
Natural History of Scoliosis in Children with NF1: An Observation Study

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
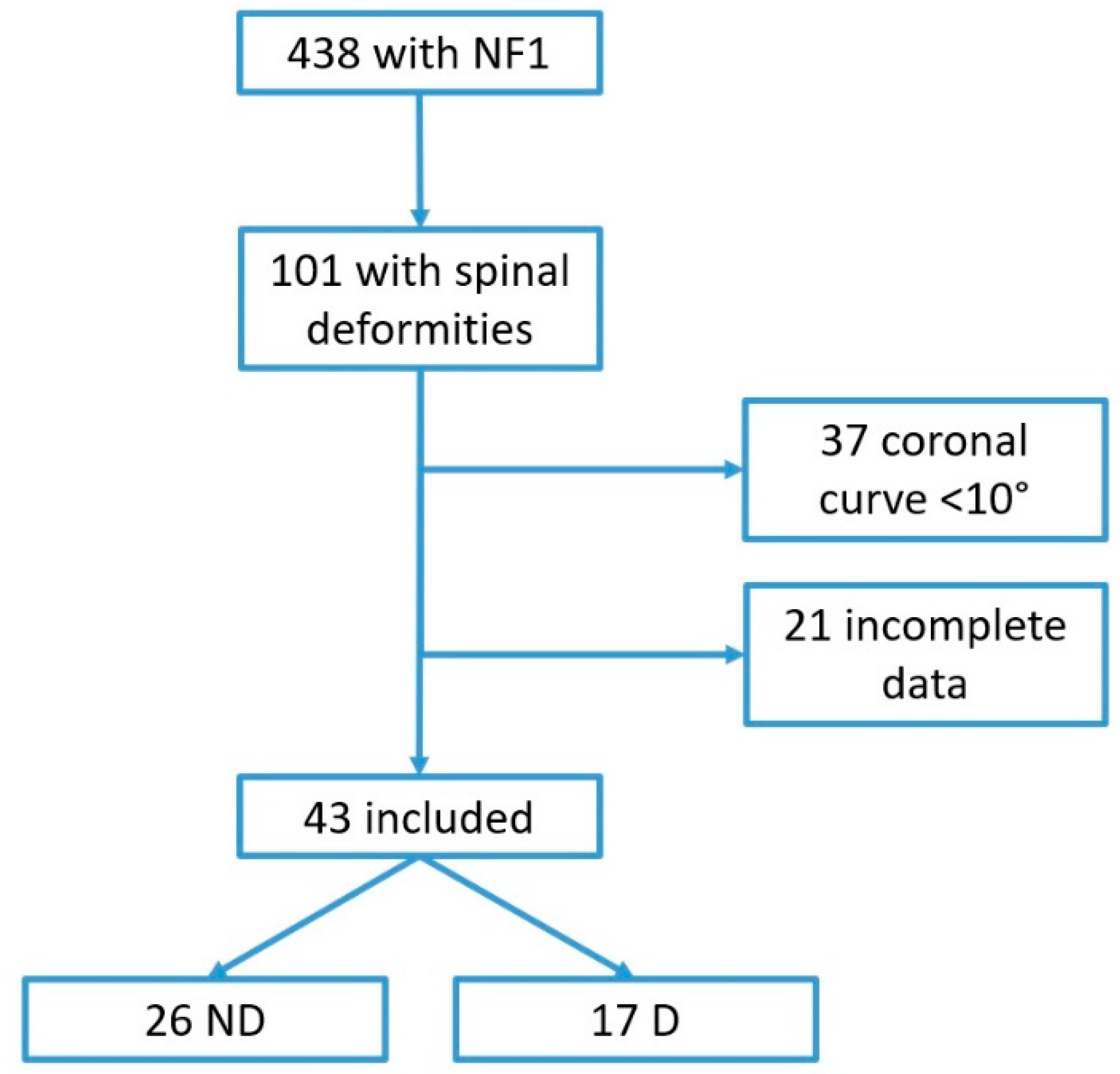
3. Results
3.1. Prevalence of Dystrophic Scoliosis in NF1
3.2. Age at Onset and Other Demographic Data of Scoliosis
3.3. Management of Scoliosis and Characteristics of Surgically Treated Patients
4. Discussion
4.1. Prevalence of Dystrophic Scoliosis in NF1
4.2. Age at Onset and Other Demographic Data of Scoliosis
4.3. Management of Scoliosis and Characteristics of Surgically Treated Patients
4.4. Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Z.; Liu, Y. Research Update and Recent Developments in the Management of Scoliosis in Neurofibromatosis Type 1. Orthopedics 2010, 33, 335–341. [Google Scholar] [CrossRef]
- Abramowicz, A.; Gos, M. Neurofibromin—Protein structure and cellular functions in the context of neurofibromatosis type I pathogenesis. Postępy Hig. Med. Dośw. 2015, 69, 1331–1348. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health Consensus Development Conference Statement: Neurofibromatosis; Bethesda: Rockville, MD, USA, 1988; Volume 1, pp. 172–178.
- Vitale, M.G.; Guha, A.; Skaggs, D.L. Orthopaedic Manifestations of Neurofibromatosis in Children: An Update. Clin. Orthop. Relat. Res. 2002, 401, 107–118. [Google Scholar] [CrossRef]
- Durrani, A.A.; Crawford, A.H.; Chouhdry, S.N.; Saifuddin, A.; Morley, T.R. Modulation of Spinal Deformities in Patients with Neurofibromatosis Type 1. Spine 2000, 25, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Funasaki, H.; Winter, R.B.; Lonstein, J.B.; Denis, F. Pathophysiology of spinal deformities in neurofibromatosis. An analysis of seventy-one patients who had curves associated with dystrophic changes. J. Bone Jt. Surg. Am. Vol. 1994, 76, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Lykissas, M.G.; Schorry, E.K.; Crawford, A.H.; Gaines, S.; Rieley, M.; Jain, V.V. Does the Presence of Dystrophic Features in Patients with Type 1 Neurofibromatosis and Spinal Deformities Increase the Risk of Surgery? Spine 2013, 38, 1595–1601. [Google Scholar] [CrossRef]
- Mccarroll, H.R. Clinical Manifestations of Congenital Neurofibromatosis. J. Bone Jt. Surg. Am. 1950, 32, 601–617. [Google Scholar] [CrossRef]
- Rezaian, S.M. The Incidence of Scoliosis Due to Neurofibromatosis. Acta Orthop. Scand. 1976, 47, 534–539. [Google Scholar] [CrossRef]
- Winter, R.B.; Moe, J.H.; Bradford, D.S.; Lonstein, J.E.; Pedras, C.V.; Weber, A.H. Spine deformity in neurofibromatosis. A review of one hundred and two patients. J. Bone Jt. Surg. Am. Vol. 1979, 61, 677–694. [Google Scholar] [CrossRef]
- Scoliosis Research Society SRS Revised Glossary. Available online: https://www.srs.org/professionals/online-education-and-resources/glossary/revised-glossary-of-terms (accessed on 21 July 2018).
- Tsirikos, A.I.; Saifuddin, A.; Noordeen, M.H. Spinal deformity in neurofibromatosis type-1: Diagnosis and treatment. Eur. Spine J. 2005, 14, 427–439. [Google Scholar] [CrossRef] [PubMed]
- Scoliosis Research Society SRS Patients and Families. Early Onset Scoliosis. Available online: https://www.srs.org/patients-and-families/conditions-and-treatments/parents/scoliosis/early-onset-scoliosis (accessed on 21 July 2018).
- Gutmann, D.; Ferner, R.E.; Listernick, R.H.; Korf, B.R.; Wolters, P.L.; Johnson, K.J. Neurofibromatosis type 1. Nat. Rev. Dis. Prim. 2017, 3, nrdp20174. [Google Scholar] [CrossRef] [PubMed]
- Akbarnia, B.A.; Gabriel, K.R.; Beckman, E.; Chalk, D. Prevalence of Scoliosis in Neurofibromatosis. Spine 1992, 17, 244–248. [Google Scholar] [CrossRef]
- Crawford, A.H.; Lykissas, M.G.; Schorry, E.K.; Gaines, S.; Jain, V.; Greggi, T.; Viskochil, D. Neurofibromatosis: Etiology, Commonly Encountered Spinal Deformities, Common Complications and Pitfalls of Surgical Treatment. Spine Deform. 2012, 1, 85–94. [Google Scholar] [CrossRef]
- Rajasekaran, S.; Kamath, V.; Kiran, R.; Shetty, A. Intraspinal anomalies in scoliosis: An MRI analysis of 177 consecutive scoliosis patients. Indian J. Orthop. 2010, 44, 57–63. [Google Scholar] [CrossRef]
- Ramachandran, M.; Tsirikos, A.I.; Lee, J.; Saifuddin, A. Whole-Spine Magnetic Resonance Imaging in Patients with Neurofibromatosis Type 1 and Spinal Deformity. J. Spinal Disord. Tech. 2004, 17, 483–491. [Google Scholar] [CrossRef]
- Feldman, D.S.; Jordan, C.; Fonseca, L. Orthopaedic Manifestations of Neurofibromatosis Type 1. J. Am. Acad. Orthop. Surg. 2010, 18, 346–357. [Google Scholar] [CrossRef]
- Rhodes, S.D.; Zhang, W.; Yang, D.; Yang, H.; Chen, S.; Wu, X.; Li, X.; Yang, X.; Mohammad, K.S.; Guise, T.A.; et al. Dystrophic Spinal Deformities in a Neurofibromatosis Type 1 Murine Model. PLoS ONE 2015, 10, e0119093. [Google Scholar] [CrossRef][Green Version]
- Zhang, W.; Rhodes, S.D.; Zhao, L.; He, Y.; Zhang, Y.; Shen, Y.; Yang, D.; Wu, X.; Li, X.; Yang, X.; et al. Primary osteopathy of vertebrae in a neurofibromatosis type 1 murine model. Bone 2011, 48, 1378–1387. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wu, X.; Estwick, S.A.; Chen, S.; Yu, M.; Ming, W.; Nebesio, T.D.; Li, Y.; Yuan, J.; Kapur, R.; Ingram, D.; et al. Neurofibromin plays a critical role in modulating osteoblast differentiation of mesenchymal stem/progenitor cells. Hum. Mol. Genet. 2006, 15, 2837–2845. [Google Scholar] [CrossRef]
- Böker, T.; Vanem, T.T.; Pripp, A.H.; Rand-Hendriksen, S.; Paus, B.; Smith, H.-J.; Lundby, R. Dural ectasia in Marfan syndrome and other hereditary connective tissue disorders: A 10-year follow-up study. Spine J. 2019, 19, 1412–1421. [Google Scholar] [CrossRef]
- Nehls, M.C.; Grapilon, M.L.; Brenner, D.A. NF-I/Sp1 Switch Elements Regulate Collagen α1(I) Gene Expression. DNA Cell Biol. 1992, 11, 443–452. [Google Scholar] [CrossRef]
- Parisini, P.; Di Silvestre, M.; Greggi, T.; Paderni, S.; Cervellati, S.; Savini, R. Surgical Correction of Dystrophic Spinal Curves in Neurofibromatosis. Spine 1999, 24, 2247–2253. [Google Scholar] [CrossRef] [PubMed]
- Wilde, P.H.; Upadhyay, S.S.; Leong, J.C.Y. Deterioration of Operative Correction in Dystrophic Spinal Neurofibromatosis. Spine 1994, 19, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Aulisa, A.G.; Giordano, M.; Guzzanti, V.; Falciglia, F.; Pizzetti, P.; Toniolo, R.M. Effectiveness of school scoliosis screening and the importance of this method in measures to reduce morbidity in an Italian territory. J. Pediatr. Orthop. B 2019, 28, 271–277. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, Z.; Zhu, F.; Sun, C.; Wang, Z.; Sun, X.; Qiu, Y. Different Curve Pattern and Other Radiographical Characteristics in Male and Female Patients with Adolescent Idiopathic Scoliosis. Spine 2012, 37, 1586–1592. [Google Scholar] [CrossRef]
- Rietman, A.B.; Van Der Vaart, T.; Plasschaert, E.; Nicholson, B.; Oostenbrink, R.; Krab, L.C.; Descheemaeker, M.-J.; Wit, M.-C.Y.; Moll, H.A.; Legius, E.; et al. Emotional and behavioral problems in children and adolescents with neurofibromatosis type 1. Am. J. Med Genet. Part B Neuropsychiatr. Genet. 2018, 177, 319–328. [Google Scholar] [CrossRef]
- Rigo, M.; Reiter, C.; Weiss, H.-R. Effect of conservative management on the prevalence of surgery in patients with adolescent idiopathic scoliosis. Pediatr. Rehabil. 2003, 6, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, E.; Fabbrini, G.; Di Biasi, C.; Iacovino, C.; Ferrazzano, G.; Gualdi, G.; Calvieri, S.; Giustini, S. Chiari type 1 malformation in Neurofibromatosis type 1: Experience of a center and review of the literature. La Clin. Ter. 2016, 167, 6–10. [Google Scholar]
- Strahle, J.; Smith, B.W.; Martinez, M.; Bapuraj, J.R.; Muraszko, K.M.; Garton, H.J.L.; Maher, C.O. The association between Chiari malformation Type I, spinal syrinx, and scoliosis. J. Neurosurg. Pediatr. 2015, 15, 607–611. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vertebral Dystrophic Changes |
|---|
| Vertebral Scalloping (present when the depth of scalloping is >3 mm in the thoracic spine or >4 mm in the lumbar spine) |
| Rib penciling (rib width lower than the narrowest portion of the second rib) |
| Spindling of the transverse processes (loss of 50% from the height of the transverse process measured in the middle point between the lateral edge of the vertebral body and tip of the transverse process and compared with the contralateral normal side or uninvolved vertebra above or below) |
| Focal, short-segmented curve (involving 6 or less vertebrae) |
| Dural ectasia |
| Paraspinal tumors or plexiform neurofibromas close to the scoliosis curve |
| Vertebral wedging |
| Intervertebral foraminal widening |
| Widened interpediculate distances |
| Dysplastic pedicles |
| NF1 Cohort | ND Group (n = 26) | D Group (n = 17) | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Mean age at scoliosis diagnosis (yrs) | N/A | 10.08 (2–12) | 8.8 (3–16) | 0.167 |
| Sex (M) | 246 | 14 | 9 | 1 |
| Early Onset (%) | N/A | 13/26 (50%) | 12/17 (70%) | 0.307 |
| Infantile scoliosis | 0 | 1 | 0.395 | |
| Juvenile scoliosis | 13 | 11 | 0.369 | |
| Adolescent scoliosis | 13 | 5 | 0.219 | |
| Sporadic NF1 | 215 | 18 | 7 | 0.114 |
| Hereditary NF1 | 223 | 8 | 10 | |
| Maternal NF1 | 115 | 6 | 7 | 1 |
| Paternal NF1 | 90 | 2 | 3 | |
| Unspecified | 18 | |||
| Dystrophic features | N/A | |||
| Vertebral scalloping (n) | 0 | 10 | 0.001 | |
| Dural ectasia (n) | 0 | 5 | 0.006 | |
| Paravertebral neurofibromas (n. of patients) | 3 | 11 | 0.0006 | |
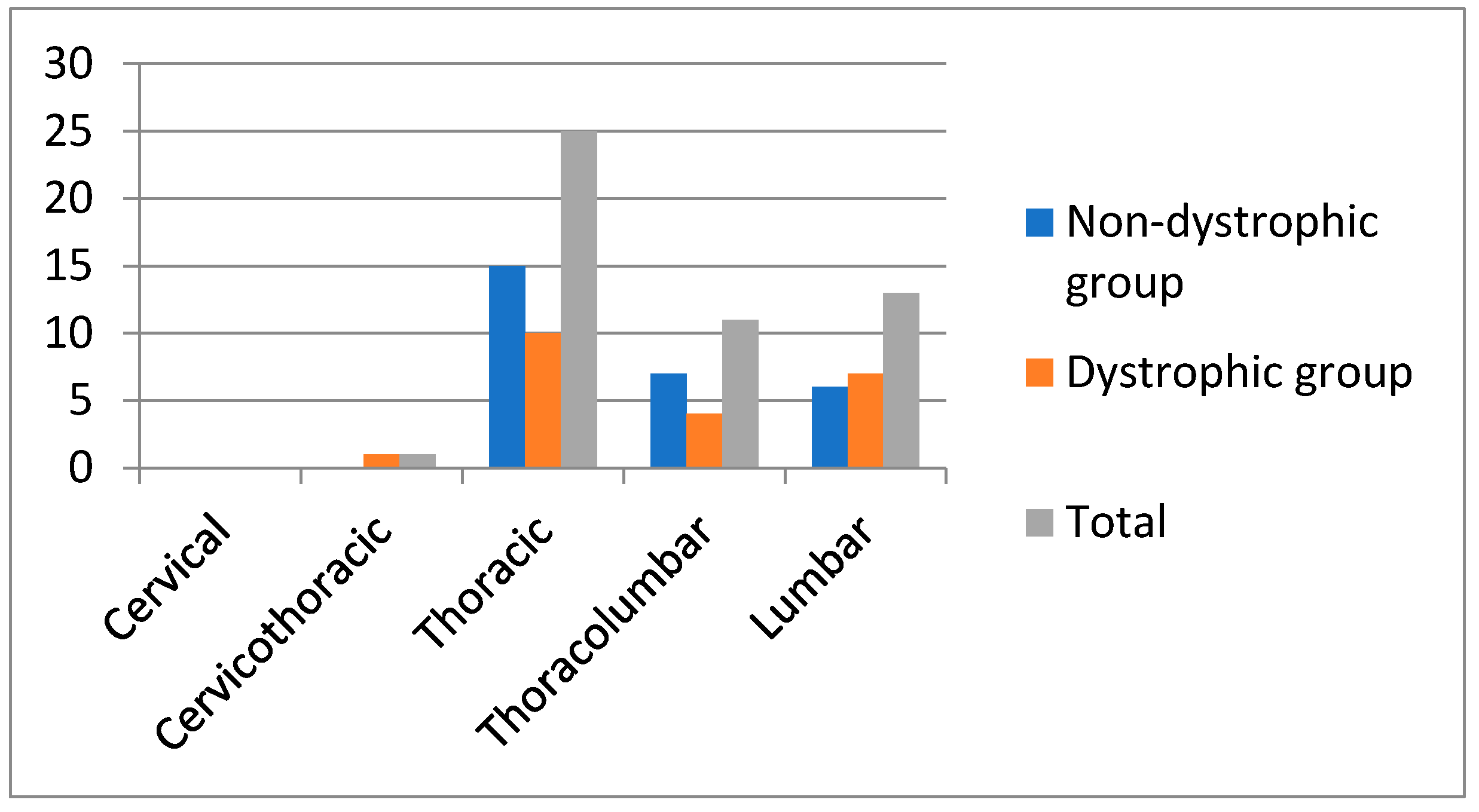
| Cervicothoracic (n. of patients) | 1 | 4 | 1 | |
| Thoracic (n. of patients) | 0 | 5 | 0.51 | |
| Thoracolumbar (n. of patients) | 0 | 3 | 1 | |
| Lumbar (n. of patients) | 2 | 3 | 0.17 | |
| Focal, short segment curve, n (%) | 16 (57%) | 13 (59%) | 0.34 | |
| Syringomyelia (n) | 0 | 1 | ||
| Chiari I (n) | 0 | 1 | ||
| Long bone dysplasia (n) | 1 | 0 | ||
| Treatment | N/A | |||
| Conservative treatment, n (%) | 11 (42%) | 7 (41%) | 0.94 | |
| Cheneau | 3 | 3 | ||
| Lyonnaise | 3 | 2 | ||
| Boston | 2 | 1 | ||
| Milwaukee | 3 | 1 | ||
| Surgery (n) | N/A | 4 (15%) | 5 (29%) | 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toro, G.; Santoro, C.; Ambrosio, D.; Landi, G.; Scilipoti, M.; Moretti, A.; Paoletta, M.; Liguori, S.; Schiavone Panni, A.; Picariello, S.; et al. Natural History of Scoliosis in Children with NF1: An Observation Study. Healthcare 2021, 9, 881. https://doi.org/10.3390/healthcare9070881
Toro G, Santoro C, Ambrosio D, Landi G, Scilipoti M, Moretti A, Paoletta M, Liguori S, Schiavone Panni A, Picariello S, et al. Natural History of Scoliosis in Children with NF1: An Observation Study. Healthcare. 2021; 9(7):881. https://doi.org/10.3390/healthcare9070881
Chicago/Turabian StyleToro, Giuseppe, Claudia Santoro, Daniele Ambrosio, Giovanni Landi, Martina Scilipoti, Antimo Moretti, Marco Paoletta, Sara Liguori, Alfredo Schiavone Panni, Stefania Picariello, and et al. 2021. "Natural History of Scoliosis in Children with NF1: An Observation Study" Healthcare 9, no. 7: 881. https://doi.org/10.3390/healthcare9070881
APA StyleToro, G., Santoro, C., Ambrosio, D., Landi, G., Scilipoti, M., Moretti, A., Paoletta, M., Liguori, S., Schiavone Panni, A., Picariello, S., & Iolascon, G. (2021). Natural History of Scoliosis in Children with NF1: An Observation Study. Healthcare, 9(7), 881. https://doi.org/10.3390/healthcare9070881