
How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment
Abstract
1. Introduction
Purpose of the Present Study
2. Materials and Methods
3. Results
3.1. Treatment Effects on SBP
3.2. Treatment Effects on Cardiac Hypertrophy
3.2.1. Heart Weight
3.2.2. ANP mRNA
3.3. Treatment Effects on Cardiac Remodeling and Fibrosis
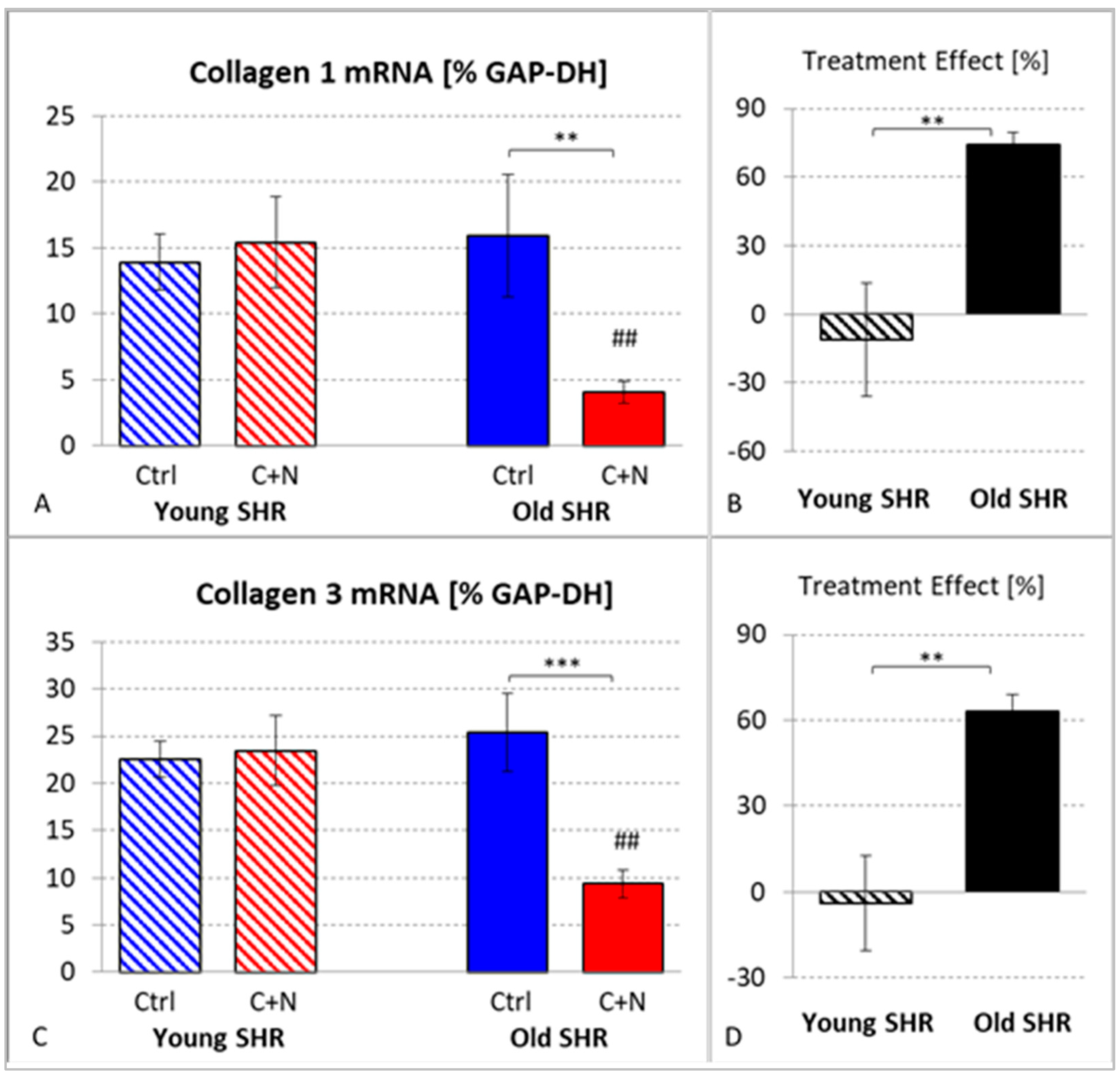
3.3.1. mRNA Expression of Collagens I and III
3.3.2. Fibrosis
4. Discussion
4.1. Effects on SBP
4.2. Cardioprotective Effects
4.2.1. Effects on Cardiac Hypertrophy and Remodeling in Young SHRs
4.2.2. Effects on Cardiac Hypertrophy and Remodeling in Old SHRs
4.2.3. Early-Onset versus Late-Onset Treatment
4.2.4. Applications to Antihypertensive Treatment in Humans
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | angiotensin-converting enzyme |
| ANP | atrial natriuretic peptide |
| BP | blood pressure |
| BW | body weight |
| C+N | captopril + nifedipine |
| CCB | calcium channel blocker |
| Coll 1 | collagen type I |
| Coll 3 | collagen type III |
| Ctrl | control |
| GAP-DH | glyceraldehyde-3-phosphate dehydrogenase |
| HW | heart weight |
| LV | left ventricle/left ventricular |
| LVW | left ventricular weight |
| o | old rats (aged 60–82 weeks) |
| RAS | renin-angiotensin system |
| SBP | systolic blood pressure |
| SHR | spontaneously hypertensive rats |
| TPR | total peripheral resistance |
| WKY | Wistar–Kyoto rats |
| y | young rats (aged 7–10 weeks) |
References
- Mazur, I.; Belenichev, I.; Kucherenko, L.; Bukhtiyarova, N.; Puzyrenko, A.; Khromylova, O.; Bidnenko, O.; Gorchakova, N. Antihypertensive and cardioprotective effects of new compound 1-(b-phenylethyl)-4-amino-1,2,4-triazolium bromide (Hypertril). Eur. J. Pharmacol. 2019, 853, 336–344. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Blood pressure is the most important cause of death and disability in the world. Eur. Heart J. Suppl. 2007, 9, B23–B28. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Briasoulis, A.; Agarwal, V.; Tousoulis, D.; Stefanadis, C. Effects of antihypertensive treatment in patients over 65 years of age: A meta-analysis of randomised controlled studies. Heart 2014, 100, 317–323. [Google Scholar] [CrossRef]
- Tiffe, T.; Wagner, M.; Rücker, V.; Morbach, C.; Gelbrich, G.; Störk, S.; Heuschmann, P.U. Control of cardiovascular risk factors and its determinants in the general population-findings from the STAAB cohort study. BMC Cardiovasc. Disord. 2017, 17, 276. [Google Scholar] [CrossRef]
- Volpe, M.; Gallo, G.; Tocci, G. Is early and fast blood pressure control important in hypertension management? Int. J. Cardiol. 2018, 254, 328–332. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Raja, W.; Ayub, T.; Jeelani, A.; Khan, S.M.S. Adherence to antihypertensive therapy and its determinants among patients attending primary care hospitals of Kashmir, India. J. Family Med. Prim. Care 2021, 10, 4153–4159. [Google Scholar] [CrossRef]
- Hinton, T.C.; Adams, Z.H.; Baker, R.P.; Hope, K.A.; Paton, J.F.R.; Hart, E.C.; Nightingale, A.K. Investigation and Treatment of High Blood Pressure in Young People: Too Much Medicine or Appropriate Risk Reduction? Hypertension 2020, 75, 16–22. [Google Scholar] [CrossRef]
- Yano, Y.; Reis, J.P.; Colangelo, L.A.; Shimbo, D.; Viera, A.J.; Allen, N.B.; Gidding, S.S.; Bress, A.P.; Greenland, P.; Muntner, P.; et al. Association of Blood Pressure Classification in Young Adults Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline With Cardiovascular Events Later in Life. JAMA 2018, 320, 1774–1782. [Google Scholar] [CrossRef]
- Moreira, L.B.; Fuchs, S.C.; Wiehe, M.; Gus, M.; Moraes, R.S.; Fuchs, F.D. Incidence of hypertension in Porto Alegre, Brazil: A population-based study. J. Hum. Hypertens. 2008, 22, 48–50. [Google Scholar] [CrossRef]
- Gooding, H.C.; McGinty, S.; Richmond, T.K.; Gillman, M.W.; Field, A.E. Hypertension awareness and control among young adults in the national longitudinal study of adolescent health. J. Gen. Intern. Med. 2014, 29, 1098–1104. [Google Scholar] [CrossRef]
- Drukteinis, J.S.; Roman, M.J.; Fabsitz, R.R.; Lee, E.T.; Best, L.G.; Russell, M.; Devereux, R.B. Cardiac and systemic hemodynamic characteristics of hypertension and prehypertension in adolescents and young adults: The Strong Heart Study. Circulation 2007, 115, 221–227. [Google Scholar] [CrossRef]
- Sundström, J.; Neovius, M.; Tynelius, P.; Rasmussen, F. Association of blood pressure in late adolescence with subsequent mortality: Cohort study of Swedish male conscripts. BMJ 2011, 342, d643. [Google Scholar] [CrossRef]
- Yano, Y.; Stamler, J.; Garside, D.B.; Daviglus, M.L.; Franklin, S.S.; Carnethon, M.R.; Liu, K.; Greenland, P.; Lloyd-Jones, D.M. Isolated systolic hypertension in young and middle-aged adults and 31-year risk for cardiovascular mortality: The Chicago Heart Association Detection Project in Industry study. J. Am. Coll. Cardiol. 2015, 65, 327–335. [Google Scholar] [CrossRef]
- SPRINT Research Group; Wright, J.T., Jr.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Volpe, M.; Citoni, B.; Coluccia, R.; Battistoni, A.; Tocci, G. Hypertension Across the Atlantic: A Sprint or a Marathon? High Blood Press. Cardiovasc. Prev. 2017, 24, 99–102. [Google Scholar] [CrossRef]
- SPRINT Research Group; Lewis, C.E.; Fine, L.J.; Beddhu, S.; Cheung, A.K.; Cushman, W.C.; Cutler, J.A.; Evans, G.W.; Johnson, K.C.; Kitzman, D.W.; et al. Final Report of a Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2021, 384, 1921–1930. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef] [PubMed]
- Al-Makki, A.; DiPette, D.; Whelton, P.K.; Murad, M.H.; Mustafa, R.A.; Acharya, S.; Beheiry, H.M.; Champagne, B.; Connell, K.; Cooney, M.T.; et al. Hypertension Pharmacological Treatment in Adults: A World Health Organization Guideline Executive Summary. Hypertension 2022, 79, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Volpe, M.; Gallo, G. To whom recommend intensive treatment for hypertension? Eur. Heart J. Suppl. 2020, 22, E167–E172. [Google Scholar] [CrossRef]
- Demirci, B.; McKeown, P.P.; Bayraktutan, U. Blockade of angiotensin II provides additional benefits in hypertension- and ageing-related cardiac and vascular dysfunctions beyond its blood pressure-lowering effects. J. Hypertens. 2005, 23, 2219–2227. [Google Scholar] [CrossRef] [PubMed]
- Zicha, J.; Dobesova, Z.; Kunes, J. Late blood pressure reduction in SHR subjected to transient captopril treatment in youth: Possible mechanisms. Physiol. Res. 2008, 57, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Hawlitschek, C.; Brendel, J.; Gabriel, P.; Schierle, K.; Salameh, A.; Zimmer, H.G.; Rassler, B. Antihypertensive and cardioprotective effects of different monotherapies and combination therapies in young spontaneously hypertensive rats: A pilot study. Saudi J. Biol. Sci. 2022, 29, 339–345. [Google Scholar] [CrossRef]
- Hawlitschek, C.; Brendel, J.; Gabriel, P.; Schierle, K.; Salameh, A.; Zimmer, H.G.; Rassler, B. How Effective Is a Late-Onset Antihypertensive Treatment? Studies with Captopril as Monotherapy and in Combination with Nifedipine in Old Spontaneously Hypertensive Rats. Biomedicines 2022, 10, 1964. [Google Scholar] [CrossRef]
- Paulis, L.; Líšková, S.; Pintérová, M.; Dobešová, Z.; Kuneš, J.; Zicha, J. Nifedipine-sensitive noradrenergic vasoconstriction is enhanced in spontaneously hypertensive rats: The influence of chronic captopril treatment. Acta Physiol. 2007, 191, 255–266. [Google Scholar] [CrossRef]
- Hale, T.M.; Robertson, S.J.; Burns, K.D.; deBlois, D. Short-term ACE inhibition confers long-term protection against target organ damage. Hypertens. Res. 2012, 35, 604–610. [Google Scholar] [CrossRef]
- Harrap, S.B.; Van der Merwe, W.M.; Griffin, S.A.; Macpherson, F.; Lever, A.F. Brief angiotensin converting enzyme inhibitor treatment in young spontaneously hypertensive rats reduces blood pressure long-term. Hypertension 1990, 16, 603–614. [Google Scholar] [CrossRef]
- Kost, C.K.; Li, P.; Jackson, E.K. Blood Pressure After Captopril Withdrawal From Spontaneously Hypertensive Rats. Hypertension 1995, 25, 82–87. [Google Scholar] [CrossRef]
- Zicha, J.; Dobešová, Z.; Behuliak, M.; Pintérová, M.; Kuneš, J.; Vaněčková, I. Nifedipine-sensitive blood pressure component in hypertensive models characterized by high activity of either sympathetic nervous system or renin-angiotensin system. Physiol. Res. 2014, 63, 13–26. [Google Scholar] [CrossRef]
- Zicha, J.; Kunes, J. Ontogenetic aspects of hypertension development: Analysis in the rat. Physiol. Rev. 1999, 79, 1227–1282. [Google Scholar] [CrossRef]
- Lemay, J.; Tea, B.S.; Hamet, P.; deBlois, D. Regression of neointimal lesions in the carotid artery of nifedipine-treated SHR and WKY rats: Possible role of apoptosis. J. Vasc. Res. 2001, 38, 462–470. [Google Scholar] [CrossRef]
- Ziegelhöffer-Mihalovicova, B.; Arnold, N.; Marx, G.; Tannapfel, A.; Zimmer, H.G.; Rassler, B. Effects of salt loading and various therapies on cardiac hypertrophy and fibrosis in young spontaneously hypertensive rats. Life Sci. 2006, 79, 838–846. [Google Scholar] [CrossRef]
- van Empel, V.P.; De Windt, L.J. Myocyte hypertrophy and apoptosis: A balancing act. Cardiovasc. Res. 2004, 63, 487–499. [Google Scholar] [CrossRef]
- Kokubo, M.; Uemura, A.; Matsubara, T.; Murohara, T. Noninvasive evaluation of the time course of change in cardiac function in spontaneously hypertensive rats by echocardiography. Hypertens. Res. 2005, 28, 601–609. [Google Scholar] [CrossRef][Green Version]
- Asai, T.; Kushiro, T.; Fujita, H.; Kanmatsuse, K. Different effects on inhibition of cardiac hypertrophy in spontaneously hypertensive rats by monotherapy and combination therapy of adrenergic receptor antagonists and/or the angiotensin II type 1 receptor blocker under comparable blood pressure reduction. Hypertens. Res. 2005, 28, 79–87. [Google Scholar] [CrossRef][Green Version]
- Rocha, W.A.; Lunz, W.; Baldo, M.P.; Pimentel, E.B.; Dantas, E.M.; Rodrigues, S.L.; Mill, J.G. Kinetics of cardiac and vascular remodeling by spontaneously hypertensive rats after discontinuation of long-term captopril treatment. Braz.J. Med. Biol. Res. 2010, 43, 390–396. [Google Scholar] [CrossRef]
- Hojná, S.; Kadlecová, M.; Dobešová, Z.; Valoušková, V.; Zicha, J.; Kuneš, J. The participation of brain NO synthase in blood pressure control of adult spontaneously hypertensive rats. Mol. Cell Biochem. 2007, 297, 21–29. [Google Scholar] [CrossRef]
- Perrucci, G.L.; Barbagallo, V.A.; Corlianò, M.; Tosi, D.; Santoro, R.; Nigro, P.; Poggio, P.; Bulfamante, G.; Lombardi, F.; Pompilio, G. Integrin amb5 in vitro inhibition limits pro-fibrotic response in cardiac fibroblasts of spontaneously hypertensive rats. J. Transl. Med. 2018, 16, 352. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Li, H.; Zeng, C.; Chen, W.; Wei, L.; Liu, Y.; Qi, X. Endogenous CCN5 Participates in Angiotensin II/TGF-β1 Networking of Cardiac Fibrosis in High Angiotensin II-Induced Hypertensive Heart Failure. Front. Pharmacol. 2020, 11, 1235. [Google Scholar] [CrossRef] [PubMed]
- Schlüter, K.D.; Wenzel, S. Angiotensin II: A hormone involved in and contributing to pro-hypertrophic cardiac networks and target of anti-hypertrophic cross-talks. Pharmacol. Ther. 2008, 119, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, J.M.; Pfeffer, M.A.; Mirsky, I.; Braunwald, E. Regression of left ventricular hypertrophy and prevention of left ventricular dysfunction by captopril in the spontaneously hypertensive rat. Proc. Natl. Acad. Sci. USA 1982, 79, 3310–3314. [Google Scholar] [CrossRef] [PubMed]
- Ago, T.; Yang, Y.; Zhai, P.; Sadoshima, J. Nifedipine inhibits cardiac hypertrophy and left ventricular dysfunction in response to pressure overload. J. Cardiovasc. Transl. Res. 2010, 3, 304–313. [Google Scholar] [CrossRef]
- Besse, S.; Robert, V.; Assayag, P.; Delcayre, C.; Swynghedauw, B. Nonsynchronous changes in myocardial collagen mRNA and protein during aging: Effect of DOCA-salt hypertension. Am. J. Physiol. 1994, 267, H2237–H2244. [Google Scholar] [CrossRef]
- Slama, M.; Ahn, J.; Varagic, J.; Susic, D.; Frohlich, E.D. Long-term left ventricular echocardiographic follow-up of SHR and WKY rats: Effects of hypertension and age. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H181–H185. [Google Scholar] [CrossRef]
- Zimmer, J.; Hawlitschek, C.; Rabald, S.; Hagendorff, A.; Zimmer, H.G.; Rassler, B. Effects of late-onset and long-term captopril and nifedipine treatment in aged spontaneously hypertensive rats: Echocardiographic studies. Hypertens. Res. 2015, 38, 716–722. [Google Scholar] [CrossRef][Green Version]
- Linz, W.; Jessen, T.; Becker, R.H.; Schölkens, B.A.; Wiemer, G. Long-term ACE inhibition doubles lifespan of hypertensive rats. Circulation 1997, 96, 3164–3172. [Google Scholar] [CrossRef]
- Briest, W.; Hölzl, A.; Rassler, B.; Deten, A.; Leicht, M.; Baba, H.A.; Zimmer, H.-G. Cardiac remodeling after long term norepinephrine treatment in rats. Cardiovasc. Res. 2001, 52, 265–273. [Google Scholar] [CrossRef]
- Briest, W.; Hölzl, A.; Rassler, B.; Deten, A.; Baba, H.A.; Zimmer, H.-G. Significance of matrix metalloproteinases in norepinephrine-induced remodelling of rat hearts. Cardiovasc. Res. 2003, 57, 379–387. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Animal Group | SBP [mmHg] | HR [min−1] | BW [g] | |||
|---|---|---|---|---|---|---|
| Baseline | Final | Baseline | Final | Baseline | Final | |
| yCtrl | 173.8 ± 3.1 | 201.7 ± 6.5 ° | 384.2 ± 10.3 | 416.5 ± 13.5 | 185.7 ± 4.2 | 309.7 ± 7.3 °° |
| yC+N | 157.5 ± 3.7 | 152.5 ± 2.8 | 396.9 ± 9.1 | 397.7 ± 9.2 | 175.8 ± 7.3 | 308.0 ± 7.3 °° |
| oCtrl | 231.0 ± 8.7 | 239.0 ± 5.1 | 413.5 ± 14.3 | 400.2 ± 20.6 | 396.7 ± 9.7 | 377.6 ± 37.2 |
| oC+N | 244.5 ± 8.1 | 193.6 ± 4.8 ° | 401.0 ± 14.6 | 409.2 ± 6.7 | 414.7 ± 8.6 | 418.6 ± 5.4 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rassler, B.; Hawlitschek, C.; Brendel, J.; Zimmer, H.-G. How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment. Biomedicines 2022, 10, 3059. https://doi.org/10.3390/biomedicines10123059
Rassler B, Hawlitschek C, Brendel J, Zimmer H-G. How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment. Biomedicines. 2022; 10(12):3059. https://doi.org/10.3390/biomedicines10123059
Chicago/Turabian StyleRassler, Beate, Christina Hawlitschek, Julia Brendel, and Heinz-Gerd Zimmer. 2022. "How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment" Biomedicines 10, no. 12: 3059. https://doi.org/10.3390/biomedicines10123059
APA StyleRassler, B., Hawlitschek, C., Brendel, J., & Zimmer, H.-G. (2022). How Do Young and Old Spontaneously Hypertensive Rats Respond to Antihypertensive Therapy? Comparative Studies on the Effects of Combined Captopril and Nifedipine Treatment. Biomedicines, 10(12), 3059. https://doi.org/10.3390/biomedicines10123059