
Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database

 , , , , , ,
, , , , , ,  ,
,  , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Data and Samples Collection
2.3. Mortality and Organ Damage
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
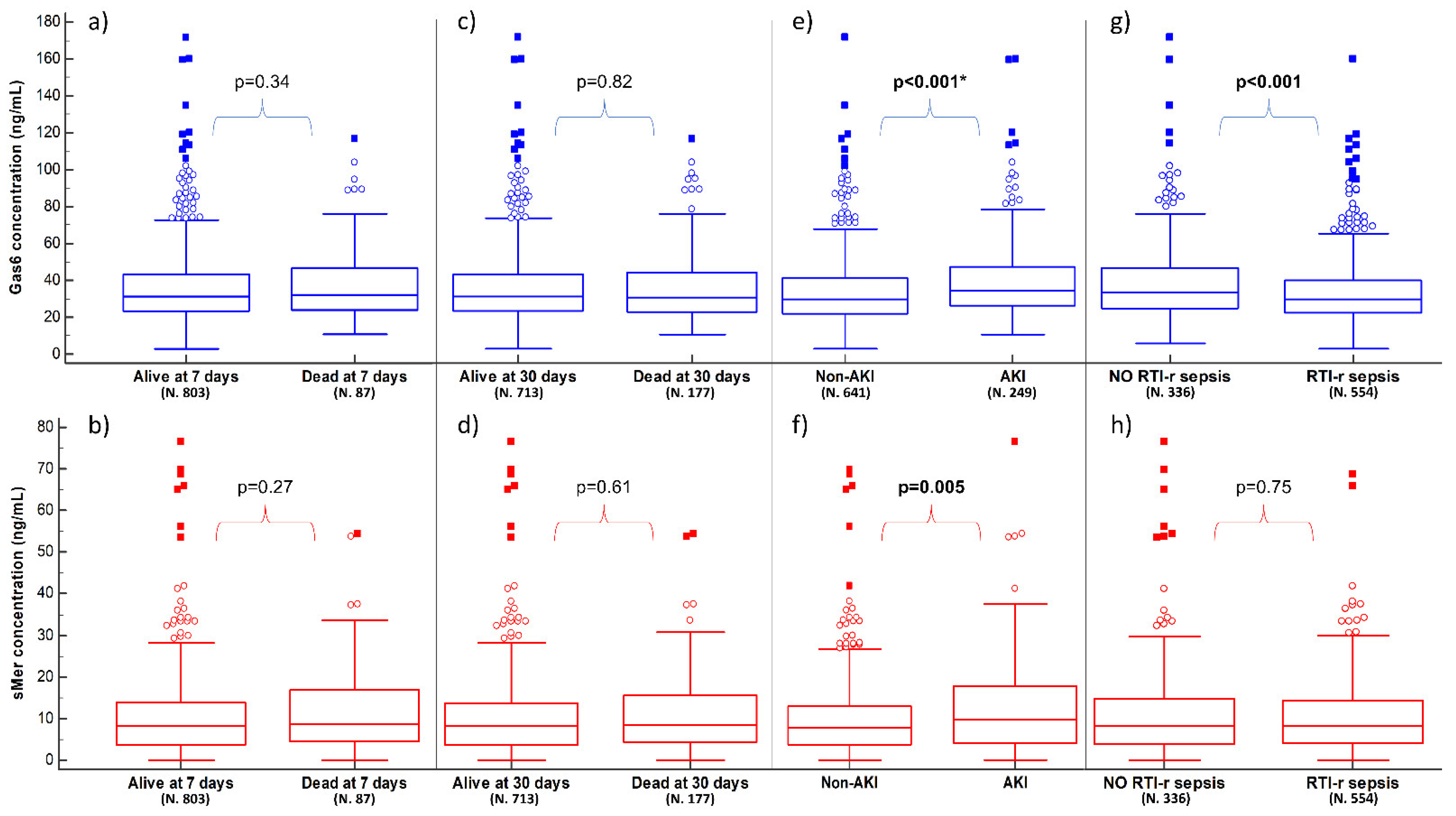
3.2. Mortality
3.3. Acute Kidney Injury
3.4. Sepsis Related to Respiratory Tract Infection
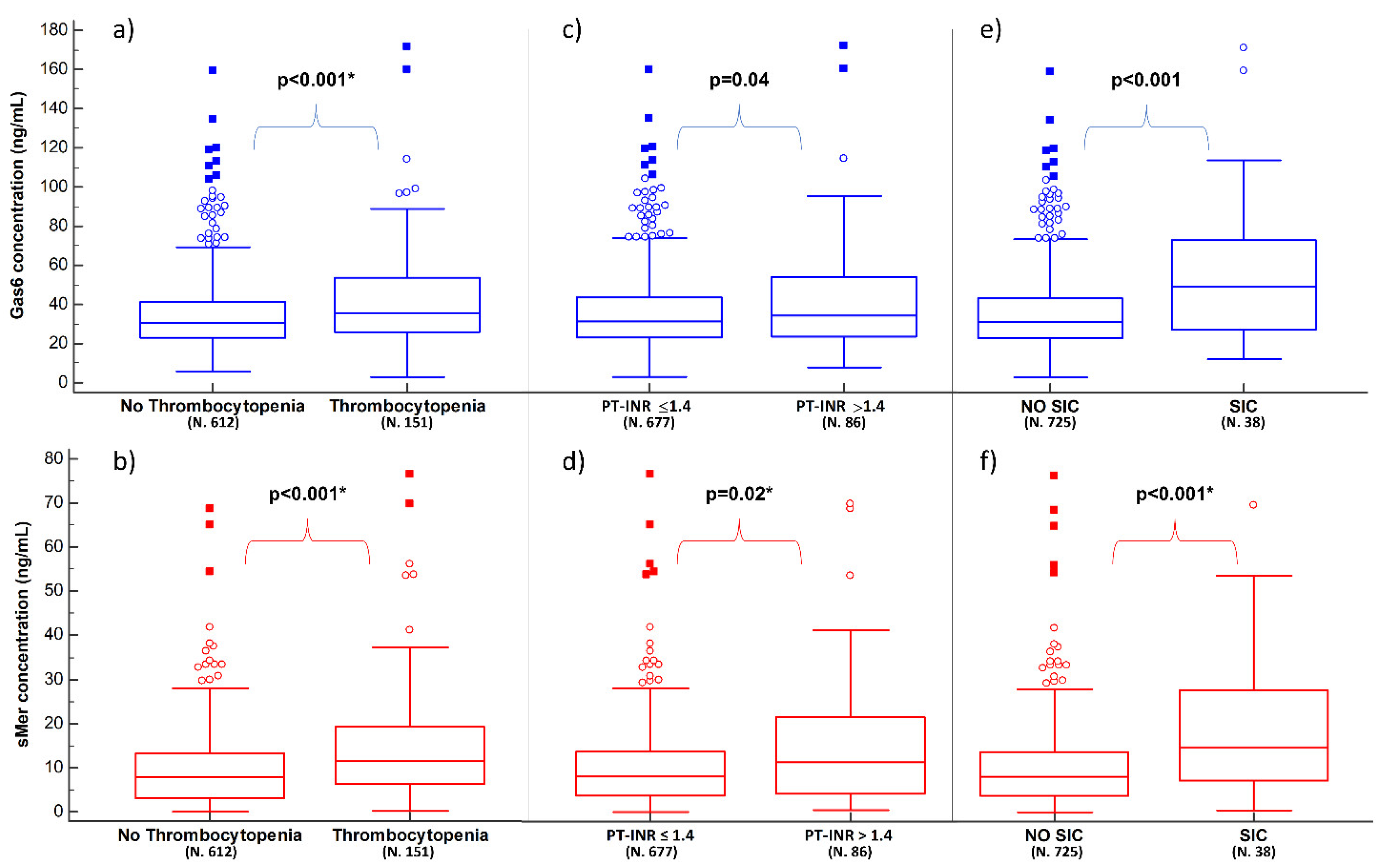
3.5. Coaguopathy
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Escher, M.; Ricou, B.; Nendaz, M.; Scherer, F.; Cullati, S.; Hudelson, P.; Perneger, T. ICU physicians’ and internists’ survival predictions for patients evaluated for admission to the intensive care unit. Ann. Intensive Care 2018, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Guia, M.C.; Vallecoccia, M.S.; Suarez, D.; Ibarz, M.; Irazabal, M.; Ferrer, R.; Artigas, A. Risk factors for mortality in elderly and very elderly critically ill patients with sepsis: A prospective, observational, multicenter cohort study. Ann. Intensive Care 2019, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Ljungstrom, L.; Pernestig, A.K.; Jacobsson, G.; Andersson, R.; Usener, B.; Tilevik, D. Diagnostic accuracy of procalcitonin, neutrophil-lymphocyte count ratio, C-reactive protein, and lactate in patients with suspected bacterial sepsis. PLoS ONE 2017, 12, e0181704. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Lu, Y.; Jiang, H.; Zhang, L. The diagnostic accuracy of procalcitonin and C-reactive protein for sepsis: A systematic review and meta-analysis. J. Cell. Biochem. 2019, 120, 5852–5859. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef]
- Okorie, O.N.; Dellinger, P. Lactate: Biomarker and potential therapeutic target. Crit. Care Clin. 2011, 27, 299–326. [Google Scholar] [CrossRef]
- Gillespie, Í.; Rosenstein, P.G.; Hughes, D. Update: Clinical Use of Plasma Lactate. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 325–342. [Google Scholar] [CrossRef]
- Masyuk, M.; Wernly, B.; Lichtenauer, M.; Franz, M.; Kabisch, B.; Muessig, J.M.; Zimmermann, G.; Lauten, A.; Schulze, P.C.; Hoppe, U.C.; et al. Prognostic relevance of serum lactate kinetics in critically ill patients. Intensive Care Med. 2019, 45, 55–61. [Google Scholar] [CrossRef]
- Vincent, J.L.; Quintairos, E.; Silva, A.; Couto, L.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: A systematic review. Crit. Care 2016, 20, 257. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, G.; Bellomo, R.; Bakker, J. The ten pitfalls of lactate clearance in sepsis. Intensive Care Med. 2019, 45, 82–85. [Google Scholar] [CrossRef] [Green Version]
- Alegría, L.; Vera, M.; Dreyse, J.; Castro, R.; Carpio, D.; Henriquez, C.; Gajardo, D.; Bravo, S.; Araneda, F.; Kattan, E.; et al. A hypoperfusion context may aid to interpret hyperlactatemia in sepsis-3 septic shock patients: A proof-of-concept study. Ann. Intensive Care 2017, 7, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Hur, M.; Moon, H.W.; Yun, Y.M.; Di Somma, S.; Network, G. Multi-marker approach using procalcitonin, presepsin, galectin-3, and soluble suppression of tumorigenicity 2 for the prediction of mortality in sepsis. Ann. Intensive Care 2017, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Castello, L.M.; Baldrighi, M.; Molinari, L.; Salmi, L.; Cantaluppi, V.; Vaschetto, R.; Zunino, G.; Quaglia, M.; Bellan, M.; Gavelli, F.; et al. The Role of Osteopontin as a Diagnostic and Prognostic Biomarker in Sepsis and Septic Shock. Cells 2019, 8, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mebazaa, A.; Geven, C.; Hollinger, A.; Wittebole, X.; Chousterman, B.G.; Blet, A.; Gayat, E.; Hartmann, O.; Scigalla, P.; Struck, J.; et al. Circulating adrenomedullin estimates survival and reversibility of organ failure in sepsis: The prospective observational multinational Adrenomedullin and Outcome in Sepsis and Septic Shock-1 (AdrenOSS-1) study. Crit. Care 2018, 22, 354. [Google Scholar] [CrossRef] [Green Version]
- Mearelli, F.; Fiotti, N.; Giansante, C.; Casarsa, C.; Orso, D.; De Helmersen, M.; Altamura, N.; Ruscio, M.; Castello, L.M.; Colonetti, E.; et al. Derivation and Validation of a Biomarker-Based Clinical Algorithm to Rule Out Sepsis From Noninfectious Systemic Inflammatory Response Syndrome at Emergency Department Admission: A Multicenter Prospective Study. Crit. Care Med. 2018, 46, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.F.; Wu, C.C.; Liu, S.H.; Chen, K.F. Comparison of the accuracy of neutrophil CD64, procalcitonin, and C-reactive protein for sepsis identification: A systematic review and meta-analysis. Ann. Intensive Care 2019, 9, 5. [Google Scholar] [CrossRef]
- Salmi, L.; Gavelli, F.; Patrucco, F.; Caputo, M.; Avanzi, G.C.; Castello, L.M. Gas6/TAM Axis in Sepsis: Time to Consider Its Potential Role as a Therapeutic Target. Dis. Markers 2019, 2019, 6156493. [Google Scholar] [CrossRef]
- Guignant, C.; Venet, F.; Planel, S.; Demaret, J.; Gouel-Chéron, A.; Nougier, C.; Friggeri, A.; Allaouchiche, B.; Lepape, A.; Monneret, G. Increased MerTK expression in circulating innate immune cells of patients with septic shock. Intensive Care Med. 2013, 39, 1556–1564. [Google Scholar] [CrossRef]
- Stalder, G.; Que, Y.A.; Calzavarini, S.; Burnier, L.; Kosinski, C.; Ballabeni, P.; Roger, T.; Calandra, T.; Duchosal, M.A.; Liaudet, L.; et al. Study of Early Elevated Gas6 Plasma Level as a Predictor of Mortality in a Prospective Cohort of Patients with Sepsis. PLoS ONE 2016, 11, e0163542. [Google Scholar] [CrossRef] [Green Version]
- Ekman, C.; Linder, A.; Akesson, P.; Dahlbäck, B. Plasma concentrations of Gas6 (growth arrest specific protein 6) and its soluble tyrosine kinase receptor sAxl in sepsis and systemic inflammatory response syndromes. Crit. Care 2010, 14, R158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, L.C.; Huang, P.W.; Hsieh, K.H.; Wang, C.H.; Kao, Y.K.; Lin, T.H.; Lee, X.L. Elevated Plasma Levels of Gas6 Are Associated with Acute Lung Injury in Patients with Severe Sepsis. Tohoku J. Exp. Med. 2017, 243, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G.; et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef]
- Castello, L.M.; Gavelli, F.; Baldrighi, M.; Salmi, L.; Mearelli, F.; Fiotti, N.; Patrucco, F.; Bellan, M.; Sainaghi, P.P.; Ronzoni, G.; et al. Hypernatremia and moderate-to-severe hyponatremia are independent predictors of mortality in septic patients at emergency department presentation: A sub-group analysis of the need-speed trial. Eur. J. Intern. Med. 2021, 83, 21–27. [Google Scholar] [CrossRef]
- Alciato, F.; Sainaghi, P.P.; Castello, L.; Bergamasco, L.; Carnieletto, S.; Avanzi, G.C. Development and validation of an ELISA method for detection of growth arrest specific 6 (GAS6) protein in human plasma. J. Immunoass. Immunochem. 2008, 29, 167–180. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Le Gall, J.-R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, J.H.; van der Poll, T.; van’t Veer, C. TAM receptors, Gas6, and protein S: Roles in inflammation and hemostasis. Blood 2014, 123, 2460–2469. [Google Scholar] [CrossRef] [PubMed]
- Thorp, E.; Vaisar, T.; Subramanian, M.; Mautner, L.; Blobel, C.; Tabas, I. Shedding of the Mer tyrosine kinase receptor is mediated by ADAM17 protein through a pathway involving reactive oxygen species, protein kinase Cδ, and p38 mitogen-activated protein kinase (MAPK). J. Biol. Chem. 2011, 286, 33335–33344. [Google Scholar] [CrossRef] [Green Version]
- Manfioletti, G.; Brancolini, C.; Avanzi, G.; Schneider, C. The protein encoded by a growth arrest-specific gene (gas6) is a new member of the vitamin K-dependent proteins related to protein S, a negative coregulator in the blood coagulation cascade. Mol. Cell Biol. 1993, 13, 4976–4985. [Google Scholar]
- Avanzi, G.C.; Gallicchio, M.; Cavalloni, G.; Gammaitoni, L.; Leone, F.; Rosina, A.; Boldorini, R.; Monga, G.; Pegoraro, L.; Varnum, B.; et al. GAS6, the ligand of Axl and Rse receptors, is expressed in hematopoietic tissue but lacks mitogenic activity. Exp. Hematol. 1997, 25, 1219–1226. [Google Scholar] [PubMed]
- Gould, W.R.; Baxi, S.M.; Schroeder, R.; Peng, Y.W.; Leadley, R.J.; Peterson, J.T.; Perrin, L.A. Gas6 receptors Axl, Sky and Mer enhance platelet activation and regulate thrombotic responses. J. Thromb. Haemost. 2005, 3, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Levi, M.; Toh, C.H. Disseminated intravascular coagulation. Nat. Rev. Dis. Primers 2016, 2, 16037. [Google Scholar] [CrossRef] [PubMed]
- Dhainaut, J.F.; Yan, S.B.; Joyce, D.E.; Pettila, V.; Basson, B.; Brandt, J.T.; Sundin, D.P.; Levi, M. Treatment effects of drotrecogin alfa (activated) in patients with severe sepsis with or without overt disseminated intravascular coagulation. J. Thromb. Haemost. 2004, 2, 1924–1933. [Google Scholar] [CrossRef]
- Iba, T.; Nisio, M.D.; Levy, J.H.; Kitamura, N.; Thachil, J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: A retrospective analysis of a nationwide survey. BMJ Open 2017, 7, e017046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, C.W.; Kennedy, J.N.; Wang, S.; Chang, C.H.; Elliott, C.F.; Xu, Z.; Berry, S.; Clermont, G.; Cooper, G.; Gomez, H.; et al. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis. JAMA 2019, 321, 2003–2017. [Google Scholar] [CrossRef]
- Gomez, H.; Kellum, J.A. Sepsis-induced acute kidney injury. Curr. Opin. Crit. Care 2016, 22, 546–553. [Google Scholar] [CrossRef] [Green Version]
- Ochodnicky, P.; Lattenist, L.; Ahdi, M.; Kers, J.; Uil, M.; Claessen, N.; Leemans, J.C.; Florquin, S.; Meijers, J.C.M.; Gerdes, V.E.A.; et al. Increased Circulating and Urinary Levels of Soluble TAM Receptors in Diabetic Nephropathy. Am. J. Pathol. 2017, 187, 1971–1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurata, A.; Tachibana, Y.; Takahashi, T.; Horiba, N. Novel AXL-specific inhibitor ameliorates kidney dysfunction through the inhibition of epithelial-to-mesenchymal transition of renal tubular cells. PLoS ONE 2020, 15, e0232055. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef] [Green Version]
- Kashani, K.; Rosner, M.H.; Ostermann, M. Creatinine: From physiology to clinical application. Eur. J. Intern. Med. 2020, 72, 9–14. [Google Scholar] [CrossRef]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers From the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw. Open 2020, 3, e2019209. [Google Scholar] [CrossRef]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef] [Green Version]
- Gocze, I.; Jauch, D.; Gotz, M.; Kennedy, P.; Jung, B.; Zeman, F.; Gnewuch, C.; Graf, B.M.; Gnann, W.; Banas, B.; et al. Biomarker-guided Intervention to Prevent Acute Kidney Injury After Major Surgery: The Prospective Randomized BigpAK Study. Ann. Surg. 2018, 267, 1013–1020. [Google Scholar] [CrossRef]
- Molinari, L.; Heskia, F.; Peerapornratana, S.; Ronco, C.; Guzzi, L.; Toback, S.; Birch, R.; Beyhaghi, H.; Kwan, T.; Kampf, J.P.; et al. Limiting Acute Kidney Injury Progression In Sepsis: Study Protocol and Trial Simulation. Crit. Care Med. 2021, 49, 1706. [Google Scholar] [CrossRef]
- Sainaghi, P.P.; Alciato, F.; Carnieletto, S.; Castello, L.; Bergamasco, L.; Sola, D.; Bongo, A.S.; Inglese, E.; Polosa, R.; Avanzi, G.C. Gas6 evaluation in patients with acute dyspnea due to suspected pulmonary embolism. Respir. Med. 2009, 103, 589–594. [Google Scholar] [CrossRef] [Green Version]
- Giangola, M.D.; Yang, W.L.; Rajayer, S.R.; Nicastro, J.; Coppa, G.F.; Wang, P. Growth arrest-specific protein 6 attenuates neutrophil migration and acute lung injury in sepsis. Shock 2013, 40, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Alciato, F.; Sainaghi, P.P.; Sola, D.; Castello, L.; Avanzi, G.C. TNF-alpha, IL-6, and IL-1 expression is inhibited by GAS6 in monocytes/macrophages. J. Leukoc. Biol. 2010, 87, 869–875. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| General Characteristics | |
| Age (years) | 80 (72–87) |
| Sex, male/female | 477 (54%)/413 (46%) |
| Body mass index | 24.2 (21.7–27.3) |
| Comorbidities | |
| Arterial hypertension | 399 (45%) |
| Cardiovascular disease | 479 (54%) |
| Chronic obstructive pulmonary disease | 231 (26%) |
| Chronic kidney disease | 202 (23%) |
| Diabetes | 243 (27%) |
| Clinical parameters | |
| Systolic blood pressure (mmHg) | 120 (110–137) |
| Diastolic blood pressure (mmHg) | 70 (60–80) |
| Mean arterial pressure (mmHg) | 87 (77–97) |
| Heart rate (bpm) | 100 (90–110) |
| Respiratory rate (bpm) | 24 (20–28) |
| Pulse oxygen saturation (%) | 94 (92–96) |
| Glasgow coma scale | 15 (15–15) |
| Temperature (°C) | 37.7 (36.6–38.2) |
| Laboratory data | |
| White blood cells (×103/mm3) | 12.9 (9.3–17.0) |
| Hemoglobin (g/dL) | 12.2 (10.8–13.5) |
| Platelets (×103/mm3) | 221 (157–300) |
| Glucose (mg/dL) | 131 (109–167) |
| Creatinine (mg/dL) | 1.08 (0.83–1.67) |
| Total bilirubin (mg/dL) | 0.91 (0.66–1.43) |
| PT-INR | 1.19 (1.10–1.36) |
| aPTT (seconds) | 30 (28–34) |
| C-reactive protein (mg/dL) | 10.11 (3.42–18.62) |
| Lactate (mmol/L) | 1.54 (1.09–2.22) |
| PaO2/FiO2 | 286 (230–346) |
| Biomarkers | |
| Gas6 (ng/mL) | 31.1 (23.2–43.5) |
| sMer (ng/mL) | 8.3 (4.0–14.4) |
| Scores | |
| SOFA | 3 (1–4) |
| APACHE II | 13 (10–16) |
| SAPS II | 36 (30–42) |
| Mortality | |
| 7-day | 87 (9.7%) |
| 30-day | 177 (19.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavelli, F.; Molinari, L.; Baldrighi, M.; Salmi, L.; Mearelli, F.; Fiotti, N.; Patrucco, F.; Airoldi, C.; Bellan, M.; Sainaghi, P.P.; et al. Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database. Biomedicines 2022, 10, 198. https://doi.org/10.3390/biomedicines10020198
Gavelli F, Molinari L, Baldrighi M, Salmi L, Mearelli F, Fiotti N, Patrucco F, Airoldi C, Bellan M, Sainaghi PP, et al. Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database. Biomedicines. 2022; 10(2):198. https://doi.org/10.3390/biomedicines10020198
Chicago/Turabian StyleGavelli, Francesco, Luca Molinari, Marco Baldrighi, Livia Salmi, Filippo Mearelli, Nicola Fiotti, Filippo Patrucco, Chiara Airoldi, Mattia Bellan, Pier Paolo Sainaghi, and et al. 2022. "Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database" Biomedicines 10, no. 2: 198. https://doi.org/10.3390/biomedicines10020198
APA StyleGavelli, F., Molinari, L., Baldrighi, M., Salmi, L., Mearelli, F., Fiotti, N., Patrucco, F., Airoldi, C., Bellan, M., Sainaghi, P. P., Di Somma, S., Lupia, E., Colonetti, E., Muiesan, M. L., Biolo, G., Avanzi, G. C., & Castello, L. M. (2022). Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database. Biomedicines, 10(2), 198. https://doi.org/10.3390/biomedicines10020198