
Neuroprotective Effects of Novel Treatments on Acute Optic Neuritis—A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria for Selecting Studies
2.2. Search Methods
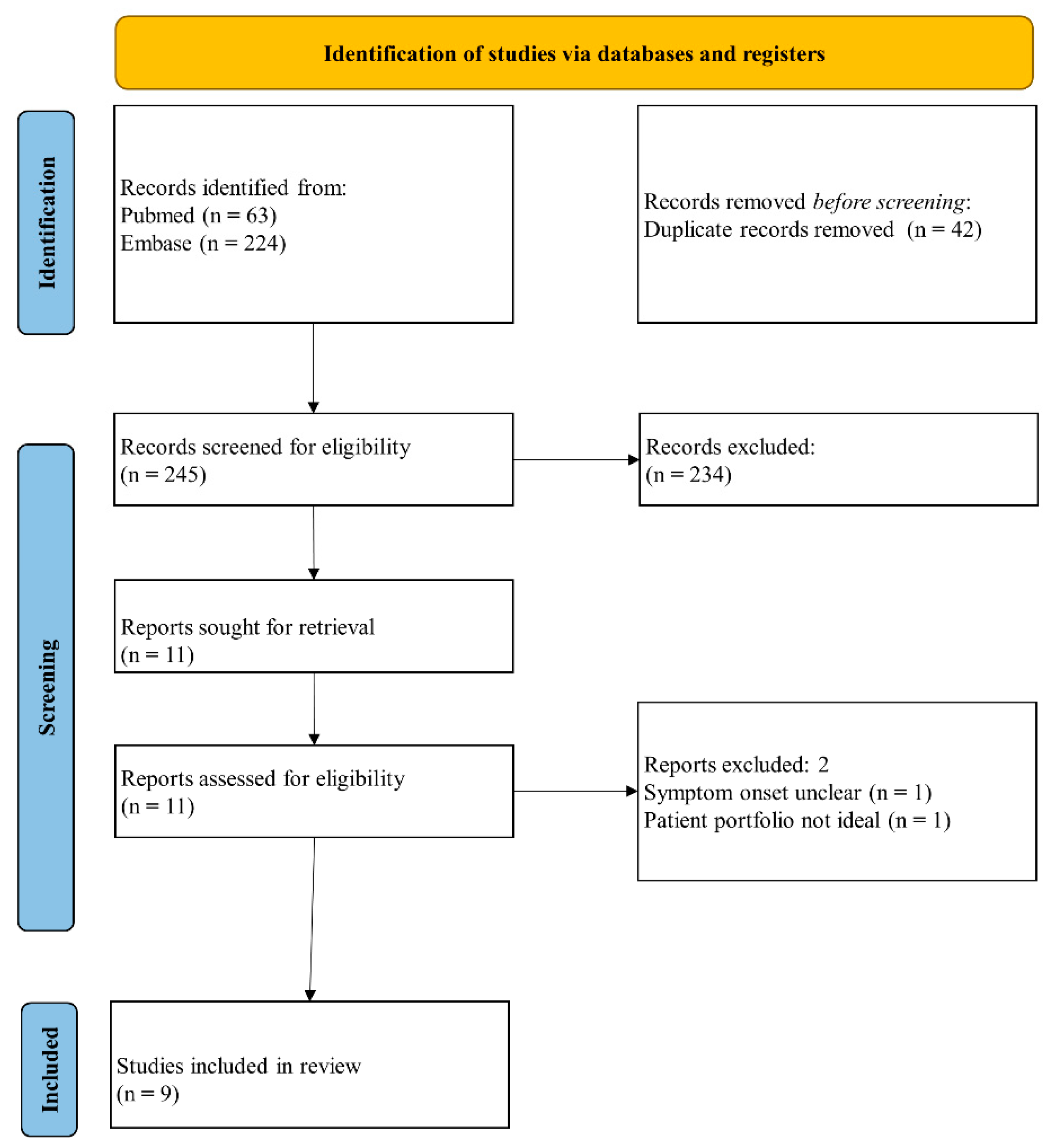
2.3. Data Screening, Data Extraction, and Risk of Bias Assessment
2.4. Data Synthesis and Analysis
3. Results
3.1. Study Characteristics
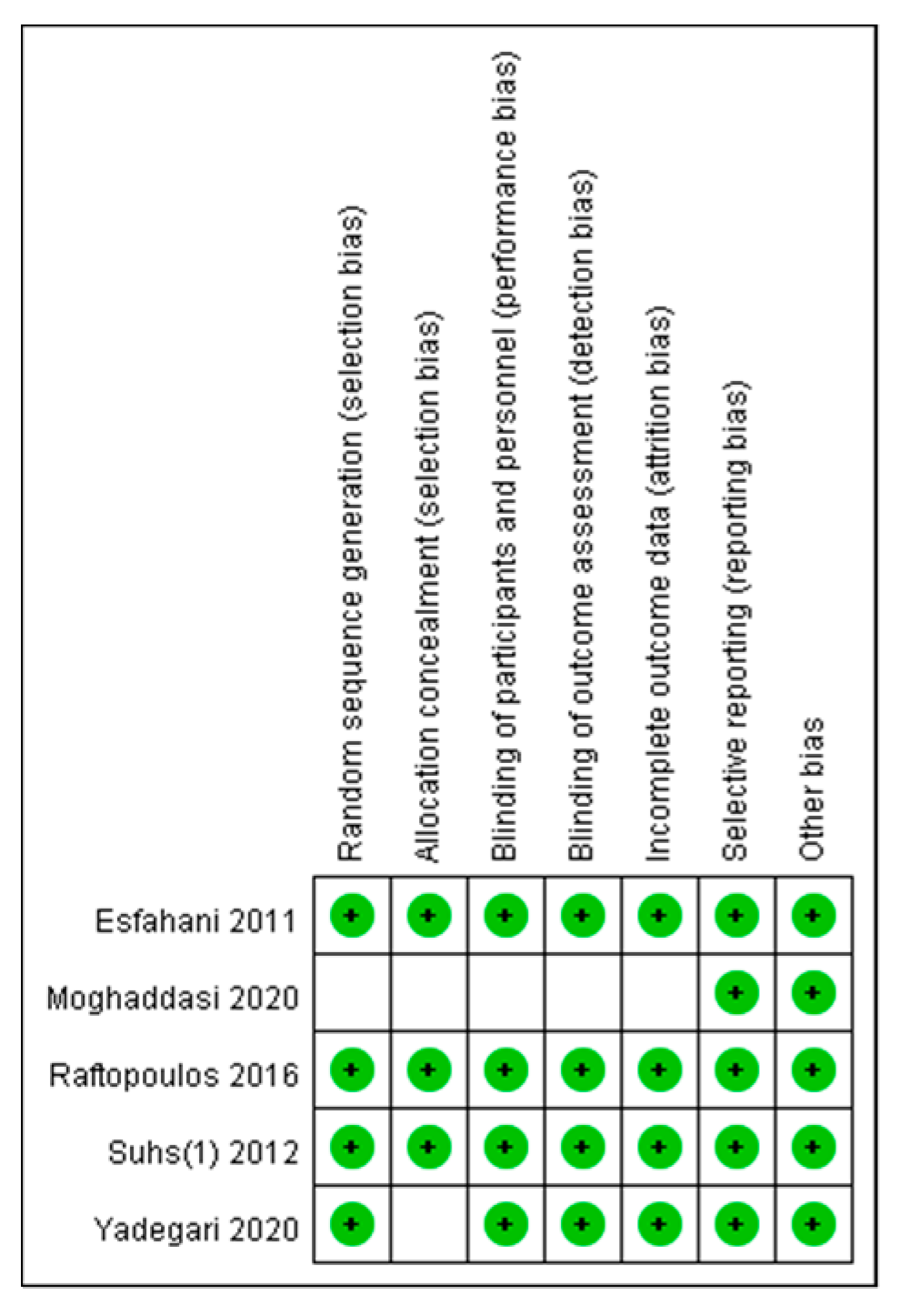
3.2. Risk of Bias
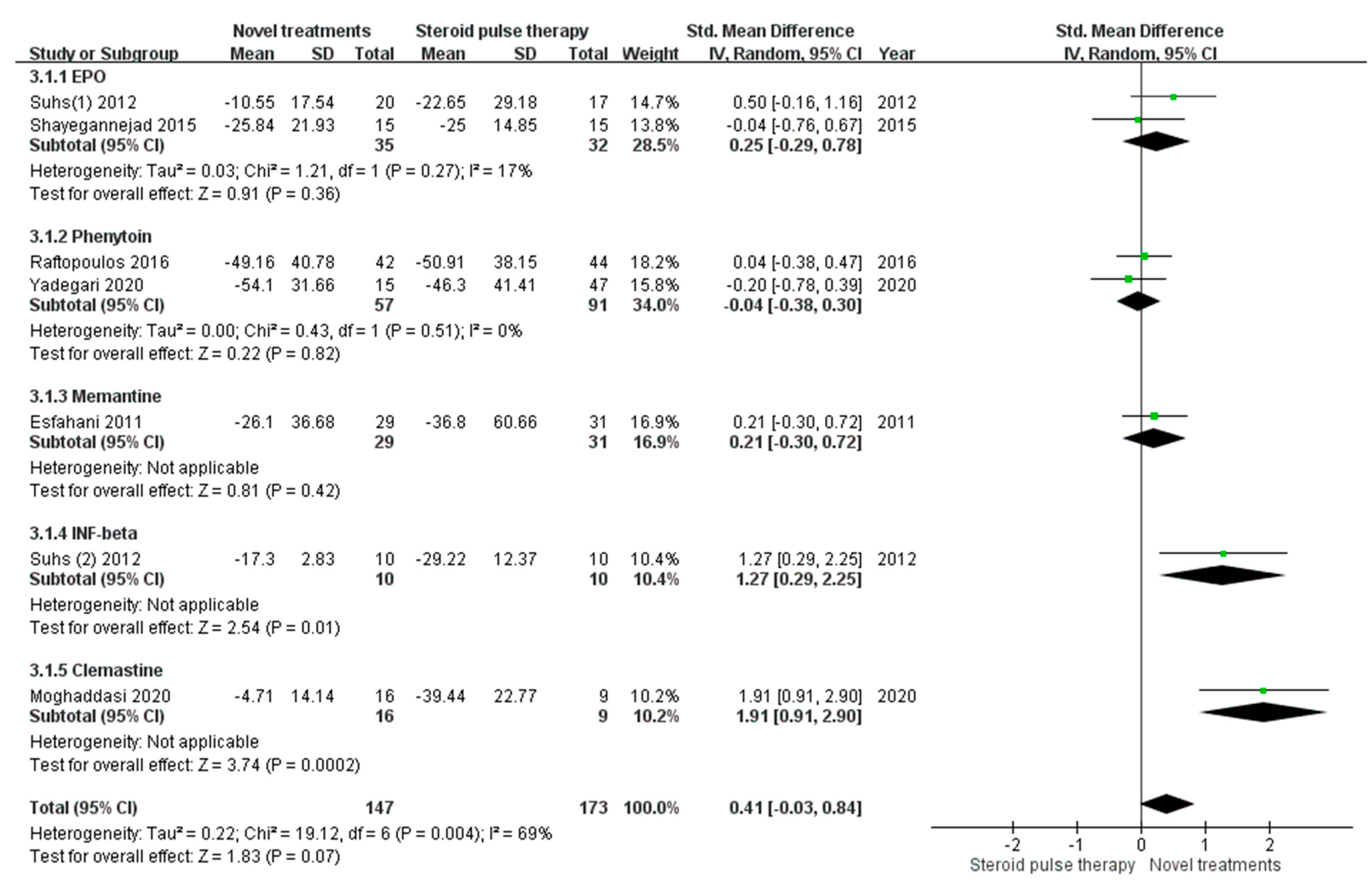
3.3. Mean Differences in RNFL Thickness Compared with Baseline Data of the Affected Eye
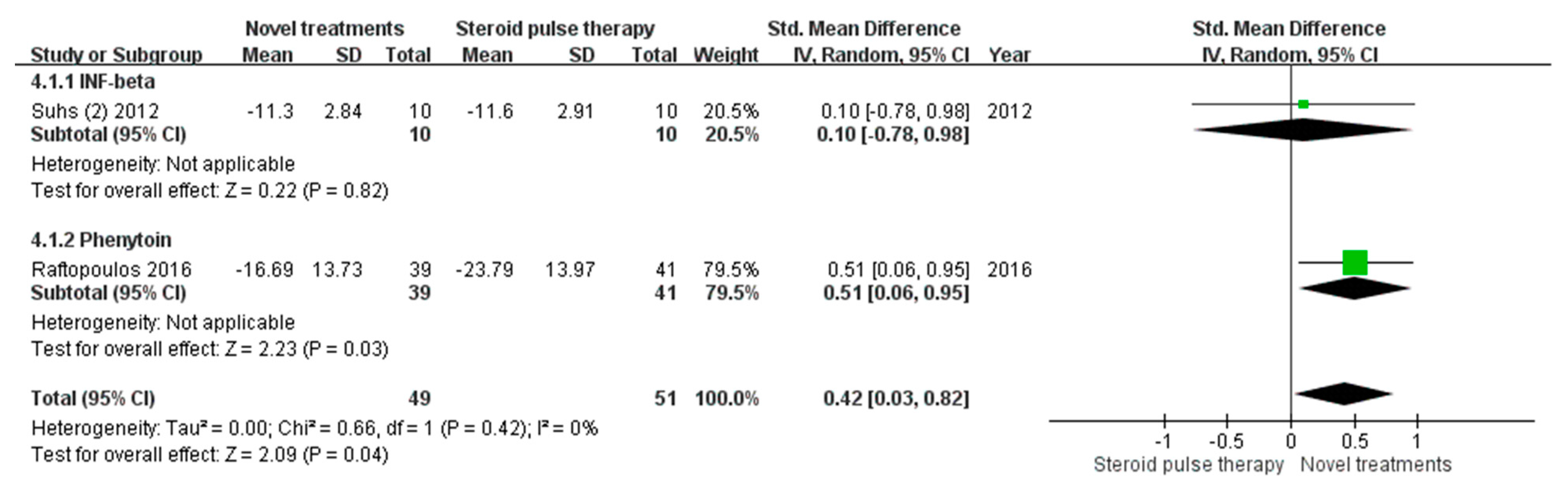
3.4. Mean Differences in RNFL Thickness Compared with Baseline Data of the Unaffected Eye
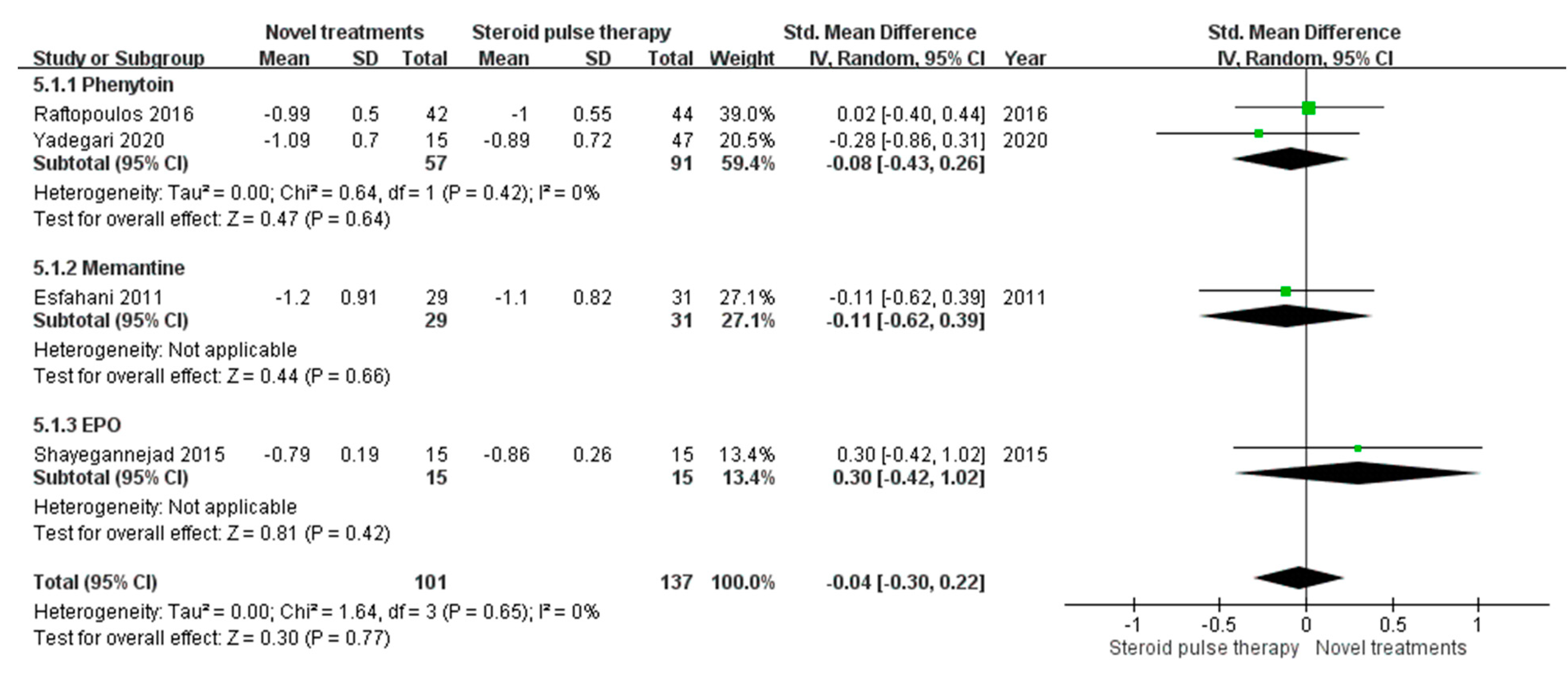
3.5. Mean Difference in LogMAR VA
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Abel, A.; McClelland, C.; Lee, M.S. Critical review: Typical and atypical optic neuritis. Surv. Ophthalmol. 2019, 64, 770–779. [Google Scholar] [CrossRef]
- Toosy, A.T.; Mason, D.F.; Miller, D.H. Optic neuritis. Lancet Neurol. 2014, 13, 83–99. [Google Scholar] [CrossRef]
- Beck, R.W.; Cleary, P.A.; Backlund, J.C. The course of visual recovery after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Ophthalmology 1994, 101, 1771–1778. [Google Scholar] [CrossRef]
- Frederiksen, J.L.; Sørensen, T.L.; Sellebjerg, F.T. Residual symptoms and signs after untreated acute optic neuritis. A one-year follow-up. Acta Ophthalmol. Scand. 1997, 75, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Cleary, P.A.; Anderson, M.M., Jr.; Keltner, J.L.; Shults, W.T.; Kaufman, D.I.; Buckley, E.G.; Corbett, J.J.; Kupersmith, M.J.; Miller, N.R.; et al. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N. Engl. J. Med. 1992, 326, 581–588. [Google Scholar] [CrossRef]
- Hickman, S.J.; Dalton, C.M.; Miller, D.H.; Plant, G.T. Management of acute optic neuritis. Lancet 2002, 360, 1953–1962. [Google Scholar] [CrossRef]
- Lee, T.H.; Ji, Y.S.; Park, S.W.; Heo, H. Retinal ganglion cell and axonal loss in optic neuritis: Risk factors and visual functions. Eye 2017, 31, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Costello, F.; Coupland, S.; Hodge, W.; Lorello, G.R.; Koroluk, J.; Pan, Y.I.; Freedman, M.S.; Zackon, D.H.; Kardon, R.H. Quantifying axonal loss after optic neuritis with optical coherence tomography. Ann. Neurol. 2006, 59, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Petzold, A.; de Boer, J.F.; Schippling, S.; Vermersch, P.; Kardon, R.; Green, A.; Calabresi, P.A.; Polman, C. Optical coherence tomography in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 921–932. [Google Scholar] [CrossRef] [Green Version]
- Frohman, E.; Costello, F.; Zivadinov, R.; Stuve, O.; Conger, A.; Winslow, H.; Trip, A.; Frohman, T.; Balcer, L. Optical coherence tomography in multiple sclerosis. Lancet Neurol. 2006, 5, 853–863. [Google Scholar] [CrossRef]
- Syc, S.B.; Saidha, S.; Newsome, S.D.; Ratchford, J.N.; Levy, M.; Ford, E.; Crainiceanu, C.M.; Durbin, M.K.; Oakley, J.D.; Meyer, S.A.; et al. Optical coherence tomography segmentation reveals ganglion cell layer pathology after optic neuritis. Brain 2012, 135 Pt 2, 521–533. [Google Scholar] [CrossRef]
- Britze, J.; Pihl-Jensen, G.; Frederiksen, J.L. Retinal ganglion cell analysis in multiple sclerosis and optic neuritis: A systematic review and meta-analysis. J. Neurol. 2017, 264, 1837–1853. [Google Scholar] [CrossRef] [PubMed]
- Sühs, K.W.; Hein, K.; Sättler, M.B.; Görlitz, A.; Ciupka, C.; Scholz, K.; Käsmann-Kellner, B.; Papanagiotou, P.; Schäffler, N.; Restemeyer, C.; et al. A randomized, double-blind, phase 2 study of erythropoietin in optic neuritis. Ann. Neurol. 2012, 72, 199–210. [Google Scholar] [CrossRef]
- Yadegari, S.; Gholizade, A.; Ghahvehchian, H.; Aghsaei Fard, M. Effect of phenytoin on retinal ganglion cells in acute isolated optic neuritis. Neurol. Sci. 2020, 41, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Raftopoulos, R.; Hickman, S.J.; Toosy, A.; Sharrack, B.; Mallik, S.; Paling, D.; Altmann, D.R.; Yiannakas, M.C.; Malladi, P.; Sheridan, R.; et al. Phenytoin for neuroprotection in patients with acute optic neuritis: A randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2016, 15, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Liu, K.; Tan, X.; Zhou, L.; Zhang, Y.; Liu, X.; Fu, Y.; Qiu, W.; Yang, H. Remedial Effect of Intravenous Cyclophosphamide in Corticosteroid-Refractory Patients in the Acute Phase of Neuromyelitis Optica Spectrum Disorder-Related Optic Neuritis. Front. Neurol. 2021, 11, 612097. [Google Scholar] [CrossRef]
- Salari, M.; Janghorbani, M.; Etemadifar, M.; Dehghani, A.; Razmjoo, H.; Naderian, G. Effects of vitamin D on retinal nerve fiber layer in vitamin D deficient patients with optic neuritis: Preliminary findings of a randomized, placebo-controlled trial. J. Res. Med. Sci. 2015, 20, 372–378. [Google Scholar] [PubMed]
- Esfahani, M.R.; Harandi, Z.A.; Movasat, M.; Nikdel, M.; Adelpour, M.; Momeni, A.; Merat, H.; Fard, M.A. Memantine for axonal loss of optic neuritis. Graefes Arch. Clin. Exp. Ophthalmol. 2012, 250, 863–869. [Google Scholar] [CrossRef]
- Sühs, K.W.; Hein, K.; Pehlke, J.R.; Käsmann-Kellner, B.; Diem, R. Retinal nerve fibre layer thinning in patients with clinically isolated optic neuritis and early treatment with interferon-beta. PLoS ONE 2012, 7, e51645. [Google Scholar] [CrossRef]
- Shayegannejad, V.; Shahzamani, S.; Dehghani, A.; Dast Borhan, Z.; Rahimi, M.; Mirmohammadsadeghi, A. A double-blind, placebo-controlled trial of adding erythropoietin to intravenous methylprednisolone for the treatment of unilateral acute optic neuritis of unknown or demyelinative origin. Graefes Arch. Clin. Exp. Ophthalmol 2015, 253, 797–801. [Google Scholar] [CrossRef]
- Moghaddasi, M.; Nabovvati, M.; Koushki, A.; Soltansanjari, M.; Sardarinia, M.; Mohebi, N.; Rabani, S. Randomized control trial of evaluation of Clemastine effects on visual evoked potential, nerve fiber layer and ganglion cell layer complex in patients with optic neuritis. Clin. Neurol. Neurosurg. 2020, 193, 105741. [Google Scholar] [CrossRef]
- Sergott, R.C.; Bennett, J.L.; Rieckmann, P.; Montalban, X.; Mikol, D.; Freudensprung, U.; Plitz, T.; van Beek, J.; ATON Trial Group. ATON: Results from a Phase II randomized trial of the B-cell-targeting agent atacicept in patients with optic neuritis. J. Neurol. Sci. 2015, 351, 174–178. [Google Scholar] [CrossRef]
- McKee, J.B.; Cottriall, C.L.; Elston, J.; Epps, S.; Evangelou, N.; Gerry, S.; Kennard, C.; Kong, Y.; Koelewyn, A.; Kueker, W.; et al. Amiloride does not protect retinal nerve fibre layer thickness in optic neuritis in a phase 2 randomised controlled trial. Mult. Scler. J. 2019, 25, 246–255. [Google Scholar] [CrossRef]
- Rodriguez, M.; Siva, A.; Cross, S.A.; O’Brien, P.C.; Kurland, L.T. Optic neuritis: A population-based study in Olmsted County, Minnesota. Neurology 1995, 45, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Petzold, A.; Braithwaite, T.; van Oosten, B.W.; Balk, L.; Martinez-Lapiscina, E.H.; Wheeler, R.; Wiegerinck, N.; Waters, C.; Plant, G.T. Case for a new corticosteroid treatment trial in optic neuritis: Review of updated evidence. J. Neurol. Neurosurg. Psychiatry 2020, 91, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Petzold, A.; Balcer, L.J.; Calabresi, P.A.; Costello, F.; Frohman, T.C.; Frohman, E.M.; Martinez-Lapiscina, E.H.; Green, A.J.; Kardon, R.; Outteryck, O.; et al. Retinal layer segmentation in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2017, 16, 797–812. [Google Scholar] [CrossRef] [Green Version]
- Reisberg, B.; Doody, R.; Stöffler, A.; Schmitt, F.; Ferris, S.; Möbius, H.J.; Memantine Study Group. Memantine in moderate-to-severe Alzheimer’s disease. N. Engl. J. Med. 2003, 348, 1333–1341. [Google Scholar] [CrossRef]
- Diem, R.; Sättler, M.B.; Merkler, D.; Demmer, I.; Maier, K.; Stadelmann, C.; Ehrenreich, H.; Bähr, M. Combined therapy with methylprednisolone and erythropoietin in a model of multiple sclerosis. Brain 2005, 128 Pt 2, 375–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comi, G.; Filippi, M.; Barkhof, F.; Durelli, L.; Edan, G.; Fernández, O.; Hartung, H.; Seeldrayers, P.; Sørensen, P.S.; Rovaris, M.; et al. Effect of early interferon treatment on conversion to definite multiple sclerosis: A randomised study. Lancet 2001, 357, 1576–1582. [Google Scholar] [CrossRef]
- Lo, A.C.; Saab, C.Y.; Black, J.A.; Waxman, S.G. Phenytoin protects spinal cord axons and preserves axonal conduction and neurological function in a model of neuroinflammation in vivo. J. Neurophysiol. 2003, 90, 3566–3571. [Google Scholar] [CrossRef] [Green Version]
- Green, A.J.; Gelfand, J.M.; Cree, B.A.; Bevan, C.; Boscardin, W.J.; Mei, F.; Inman, J.; Arnow, S.; Devereux, M.; Abounasr, A.; et al. Clemastine fumarate as a remyelinating therapy for multiple sclerosis (ReBUILD): A randomised, controlled, double-blind, crossover trial. Lancet 2017, 390, 2481–2489. [Google Scholar] [CrossRef] [Green Version]
- Naismith, R.T.; Tutlam, N.T.; Xu, J.; Shepherd, J.B.; Klawiter, E.C.; Song, S.K.; Cross, A.H. Optical coherence tomography is less sensitive than visual evoked potentials in optic neuritis. Neurology 2009, 73, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Diem, R.; Hobom, M.; Maier, K.; Weissert, R.; Storch, M.K.; Meyer, R.; Bähr, M. Methylprednisolone increases neuronal apoptosis during autoimmune CNS inflammation by inhibition of an endogenous neuroprotective pathway. J. Neurosci. 2003, 23, 6993–7000. [Google Scholar] [CrossRef]
- Henderson, A.P.; Altmann, D.R.; Trip, A.S.; Kallis, C.; Jones, S.J.; Schlottmann, P.G.; Garway-Heath, D.F.; Plant, G.T.; Miller, D.H. A serial study of retinal changes following optic neuritis with sample size estimates for acute neuroprotection trials. Brain 2010, 133, 2592–2602. [Google Scholar] [CrossRef] [Green Version]
- Saxena, R.; Bandyopadhyay, G.; Singh, D.; Singh, S.; Sharma, P.; Menon, V. Evaluation of changes in retinal nerve fiber layer thickness and visual functions in cases of optic neuritis and multiple sclerosis. Indian J. Ophthalmol. 2013, 61, 562–566. [Google Scholar] [CrossRef]
- Walter, S.D.; Ishikawa, H.; Galetta, K.M.; Sakai, R.E.; Feller, D.J.; Henderson, S.B.; Wilson, J.A.; Maguire, M.G.; Galetta, S.L.; Frohman, E.; et al. Ganglion cell loss in relation to visual disability in multiple sclerosis. Ophthalmology 2012, 119, 1250–1257. [Google Scholar] [CrossRef] [Green Version]
- Balk, L.J.; Coric, D.; Nij Bijvank, J.A.; Killestein, J.; Uitdehaag, B.M.; Petzold, A. Retinal atrophy in relation to visual functioning and vision-related quality of life in patients with multiple sclerosis. Mult. Scler. J. 2018, 24, 767–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippatou, A.G.; Mukharesh, L.; Saidha, S.; Calabresi, P.A.; Sotirchos, E.S. AQP4-IgG and MOG-IgG Related Optic Neuritis-Prevalence, Optical Coherence Tomography Findings, and Visual Outcomes: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 540156. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year). | Study Design | Study Population | Number of Patients | ON Symptom Onset | Novel Treatment | Control | OCT Outcome | Time of OCT f/u |
|---|---|---|---|---|---|---|---|---|
| Articles included in the final analysis | ||||||||
| Esfahani et al. (2011) [18] | RCT | New onset unilateral ON | 60 | ≤8 days | Memantine 5 mg for first week and 10 mg for the next 2 weeks after standard treatment | Placebo after standard treatment | pRNFL thickness | 3 months |
| Suhs et al. (1) (2012) [13] | RCT | New onset ON | 40 | ≤10 days | IV EPO 33,000 IU for 3 days after standard treatment | Placebo after standard treatment | RNFL thickness | 4 months |
| Suhs et al. (2) (2012) [19] | Cohort study | ON as CIS | 20 | ≤10 days | Subcutaneous INF-beta after standard treatment | Standard treatment | pRNFL thickness | 4 months |
| Shayegannejad et al. (2015) [20] | Cohort study | Unilateral ON of unknown or demyelinating origin | 30 | ≤10 days | IV EPO 33,000 IU for 3 days after standard treatment | Placebo after standard treatment | pRNFL thickness | 6 months |
| Raftopoulos et al. (2016) [15] | RCT | Unilateral demyelinating ON | 86 | ≤14 days | Oral phenytoin after standard treatment | Placebo after standard treatment | pRNFL thickness | 6 months |
| Moghaddasi et al. (2020) [21] | RCT | MS with acute ON | 25 | ≤30 days | Clemastine flumarate 1 mg twice a day for 3 months after standard treatment | Placebo after standard treatment | pRNFL and GCL complex thickness | 3 months |
| Yadegari et al. (2020) [14] | RCT | Unilateral ON | 74 | ≤14 days | Oral phenytoin for 3 months after standard treatment | Placebo after standard treatment | pRNFL and mGCIPL thickness | 6 months |
| Articles not included in the final analysis | ||||||||
| Sergott et al. (2015) [22] | RCT | Unilateral ON as CIS | 34 | ≤28 days | Subcutaneous atacicept for 9 months | +/−steroids | pRNFL thickness | 9 months |
| McKee et al. (2017) [23] | RCT | New onset unilateral ON | 48 | ≤28 days | Amiloride 10 mg daily for 3 months +/− steroids | +/−steroids | pRNFL thickness | 6 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, T.-H.; Lin, C.-W.; Chan, L.-W.; Tew, T.-B.; Chen, T.-C. Neuroprotective Effects of Novel Treatments on Acute Optic Neuritis—A Meta-Analysis. Biomedicines 2022, 10, 192. https://doi.org/10.3390/biomedicines10010192
Tsai T-H, Lin C-W, Chan L-W, Tew T-B, Chen T-C. Neuroprotective Effects of Novel Treatments on Acute Optic Neuritis—A Meta-Analysis. Biomedicines. 2022; 10(1):192. https://doi.org/10.3390/biomedicines10010192
Chicago/Turabian StyleTsai, Tsung-Hsien, Chao-Wen Lin, Li-Wei Chan, Teck-Boon Tew, and Ta-Ching Chen. 2022. "Neuroprotective Effects of Novel Treatments on Acute Optic Neuritis—A Meta-Analysis" Biomedicines 10, no. 1: 192. https://doi.org/10.3390/biomedicines10010192
APA StyleTsai, T.-H., Lin, C.-W., Chan, L.-W., Tew, T.-B., & Chen, T.-C. (2022). Neuroprotective Effects of Novel Treatments on Acute Optic Neuritis—A Meta-Analysis. Biomedicines, 10(1), 192. https://doi.org/10.3390/biomedicines10010192