
The Role of Neuropilin-2 in the Epithelial to Mesenchymal Transition of Colorectal Cancer: A Systematic Review

Abstract
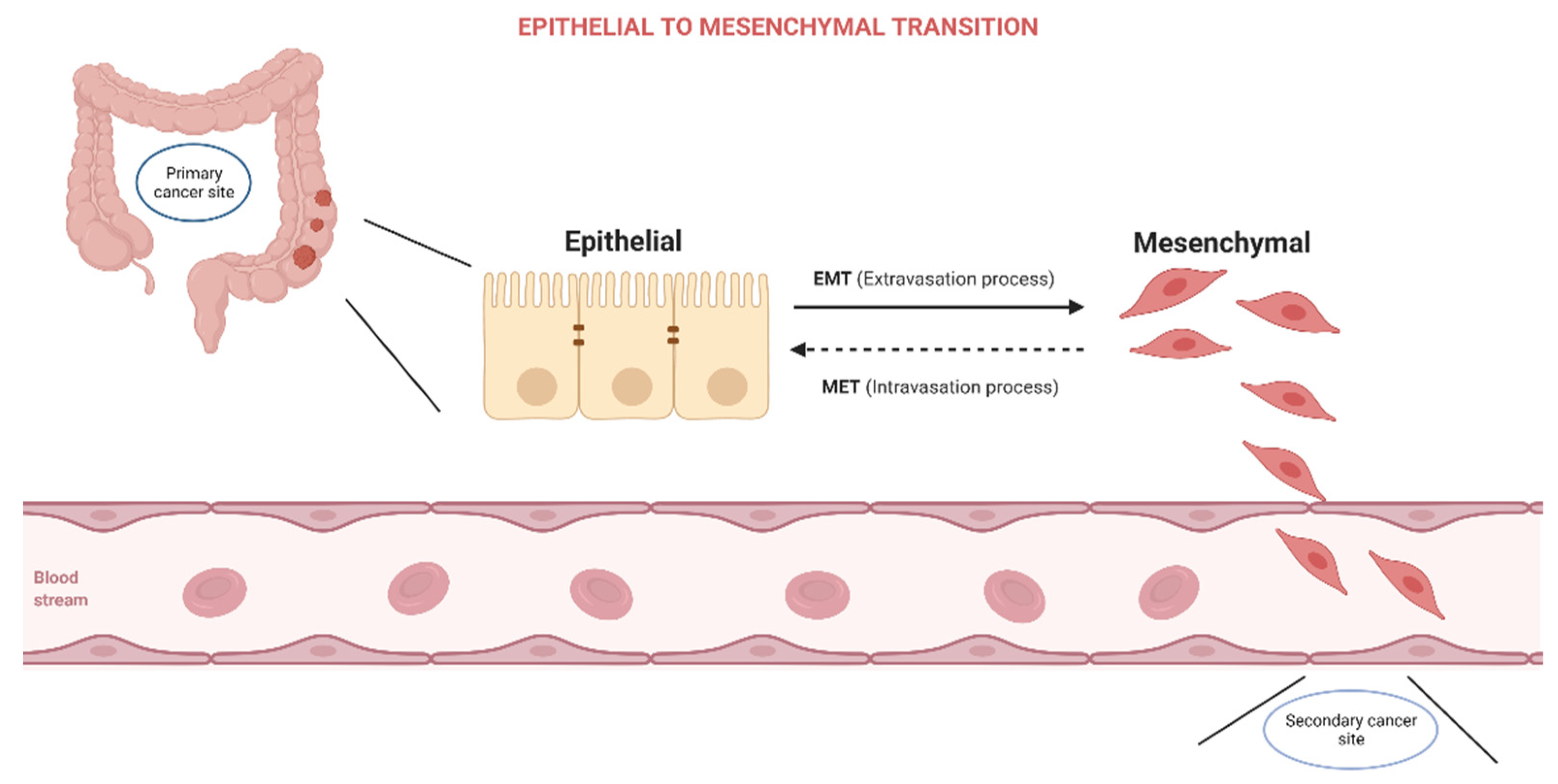
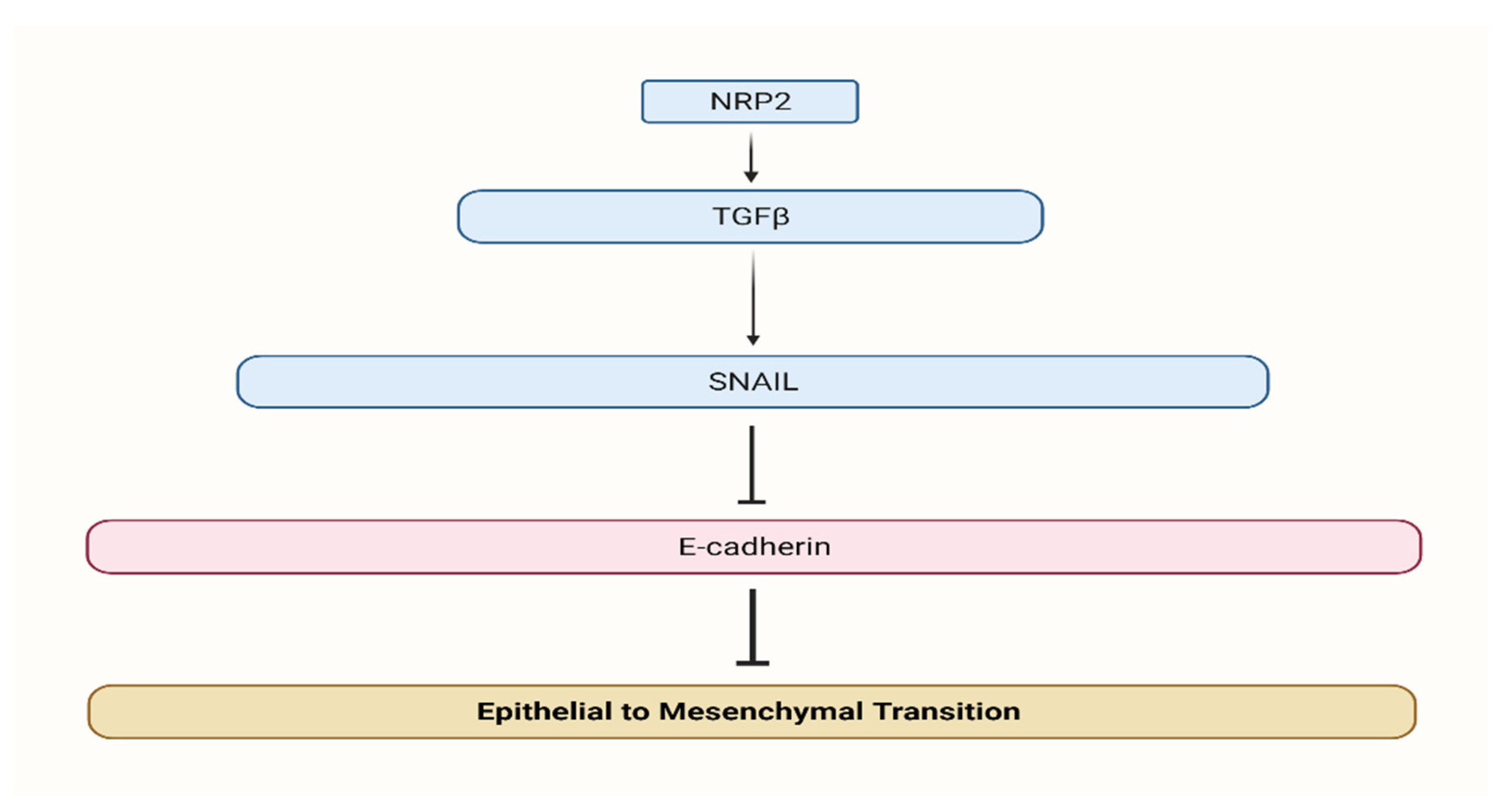
:1. Introduction
2. Materials and Methods
2.1. Data Source and Literature Search Strategy
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
- randomized controlled trials, cross-sectional, case-control, and cohort studies;
- studies with adult patients (18 years old or above) diagnosed with colorectal cancer;
- studies with NRP-2 data in relation to colorectal cancer;
- only peer-reviewed studies published in English with full text available.
2.4. Data Extraction
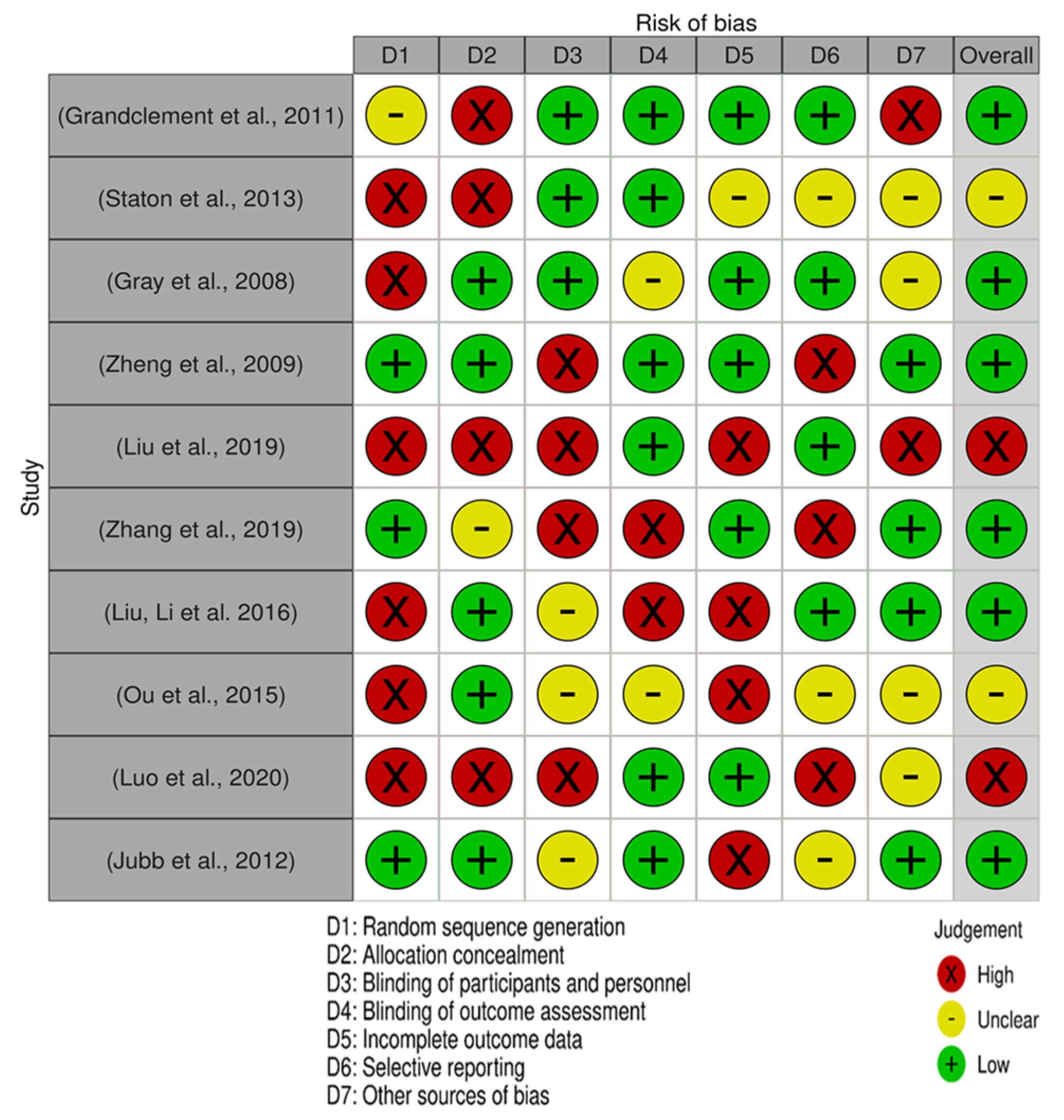
2.5. Quality Assessment—QUADAS 2 Tool
- “Traffic light” plots of the domain-level judgments for each result;
- Weighted bar plots of the distribution of risk-of-bias judgments within each bias domain.
3. Results
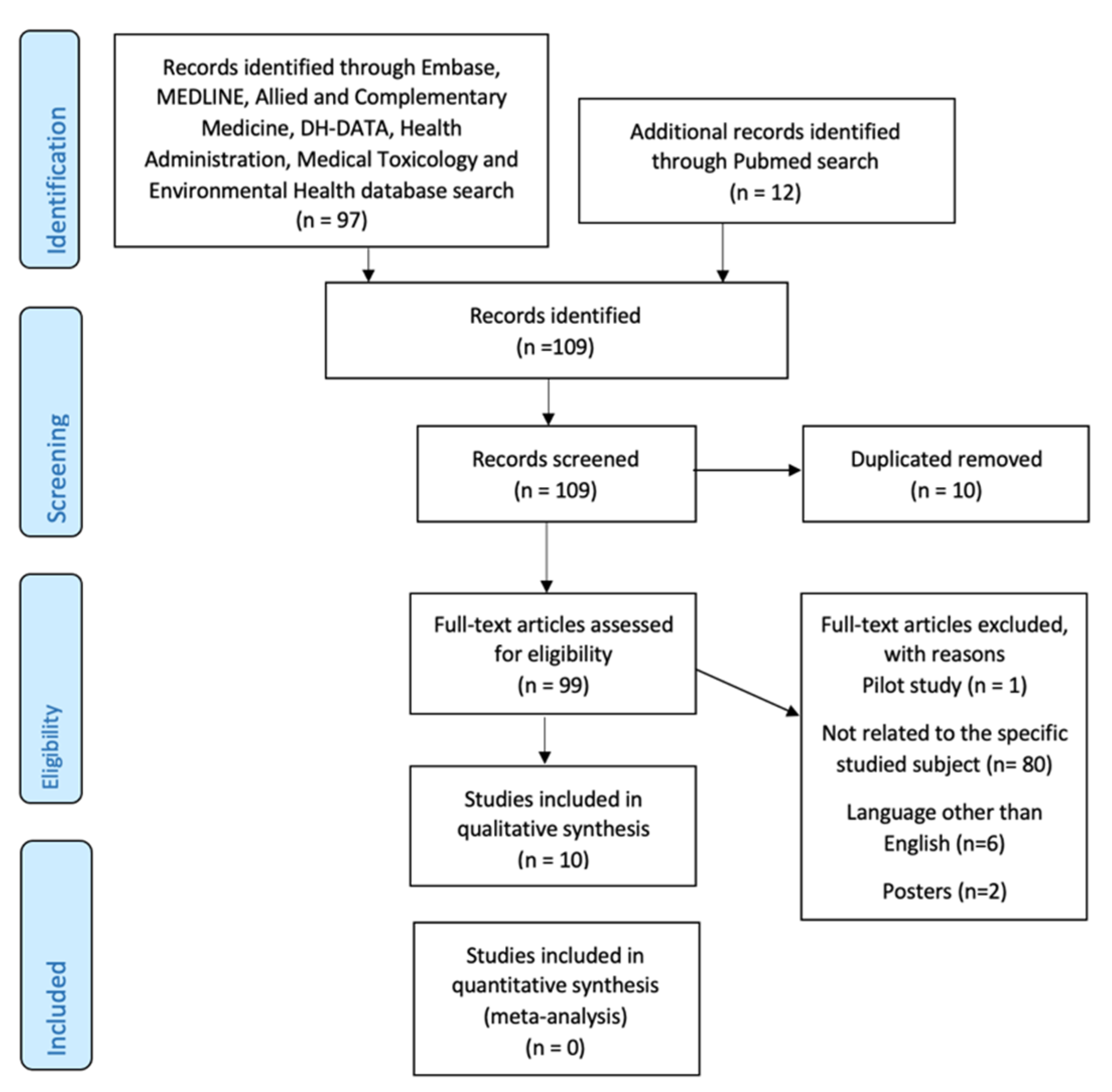
3.1. Overview of Selected Studies
3.2. Characteristics of the Selected Studies
3.3. NRP-2 up and Downregulation in CRC
3.4. Bias Assessment and Applicability Judgements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shook, D.; Keller, R. Mechanisms, Mechanics and Function of Epithelial–Mesenchymal Transitions in Early Development. Mech. Dev. 2003, 120, 1351–1383. [Google Scholar] [CrossRef]
- Kalluri, R. EMT: When Epithelial Cells Decide to Become Mesenchymal-like Cells. J. Clin. Investig. 2009, 119, 1417–1419. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.; Massagué, J. Epithelial-Mesenchymal Transitions. Cell 2004, 118, 277–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, J.H.; Yang, J. Epithelial–Mesenchymal Plasticity in Carcinoma Metastasis. Genes Dev. 2013, 27, 2192–2206. [Google Scholar] [CrossRef] [Green Version]
- Vu, T.; Datta, P. Regulation of EMT in Colorectal Cancer: A Culprit in Metastasis. Cancers 2017, 9, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dongre, A.; Weinberg, R.A. New Insights into the Mechanisms of Epithelial–Mesenchymal Transition and Implications for Cancer. Nat. Rev. Mol. Cell Biol. 2019, 20, 69–84. [Google Scholar] [CrossRef]
- Grandclement, C.; Pallandre, J.R.; Valmary Degano, S.; Viel, E.; Bouard, A.; Balland, J.; Rémy-Martin, J.-P.; Simon, B.; Rouleau, A.; Boireau, W.; et al. Neuropilin-2 Expression Promotes TGF-Β1-Mediated Epithelial to Mesenchymal Transition in Colorectal Cancer Cells. PLoS ONE 2011, 6, e20444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staton, C.; Kumar, I.; Reed, M.; Brown, N. Neuropilins in Physiological and Pathological Angiogenesis. J. Pathol. 2007, 212, 237–248. [Google Scholar] [CrossRef]
- Wang, J.; Huang, Y.; Zhang, J.; Xing, B.; Xuan, W.; Wang, H.; Huang, H.; Yang, J.; Tang, J. NRP-2 in Tumor Lymphangiogenesis and Lymphatic Metastasis. Cancer Lett. 2018, 418, 176–184. [Google Scholar] [CrossRef]
- Dutta, S.; Roy, S.; Polavaram, N.S.; Stanton, M.J.; Zhang, H.; Bhola, T.; Hönscheid, P.; Donohue, T.M.; Band, H.; Batra, S.K.; et al. Neuropilin-2 Regulates Endosome Maturation and EGFR Trafficking to Support Cancer Cell Pathobiology. Cancer Res. 2016, 76, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Handa, A.; Tokunaga, T.; Tsuchida, T.; Lee, Y.H.; Kijima, H.; Yamazaki, H.; Ueyama, Y.; Fukuda, H.; Nakamura, M. Neuropilin-2 Expression Affects the Increased Vascularization and Is a Prognostic Factor in Osteosarcoma. Int. J. Oncol. 2000, 17, 291–296. [Google Scholar] [CrossRef]
- Lacal, P.M.; Failla, C.M.; Pagani, E.; Odorisio, T.; Schietroma, C.; Falcinelli, S.; Zambruno, G.; D’Atri, S. Human Melanoma Cells Secrete and Respond to Placenta Growth Factor and Vascular Endothelial Growth Factor. J. Investig. Dermatol. 2000, 115, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, T.; Tokunaga, T.; Hatanaka, H.; Kijima, H.; Yamazaki, H.; Abe, Y.; Osamura, Y.; Inoue, H.; Ueyama, Y.; Nakamura, M. Neuropilin 1 and Neuropilin 2 Co-Expression Is Significantly Correlated with Increased Vascularity and Poor Prognosis in Nonsmall Cell Lung Carcinoma. Cancer 2002, 95, 2196–2201. [Google Scholar] [CrossRef]
- Tomizawa, Y.; Sekido, Y.; Kondo, M.; Gao, B.; Yokota, J.; Roche, J.; Drabkin, H.; Lerman, M.I.; Gazdar, A.F.; Minna, J.D. Inhibition of Lung Cancer Cell Growth and Induction of Apoptosis after Reexpression of 3p21.3 Candidate Tumor Suppressor Gene SEMA3B. Proc. Natl. Acad. Sci. USA 2001, 98, 13954–13959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieger, J.; Wick, W.; Weller, M. Human Malignant Glioma Cells Express Semaphorins and Their Receptors, Neuropilins and Plexins. Glia 2003, 42, 379–389. [Google Scholar] [CrossRef]
- Fakhari, M.; Pullirsch, D.; Abraham, D.; Paya, K.; Hofbauer, R.; Holzfeind, P.; Hofmann, M.; Aharinejad, S. Selective Upregulation of Vascular Endothelial Growth Factor Receptors Neuropilin-1 and -2 in Human Neuroblastoma. Cancer 2002, 94, 258–263. [Google Scholar] [CrossRef]
- Gray, M.J.; van Buren, G.; Dallas, N.A.; Xia, L.; Wang, X.; Yang, A.D.; Somcio, R.J.; Lin, Y.G.; Lim, S.; Fan, F.; et al. Therapeutic Targeting of Neuropilin-2 on Colorectal Carcinoma Cells Implanted in the Murine Liver. JNCI J. Natl. Cancer Inst. 2008, 100, 109–120. [Google Scholar] [CrossRef] [Green Version]
- Dallas, N.A.; Gray, M.J.; Xia, L.; Fan, F.; van Buren, G.; Gaur, P.; Samuel, S.; Lim, S.J.; Arumugam, T.; Ramachandran, V.; et al. Neuropilin-2-Mediated Tumor Growth and Angiogenesis in Pancreatic Adenocarcinoma. Clin. Cancer Res. 2008, 14, 8052–8060. [Google Scholar] [CrossRef] [Green Version]
- Cohen, T.; Herzog, Y.; Brodzky, A.; Greenson, J.K.; Eldar, S.; Gluzman-Poltorak, Z.; Neufeld, G.; Resnick, M.B. Neuropilin-2 Is a Novel Marker Expressed in Pancreatic Islet Cells and Endocrine Pancreatic Tumours. J. Pathol. 2002, 198, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Fukahi, K.; Fukasawa, M.; Neufeld, G.; Itakura, J.; Korc, M. Aberrant Expression of Neuropilin-1 and -2 in Human Pancreatic Cancer Cells. Clin. Cancer Res. 2004, 10, 581–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuoka, H.; Kodama, R.; Tsujimoto, M.; Yoshidome, K.; Akamatsu, H.; Nakahara, M.; Inagaki, M.; Sanke, T.; Nakamura, Y. Neuropilin-2 Expression in Breast Cancer: Correlation with Lymph Node Metastasis, Poor Prognosis, and Regulation of CXCR4 Expression. BMC Cancer 2009, 9, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vales, A.; Kondo, R.; Aichberger, K.J.; Mayerhofer, M.; Kainz, B.; Sperr, W.R.; Sillaber, C.; Jäger, U.; Valent, P. Myeloid Leukemias Express a Broad Spectrum of VEGF Receptors Including Neuropilin-1 (NRP-1) and NRP-2. Leuk. Lymphoma 2007, 48, 1997–2007. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Wang, R.; Zhao, Y.-F.; Jia, J.; Sun, Z.-J.; Chen, X.-M. Expression of Neuropilin-2 in Salivary Adenoid Cystic Carcinoma: Its Implication in Tumor Progression and Angiogenesis. Pathol. Res. Pract. 2010, 206, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Calicchio, M.L.; Collins, T.; Kozakewich, H.P. Identification of Signaling Systems in Proliferating and Involuting Phase Infantile Hemangiomas by Genome-Wide Transcriptional Profiling. Am. J. Pathol. 2009, 174, 1638–1649. [Google Scholar] [CrossRef] [Green Version]
- Pellet-Many, C.; Frankel, P.; Jia, H.; Zachary, I. Neuropilins: Structure, Function and Role in Disease. Biochem. J. 2008, 411, 211–226. [Google Scholar] [CrossRef] [Green Version]
- Favier, B.; Alam, A.; Barron, P.; Bonnin, J.; Laboudie, P.; Fons, P.; Mandron, M.; Herault, J.-P.; Neufeld, G.; Savi, P.; et al. Neuropilin-2 Interacts with VEGFR-2 and VEGFR-3 and Promotes Human Endothelial Cell Survival and Migration. Blood 2006, 108, 1243–1250. [Google Scholar] [CrossRef]
- Dallas, N.A.; Fan, F.; Gray, M.J.; van Buren, G.; Lim, S.J.; Xia, L.; Ellis, L.M. Functional Significance of Vascular Endothelial Growth Factor Receptors on Gastrointestinal Cancer Cells. Cancer Metastasis Rev. 2007, 26, 433. [Google Scholar] [CrossRef]
- Cao, M.; Tang, Y.; Zhang, W.; Tang, Y.-J.; Liang, X. Non-Coding RNAs as Regulators of Lymphangiogenesis in Lymphatic Development, Inflammation, and Cancer Metastasis. Front. Oncol. 2019, 9, 916. [Google Scholar] [CrossRef]
- Xu, Y.; Yuan, L.; Mak, J.; Pardanaud, L.; Caunt, M.; Kasman, I.; Larrivée, B.; del Toro, R.; Suchting, S.; Medvinsky, A.; et al. Neuropilin-2 Mediates VEGF-C–Induced Lymphatic Sprouting Together with VEGFR3. J. Cell Biol. 2010, 188, 115–130. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-D.; Zhong, L.-P.; He, J.; Zhao, Y.-X. Targeting Neuropilin-1 Interactions Is a Promising Anti-Tumor Strategy. Chin. Med. J. 2021, 134, 508–517. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Jubb, A.M.; Sa, S.M.; Ratti, N.; Strickland, L.A.; Schmidt, M.; Callahan, C.A.; Koeppen, H. Neuropilin-2 Expression in Cancer. Histopathology 2012, 61, 340–349. [Google Scholar] [CrossRef]
- Staton, C.A.; Koay, I.; Wu, J.M.; Hoh, L.; Reed, M.W.R.; Brown, N.J. Neuropilin-1 and Neuropilin-2 Expression in the Adenoma-Carcinoma Sequence of Colorectal Cancer. Histopathology 2013, 62, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Zhou, Q.; Wu, F.; Peng, Q.; Tang, A.; Liang, H.; Zeng, Y. Semaphorin3F Down-Regulates the Expression of Integrin αvβ3 and Sensitizes Multicellular Tumor Spheroids to Chemotherapy via the Neuropilin-2 Receptor in vitro. Chemotherapy 2009, 55, 344–352. [Google Scholar] [CrossRef]
- Liu, A.; Liu, L.; Lu, H. LncRNA XIST Facilitates Proliferation and Epithelial–Mesenchymal Transition of Colorectal Cancer Cells through Targeting MiR-486-5p and Promoting Neuropilin-2. J. Cell. Physiol. 2019, 234, 13747–13761. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, R.; Wang, M. MiR-331-3p Suppresses Cell Invasion and Migration in Colorectal Carcinoma by Directly Targeting NRP2. Oncol. Lett. 2019, 18, 6501–6508. [Google Scholar] [CrossRef]
- Lian, H.; Liu, C.; Li, M.; Hu, Y.; Shi, N.; Yu, H.; Liu, H. MiR-486-5p Attenuates Tumor Growth and Lymphangiogenesis by Targeting Neuropilin-2 in Colorectal Carcinoma. OncoTargets Ther. 2016, 9, 2865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ou, J.-J.; Wei, X.; Peng, Y.; Zha, L.; Zhou, R.-B.; Shi, H.; Zhou, Q.; Liang, H.-J. Neuropilin-2 Mediates Lymphangiogenesis of Colorectal Carcinoma via a VEGFC/VEGFR3 Independent Signaling. Cancer Lett. 2015, 358, 200–209. [Google Scholar] [CrossRef]
- Luo, X.; He, J.; Xu, J.; Hu, S.; Mo, B.; Shu, Q.; Chen, C.; Gong, Y.; Zhao, X.; Xie, G.; et al. Vascular NRP2 Triggers PNET Angiogenesis by Activating the SSH1-Cofilin Axis. Cell Biosci. 2020, 10, 113. [Google Scholar] [CrossRef] [PubMed]
- Weekes, C.D.; Beeram, M.; Tolcher, A.W.; Papadopoulos, K.P.; Gore, L.; Hegde, P.; Xin, Y.; Yu, R.; Shih, L.M.; Xiang, H.; et al. A Phase I Study of the Human Monoclonal Anti-NRP1 Antibody MNRP1685A in Patients with Advanced Solid Tumors. Investig. New Drugs 2014, 32, 653–660. [Google Scholar] [CrossRef]
- Patnaik, A.; LoRusso, P.M.; Messersmith, W.A.; Papadopoulos, K.P.; Gore, L.; Beeram, M.; Ramakrishnan, V.; Kim, A.H.; Beyer, J.C.; Mason Shih, L.; et al. A Phase Ib Study Evaluating MNRP1685A, a Fully Human Anti-NRP1 Monoclonal Antibody, in Combination with Bevacizumab and Paclitaxel in Patients with Advanced Solid Tumors. Cancer Chemother. Pharmacol. 2014, 73, 951–960. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. crt. | Author | Population | Sample Properties | Cancer Type | Cell Lines | Assays/Techniques Applied | Vectors | Plasmid | Gene/NRP-2 Expression | NRP-2 Correlation with CRC | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Grandclement C. et. al. [7] | 11 | Tumor cell lines | Colorectal cancer cells | HT29, Colo320, SW620, MCF7 | STR analysis, Flow cytometry, Cell | P proliferation and ELISA assay | hNRP-2 (pcDNA3.1-NRP-2 & | pCMV6-XL5-NRP-2 | NRP-2 & TGF-β1expressed | NRP-2 role in epithelial-mesenchymal transition is suggested. The cross-talk between NRP-2 and TGF-b1 | signaling supports cancer progression. | NRP-2 is expressed at the membrane of several human CRC cell lines, while it is not expressed in normal tissues. | |
| 2 | Staton CA et al. [33] | 167 | Aged persons | Epithelial and colorectal | - | Immunohistochemistry | - | NRP-1 and NRP-2 increased | NRP-2 is overexpressed in all cancers. No relevant connection with MVD, VEGF, or NRP-1 was discovered. | Poor prognosis was more likely for the patients that expressed NRP-1 and NRP-2, compared with | the ones expressing only NRP-1 or NRP-2 or even no NRP at all. | |||
| 3 | Gray MJ et al. [17] | 10 | Derivation from sh-Con | Colon adenocarcinoma | HCT-116, HT-29, RKO, SW480 & KM12 | Immunoprecipitation & Immunoblot analysis RT-PCR, (ELIA) and MTT analysis | shRNA | NRP-2 expressed | Tumors presented a | NRP-2 was overexpressed in tumors compared with the adjacent mucosa | ||||
| 4 | Zheng C et al. [34] | 5 | After chemotherapy | Ovarian cells | HT29, HCT116, and Lobo | 3D cell culture, SEM and TEM analysis, Western blotting & Chemosensitivity | Sema3F cDNA pSecTag | Sema3F & NRP-2 increase | The up-regulation of NRP-2 receptor expression was linked to elevated expression of Sema3F and down-regulation of integrin alphaVbeta3 expression | |||||
| 5 | Liu A et al. [35] | 317 | CRC Population | Rectum & Colon | HCT116, HT29 & SW620 | RT-PCR, Western blotting, Cell apoptosis, and cell invasion assay | IncRNA3.1-XIST | XIST & NRP-2 high | miR-486-5p is decreased in CRC tissues. By directly targeting NRP-2, it attenuated in vivo the proliferation and lymphangiogenesis of the tumoral cells | |||||
| 6 | Zhang H et al. [36] | 54 | CRC Population | Colorectal carcinoma Colon and rectum | SW480 & HCT116) | RT-qPCR, Transwell assays, western blot analysis, and IHC | pGL3 | luciferase vectors (Promega) | miR-331-3p expressed | NRP-2 was upregulated in CRC | ||||
| 7 | Liu C et al. [37] | 66 | Before chemotherapy | Malignant gastrointestinal tumor | SW620 and HT-29 | qRT-PCR, Western blot, luciferase reporter assay, Tumorigenicity assay, and in silico analysis | pMIR-GLO | miR-486-5p downregulated and NRP-2 was overexpressed. | Normal tissues and cells had lower NRP-2 expression by comparison with CRC tissues and cells | |||||
| 8 | Ou J-J et al. [38] | 200 | After surgery | Tumor lymphatic endothelial cells | SW480 & SW620 | ELISA, qPCR & Transwell assay & | Tubologenisis assay | FAK shRNA & Rac1 siRNA & RNAi (TG320362) | Integrin α9 & β1, XIST & NRP-2 low expressed | The density of tumor lymphatic vessels is linked to NRP-2 expression levels in CRC | ||||
| 9 | Luo X et al. [39] | 13 | Non-small-cell lung & | colon cancer | Pancreatic neuroendocrine tumors (pnets | HUVECs & BON | Western blotting, Immunohistochemistry, Cellular F-actin/G-actin assay, Phalloidin staining say | pGC-LV-GV308 | VEGFR2 | If conditioned medium from colorectal is present, NRP-2 doesn’t act to promote cell migration | ||||
| 10 | Jubb AM et [32] | 275 | Paraffin-embedded tissue | Lung, breast, and Colo-rectal cancer | NSCLC lines | Immunohistochemistry | - | Neuropilin-2 expressed | Blood and/or lymphatic vessels showed immunoreactivity for NRP-2. | NRP-2 | protein expression was detected in tumor cells from 22% of colorectal cancers | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lungulescu, C.; Ghimpau, V.; Gheonea, D.I.; Sur, D.; Lungulescu, C.V. The Role of Neuropilin-2 in the Epithelial to Mesenchymal Transition of Colorectal Cancer: A Systematic Review. Biomedicines 2022, 10, 172. https://doi.org/10.3390/biomedicines10010172
Lungulescu C, Ghimpau V, Gheonea DI, Sur D, Lungulescu CV. The Role of Neuropilin-2 in the Epithelial to Mesenchymal Transition of Colorectal Cancer: A Systematic Review. Biomedicines. 2022; 10(1):172. https://doi.org/10.3390/biomedicines10010172
Chicago/Turabian StyleLungulescu, Cristina, Valentina Ghimpau, Dan Ionut Gheonea, Daniel Sur, and Cristian Virgil Lungulescu. 2022. "The Role of Neuropilin-2 in the Epithelial to Mesenchymal Transition of Colorectal Cancer: A Systematic Review" Biomedicines 10, no. 1: 172. https://doi.org/10.3390/biomedicines10010172
APA StyleLungulescu, C., Ghimpau, V., Gheonea, D. I., Sur, D., & Lungulescu, C. V. (2022). The Role of Neuropilin-2 in the Epithelial to Mesenchymal Transition of Colorectal Cancer: A Systematic Review. Biomedicines, 10(1), 172. https://doi.org/10.3390/biomedicines10010172