynoid | 0.964 | −0.052 | −0.061 | −0.032 | 0.032 | 0.935 | −0.064 | −0.155 |
| ΔBW% | 0.005 | 0.460 | 0.732 | −0.348 | −0.185 | −0.267 | 0.790 | 0.390 |
| ΔBMI% | 0.043 | 0.400 | 0.717 | −0.341 | −0.134 | −0.305 | 0.794 | 0.362 |
| ΔLBM% | −0.072 | 0.031 | 0.923 | −0.046 | −0.223 | −0.062 | 0.886 | −0.239 |
| ΔASM% | −0.086 | 0.137 | 0.887 | 0.042 | −0.134 | −0.048 | 0.853 | −0.014 |
| ΔTFM% | −0.133 | 0.900 | 0.322 | −0.172 | −0.063 | −0.105 | 0.200 | 0.951 |
| ΔAndroid% | −0.193 | 0.895 | −0.150 | −0.081 | −0.089 | −0.125 | 0.182 | 0.907 |
| ΔGynoid% | 0.019 | 0.936 | −0.049 | 0.005 | 0.076 | −0.016 | −0.222 | 0.942 |
| Eigenvalue | 4.51 | 2.21 | 1.27 | 1.06 | 4.82 | 2.04 | 1.42 | 1.05 |
| % of accumulative variances | 45.1 | 67.2 | 79.9 | 90.5 | 48.2 | 68.6 | 82.8 | 93.8 |
| OCC with Postoperative Adjuvant CCRT | NOCC with Primary CCRT | |||||
|---|---|---|---|---|---|---|
| Variables | Univariate | Multivariate | Univariate | Multivariate | ||
| p-Value | HR (95% CI) | p-Value | p-Value | HR (95% CI) | p-Value | |
| Clinicopathologic | ||||||
| Sex (ref: female) | 0.979 | 0.860 | ||||
| Age | 0.949 | 0.014 * | 1.088 (1.019~1.093) | 0.012 * | ||
| TNM stage (ref: IV) | 0.982 | 0.211 | ||||
| T status (ref: T3-4) | 0.347 | 0.166 | ||||
| N status (ref: N2-3) | 0.161 | 0.156 | ||||
| Histologic grade (ref: poorly differentiated) | 0.019 * | 0.810 | ||||
| ECOG performance status (ref: 2) | 0.012 * | 0.180 (0.038~0.842) | 0.006 * | 0.333 | ||
| Smoking (ref: yes) | 0.645 | 0.487 | ||||
| Alcohol (ref: yes) | 0.053 | 0.440 | ||||
| Betel nut (ref: yes) | 0.264 | 0.996 | ||||
| HN-CCI (ref: no) | 0.047 * | 0.255 | ||||
| Tracheostomy (ref: yes) | 0.732 | 0.055 | ||||
| CCRT | ||||||
| RT dose (Gy) | 0.446 | 0.222 | ||||
| RT fractions | 0.255 | 0.411 | ||||
| RT duration (days) | 0.140 | 0.101 | ||||
| Cisplatin dose | 0.774 | 0.458 | ||||
| CCRT-induced grade 3/4 toxicity | ||||||
| Dermatitis (ref: yes) | 0.037 * | 0.746 | ||||
| Pharyngitis (ref: yes) | 0.012 * | 0.237 | ||||
| Mucositis (ref: yes) | 0.958 | 0.885 | ||||
| Infection (ref: yes) | 0.394 | 0.027 * | ||||
| Emesis (ref: yes) | 0.218 | 0.469 | ||||
| Anemia (ref: yes) | 0.970 | 0.211 | ||||
| Neutropenia (ref: yes) | 0.855 | 0.969 | ||||
| Thrombocytopenia (ref: yes) | 0.306 | 0.555 | ||||
| Mean daily calorie intake during CCRT (ref: ≥30) | 0.045 * | 0.039 * | ||||
| Mean protein intake during CCRT | 0.269 | 0.478 | ||||
| Feeding tube placement (ref: yes) | 0.039 * | 0.052 | ||||
| Mean days of feeding tube placement during CCRT | 0.001 * | 0.022 * | ||||
| Nutritional and inflammatory markers | ||||||
| Before CCRT | ||||||
| BMI (kg/m2) | 0.005 * | 0.011 * | ||||
| BW (kg) | 0.004 * | 0.008 * | ||||
| Hb (g/dL) | 0.128 | 0.098 | ||||
| WBC (×103 cells/mm3) | 0.061 | 0.621 | ||||
| Platelet count (×103/mm3) | 0.024 * | 0.564 | ||||
| TLC (×103 cells/mm3) | 0.133 | 0.101 | ||||
| Albumin (g/dL) | 0.191 | 0.056 | ||||
| CRP (mg/dL) | 0.038 * | 0.541 | ||||
| NLR | 0.179 | 0.023 * | 1.250 (1.014~1.311) | 0.027 * | ||
| PLR | <0.001 * | 1.004 (1.002~1.005) | <0.001 * | 0.111 | ||
| PNI | 0.022 * | 0.009 * | ||||
| Treatment interval changes (%) | ||||||
| ΔBW% ** | 0.035 * | 0.502 | ||||
| ΔBMI% ** | 0.121 | 0.440 | ||||
| ΔHb% ** | 0.544 | 0.052 | ||||
| ΔWBC% ** | 0.818 | 0.008 * | ||||
| ΔPlatelet% ** | 0.041 * | 0.543 | ||||
| ΔTLC% ** | 0.481 | 0.798 | ||||
| ΔAlbumin% ** | 0.346 | 0.410 | ||||
| ΔCRP% ** | 0.046 * | 0.055 | ||||
| ΔNLR% ** | 0.009 * | 0.048 * | ||||
| ΔPLR% ** | 0.733 | 0.122 | ||||
| ΔPNI% ** | 0.419 | 0.869 | ||||
| PG-SGA before CCRT (ref: stage C) | 0.007 * | 0.098 | ||||
| Body composition parameters | ||||||
| Factor 1 | 0.023 * | 0.430 | ||||
| Factor 2 | 0.871 | 0.008 * | 0.477 (0.020~0.777) | 0.008 * | ||
| Factor 3 | 0.003 * | 1.562 (1.094~2.229) | 0.014 * | 0.054 | ||
| Factor 4 | 0.098 | 0.358 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-C.; Wang, C.-H.; Ling, H.H.; Pan, Y.-P.; Chang, P.-H.; Chou, W.-C.; Chen, F.-P.; Yeh, K.-Y. Inflammation Status and Body Composition Predict Two-Year Mortality of Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma under Provision of Recommended Energy Intake during Concurrent Chemoradiotherapy. Biomedicines 2022, 10, 388. https://doi.org/10.3390/biomedicines10020388
Lin Y-C, Wang C-H, Ling HH, Pan Y-P, Chang P-H, Chou W-C, Chen F-P, Yeh K-Y. Inflammation Status and Body Composition Predict Two-Year Mortality of Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma under Provision of Recommended Energy Intake during Concurrent Chemoradiotherapy. Biomedicines. 2022; 10(2):388. https://doi.org/10.3390/biomedicines10020388
Chicago/Turabian StyleLin, Yu-Ching, Cheng-Hsu Wang, Hang Huong Ling, Yi-Ping Pan, Pei-Hung Chang, Wen-Chi Chou, Fang-Ping Chen, and Kun-Yun Yeh. 2022. "Inflammation Status and Body Composition Predict Two-Year Mortality of Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma under Provision of Recommended Energy Intake during Concurrent Chemoradiotherapy" Biomedicines 10, no. 2: 388. https://doi.org/10.3390/biomedicines10020388
APA StyleLin, Y.-C., Wang, C.-H., Ling, H. H., Pan, Y.-P., Chang, P.-H., Chou, W.-C., Chen, F.-P., & Yeh, K.-Y. (2022). Inflammation Status and Body Composition Predict Two-Year Mortality of Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma under Provision of Recommended Energy Intake during Concurrent Chemoradiotherapy. Biomedicines, 10(2), 388. https://doi.org/10.3390/biomedicines10020388