
Cell-Free Amniotic Fluid and Regenerative Medicine: Current Applications and Future Opportunities

 , ,
, ,
Abstract
1. Introduction
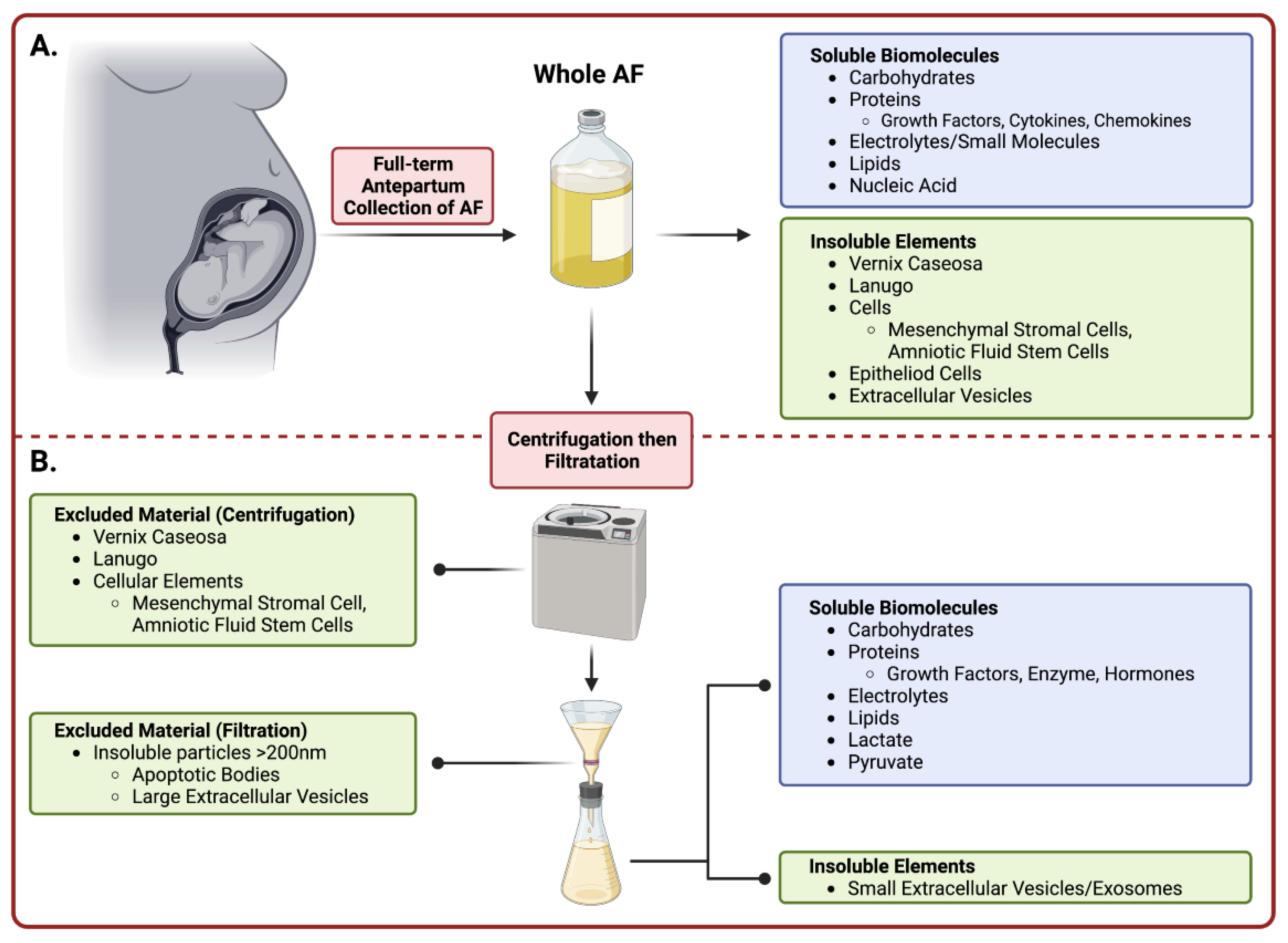
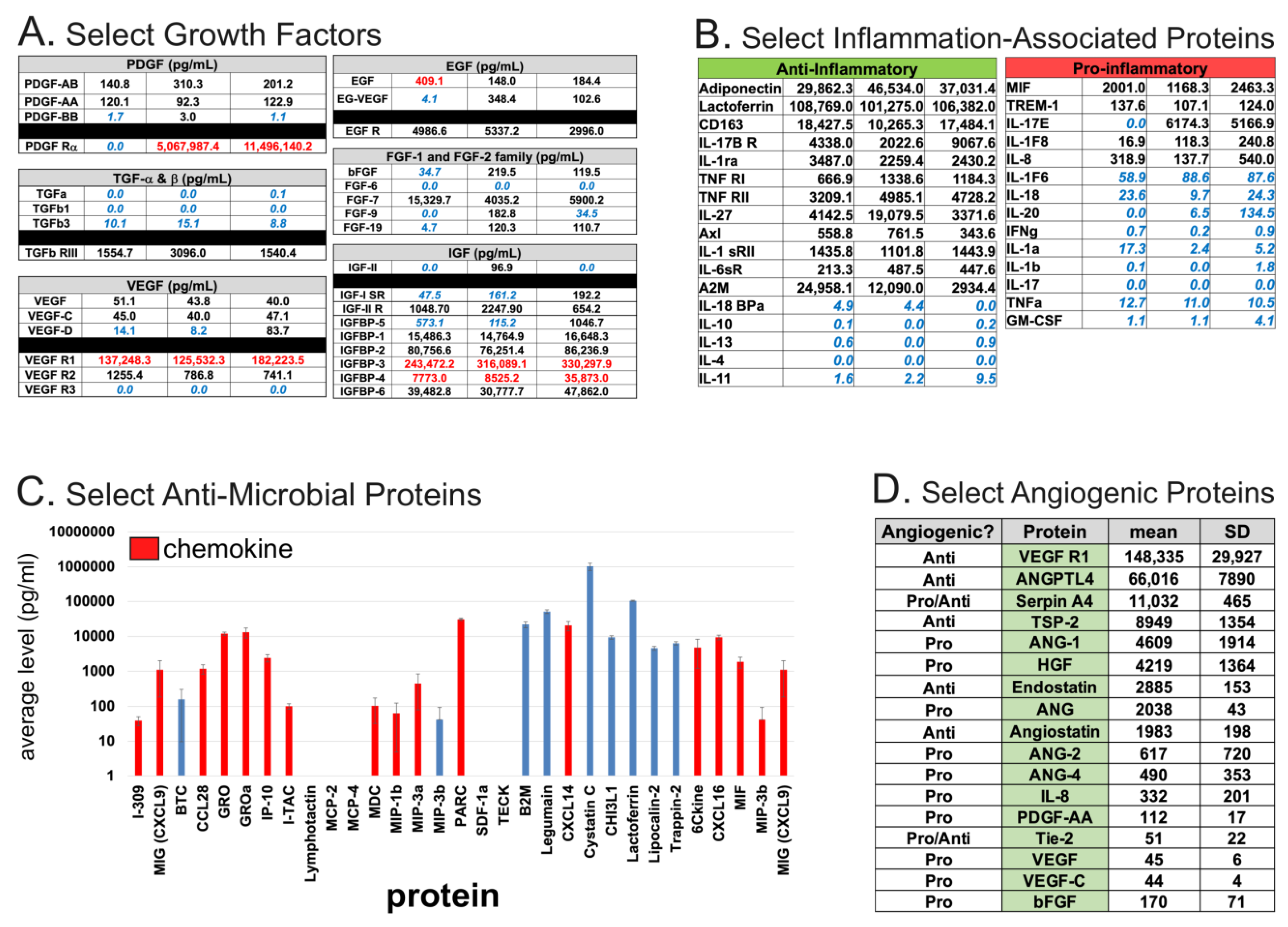
2. AF Components: Biomolecules, Cells, and Extracellular Vesicles
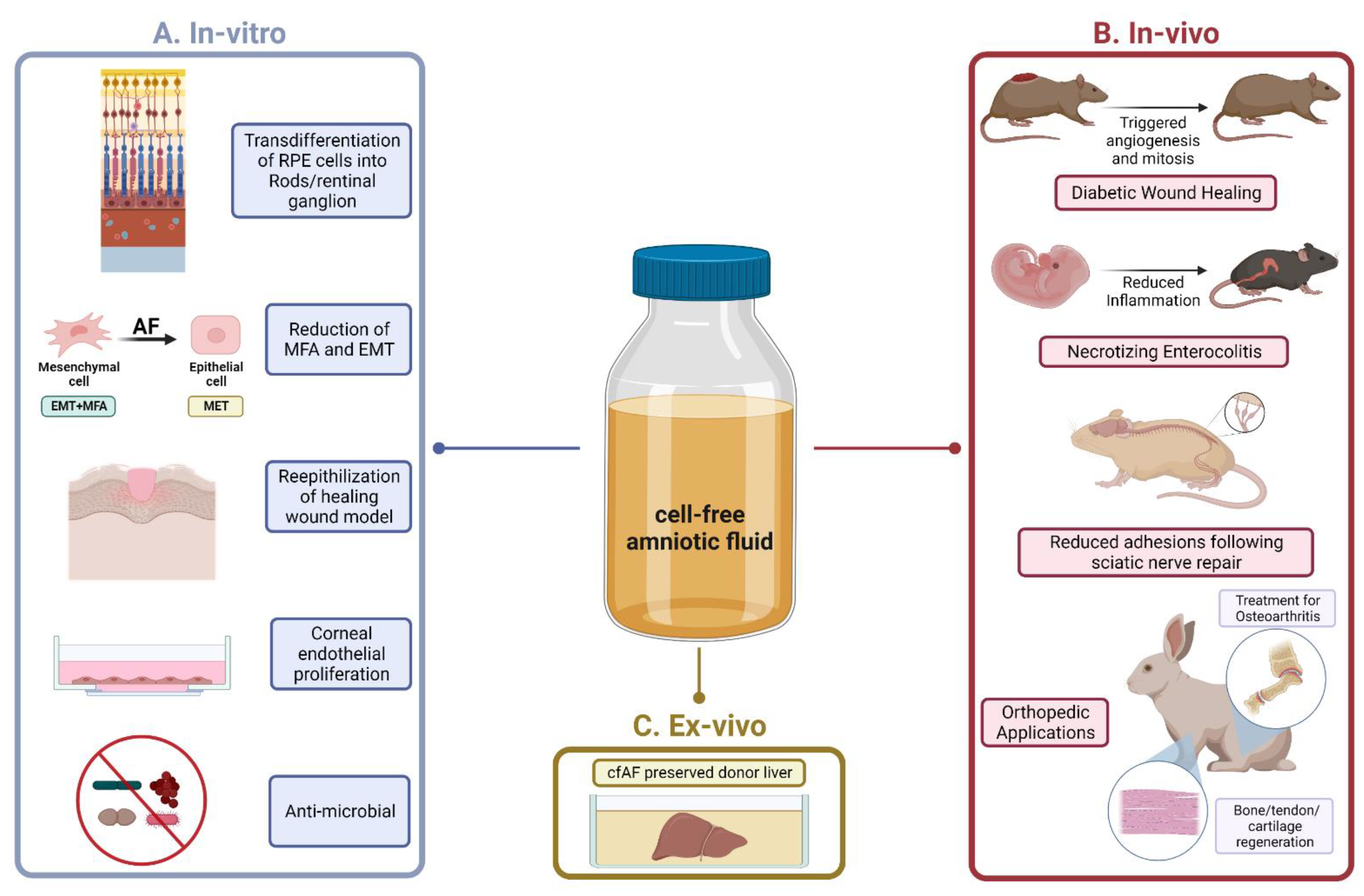
3. Fundamental and Translational Research Using cfAF
3.1. Congenital Diseases
3.2. Wound Healing
3.3. Nerve Repair
3.4. Musculoskeletal Applications
3.5. Other Translational Studies
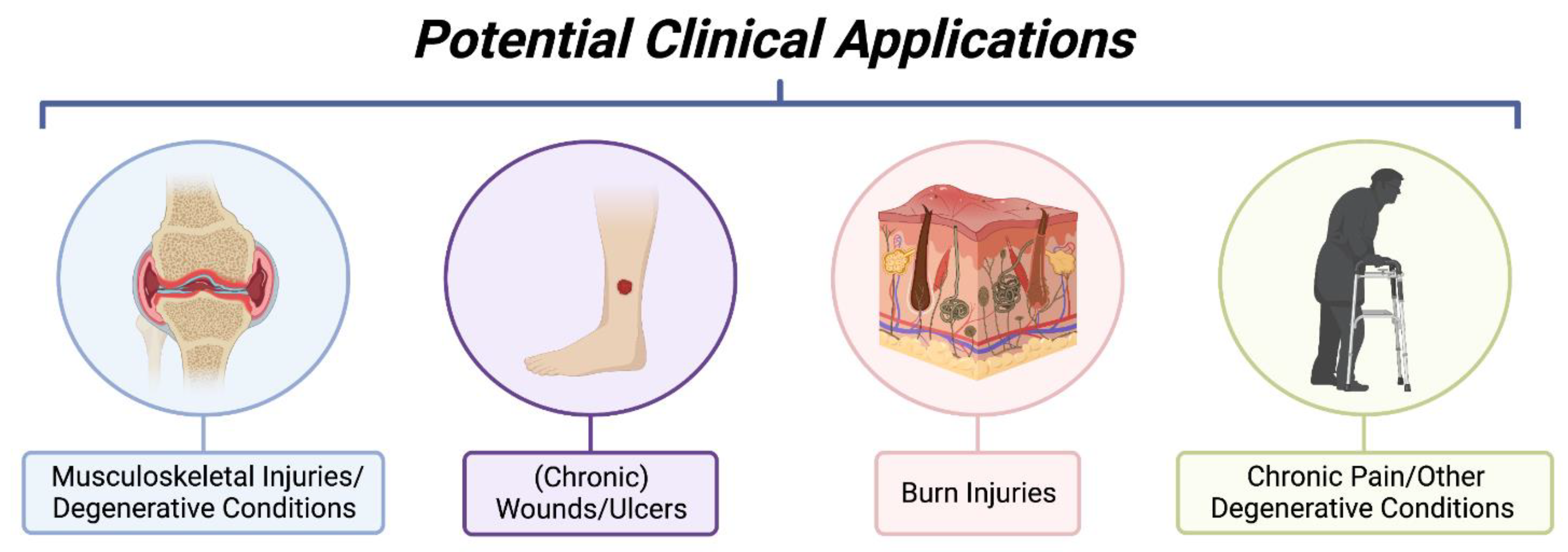
4. Current Clinical Studies/Applications Using Cell-Free Amniotic Fluid or Derivatives
4.1. Wound Healing
4.2. Orthopedic Applications
4.3. Ophthalmological Applications
4.4. COVID-19
5. Conclusions, Limitations, and Future Outlook
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, H.L. Observations on the Prevention of Postoperative Peritonitis and Abdominal Adhesions. Surg. Gynec. Obst. 1927, 45, 612. [Google Scholar]
- Johnson, H.L. Amniotic Fluid Concentrate in the Prevention of Adhesions. N. Engl. J. Med. 1928, 199, 661–664. [Google Scholar] [CrossRef]
- Trusler, H.M. Peritonitis: An Experimental Study of Healing in the Peritoneum and the Therapeutic Effect of Amniotic Fluid Concentrate. Arch. Surg. 1931, 22, 983–992. [Google Scholar] [CrossRef]
- Gepfert, J.R. Intraperitoneal Use of Amniotic Fluid to Promote Smoother Postoperative Convalescence. Am. J. Surg. 1936, 32, 40–44. [Google Scholar] [CrossRef]
- Shimberg, M. The Use of Amniotic-Fluid Concentrate in Orthopaedic Conditions. JBJS 1938, 20, 167–177. [Google Scholar]
- Loukogeorgakis, S.P.; De Coppi, P. Concise Review: Amniotic Fluid Stem Cells: The Known, the Unknown, and Potential Regenerative Medicine Applications. Stem Cells 2017, 35, 1663–1673. [Google Scholar] [CrossRef]
- Johnson, J.; Shojaee, M.; Mitchell Crow, J.; Khanabdali, R. From Mesenchymal Stromal Cells to Engineered Extracellular Vesicles: A New Therapeutic Paradigm. Front. Cell Dev. Biol. 2021, 9, 705676. [Google Scholar] [CrossRef]
- Beloosesky, R.; Ross, M.G. Amniotic Fluid. In Encyclopedia of Reproduction, 2nd ed.; Skinner, M.K., Ed.; Academic Press: Oxford, UK, 2018; pp. 380–386. ISBN 978-0-12-815145-7. [Google Scholar]
- Fetal Physiology—ClinicalKey. Available online: https://www.clinicalkey.com/#!/content/book/3-s2.0-B9780323566889000053 (accessed on 15 June 2022).
- Suliburska, J.; Kocyłowski, R.; Komorowicz, I.; Grzesiak, M.; Bogdański, P.; Barałkiewicz, D. Concentrations of Mineral in Amniotic Fluid and Their Relations to Selected Maternal and Fetal Parameters. Biol. Trace Elem. Res. 2016, 172, 37–45. [Google Scholar] [CrossRef]
- Beall, M.H.; van den Wijngaard, J.P.H.M.; van Gemert, M.J.C.; Ross, M.G. Amniotic Fluid Water Dynamics. Placenta 2007, 28, 816–823. [Google Scholar] [CrossRef]
- Fitzsimmons, E.D.; Bajaj, T. Embryology, Amniotic Fluid. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Underwood, M.A.; Gilbert, W.M.; Sherman, M.P. Amniotic Fluid: Not Just Fetal Urine Anymore. J. Perinatol. 2005, 25, 341–348. [Google Scholar] [CrossRef]
- Tong, X.-L.; Wang, L.; Gao, T.-B.; Qin, Y.-G.; Qi, Y.-Q.; Xu, Y.-P. Potential Function of Amniotic Fluid in Fetal Development—Novel Insights by Comparing the Composition of Human Amniotic Fluid with Umbilical Cord and Maternal Serum at Mid and Late Gestation. J. Chin. Med. Assoc. 2009, 72, 368–373. [Google Scholar] [CrossRef]
- Pierce, J.; Jacobson, P.; Benedetti, E.; Peterson, E.; Phibbs, J.; Preslar, A.; Reems, J.-A. Collection and Characterization of Amniotic Fluid from Scheduled C-Section Deliveries. Cell Tissue Bank. 2016, 17, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Dixon, C.L.; Sheller-Miller, S.; Saade, G.R.; Fortunato, S.J.; Lai, A.; Palma, C.; Guanzon, D.; Salomon, C.; Menon, R. Amniotic Fluid Exosome Proteomic Profile Exhibits Unique Pathways of Term and Preterm Labor. Endocrinology 2018, 159, 2229–2240. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Bowen, C.M.; Shoja, M.M.; Castro de Pereira, K.L.; Dongur, L.P.; Saad, A.; Russell, W.K.; Broderick, T.C.; Fair, J.H.; Fagg, W.S. Comparative Analysis of Co-Cultured Amniotic Cell-Conditioned Media with Cell-Free Amniotic Fluid Reveals Differential Effects on Epithelial–Mesenchymal Transition and Myofibroblast Activation. Biomedicines 2022, 10, 2189. [Google Scholar] [CrossRef]
- Chestnut, D.; Wong, C.; Tsen, L.; Kee, W.D.N.; Beilin, Y.; Mhyre, J.; Bateman, B.T.; Nathan, N. Chestnut’s Obstetric Anesthesia: Principles and Practice, 6th ed.; Elseiver: Amsterdam, The Netherlands, 2019; ISBN 978-0-323-56688-9. [Google Scholar]
- Center for Biologics Evaluation and Research; Center for Devices and Radiological Health. Regulatory Considerations for Human Cells, Tissues, and Cellular and Tissue-Based Products: Minimal Manipulation and Homologous Use. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/regulatory-considerations-human-cells-tissues-and-cellular-and-tissue-based-products-minimal (accessed on 10 August 2022).
- Rodríguez-Fuentes, D.E.; Fernández-Garza, L.E.; Samia-Meza, J.A.; Barrera-Barrera, S.A.; Caplan, A.I.; Barrera-Saldaña, H.A. Mesenchymal Stem Cells Current Clinical Applications: A Systematic Review. Arch. Med. Res. 2021, 52, 93–101. [Google Scholar] [CrossRef]
- Gwam, C.; Emara, A.K.; Mohamed, N.; Chughtai, N.; Plate, J.; Ma, X. Amniotic Stem Cell-Conditioned Media for the Treatment of Nerve and Muscle Pathology: A Systematic Review. Surg. Technol. Int. 2021, 38, 407–414. [Google Scholar] [CrossRef]
- Sultan, P.; Seligman, K.; Carvalho, B. Amniotic Fluid Embolism: Update and Review. Curr. Opin. Anaesthesiol. 2016, 29, 288–296. [Google Scholar] [CrossRef]
- van Niel, G.; D’Angelo, G.; Raposo, G. Shedding Light on the Cell Biology of Extracellular Vesicles. Nat. Rev. Mol. Cell Biol. 2018, 19, 213–228. [Google Scholar] [CrossRef]
- Costa, A.; Quarto, R.; Bollini, S. Small Extracellular Vesicles from Human Amniotic Fluid Samples as Promising Theranostics. Int. J. Mol. Sci. 2022, 23, 590. [Google Scholar] [CrossRef]
- Bellio, M.A.; Young, K.C.; Milberg, J.; Santos, I.; Abdullah, Z.; Stewart, D.; Arango, A.; Chen, P.; Huang, J.; Williams, K.; et al. Amniotic Fluid-Derived Extracellular Vesicles: Characterization and Therapeutic Efficacy in an Experimental Model of Bronchopulmonary Dysplasia. Cytotherapy 2021, 23, 1097–1107. [Google Scholar] [CrossRef]
- Costa, A.; Ceresa, D.; De Palma, A.; Rossi, R.; Turturo, S.; Santamaria, S.; Balbi, C.; Villa, F.; Reverberi, D.; Cortese, K.; et al. Comprehensive Profiling of Secretome Formulations from Fetal- and Perinatal Human Amniotic Fluid Stem Cells. Int. J. Mol. Sci. 2021, 22, 3713. [Google Scholar] [CrossRef] [PubMed]
- Torre, P.d.; Flores, A.I. Current Status and Future Prospects of Perinatal Stem Cells. Genes 2021, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Jones, J.; Gunst, P.R.; Kacerovsky, M.; Fortunato, S.J.; Saade, G.R.; Basraon, S. Amniotic Fluid Metabolomic Analysis in Spontaneous Preterm Birth. Reprod. Sci. 2014, 21, 791–803. [Google Scholar] [CrossRef]
- Zwemer, L.M.; Bianchi, D.W. The Amniotic Fluid Transcriptome as a Guide to Understanding Fetal Disease. Cold Spring Harb. Perspect. Med. 2015, 5, a023101. [Google Scholar] [CrossRef]
- Beretti, F.; Zavatti, M.; Casciaro, F.; Comitini, G.; Franchi, F.; Barbieri, V.; La Sala, G.B.; Maraldi, T. Amniotic Fluid Stem Cell Exosomes: Therapeutic Perspective. Biofactors 2018, 44, 158–167. [Google Scholar] [CrossRef]
- Zhang, Q.; Lai, D. Application of Human Amniotic Epithelial Cells in Regenerative Medicine: A Systematic Review. Stem Cell Res. Ther. 2020, 11, 439. [Google Scholar] [CrossRef] [PubMed]
- Centurione, L.; Centurione, M.A.; Antonucci, I.; Sancilio, S.; Stati, G.; Stuppia, L.; Di Pietro, R. Human Amniotic Fluid Stem Cells Are Able to Form Embryoid Body-like Aggregates Which Performs Specific Functions: Morphological Evidences. Histochem. Cell Biol. 2021, 155, 381–390. [Google Scholar] [CrossRef]
- Urabe, F.; Kosaka, N.; Ito, K.; Kimura, T.; Egawa, S.; Ochiya, T. Extracellular Vesicles as Biomarkers and Therapeutic Targets for Cancer. Am. J. Physiol. Cell Physiol. 2020, 318, C29–C39. [Google Scholar] [CrossRef]
- Lei, Q.; Gao, F.; Liu, T.; Ren, W.; Chen, L.; Cao, Y.; Chen, W.; Guo, S.; Zhang, Q.; Chen, W.; et al. Extracellular Vesicles Deposit PCNA to Rejuvenate Aged Bone Marrow-Derived Mesenchymal Stem Cells and Slow Age-Related Degeneration. Sci. Transl. Med. 2021, 13, eaaz8697. [Google Scholar] [CrossRef]
- Gupta, A.; Cady, C.; Fauser, A.-M.; Rodriguez, H.C.; Mistovich, R.J.; Potty, A.G.R.; Maffulli, N. Cell-Free Stem Cell-Derived Extract Formulation for Regenerative Medicine Applications. Int. J. Mol. Sci. 2020, 21, 9364. [Google Scholar] [CrossRef]
- Gupta, A.; Maffulli, N.; Rodriguez, H.C.; Mistovich, R.J.; Delfino, K.; Cady, C.; Fauser, A.-M.; Cundiff, E.D.; Martinez, M.A.; Potty, A.G. Cell-Free Stem Cell-Derived Extract Formulation for Treatment of Knee Osteoarthritis: Study Protocol for a Preliminary Non-Randomized, Open-Label, Multi-Center Feasibility and Safety Study. J. Orthop. Surg. Res. 2021, 16, 514. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A. Commentary: Cell-Free Stem Cell-Derived Extract Formulation for Treatment of Knee Osteoarthritis. J. Orthop. Orthop. Surg 2022, 3, 23–25. [Google Scholar] [CrossRef]
- Bazrafshan, A.; Owji, M.; Yazdani, M.; Varedi, M. Activation of Mitosis and Angiogenesis in Diabetes-Impaired Wound Healing by Processed Human Amniotic Fluid. J. Surg. Res. 2014, 188, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Kratz, G.; Palmer, B.; Haegerstrand, A. Effects of Keratinocyte Conditioned Medium, Amniotic Fluid and EGF in Reepithelialization of Human Skin Wounds in Vitro. Eur. J. Plast. Surg. 1995, 18, 209–213. [Google Scholar] [CrossRef]
- Nyman, E.; Huss, F.; Nyman, T.; Junker, J.; Kratz, G. Hyaluronic Acid, an Important Factor in the Wound Healing Properties of Amniotic Fluid: In Vitro Studies of Re-Epithelialisation in Human Skin Wounds. J. Plast. Surg. Hand Surg. 2013, 47, 89–92. [Google Scholar] [CrossRef]
- Ghaderi, S.; Soheili, Z.-S.; Ahmadieh, H.; Davari, M.; Jahromi, F.S.; Samie, S.; Rezaie-Kanavi, M.; Pakravesh, J.; Deezagi, A. Human Amniotic Fluid Promotes Retinal Pigmented Epithelial Cells’ Trans-Differentiation into Rod Photoreceptors and Retinal Ganglion Cells. Stem Cells Dev. 2011, 20, 1615–1625. [Google Scholar] [CrossRef]
- Feizi, S.; Soheili, Z.-S.; Bagheri, A.; Balagholi, S.; Mohammadian, A.; Rezaei-Kanavi, M.; Ahmadieh, H.; Samiei, S.; Negahban, K. Effect of Amniotic Fluid on the in Vitro Culture of Human Corneal Endothelial Cells. Exp. Eye Res. 2014, 122, 132–140. [Google Scholar] [CrossRef]
- Galask, R.P.; Snyder, I.S. Antimicrobial Factors in Amniotic Fluid. Am. J. Obstet. Gynecol. 1970, 106, 59–65. [Google Scholar] [CrossRef]
- Mao, Y.; Pierce, J.; Singh-Varma, A.; Boyer, M.; Kohn, J.; Reems, J.-A. Processed Human Amniotic Fluid Retains Its Antibacterial Activity. J. Transl. Med. 2019, 17, 68. [Google Scholar] [CrossRef]
- Monika, P.; Waiker, P.V.; Chandraprabha, M.N.; Rangarajan, A.; Murthy, K.N.C. Myofibroblast Progeny in Wound Biology and Wound Healing Studies. Wound Repair Regen. 2021, 29, 531–547. [Google Scholar] [CrossRef]
- Hall, C.; Gehmlich, K.; Denning, C.; Pavlovic, D. Complex Relationship Between Cardiac Fibroblasts and Cardiomyocytes in Health and Disease. J. Am. Heart Assoc. 2021, 10, e019338. [Google Scholar] [CrossRef] [PubMed]
- Ueha, S.; Shand, F.H.W.; Matsushima, K. Cellular and Molecular Mechanisms of Chronic Inflammation-Associated Organ Fibrosis. Front. Immunol. 2012, 3, 71. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Jain, S.K. Protective Effects of Amniotic Fluid in the Setting of Necrotizing Enterocolitis. Pediatr. Res. 2017, 82, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Zani, A.; Cananzi, M.; Fascetti-Leon, F.; Lauriti, G.; Smith, V.V.; Bollini, S.; Ghionzoli, M.; D’Arrigo, A.; Pozzobon, M.; Piccoli, M.; et al. Amniotic Fluid Stem Cells Improve Survival and Enhance Repair of Damaged Intestine in Necrotising Enterocolitis via a COX-2 Dependent Mechanism. Gut 2014, 63, 300–309. [Google Scholar] [CrossRef]
- O’Connell, J.S.; Lee, C.; Farhat, N.; Antounians, L.; Zani, A.; Li, B.; Pierro, A. Administration of Extracellular Vesicles Derived from Human Amniotic Fluid Stem Cells: A New Treatment for Necrotizing Enterocolitis. Pediatr. Surg. Int. 2021, 37, 301–309. [Google Scholar] [CrossRef]
- de Kroon, R.R.; de Baat, T.; Senger, S.; van Weissenbruch, M.M. Amniotic Fluid: A Perspective on Promising Advances in the Prevention and Treatment of Necrotizing Enterocolitis. Front. Pediatr. 2022, 10, 859805. [Google Scholar] [CrossRef]
- Good, M.; Siggers, R.H.; Sodhi, C.P.; Afrazi, A.; Alkhudari, F.; Egan, C.E.; Neal, M.D.; Yazji, I.; Jia, H.; Lin, J.; et al. Amniotic Fluid Inhibits Toll-like Receptor 4 Signaling in the Fetal and Neonatal Intestinal Epithelium. Proc. Natl. Acad. Sci. USA 2012, 109, 11330–11335. [Google Scholar] [CrossRef]
- Siggers, J.; Ostergaard, M.V.; Siggers, R.H.; Skovgaard, K.; Mølbak, L.; Thymann, T.; Schmidt, M.; Møller, H.K.; Purup, S.; Fink, L.N.; et al. Postnatal Amniotic Fluid Intake Reduces Gut Inflammatory Responses and Necrotizing Enterocolitis in Preterm Neonates. Am. J. Physiol. Gastrointest Liver Physiol. 2013, 304, G864–G875. [Google Scholar] [CrossRef]
- Østergaard, M.V.; Bering, S.B.; Jensen, M.L.; Thymann, T.; Purup, S.; Diness, M.; Schmidt, M.; Sangild, P.T. Modulation of Intestinal Inflammation by Minimal Enteral Nutrition with Amniotic Fluid in Preterm Pigs. JPEN J. Parenter Enter. Nutr. 2014, 38, 576–586. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Shankaran, S.; Laptook, A.R.; Walsh, M.C.; Hale, E.C.; Newman, N.S.; Schibler, K.; Carlo, W.A.; et al. Neonatal Outcomes of Extremely Preterm Infants From the NICHD Neonatal Research Network. Pediatrics 2010, 126, 443–456. [Google Scholar] [CrossRef]
- Groothuis, J.R.; Gutierrez, K.M.; Lauer, B.A. Respiratory Syncytial Virus Infection in Children With Bronchopulmonary Dysplasia. Pediatrics 1988, 82, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Garcia, O.; Carraro, G.; Turcatel, G.; Hall, M.; Sedrakyan, S.; Roche, T.; Buckley, S.; Driscoll, B.; Perin, L.; Warburton, D. Amniotic Fluid Stem Cells Inhibit the Progression of Bleomycin-Induced Pulmonary Fibrosis via CCL2 Modulation in Bronchoalveolar Lavage. PLoS ONE 2013, 8, e71679. [Google Scholar] [CrossRef] [PubMed]
- Buckley, S.; Shi, W.; Carraro, G.; Sedrakyan, S.; Da Sacco, S.; Driscoll, B.A.; Perin, L.; De Filippo, R.E.; Warburton, D. The Milieu of Damaged Alveolar Epithelial Type 2 Cells Stimulates Alveolar Wound Repair by Endogenous and Exogenous Progenitors. Am. J. Respir. Cell Mol. Biol. 2011, 45, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Pederiva, F.; Ghionzoli, M.; Pierro, A.; De Coppi, P.; Tovar, J.A. Amniotic Fluid Stem Cells Rescue Both in Vitro and in Vivo Growth, Innervation, and Motility in Nitrofen-Exposed Hypoplastic Rat Lungs through Paracrine Effects. Cell Transpl. 2013, 22, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Di Bernardo, J.; Maiden, M.M.; Hershenson, M.B.; Kunisaki, S.M. Amniotic Fluid Derived Mesenchymal Stromal Cells Augment Fetal Lung Growth in a Nitrofen Explant Model. J. Pediatr. Surg. 2014, 49, 859–864; discussion 864–865. [Google Scholar] [CrossRef]
- Longaker, M.T.; Whitby, D.J.; Adzick, N.S.; Crombleholme, T.M.; Langer, J.C.; Duncan, B.W.; Bradley, S.M.; Stern, R.; Ferguson, M.W.; Harrison, M.R. Studies in Fetal Wound Healing, VI. Second and Early Third Trimester Fetal Wounds Demonstrate Rapid Collagen Deposition without Scar Formation. J. Pediatr. Surg. 1990, 25, 63–68; discussion 68–69. [Google Scholar] [CrossRef]
- Nyman, E.; Lindholm, E.; Rakar, J.; Junker, J.P.E.; Kratz, G. Effects of Amniotic Fluid on Human Keratinocyte Gene Expression: Implications for Wound Healing. Exp. Dermatol. 2022, 31, 764–774. [Google Scholar] [CrossRef]
- Tonnesen, M.G.; Feng, X.; Clark, R.A. Angiogenesis in Wound Healing. J. Investig. Dermatol. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef]
- DiPietro, L.A. Angiogenesis and Wound Repair: When Enough Is Enough. J. Leukoc. Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef]
- Castro-Combs, J.; Noguera, G.; Cano, M.; Yew, M.; Gehlbach, P.L.; Palmer, J.; Behrens, A. Corneal Wound Healing Is Modulated by Topical Application of Amniotic Fluid in an Ex Vivo Organ Culture Model. Exp. Eye Res. 2008, 87, 56–63. [Google Scholar] [CrossRef]
- Takigawa, T.; Shiota, K. Amniotic Fluid Induces Rapid Epithelialization in the Experimentally Ruptured Fetal Mouse Palate--Implications for Fetal Wound Healing. Int. J. Dev. Biol. 2007, 51, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Van Eps, J.L.; Boada, C.; Scherba, J.C.; Zavlin, D.; Arrighetti, N.; Shi, A.; Wang, X.; Tasciotti, E.; Buell, J.F.; Ellsworth, W.A.; et al. Amniotic Fluid Allograft Enhances the Host Response to Ventral Hernia Repair Using Acellular Dermal Matrix. J. Tissue Eng. Regen Med 2021, 15, 1092–1104. [Google Scholar] [CrossRef] [PubMed]
- Ozgenel, G.Y.; Filiz, G. Effects of Human Amniotic Fluid on Peripheral Nerve Scarring and Regeneration in Rats. J. Neurosurg 2003, 98, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Ozgenel, G.Y.; Filiz, G.; Ozcan, M. Effects of Human Amniotic Fluid on Cartilage Regeneration from Free Perichondrial Grafts in Rabbits. Br. J. Plast. Surg. 2004, 57, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Ozgenel, G.Y. The Influence of Human Amniotic Fluid on the Potential of Rabbit Ear Perichondrial Flaps to Form Cartilage Tissue. Br. J. Plast. Surg. 2002, 55, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Ozgenel, G.Y.; Samli, B.; Ozcan, M. Effects of Human Amniotic Fluid on Peritendinous Adhesion Formation and Tendon Healing after Flexor Tendon Surgery in Rabbits. J. Hand Surg. Am. 2001, 26, 332–339. [Google Scholar] [CrossRef] [PubMed]
- de Girolamo, L.; Morlin Ambra, L.F.; Perucca Orfei, C.; McQuilling, J.P.; Kimmerling, K.A.; Mowry, K.C.; Johnson, K.A.; Phan, A.T.; Whited, J.L.; Gomoll, A.H. Treatment with Human Amniotic Suspension Allograft Improves Tendon Healing in a Rat Model of Collagenase-Induced Tendinopathy. Cells 2019, 8, 1411. [Google Scholar] [CrossRef] [PubMed]
- Kavakli, K.; Gurkok, S.; Caylak, H.; Genc, O.; Gamsizkan, M.; Yucel, O.; Karasahin, E.; Gozubuyuk, A.; Tasci, C. Effects of Human Amniotic Fluid on Costal Cartilage Regeneration (an Experimental Study). Thorac. Cardiovasc. Surg. 2011, 59, 484–489. [Google Scholar] [CrossRef]
- Kimmerling, K.A.; Gomoll, A.H.; Farr, J.; Mowry, K.C. Amniotic Suspension Allograft Improves Pain and Function in a Rat Meniscal Tear-Induced Osteoarthritis Model. Arthritis Res. Ther. 2022, 24, 63. [Google Scholar] [CrossRef]
- Kimmerling, K.A.; Gomoll, A.H.; Farr, J.; Mowry, K.C. Amniotic Suspension Allograft Modulates Inflammation in a Rat Pain Model of Osteoarthritis. J. Orthop. Res. 2020, 38, 1141–1149. [Google Scholar] [CrossRef]
- Oner, M.; Dulgeroglu, T.C.; Karaman, I.; Guney, A.; Kafadar, I.H.; Erdem, S. The Effects of Human Amniotic Fluid and Different Bone Grafts on Vertebral Fusion in an Experimental Rat Model. Curr. Ther. Res Clin. Exp. 2015, 77, 35–39. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Aydin, H.; Saraçoğlu, M.; Kerimoğlu, G.; Kerimoğlu, S.; Topbaş, M. Effects of human amniotic fluid on posterolateral spinal fusion: An experimental preliminary study. Eklem Hastalik. Cerrahisi 2011, 22, 166–171. [Google Scholar] [PubMed]
- Karaçal, N.; Koşucu, P.; Cobanglu, U.; Kutlu, N. Effect of Human Amniotic Fluid on Bone Healing. J. Surg. Res. 2005, 129, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Büyük, B.; Demirci, T.; Adalı, Y.; Eroğlu, H.A. A New Organ Preservation Solution for Static Cold Storage of the Liver. Amniotic Fluid. Acta Cir. Bras. 2019, 34, e201900402. [Google Scholar] [CrossRef]
- Wu, M.-Y.; Yiang, G.-T.; Liao, W.-T.; Tsai, A.P.-Y.; Cheng, Y.-L.; Cheng, P.-W.; Li, C.-Y.; Li, C.-J. Current Mechanistic Concepts in Ischemia and Reperfusion Injury. Cell Physiol. Biochem. 2018, 46, 1650–1667. [Google Scholar] [CrossRef]
- Lee, Y.S.; Javan, H.; Reems, J.-A.; Li, L.; Lusty, J.; Schaaf, C.I.; Pierce, J.; Phillips, J.D.; Selzman, C.H. Acellular Human Amniotic Fluid Protects the Ischemic-Reperfused Rat Myocardium. Am. J. Physiol. Heart Circ. Physiol. 2022, 322, H406–H416. [Google Scholar] [CrossRef] [PubMed]
- Selzman, C.H.; Tonna, J.E.; Pierce, J.; Vargas, C.; Skidmore, C.; Lewis, G.; Hatton, N.D.; Phillips, J.D. A Pilot Trial of Human Amniotic Fluid for the Treatment of COVID-19. BMC Res. Notes 2021, 14, 32. [Google Scholar] [CrossRef]
- Tonna, J.E.; Pierce, J.; Hatton, N.; Lewis, G.; Phillips, J.D.; Messina, A.; Skidmore, C.R.; Taylor, K.; Selzman, C.H. Safety and Feasibility of Using Acellular Sterile Filtered Amniotic Fluid as a Treatment for Patients with COVID-19: Protocol for a Randomised, Double-Blinded, Placebo-Controlled Clinical Trial. BMJ Open 2021, 11, e045162. [Google Scholar] [CrossRef]
- Bellio, M.A.; Bennett, C.; Arango, A.; Khan, A.; Xu, X.; Barrera, C.; Friedewald, V.; Mitrani, M.I. Proof-of-Concept Trial of an Amniotic Fluid-Derived Extracellular Vesicle Biologic for Treating High Risk Patients with Mild-to-Moderate Acute COVID-19 Infection. Biomater. Biosyst. 2021, 4, 100031. [Google Scholar] [CrossRef]
- Quinet, M.T.; Raghavan, M.; Morris, E.; Smith, T.; Cook, H.; Walter, N.; Shuler, M. Effectiveness of Amniotic Fluid Injection in the Treatment of Trigger Finger: A Pilot Study. J. Hand Surg. Glob. Online 2020, 2, 301–305. [Google Scholar] [CrossRef]
- Farr, J.; Gomoll, A.H.; Yanke, A.B.; Strauss, E.J.; Mowry, K.C. ASA Study Group A Randomized Controlled Single-Blind Study Demonstrating Superiority of Amniotic Suspension Allograft Injection Over Hyaluronic Acid and Saline Control for Modification of Knee Osteoarthritis Symptoms. J. Knee Surg. 2019, 32, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Werber, B.; Martin, E. A Prospective Study of 20 Foot and Ankle Wounds Treated with Cryopreserved Amniotic Membrane and Fluid Allograft. J. Foot Ankle. Surg. 2013, 52, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Mitrani, M.I.; Bellio, M.A.; Sagel, A.; Saylor, M.; Kapp, W.; VanOsdol, K.; Haskell, G.; Stewart, D.; Abdullah, Z.; Santos, I.; et al. Case Report: Administration of Amniotic Fluid-Derived Nanoparticles in Three Severely Ill COVID-19 Patients. Front. Med. 2021, 8, 583842. [Google Scholar] [CrossRef] [PubMed]
- Ditmars, F.S.; Lind, R.A.; Broderick, T.C.; Fagg, W.S. Safety and Efficacy of Acellular Human Amniotic Fluid and Membrane in the Treatment of Non-Healing Wounds in a Patient with Chronic Venous Insufficiency. SAGE Open Med. Case Rep. 2022, 10, 2050313X221100882. [Google Scholar] [CrossRef] [PubMed]
- Wollmuth, C.; Foti, T.; Pergolizzi, J.; Tribuiani, A. Human Amniotic Fluid Injection as a Treatment for Diabetic Foot Ulceration: A Case Report. Int. J. Case Rep. Clin. Images 2019, 1, 111. [Google Scholar] [CrossRef]
- Bhattacharya, N.; Bhattacharya, P.S. and A. Application of Freshly Collected Amniotic Membrane and Amniotic Fluid in Arthritis and Wound Healing. MJA 2018, 2, 38–41. [Google Scholar] [CrossRef][Green Version]
- Bhattacharya, N. Clinical Use of Amniotic Fluid in Osteoarthritis: A Source of Cell Therapy. In Regenerative Medicine Using Pregnancy-Specific Biological Substances; Bhattacharya, N., Stubblefield, P., Eds.; Springer: London, UK, 2011; pp. 395–403. ISBN 978-1-84882-718-9. [Google Scholar]
- Krishnamoorthy, V.; Ramaiah, R.; Bhananker, S.M. Pediatric Burn Injuries. Int. J. Crit. Illn. Inj. Sci. 2012, 2, 128–134. [Google Scholar] [CrossRef]
- Darelli-Anderson, A.M.; South, S.; Lewis, G.M. 557 Amniotic Fluid Injections in Chronic Non-Healing Wounds in Pediatric Patients: A Case Series. J. Burn. Care Res. 2021, 42, S127–S128. [Google Scholar] [CrossRef]
- Vines, J.B.; Aliprantis, A.O.; Gomoll, A.H.; Farr, J. Cryopreserved Amniotic Suspension for the Treatment of Knee Osteoarthritis. J. Knee Surg. 2016, 29, 443–450. [Google Scholar] [CrossRef]
- Gomoll, A.H.; Farr, J.; Cole, B.J.; Flanigan, D.C.; Lattermann, C.; Mandelbaum, B.R.; Strickland, S.M.; Zaslav, K.R.; Kimmerling, K.A.; Mowry, K.C. Safety and Efficacy of an Amniotic Suspension Allograft Injection Over 12 Months in a Single-Blinded, Randomized Controlled Trial for Symptomatic Osteoarthritis of the Knee. Arthroscopy 2021, 37, 2246–2257. [Google Scholar] [CrossRef]
- Meadows, M.C.; Elisman, K.; Nho, S.J.; Mowry, K.; Safran, M.R. A Single Injection of Amniotic Suspension Allograft Is Safe and Effective for Treatment of Mild to Moderate Hip Osteoarthritis: A Prospective Study. Arthroscopy 2022, 38, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A. Allogenic Amniotic Tissue for Treatment of Knee and Hip Osteoarthritis. Pharmaceuticals 2022, 15, 404. [Google Scholar] [CrossRef] [PubMed]
- Jay, R.M.; Huish, J.P.; Wray, J.H. Amniotic Membrane in Clinical Medicine: History, Current Status, and Future Use. Extracell. Matrix-Deriv. Implant. Clin. Med. 2016, 151–176. [Google Scholar] [CrossRef]
- Liang, L.; Li, W.; Ling, S.; Sheha, H.; Qiu, W.; Li, C.; Liu, Z. Amniotic Membrane Extraction Solution for Ocular Chemical Burns. Clin. Exp. Ophthalmol. 2009, 37, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.S.; Seo, S.J.; Hong, C.K. The Effect of Amniotic Membrane Extract on the Expression of INOS MRNA and Generation of NO in HaCaT Cell by Ultraviolet B Irradiation. Photodermatol. Photoimmunol. Photomed. 2002, 18, 280–286. [Google Scholar] [CrossRef]
- Shayan Asl, N.; Nejat, F.; Mohammadi, P.; Nekoukar, A.; Hesam, S.; Ebrahimi, M.; Jadidi, K. Amniotic Membrane Extract Eye Drop Promotes Limbal Stem Cell Proliferation and Corneal Epithelium Healing. Cell J. 2019, 20, 459–468. [Google Scholar] [CrossRef]
- Dudok, D.V.; Nagdee, I.; Cheung, K.; Liu, H.; Vedovelli, L.; Ghinelli, E.; Kenyon, K.; Parapuram, S.; Hutnik, C.M. Effects of Amniotic Membrane Extract on Primary Human Corneal Epithelial and Limbal Cells. Clin. Exp. Ophthalmol. 2015, 43, 443–448. [Google Scholar] [CrossRef]
- Chen, M.; Chang, C.K.; Lin, S.Y.; Chen, M. A Pilot Study of the Short Term Effectiveness and Safety of Amniotic Fluid in Severe Dry Eye Disease. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 81–84. [Google Scholar]
- Cho, C.-K.J.; Shan, S.J.; Winsor, E.J.; Diamandis, E.P. Proteomics Analysis of Human Amniotic Fluid *. Mol. Cell. Proteom. 2007, 6, 1406–1415. [Google Scholar] [CrossRef]
- Bhatti, G.; Romero, R.; Gomez-Lopez, N.; Chaiworapongsa, T.; Jung, E.; Gotsch, F.; Pique-Regi, R.; Pacora, P.; Hsu, C.-D.; Kavdia, M.; et al. The Amniotic Fluid Proteome Changes with Gestational Age in Normal Pregnancy: A Cross-Sectional Study. Sci. Rep. 2022, 12, 601. [Google Scholar] [CrossRef]
- Kim, S.M.; Cho, B.K.; Kim, B.J.; Lee, H.Y.; Norwitz, E.R.; Kang, M.J.; Lee, S.M.; Park, C.W.; Jun, J.K.; Yi, E.C.; et al. The Amniotic Fluid Proteome Differs Significantly between Donor and Recipient Fetuses in Pregnancies Complicated by Twin-to-Twin Transfusion Syndrome. J. Korean Med. Sci. 2020, 35, e73. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Condition | Reference/Group | Efficacy | Other Comments |
|---|---|---|---|---|
| “A pilot trial of human amniotic fluid for the treatment of COVID-19” | COVID-19 | Selzman et al. 2021 [82,83] NCT04319731 Univ. of Utah | Higher dose patients had reduced C-reactive protein and improved clinical outcomes | Pilot study of 10 patients; 1 succumbed to COVID; last 6 patients received higher dose of AF; no AF-related AEs reported |
| “Proof-of-concept trial of an amniotic fluid-derived extracellular vesicle biologic for treating high risk patients with mild-to-moderate acute COVID-19 infection” | COVID-19 | Bellio et al. 2022 [84] NCT04657406 | Potentially effective use of cfAF to prevent severe disease progression in at-risk patients. | Pilot study of 8 patients; no serious AEs reported. |
| “Effectiveness of Amniotic Fluid Injection in the Treatment of Trigger Finger: A Pilot Study” | Stenosing tenosynovitis | Quinet et al. 2020 [85] NCT03583151 Athens Orthopedic Group | Half of patients noted improvements and did not receive alternative treatment. | Study included 111 digits from 96 patients with a significant reduction in pain, triggering/day, and DASH score. No AEs or complications discovered based on injection of AF. Study found AF helpful for patients with diabetes, a vulnerable population to tenosynovitis. |
| “A Randomized Controlled Single-Blind Study Demonstrating Superiority of Amniotic Suspension Allograft Injection Over Hyaluronic Acid and Saline Control for Modification of Knee Osteoarthritis Symptoms” | Osteoarthritis (OA) of the knee | Farr et al. 2019 [86] Knee Preservation and Cartilage Restoration Center; Hospital of Special Surgery; Rush Univ., NYU Lagnone Med., Organogenesis, Inc. | Demonstrated safety and trends towards improved pain and function. | Included 200 patients randomized 1:1:1 (Amniotic suspension:Hyaluronic Acid:saline) |
| “A prospective study of 20 foot and ankle wounds treated with cryopreserved amniotic membrane and fluid allograft” | Wound healing | Werber et al. 2013 [87] | May represent useful option to treat chronic diabetic foot wounds. | Clinical study using granulized amniotic membrane and fluid to treat chronic diabetic foot wounds in 20 patients. Patients were followed for 12-weeks with 90% (18/20 subjects) of wounds healed. None of the wounds (0/20) progressed to amputation. |
| “Case Report: Administration of Amniotic Fluid-Derived Nanoparticles in Three Severely Ill COVID-19 Patients” | COVID-19 | Mitrani et al. 2021 [88] | Treatment using cfAF appeared to be safe in n = 3 patients. | No adverse events associated with therapy. All three patients developed respiratory failure with hospitalization greater than 40 days and showed improved clinical status while in the ICU via resolution of acute delirium and reduction of inflammatory biomarkers. |
| Study | Condition | Reference/Group | Efficacy | Other Comments |
|---|---|---|---|---|
| “Processed Amniotic Fluid (pAF) for the Treatment of Chronic Wounds” | Chronic refractory wounds | ClinicalTrials.gov (accessed on 17 October 2022) NCT04438174 Univ. of Utah | No results posted | Primary objective aims to determine safety and efficacy of using pAF to treat chronic wounds; 1 mL/5 cm2 direct wound injection; limited to two injections |
| “pAF for the Treatment of Osteoarthritis” | Osteoarthritis (OA) of the knee | ClinicalTrials.gov (accessed on 17 October 2022) NCT04886960 Univ. of Utah | No results posted | Randomized double-blinded standard of care (steroid) vs. sterile AF for OA; 3 mL, one time injection |
| “Sterile Amniotic Fluid Filtrate Epidural Injection” | Spinal Stenosis | ClinicalTrial.gov (accessed on 17 October 2022); NCT04537026 Univ. of Utah | No results posted | Double-blinded randomized prospective study of sterile AF filtrate epidural injection for treatment of lumbosacral radicular pain due to spinal stenosis |
| “The Use of Autologous Amniotic Fluid at Cesarean Wound Closure” | Wound healing | ClinicalTrials.gov (accessed on 17 October 2022) NCT04359472 Recibio, Inc. and Duke Univ. | Not reported | Collection and reapplication of AF to cesarean wound upon skin closure |
| “Processed Amniotic Fluid (PAF) Drops After Photorefractive Keratectomy (PRK)” | Photorefractive Keratectomy | ClinicalTrials.gov (accessed on 17 October 2022) NCT04281004 Univ. of Utah | Not Reported | Randomized, double-masked, placebo-controlled study to determine: safety of AF, rate of re-epithelialization, reduction in pain, vision improvements, and effects on ocular surface staining and corneal regularity. |
| “Study for the Treatment of Ocular Chronic Graft-Versus-Host Disease (GVHD) with Amniotic Fluid Eye Drops (AFED)” | Ocular Chronic Graft-Versus-Host Disease | ClinicalTrials.gov (accessed on 17 October 2022) NCT03298815 Univ. of Utah | Not reported | Randomized, double-blinded, placebo-controlled study assessing efficacy of processed AF for patients with hematologic malignancy who have received allogenic stem cell transplantation that develop chronic GVHD of the eye. |
| “Dermacyte Amniotic Wound Care Liquid for the Treatment of Non-healing Venous Stasis Ulcers” | Venous stasis ulcer | ClinicalTrials.gov (accessed on 17 October 2022) NCT04647240 Merakris Therapeutics | Case study demonstrated safety and efficacy in the treatment of chronic venous stasis ulcers with Dermacyte liquid (cfAF) and membrane in a 65-year old patient [89]. | Randomized, double-blind, placebo controlled, two-part study. Part 1: 10 patients randomized 1:1 with Dermacyte Liquid (DL) once weekly or twice weekly to determine administration frequency for part 2. Part 2: 30 patients randomized 1:1 to receive DL or placebo (0.9% saline). Obtained FDA-approved IND. |
| “Efficacy of Amniotic Suspension Allograft in Patients with Osteoarthritis of the Knee” | Osteoarthritis (OA) of the knee | ClinicalTrials.gov (accessed on 17 October 2022) NCT04636229 Organogenesis | No results posted | Prospective, multicenter, randomized, double-blind, placebo-controlled Phase 3 study of ASA in patients with OA of the knee. Radom assignment (1:1) to receive either single intra-articular injection of 2 mL ASA (plus 2 mL saline) OR 4 mL normal saline. Estimated trial size of n = 474 subjects. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowen, C.M.; Ditmars, F.S.; Gupta, A.; Reems, J.-A.; Fagg, W.S. Cell-Free Amniotic Fluid and Regenerative Medicine: Current Applications and Future Opportunities. Biomedicines 2022, 10, 2960. https://doi.org/10.3390/biomedicines10112960
Bowen CM, Ditmars FS, Gupta A, Reems J-A, Fagg WS. Cell-Free Amniotic Fluid and Regenerative Medicine: Current Applications and Future Opportunities. Biomedicines. 2022; 10(11):2960. https://doi.org/10.3390/biomedicines10112960
Chicago/Turabian StyleBowen, Charles M., Frederick S. Ditmars, Ashim Gupta, Jo-Anna Reems, and William Samuel Fagg. 2022. "Cell-Free Amniotic Fluid and Regenerative Medicine: Current Applications and Future Opportunities" Biomedicines 10, no. 11: 2960. https://doi.org/10.3390/biomedicines10112960
APA StyleBowen, C. M., Ditmars, F. S., Gupta, A., Reems, J.-A., & Fagg, W. S. (2022). Cell-Free Amniotic Fluid and Regenerative Medicine: Current Applications and Future Opportunities. Biomedicines, 10(11), 2960. https://doi.org/10.3390/biomedicines10112960