
Psychoeducation for Patients with Fibromyalgia: A Systematic Review


Abstract
1. Introduction
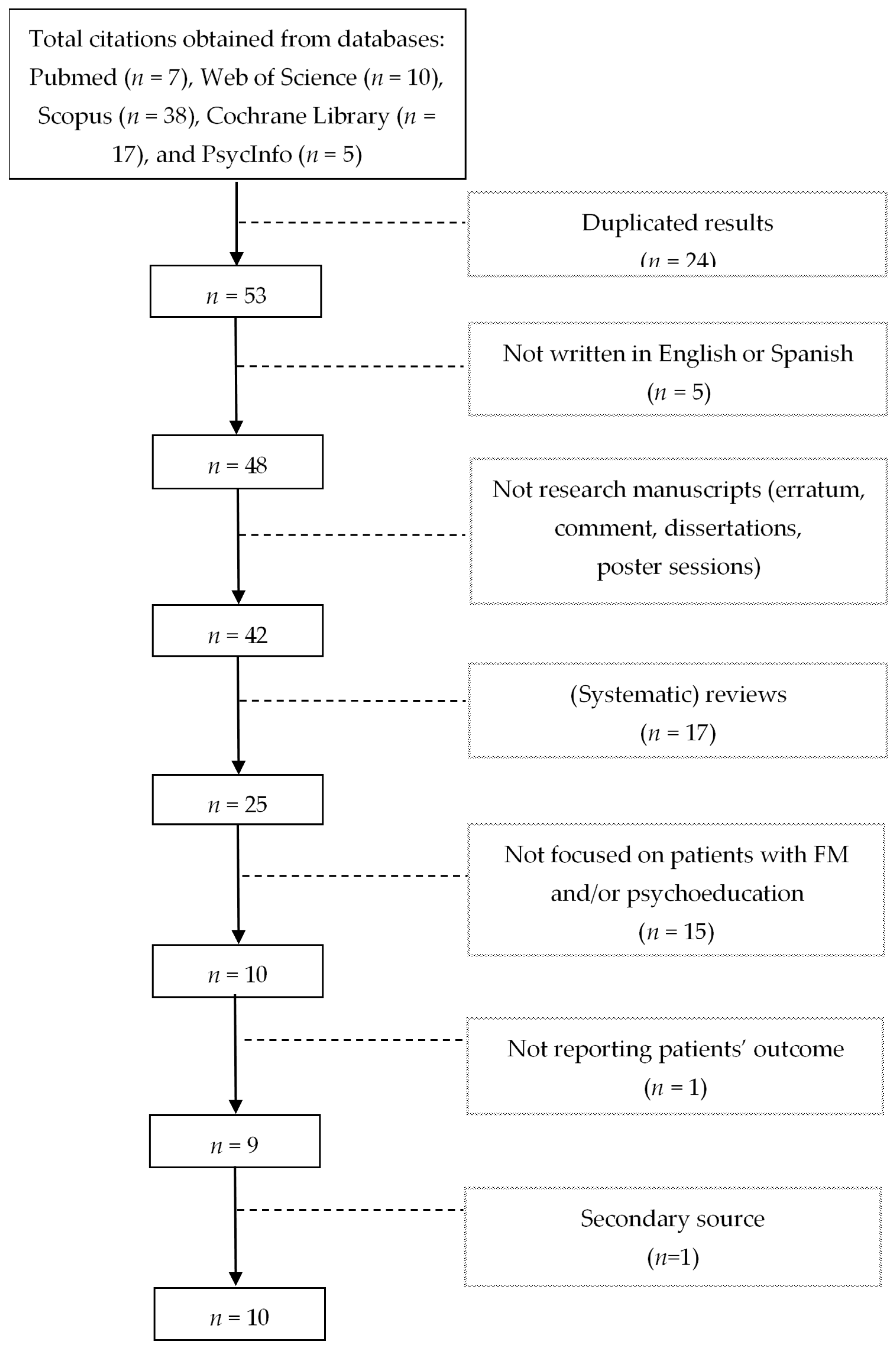
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia pathogenesis and treatment options update. Curr. Pain Headache Rep. 2016, 20, 25. [Google Scholar] [CrossRef]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef]
- Marques, A.P.; Santo, A.S.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Pelaez-Ballestas, I.; Sanin, L.H.; Moreno-Montoya, J.; Alvarez-Nemegyei, J.; Burgos-Vargas, R.; Garza-Elizondo, M.; Rodriguez-Amado, J.; Goycochea-Robles, M.-V.; Madariaga, M.; Zamudio, J.; et al. Epidemiology of the rheumatic diseases in Mexico. A study of 5 regions based on the COPCORD methodology. J. Rheumatol. Suppl. 2011, 86, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Wassem, R.; Hendrix, T.J. Direct and indirect costs of fibromyalgia to patients and their families. J. Orthop. Nurs. 2003, 7, 26–32. [Google Scholar] [CrossRef]
- Wolfe, F.; Häuser, W. Fibromyalgia diagnosis and diagnostic criteria. Ann. Med. 2011, 43, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Jahan, F.; Nanji, K.; Qidwai, W.; Qasim, R. Fibromyalgia Syndrome: An overview of pathophysiology, diagnosis and management. Oman Med. J. 2012, 27, 192–195. [Google Scholar] [CrossRef]
- Bradley, L.A. Pathophysiology of fibromyalgia. Am. J. Med. 2009, 122, S22–S30. [Google Scholar] [CrossRef] [PubMed]
- Tzadok, R.; Ablin, J.N. Current and emerging pharmacotherapy for fibromyalgia. Pain Res. Manag. 2020, 2020, 6541798. [Google Scholar] [CrossRef] [PubMed]
- Kia, S.; Choy, E. Update on treatment guideline in fibromyalgia syndrome with focus on pharmacology. Biomedicines 2017, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.J.; Kronisch, C.; Dean, L.E.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Häuser, W.; Ablin, J.; Perrot, S.; Fitzcharles, M.A. Management of fibromyalgia: Practical guides from recent evidence-based guidelines. Polish Arch. Intern. Med. 2017, 127, 47–56. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef]
- Fietta, P.; Fietta, P.; Manganelli, P. Fibromyalgia and psychiatric disorders. Acta Biomed. 2007, 78, 88–95. [Google Scholar]
- Sancassiani, F.; Machado, S.; Ruggiero, V.; Cacace, E.; Carmassi, C.; Gesi, C.; Dell’Osso, L.; Carta, M.G. The management of fibromyalgia from a psychosomatic perspective: An overview. Int. Rev. Psychiatry 2017, 29, 473–488. [Google Scholar] [CrossRef] [PubMed]
- Gómez-de-Regil, L.; Estrella-Castillo, D.F. Psychotherapy for physical pain in patients with fibromyalgia: A systematic review. Pain Res. Manag. 2020, 2020, 3408052. [Google Scholar] [CrossRef]
- Temeloğlu Şen, E.; Hocaoğlu, A.; Sertel Berk, Ö. Group psychotherapy with fibromyalgia patients: A systematic review. Arch. Rheumatol. 2019, 34, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Köllner, V.; Bernardy, K.; Greiner, W.; Krumbein, L.; Lucius, H.; Offenbächer, M.; Sarholz, M.; Settan, M.; Häuser, W. Psychotherapy and psychological procedures for fibromyalgia syndrome: Updated guidelines 2017 and overview of systematic review articles. Schmerz 2017, 31, 266–273. [Google Scholar] [CrossRef]
- Cummings, N.A.; Cummings, J.L. Psychoeducation in conjunction with psychotherapy practice. In Evidence-Based Adjunctive Treatments; Nicholas, O., Cummings, W., Eds.; Academic Press: Cambridge, MA, USA, 2008; pp. 41–59. [Google Scholar]
- Ekhtiari, H.; Rezapour, T.; Aupperle, R.L.; Paulus, M.P. Neuroscience-informed psychoeducation for addiction medicine: A neurocognitive perspective. Prog. Brain Res. 2017, 235, 239–264. [Google Scholar] [CrossRef]
- Palli, A. Psychoeducation: The way to make patients manage their illness and fill their future with life. Ment. Health Fam. Med. 2017, 13, 528–531. [Google Scholar]
- Conversano, C.; Poli, A.; Ciacchini, R.; Hitchcott, P.; Bazzichi, L.; Gemignani, A. A psychoeducational intervention is a treatment for fibromyalgia syndrome. Clin. Exp. Rheumatol. 2019, 37, 98–104. [Google Scholar] [PubMed]
- Lami, M.J.M.J.; Martínez, M.P.M.P.; Sánchez, A.I.A.I. Systematic review of psychological treatment in fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 345. [Google Scholar] [CrossRef] [PubMed]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of cognitive behavioural therapies in fibromyalgia syndrome. A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2018, 22, 242–260. [Google Scholar] [CrossRef] [PubMed]
- Lauche, R.; Cramer, H.; Dobos, G.; Langhorst, J.; Schmidt, S. A systematic review and meta-analysis of mindfulness-based stress reduction for the fibromyalgia syndrome. J. Psychosom. Res. 2013, 75, 500–510. [Google Scholar] [CrossRef]
- Zech, N.; Hansen, E.; Bernardy, K.; Häuser, W. Efficacy, acceptability and safety of guided imagery/hypnosis in fibromyalgia. A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2017, 21, 217–227. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of Internet-delivered psychological therapies for fibromyalgia syndrome: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2019, 23, 3–14. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- U.S. Department of Health & Human Services Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 26 October 2020).
- Anderson, F.J.; Winkler, A.E. Benefits of long-term fibromyalgia syndrome treatment with a multidisciplinary program. J. Musculoskelet. Pain 2006, 14, 11–25. [Google Scholar] [CrossRef]
- Ang, D.C.; Jensen, M.P.; Steiner, J.L.; Hilligoss, J.; Gracely, R.H.; Saha, C. Combining cognitive-behavioral therapy and milnacipran for fibromyalgia. Clin. J. Pain 2013, 29, 747–754. [Google Scholar] [CrossRef]
- Bourgault, P.; Lacasse, A.; Marchand, S.; Courtemanche-Harel, R.; Charest, J.; Gaumond, I.; Barcellos de Souza, J.; Choinière, M. Multicomponent interdisciplinary group intervention for self-management of fibromyalgia: A mixed-methods randomized controlled trial. PLoS ONE 2015, 10, e0126324. [Google Scholar] [CrossRef] [PubMed]
- Degotardi, P.J.; Klass, E.S.; Rosenberg, B.S.; Fox, D.G.; Gallelli, K.A.; Gottlieb, B.S. Development and evaluation of a cognitive-behavioral intervention for juvenile fibromyalgia. J. Pediatr. Psychol. 2005, 31, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; Martínez, N.; Peñarrubia-María, M.T.; Fernández-Vergel, R.; García-Campayo, J.; Verduras, C.; Blanco, M.E.; Jiménez, M.; Ruiz, J.M.; del Hoyo, Y.L.; et al. Effectiveness of a psychoeducational treatment program implemented in general practice for fibromyalgia patients. Clin. J. Pain 2011, 27, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; Sabes-Figuera, R.; Cardeñosa, E.; Peñarrubia-María, M.T.; Fernández-Vergel, R.; García-Campayo, J.; Knapp, M.; Serrano-Blanco, A. Cost-utility of a psychoeducational intervention in fibromyalgia patients compared with usual care: An economic evaluation alongside a 12-month randomized controlled trial. Clin. J. Pain 2013, 29, 702–711. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Angarita-Osorio, N.; Feliu-Soler, A.; Andrés-Rodríguez, L.; Borràs, X.; Luciano, J.V. Do humor styles predict clinical response to the MINDSET (MINDfulneSs & EducaTion) program? A pilot study in patients with fibromyalgia. Reumatol. Clin. 2019, 17, 137–140. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Feliu-Soler, A.; Montero-Marín, J.; García-Campayo, J.; Andrés-Rodríguez, L.; Borràs, X.; Rozadilla-Sacanell, A.; Peñarrubia-Maria, M.T.; Angarita-Osorio, N.; McCracken, L.M.; et al. A randomized controlled efficacy trial of mindfulness-based stress reduction compared with an active control group and usual care for fibromyalgia. Pain 2019, 160, 2508–2523. [Google Scholar] [CrossRef]
- Feliu-Soler, A.; Borràs, X.; Peñarrubia-María, M.T.M.T.; Rozadilla-Sacanell, A.; D’Amico, F.; Moss-Morris, R.; Howard, M.A.M.A.; Fayed, N.; Soriano-Mas, C.; Puebla-Guedea, M.; et al. Cost-utility and biological underpinnings of Mindfulness-Based Stress Reduction (MBSR) versus a psychoeducational programme (FibroQoL) for fibromyalgia: A 12-month randomised controlled trial (EUDAIMON study). BMC Complement. Altern. Med. 2016, 16, 81. [Google Scholar] [CrossRef] [PubMed]
- Fernández, R.; Peñarubia, M.T.; Luciano, J.V.; Blanco, M.E.; Jiménez, M.; Montesano, A.; Verduras, C.; Ruiz, J.M.; Serrano-Blanco, A. Effectiveness of a psycho-educational program for improving quality of life of fibromyalgia patients. BMC Musculoskelet. Disord. 2008, 9, 2. [Google Scholar] [CrossRef]
- Häuser, W.; Walitt, B.; Fitzcharles, M.-A.; Sommer, C. Review of pharmacological therapies in fibromyalgia syndrome. Arthritis Res. Ther. 2014, 16, 201. [Google Scholar] [CrossRef]
- Bennett, R.; Nelson, D. Cognitive behavioral therapy for fibromyalgia. Nat. Clin. Pract. Rheumatol. 2006, 2, 416–424. [Google Scholar] [CrossRef]
- De Sanctis, V.; Abbasciano, V.; Soliman, A.T.; Soliman, N.; Di Maio, S.; Fiscina, B.; Kattamis, C. The juvenile fibromyalgia syndrome (JFMS): A poorly defined disorder. Acta Biomed. 2019, 90, 134–148. [Google Scholar] [CrossRef] [PubMed]
- Lukens, E.P.; McFarlane, W.R. Psychoeducation as evidence-based practice: Considerations for practice, research, and policy. Br. Treat. Cris. Interv. 2004, 4, 205–225. [Google Scholar] [CrossRef]
- De Miquel, C.A.; Campayo, J.G.; Flórez, M.T.; Arguelles, J.M.G.; Tarrio, E.B.; Montoya, M.G.; Martin, Á.P.; Salio, A.M.; Fuentes, J.V.; Alberch, E.A.; et al. Interdisciplinary consensus document for the treatment of fibromyalgia. Actas Esp. Psiquiatr. 2010, 38, 108–120. [Google Scholar] [PubMed]


{kind=link}
| Database | Date of Search | Query | Results |
|---|---|---|---|
| PubMed | 13 October 2020 | (fibromyalgia[Title/Abstract]) AND (psychoeducation[Title/Abstract]) | 7 |
| Web of Science | 13 October 2020 | TOPIC: (fibromyalgia) AND TOPIC: (psychoeducation) | 10 |
| Scopus | 13 October 2020 | (TITLE-ABS-KEY (fibromyalgia) AND TITLE-ABS-KEY (psychoeducation)) | 38 |
| Cochrane Library | 13 October 2020 | “fibromyalgia” in Title Abstract Keyword AND “psychoeducation” in Title Abstract Keyword | 17 |
| PsycInfo | 13 October 2020 | (fibromyalgia and psychoeducation).ti. fibromyalgia.ti. and psychoeducation.ab. (fibromyalgia and psychoeducation).ab. fibromyalgia.ab. and psychoeducation.ti. | 5 |
| Reference | Setting | Funding | Design | Sample Size | % of Females | Age Inclusion Criterion | Sample Mean Age | Assessment Time Points |
|---|---|---|---|---|---|---|---|---|
| Original Research | ||||||||
| [34] | USA | NR | Two-arm RCT | 98 | 91.8 | NR | 52.06 | Before/After treatment |
| [35] | USA | NR | Three-arm RCT | 58 | 93 | 18–65 | 46.59 | Before/After treatment 21-week follow-up |
| [36] | Canada | Yes | Two-arm RCT (wait list) | 58 | 92.9 | ≥18 | 48.36 | Before/After treatment 3-month follow-up |
| [37] | USA | Yes | Single-arm pre-post | 67 | 88 | 8–20 | 13.9 | Before/After treatment |
| [38] * | Spain | Yes | Two-arm RCT | 216 | 97.65 | 18–75 | 55.3 | Before/After treatment |
| [39] * | Spain | Yes | Two-arm RCT | 216 | 97.65 | 18–75 | 55.3 | Before treatment 12-month follow-up |
| [40] ** | Spain | Yes | Single-arm pre-post (RCT pilot) | 35 | 97.1 | NR | 54.97 | Before/After treatment |
| [41] ** | Spain | Yes | Three-arm RCT | 225 | 98.23 | 18–65 | 53.27 | Before/After treatment 12-month follow-up |
| Study Protocol | ||||||||
| [42] ** | Spain | Yes | Three-arm RCT | 180 | - | 18–65 | - | Before/After treatment 12-month follow-up |
| [43] * | Spain | Yes | Two-arm RCT | 218 | - | 18–75 | - | Before treatment 1, 2, 6, and 12 months after the beginning of the intervention |
| Original Research | |
|---|---|
| [34] | Groups. (1) Pharmacological treatment, n = 20, (2) pharmacological and non-pharmacological treatment, n = 78 |
| Instruments: Fibromyalgia Impact Questionnaire (20 items), The Multiaxial Diagnostic Inventory–Revised, Short Form 36 Health Survey, Visual Analogue Scale (0 to 10), Number of tender points. Outcome. A significant decrease in measures of function, chronic depression, general anxiety, somatization, pain, anxiety, and tender points for the group 2. Also a significant increase in the patients’ perceived overall better health. No significant changes in the control group. Effect size values: Not reported. | |
| [35] | Groups. (1) Cognitive behavioral therapy and milnacipran, n = 20, (2) Education and milnacipran, n = 19, (3) Cognitive behavioral therapy and placebo, n = 19 |
| Instruments: Wrist-watch pain monitor (ActiWatch), Short Form 36 Health Survey Physical Functioning Subscale, Fibromyalgia Impact Questionnaire, Patient Health Questionnaire 8-item Depression Scale, Thumb Pressure Pain Sensitivity Test. Outcome. Compared with group 2, group 1 improved in physical function and in reduced pain intensity. Compared with group 2, group 3 had a moderate to large effect in improving physical function. Effect size values: Group 1, compared to group 2, showed improvement on physical function (0.60) and a reduction in pain intensity (0.67). Group 3, compared to group 2, showed improvement in physical function (0.70). Group 1, compared to group 2, showed improvement in physical function (0.60) and in reducing pain intensity (0.67). Group 1, compared to group 2, showed no significant differences in neither pain intensity (0.27) or physical function (0.10). Group 3, compared to group 2, showed little improvement in physical function (0.70) and no significant difference in pain intensity (0.40). The effect sizes for all the pair-wise group comparisons were very small (<0.30) regarding disease impact, depression severity, and changes in pain Sensitivity. | |
| [36] | Groups. (1) Intervention, n = 29, (2) Wait list, n = 29 Instruments: Numerical rating scale for pain sensitivity (0 to 10), Fibromyalgia Impact Questionnaire (20 items), Modified Brief Pain Inventory, Chronic Pain Sleep Inventory, Coping Strategy Questionnaire, Beck Depression Inventory, Short Form 12 Health Survey, Global Impression of Change, Pain Relief Scale (0 to 100). |
| Outcome. Group 1 significantly improved in perceived pain levels, pain relief and quality of life. Effect size values: Intervention group showed improvement after treatment (−0.13) and 3 months later in perceived pain levels (−0.55). Intervention group showed improvement after treatment (−0.36) and 3 months later in pain relief (−0.64). Intervention group showed improvement after treatment (1.14) and 3 months later in quality of life (1.84). | |
| [37] | Groups. (1) Intervention, n = 67 |
| Instruments: Brief Symptom Inventory, Visual Analogue Scale of the Pediatric Pain Questionnaire, Pittsburgh Sleep Quality Index, Fatigue Severity Scale, Functional Disability Inventory, Multidimensional Anxiety Scale, Children’s Somatization Inventory, Child Behavior Checklist, Satisfaction with Abilities and Well-Being Scale. Outcome. Significant reductions in pain, somatic symptoms, anxiety, and fatigue. Significant improvements in sleep quality, functional ability and fewer school absences. Effect size values: Not reported. | |
| [38] | Groups. (1) Psychoeducation and usual care, n = 108, (2) Usual care, n = 108 Instruments: Fibromyalgia Impact Questionnaire (Spanish Version, 10 items), Chronic Medical Conditions Checklist, State Trait Anxiety Inventory (Spanish Version), Marlowe-Crowne Social Desirability Scale. |
| Outcome. Group 1 improved in functional status, physical impairment, days not feeling well, pain, general fatigue, morning fatigue, stiffness, anxiety, and depression. Effect size values: functional status (0.16), physical impairment (0.09), days not feeling well (0.08), pain (0.12), general fatigue (0.04), morning fatigue (0.05), stiffness (0.03), anxiety (0.08), depression (0.09). | |
| [39] | Groups. (1) Psychoeducation and usual care, n = 108, (2) Usual care, n = 108 Instruments: Chronic Medical Conditions Checklist, Fibromyalgia Impact Questionnaire (10 items), EuroQoL-5D questionnaire, Client Service Receipt Inventory—Adapted. |
| Outcome. Group 1 showed greater improvement in global functional status, physical functioning, days feeling well, pain, morning fatigue, stiffness, and depression. Effect size values: Global functional status (0.36), physical functioning (0.56), days feeling well (0.40), pain (0.35), morning fatigue (0.24), stiffness (0.34), depression (0.30). | |
| [40] | Groups. (1) Intervention, n = 35 |
| Instruments: Humor Styles Questionnaire, Five-Facets Mindfulness Questionnaire, Patient Global Impression of Change (PGIC), Revised Fibromyalgia Impact Questionnaire (21 items). Outcome. Improvement in the perceived impact of FM, and perceived changes in observed mood, social activity, over-all status, physical activity, work activity, and pain. Effect size values: Not reported. | |
| [41] | Groups. (1) MBSR and treatment as usual, n = 75, (2) FibroQoL and treatment as usual, n = 75, (3) treatment as usual, n = 75 |
| Instruments: Revised Fibromyalgia Impact Questionnaire (21 items), Fibromyalgia Survey Diagnostic Criteria, Hospital Anxiety and Depression Scale, Pain Catastrophizing Scale, Perceived Stress Scale, Multidimensional Inventory of Subjective Cognitive Impairment, Five Facets of Mindfulness Questionnaire, Self-Compassion Scale—short form, Psychological Inflexibility in Pain Scale, Patient Global Impression of Change, Pain-Specific Impression of Change, Credibility/Expectancy Questionnaire, daily logs for recording the frequency of practice of MBSR exercises during the intervention. Outcome. Group 1 was superior to group 2 at post-treatment in measures of functional impact, anxiety and depression, perceived stress, and cognitive impairment, and at post-treatment and follow-up in measures of pain catastrophizing. Group 1 was superior to group 3 both at post-treatment and at follow-up in measures of functional impact of FM, symptoms of FM, anxiety and depression, pain catastrophizing, perceived stress, and cognitive impairment. Group 2 was superior to group 3 at post-treatment in measures of symptoms of FM, and at follow-up in measures of anxiety and depression, and cognitive impairment. Effect size values: Group 1 compared to group 2 at post-treatment in measures of functional impact (0.86), anxiety and depression (0.49), perceived stress (0.77), and cognitive impairment (0.95), and at post-treatment and follow-up in measures of pain catastrophizing (0.65, 0.58). Group 1 compared to group 3 at post-treatment and at follow-up in measures of functional impact of FM (1.11, 0.80), symptoms of FM (0.97, 1.04), and cognitive impairment (0.86, 0.99). Group 2 was superior to group 3 at post-treatment in measures of symptoms of FM (0.54) and at follow-up in measures of anxiety and depression (0.57), and cognitive impairment (0.65). | |
| Study Protocol | |
| [42] | Groups. (1) Mindfulness-Based Stress Reduction and treatment as usual, n = 60, (2) FibroQoL and treatment as usual, n = 60, (3) treatment as usual, n = 60 Instruments: SCID-I Structured Clinical Interview for DSM Axis I Disorders—Depression module, Mini-Mental State Examination, Revised Fibromyalgia Impact Questionnaire, Fibromyalgia Survey Diagnostic Criteria, Hospital Anxiety and Depression Scale, Perceived Stress Scale, Multidimensional Inventory of Subjective Cognitive Impairment, EuroQoL-5D questionnaire, CSRI Client Service Receipt Inventory, Five Facet Mindfulness Questionnaire, Pain Catastrophizing Scale, Psychological Inflexibility in Pain Scale, Self-Compassion Scale, Structural and Functional Neuroimaging data, Inflammatory data, Credibility/Expectancy Questionnaire, Patient Global Impression of Change, Patients Specific Impression of Change. |
| [43] | Groups. (1) Psychoeducation and usual care, n = 109, (2) Usual care, n = 109 Instruments: Questionnaire on chronic medical condition, Fibromyalgia Impact Questionnaire (Spanish Version, 10 items), EuroQoL-5D questionnaire, Client Service Receipt Inventory—Adapted. |
| Ref. [34] Non-pharmacologic treatment included cognitive behavioral therapy, coping skills classes, pool or land exercise, massage therapy, auricular therapy, microcurrent therapy, and nutritional counselling. The intervention lasted for approximately one year. Psychoeducation/cognitive behavioral therapy sessions were part of the phase 1 of the program, lasting eight weeks. |
| Ref. [35] Eight sessions of psychoeducation/cognitive behavioral therapy: (1) education on chronic pain including theories of pain; (2) training in progressive muscle relaxation and visual imagery; (3) education on the relationship between automatic thoughts and pain; (4) cognitive restructuring; (5) stress management; (6) time-based pacing and pleasant activity scheduling; (7) anger management and sleep hygiene; and (8) relapse prevention and flare-up planning. |
| Ref. [36] The PASSAGE program includes 9 sessions covering three dimensions: (1) psychoeducational tools, (2) cognitive behavioral therapy techniques, and (3) exercise activities. Psychoeducational topics: (1) introduction, (2) FM symptoms, (3) exercise and physical activity, (4) psychological state, (5) energy and capacity, (6) the vicious circle of chronic pain, (7) pharmacological and non-pharmacological treatment, (8) review and summary, (9) follow-up visit. |
| Ref. [37] Intervention for children and their parents, with four primary treatment modules lasting 8 weeks. (1) Psychoeducation (symptoms, etiology, treatments), week 1, (2) sleep improvement, weeks 2–3, (3) pain management, weeks 4–6, (4) activities of daily livings, weeks 7–8. |
| Refs. [38,39,43] The intervention consisted of 9 sessions over a 2-month period, intercalating 5 educational sessions with 4 autogenic training sessions. The educative sessions included information about typical symptoms, usual course, comorbid medical conditions, potential causes of the illness, the influence of psychosocial factors on pain, current pharmacologic and nonpharmacologic treatments, the benefits of regular exercise, and the typical barriers to behavior change. The autogenic training sessions focused on immediate physical and mental relaxation, pain relief, and stress reduction, |
| Ref. [40] The MINDSET (MINDfulneSs & EducaTion) program included intercalated four sessions of psychoeducation and four sessions of mindfulness training. Education sessions focused on: (1) overview of FM, (2) the pillars of good health, (3) emotion management and communication skills, (4) services and resources. Mindfulness sessions focused on: (1) mindfulness and chronic pain, (2) focus on the breath, thoughts and emotions, (3) management of unpleasant experiences, (4) action plan for the daily use of mindfulness. |
| Refs. [41,42] The eight Mindfulness-Based Stress Reduction sessions introduced and practiced techniques to change the reaction to pain: the raisin-eating task, the inquiry, and the body scan, conscious movements, the 9-point exercise, sitting meditation, walking meditation, and the metta exercise. The eight FibroQoL sessions focused on (1) updated medical information on FM, (2) physical and emotional pain, (3) diagnosis and treatment, (4) personal goals and obstacles, (5) self-esteem and emotions, (6) plans for personal changes, (7) review of achievements, and (8) the role of specialized care. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-de-Regil, L. Psychoeducation for Patients with Fibromyalgia: A Systematic Review. Healthcare 2021, 9, 737. https://doi.org/10.3390/healthcare9060737
Gómez-de-Regil L. Psychoeducation for Patients with Fibromyalgia: A Systematic Review. Healthcare. 2021; 9(6):737. https://doi.org/10.3390/healthcare9060737
Chicago/Turabian StyleGómez-de-Regil, Lizzette. 2021. "Psychoeducation for Patients with Fibromyalgia: A Systematic Review" Healthcare 9, no. 6: 737. https://doi.org/10.3390/healthcare9060737
APA StyleGómez-de-Regil, L. (2021). Psychoeducation for Patients with Fibromyalgia: A Systematic Review. Healthcare, 9(6), 737. https://doi.org/10.3390/healthcare9060737