

Investigation of Cerebral Autoregulation Using Time-Frequency Transformations


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Volunteers
2.2. Time-Frequency Analysis of Signals Characterizing CA
2.2.1. Short-Time Fourier Transform
2.2.2. Continuous Wavelet Transform
2.3. Wavelet Transform of Signals Characterizing CA
2.3.1. Smoothing
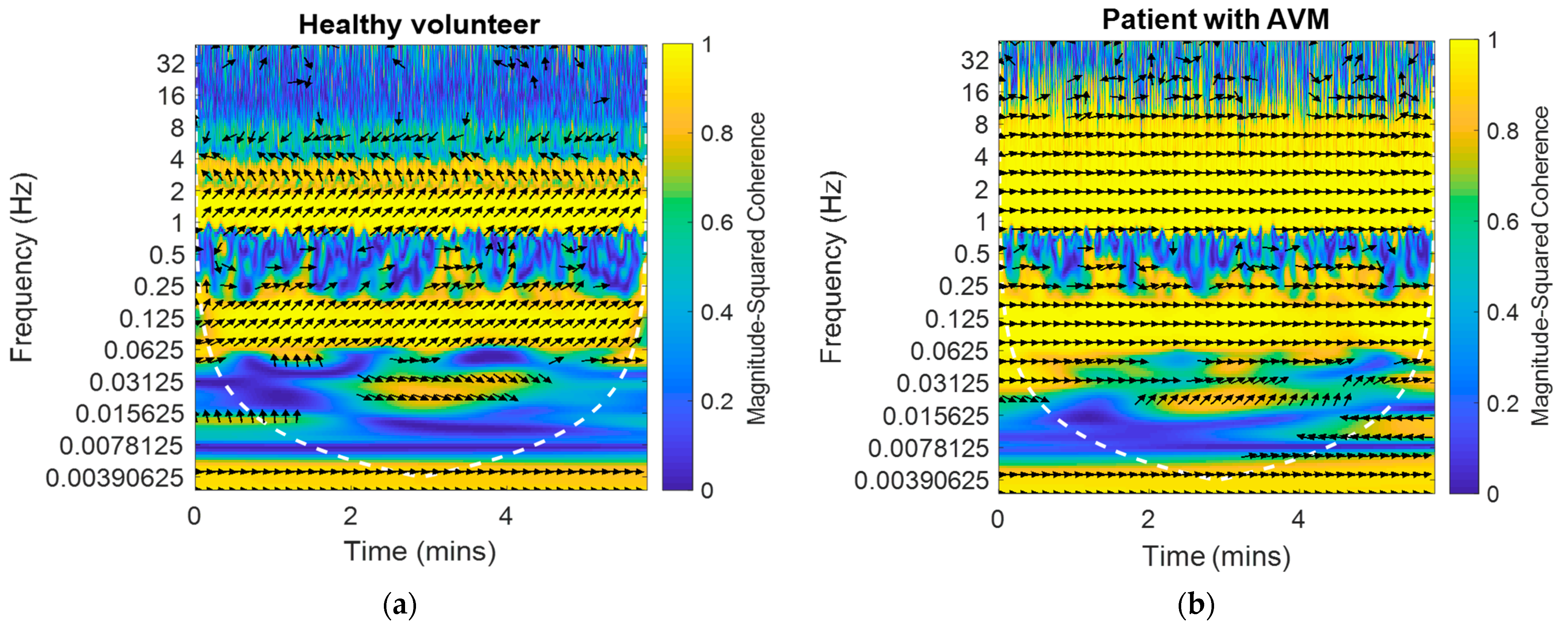
2.3.2. Cross-Wavelet Transform
3. Results
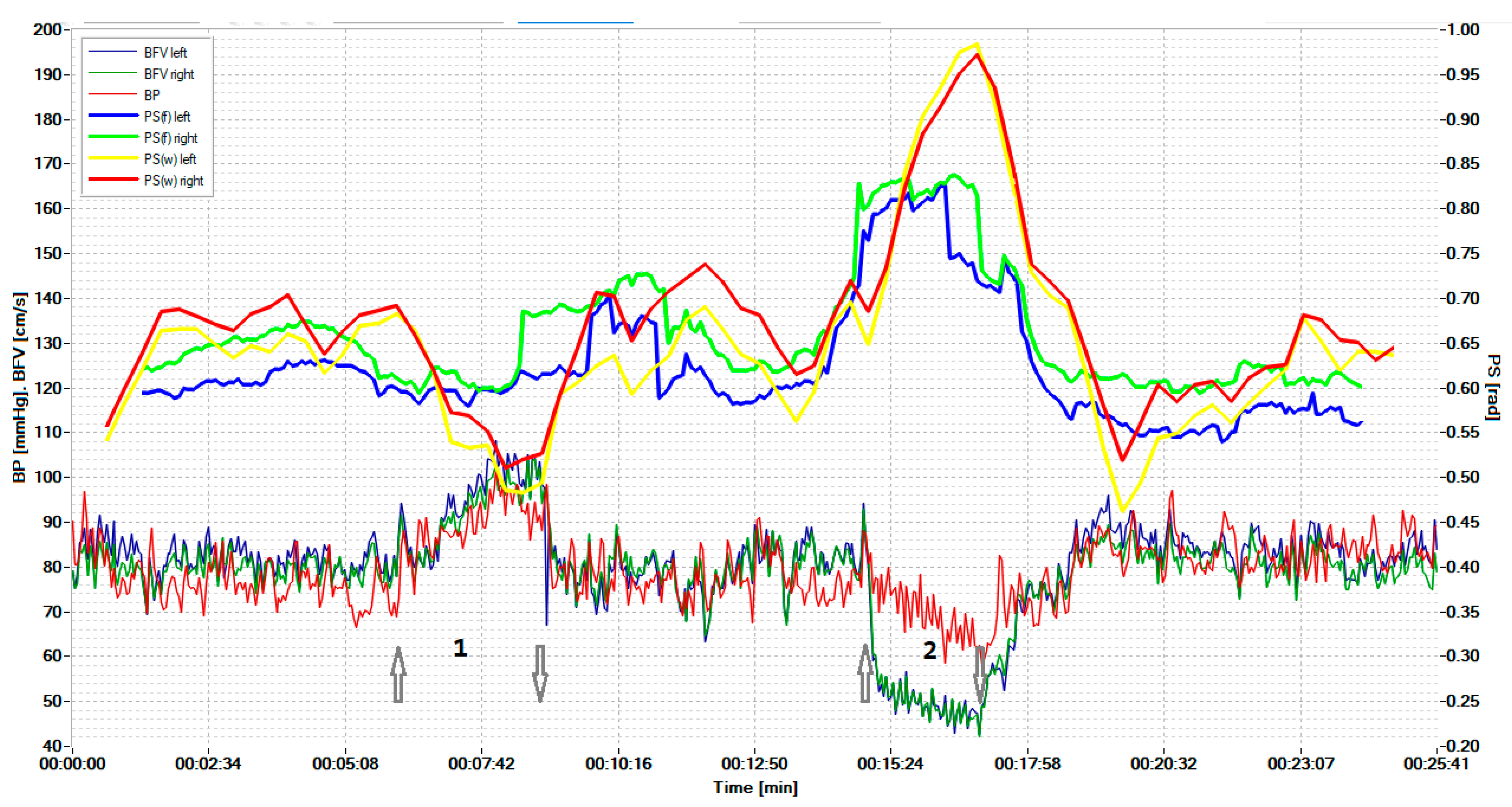
3.1. Results of the Wavelet Analysis of the BP and BFV Signals
3.2. System of Neuro Care Monitoring
- -
- The hypercapnic test led to a greater relative decrease in PS on both sides for the CWT method than for the STFT method; the magnitude of the decrease was 14.6 ± 6.6% for CWT and 8.2 ± 4.5% on the left (p = 0.022), and for STFT—14.4 ± 5.8% and 8.2 ± 4.2% on the right (p = 0.014).
- -
- The hypocapnic test led to a greater relative increase in PS on both sides for the CWT method than for the STFT method; the magnitude of the increase was 44.4 ± 22.7% for CWT and 28.8 ± 17.3% for STFT on the left (p = 0.035), 45.9 ± 24.8% and 28.2 ± 17.9% on the right (p = 0.041).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olesen, J. Quantitative evaluation of normal and pathologic cerebral blood regulation to perfusion pressure: Changes in man. Arch. Neurol. 1973, 28, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Aaslid, R.; Markwalder, T.M.; Nornes, H. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. J. Neurosurg. 1982, 57, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Kontos, H. Validity of cerebral arterial blood flow calculations from velocity measurements. Stroke 1989, 20, 1–3. [Google Scholar] [CrossRef]
- Newell, D.; Wim, H. Transcranial Doppler in cerebral vasospasm. Neurosurg. Clin. N. Am. 1990, 1, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.B.; Wong, M.L.; Bannan, P.E.; Piper, I.R.; Reilly, P.L. Transcranial Doppler identification of changing autoregulatory threshold after autoregulatory impartment. Neurosurgery 2001, 48, 369–375. [Google Scholar]
- Kuo, T.C.; Chern, C.C.; Yang Hsu, H.-Y.; Wong, W.-J.; Sheng, W.Y.; Hu, H.-H. Mechanisms underlying phase lag between systemic arterial blood pressure and cerebral blood flow velocity. Cerebrovasc. Dis. 2003, 16, 402–409. [Google Scholar] [CrossRef]
- Soehle, M.; Czosnyka, M.; Pickard, J.D.; Kirkpatrick, P.J. Continuous assessment of cerebral autoregulation in subarachnoid hemorrhage. Anedth. Amalg. 2004, 98, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Van Beek, A.H.; Claassen, J.; Rikkert, M.; Jansen, R. Cerebral autoregulation on overview of current concepts and methodology with special focus on the elderly. J. Cereb. Blood Flow Metab. 2008, 28, 1071–1085. [Google Scholar] [CrossRef] [PubMed]
- Panerai, R. Transcranial Doppler for evaluation of cerebral autoregulation. Cerebral autoregulation dynamics in premature newborns. Clin. Auton Res. 2009, 19, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Porras, S.; Santos, E.; Czosnyka, M.; Zheng, Z.; Unterberg, A.W.; Sakowitz, O.W. Long pressure reactivity index (L-PRx) as a measure of autoregulation correlates with outcomes in traumatic brain injury patients. Acta Neurochir. 2012, 154, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Hlatky, R.; Valadka, A.B.; Robertson, C.S. Analisis of dynamic autoregulation assessed by the cuff deflation method. Neurocrit. Care 2006, 4, 127–132. [Google Scholar] [CrossRef]
- Julien, C. The enigma of Mayer waves: Facts and models. Cardiovasc. Res. 2006, 70, 12–21. [Google Scholar] [CrossRef]
- Mayer, S. Studien zur physiologie des herzens und der blutgefässe. Sitz. Kais. Akad. Wiss. 1876, 74, 281–307. [Google Scholar]
- Reinhard, M.; Roth, M.; Müller, T.; Guschlbauer, B.; Timmer, J.; Czosnyka, M.; Hetzel, A. Effect of carotid Endarterectomy or Stenting on improvement of dynamic cerebral autoregulation. Stroke 2004, 35, 1381–1387. [Google Scholar] [CrossRef]
- Czosnyka, M.; Brady, K.; Reinhard, M.; Smielewski, P.; Steiner, L.A. Monitoring of cerebrovascular autoregulation: Facts, myths, and missing links. Naurocrit. Care 2009, 10, 373–386. [Google Scholar] [CrossRef]
- Payne, S. Cerebral Autoregulation Control of Blood Flow in the Brain; Springer: Berlin, Germany, 2016; Volume XV, p. 125. [Google Scholar]
- Smielewski, P.; Czosnyka, M.; Zabolotny, W.; Kirkpatrick, P. A computing system for the clinical and experimental investigation of cerebrovascular reactivity. Int. J. Clin. Monit. Comput. 1997, 14, 185–198. [Google Scholar] [CrossRef]
- Budohoski, K.; Czosnyka, M.; de Riva, N.; Smielewski, P.; Pickard, J.D.; Menon, D.K.; Kirkpatrick, P.J.; Lavinio, A. The relationship between cerebral blood flow autoregulation and cerebrovascular pressure reactivity after traumatic brain injury. Neurosurgery 2012, 71, 652–660. [Google Scholar] [CrossRef]
- Xiuyun, L.; Czosnyka, M.; Donnelly, J.; Smielewski, P. Comparison of Frequency and Time Domain Methods of Assessment of Cerebral Autoregulation in Traumatic Brain Injury. J. Cereb. Blood Flow Metab. 2014, 35, 192. [Google Scholar]
- Liu, X.; Hu, X.; Brady, K.M. Comparison of wavelet and correlation indices of cerebral autoregulation in a pediatric swine model of cardiac arrest. Sci. Rep. 2020, 10, 5926. [Google Scholar] [CrossRef]
- Tian, F.; Tarumi, T.; Liu, H.; Zhang, R.; Chalak, L. Wavelet coherence analysis of dynamic cerebral autoregulation in neonatal hypoxic–ischemic encephalopathy. NeuroImage Clin. 2016, 11, 124–132. [Google Scholar] [CrossRef]
- Smielewski, P.; Czosnyka, M.; Kirkpatrick, P.; McEroy, H.; Rutkowska, H.; Pickard, J.D. Assessment of cerebral autoregulation using carotid artery compression. Stroke 1996, 27, 2197–2203. [Google Scholar] [CrossRef]
- Lewis, P.M.; Smielewski, P.; Rosenfeld, J.V.; Pickard, J.D.; Czosnyka, M. Assessment of cerebral autoregulation from respiratory oscillations in ventilated patients after traumatic brain injury. Acta Neurochir. Suppl. 2012, 114, 141–146. [Google Scholar]
- Pan, Y.; Wan, W.; Xiang, M.; Guan, Y. Transcranial Doppler Ultrasonography as a Diagnostic Tool for Cerebrovascular Disorders. Front. Hum. Neurosci. 2022, 16, 841809. [Google Scholar] [CrossRef]
- D’Andrea, A.; Conte, M.; Cavallaro, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Carbone, A.; Natale, F.; Santoro, G.; et al. Transcranial Doppler ultrasonography: From methodology to major clinical applications. World J. Cardiol. 2016, 8, 383–400. [Google Scholar] [CrossRef]
- Tas, J.; Eleveld, N.; Borg, M.; Bos, K.D.J.; Langermans, A.P.; van Kuijk, S.M.J.; van der Horst, I.C.C.; Elting, J.W.J.; Aries, M.J.H. Cerebral Autoregulation Assessment Using the Near Infrared Spectroscopy ‘NIRS-Only’ High Frequency Methodology in Critically Ill Patients: A Prospective Cross-Sectional Study. Cells 2022, 11, 2254. [Google Scholar] [CrossRef]
- Panerai, R.B.; Jara, J.L.; Saeed, N.P.; Horsfield, M.A.; Robinson, T.G. Dynamic cerebral autoregulation following acute ischaemic stroke: Comparison of transcranial Doppler and magnetic resonance imaging techniques. J. Cereb. Blood Flow Metab. 2016, 36, 2194–2202. [Google Scholar] [CrossRef]
- Watanabe, H.; Washio, T.; Saito, S.; Hirasawa, A.; Suzuki, R.; Shibata, S.; Brothers, R.M.; Ogoh, S. Validity of transcranial Doppler ultrasonography-determined dynamic cerebral autoregulation estimated using transfer function analysis. J. Clin. Monit. Comput. 2022, 36, 1711–1721. [Google Scholar] [CrossRef]
- Classen, J.; Abeelen, A.M.; Simpson, D.M. Transfer function analysis of dynamic cerebral autoregulation research network. J. Cereb. Blood Flow Metab. 2016, 1, 1–16. [Google Scholar]
- Alkhachroum, A.; Kromm, J.; De Georgia, M.A. Big data and predictive analytics in neurocritical care. Curr. Neurol. Neurosci. Rep. 2022, 22, 19–32. [Google Scholar] [CrossRef]
- Malykhina, G.F.; Merkusheva, A.V. Classes of transformations of a non-stationary signal in information-measuring systems. VI. Correspondence of the form of covariance and the type of time-frequency transformation. Sci. Instrum. 2007, 17, 75–87. [Google Scholar]
- Merkusheva, A.V.; Malykhina, G.F. The generalized Fourier transform method for time-frequency transformations, multiplexing and filtering of non-stationary signals in information systems. Sci. Instrum. 2006, 16, 85–96. [Google Scholar]
- Torrence, C.; Compo, G.P. Program in Atmospheric and Oceanic Sciences, University of Colorado, Boulder, Colorado. Bull. Am. Meteorol. Soc. 1998, 79, 61–78. [Google Scholar] [CrossRef]
- Grinsted, A.; Moore, J.C.; Jevrejeva, S. Application of the cross wavelet transform and wavelet coherence to geophysical time series. Nonlinear Processes in Geophysics. Eur. Geosci. Union (EGU) 2004, 11, 561–566. [Google Scholar]
- Kulaichev, A.P. The Informativeness of Coherence Analysis in EEG Studies. Neurosci. Behav. Phys. 2011, 41, 321–328. [Google Scholar] [CrossRef]
- Malykhina, G.; Salnikov, V.; Semenyutin, V.; Tarkhov, D. Digitalization of medical services for detecting violations of cerebrovascular regulation based on a neural network signal analysis algorithm. ACM Int. Conf. Proc. Ser. 2020, 61, 1–11. [Google Scholar]
- Malykhina, G.F.; Salnikov, V.Y.; Semenyutin, V.B. Neural network algorithm for the diagnosis of impaired cerebral autoregulation. In Neuralinformatics; Publishing House of the Moscow Engineering Physics Institute: Moscow, Russia, 2020. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Semenyutin, V.; Antonov, V.; Malykhina, G.; Salnikov, V. Investigation of Cerebral Autoregulation Using Time-Frequency Transformations. Biomedicines 2022, 10, 3057. https://doi.org/10.3390/biomedicines10123057
Semenyutin V, Antonov V, Malykhina G, Salnikov V. Investigation of Cerebral Autoregulation Using Time-Frequency Transformations. Biomedicines. 2022; 10(12):3057. https://doi.org/10.3390/biomedicines10123057
Chicago/Turabian StyleSemenyutin, Vladimir, Valery Antonov, Galina Malykhina, and Vyacheslav Salnikov. 2022. "Investigation of Cerebral Autoregulation Using Time-Frequency Transformations" Biomedicines 10, no. 12: 3057. https://doi.org/10.3390/biomedicines10123057
APA StyleSemenyutin, V., Antonov, V., Malykhina, G., & Salnikov, V. (2022). Investigation of Cerebral Autoregulation Using Time-Frequency Transformations. Biomedicines, 10(12), 3057. https://doi.org/10.3390/biomedicines10123057