
Impact of Rehabilitation Dose on Nutritional Status at Discharge from a Convalescent Rehabilitation Ward in Malnourished Patients with Hip Fracture




Abstract
1. Introduction
2. Materials and Methods
2.1. Japan Rehabilitation Nutrition Database
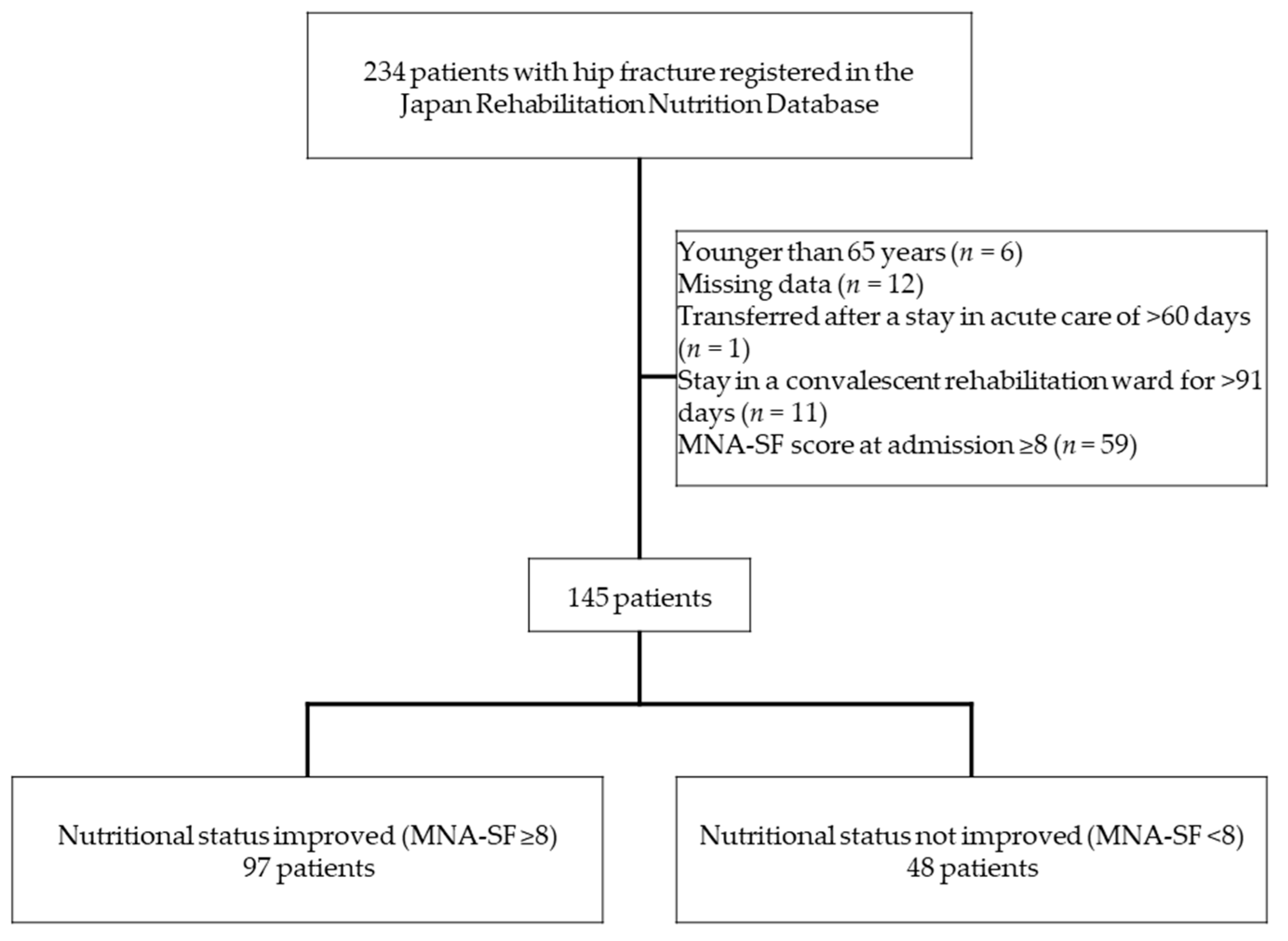
2.2. Participants
2.3. Main Outcome Measurement
2.4. Rehabilitation Dose
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miyasaka, D.; Endo, N.; Endo, E.; Sakuma, M.; Yamamoto, N.; Tanabe, N.; Imai, N.; Suda, K. Incidence of hip fracture in Niigata, Japan in 2004 and 2010 and the long-term trends from 1985 to 2010. J. Bone Miner. Metabol. 2016, 34, 92–98. [Google Scholar] [CrossRef]
- Orimo, H.; Yaegashi, Y.; Onoda, T.; Fukushima, Y.; Hosoi, T.; Sakata, K. Hip fracture incidence in Japan: Estimates of new patients in 2007 and 20-year trends. Arch. Osteoporos. 2009, 4, 71–77. [Google Scholar] [CrossRef]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair. 2011, 25, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S. Protein-energy malnutrition in the rehabilitation setting: Evidence to improve identification. Maturitas 2016, 86, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Churilov, I.; Churilov, L.; Maclsaac, R.J.; Ekinci, E.I. Systematic review and meta-analysis of prevalence of sarcopenia in post acute inpatient rehabilitation. Osteoporosis Int. 2018, 29, 805–812. [Google Scholar] [CrossRef]
- Inoue, H.; Morioka, K.; Okamoto, K.; Tsutsumi, H.; Ishino, S.; Kiritani, N.; Kubo, H.; Nara, M.; Tsuji, Y. Energy requirements for patients in convalescent rehabilitation using motor scores as in the Functional Independent Measure. Asia Pac. J. Clin. Nutr. 2019, 28, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Nii, M.; Maeda, K.; Wakabayashi, H.; Nishioka, S.; Tanaka, A. Nutritional improvement and energy intake are associated with functional recovery in patients after cerebrovascular disorders. J. Stroke Cerebrovasc. Dis. 2016, 25, 57–62. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE study group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Antoniak, A.E.; Greig, C.A. The effect of combined resistance exercise training and vitamin D 3 supplementation on musculoskeletal health and function in older adults: A systematic review and meta-analysis. BMJ Open 2017, 7, e014619. [Google Scholar] [CrossRef]
- Nishioka, S.; Wakabayashi, H.; Momosaki, R. Nutritional status changes and activities of daily living after hip fracture in convalescent rehabilitation wards: A retrospective observational cohort study from the Japan Rehabilitation Nutrition Database. J. Acad. Nutr. Diet. 2018, 118, 1270–1276. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The food intake LEVEL Scale. J. Pain Symptom Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Standard Tables of Food Composition in Japan-2015, Seventh Revised Edition. Available online: http://www.mext.go.jp/en/policy/science_technology/policy/title01/detail01/1374030.htm (accessed on 30 May 2021).
- Nishiyama, A.; Wakabayashi, H.; Nishioka, S.; Nagano, A.; Momosaki, R. Energy intake at admission for improving activities of daily living and nutritional status among convalescent stroke patients. Neurol. Med. Chir. 2019, 59, 313–320. [Google Scholar] [CrossRef]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA®- its history and challenges. J. Nutr. Health Aging 2006, 10, 456–463. [Google Scholar] [PubMed]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vallas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Guigoz, Y. The mini-nutritional assessment (MNA®) review of the literature—What does it tell us? J. Nutr. Health Aging 2006, 10, 466–485. [Google Scholar]
- Umezawa, H.; Kokura, Y.; Abe, S.; Suzuki, C.; Nishida, A.; Uchiyama, Y.; Maeda, K.; Wakabayashi, H.; Momosaki, R. Relationship Between Performance Improvement in Activities of Daily Living and Energy Intake in Older Patients with Hip Fracture Undergoing Rehabilitation. Ann. Rehabil. Med. 2019, 43, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, J.E.; Murton, A.J. Mechanisms responsible for disuse muscle atrophy: Potential role of protein provision and exercise as countermeasures. Nutrition 2013, 29, 22–28. [Google Scholar] [CrossRef]
- Drummond, M.J.; Dreyer, H.C.; Fry, C.S.; Glynn, E.L.; Rasmussen, B.B. Nutritional and contractile regulation of human skeletal muscle protein synthesis and mTORC1 signaling. J. Appl. Physiol. 2009, 106, 1374–1384. [Google Scholar] [CrossRef]
- Abizanda, P.; López, M.D.; Garcia, V.P.; Estrella, J.D.; Gonzalez, A.S.; Vilardell, N.B.; Torres, K.A. Effects of an Oral Nutritional Supplementation Plus Physical Exercise Intervention on the Physical Function, Nutritional Status, and Quality of Life in Frail Institutionalized Older Adults: The ACTIVNES Study. J. Am. Med. Dir. Assoc. 2015, 16, 439.e9–439.e16. [Google Scholar] [CrossRef]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Kirk-Sanchez, N.J.; Roach, K.E. Relationship between duration of therapy services in a comprehensive rehabilitation program and mobility at discharge in patients with orthopedic problems. Phys. Ther. 2001, 81, 888–895. [Google Scholar] [CrossRef]
- Nishioka, S.; Wakabayashi, H.; Nishioka, E.; Yoshida, T.; Mori, N.; Watanabe, R. Nutritional Improvement Correlates with Recovery of Activities of Daily Living among Malnourished Elderly Stroke Patients in the Convalescent Stage: A Cross-Sectional Study. J. Acad. Nutr. Diet. 2016, 116, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Kaifukuki Rehabilitation Ward Association. 2019 Annual Report from the Annual Survey Committee of Kaifukuki Rehabilitation Ward Association; Kaifukuki Rehabilitation Ward Association: Tokyo, Japan, 2020. [Google Scholar]
- Paillaud, E.; Bories, P.N.; Le Parco, J.C.; Campillo, B. Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up. Br. J. Nutr. 2000, 83, 97–103. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bell, J.J.; Bauer, J.D.; Capra, S.; Pulle, C.R. Multidisciplinary, multi-modal nutritional care in acute hip fracture inpatients-results of a pragmatic intervention. Clin. Nutr. 2014, 33, 1101–1107. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Overall (n = 145) | Nutritional Status Improved (n = 97) | Nutritional Status Not Improved (n = 48) | p-Value |
|---|---|---|---|---|
| Age, years, mean ± SD | 85.1 ± 7.9 | 84.2 ± 6.9 | 86.9 ± 9.6 | 0.009 a |
| Female sex, n (%) | 118 (81) | 80 (82) | 38 (79) | 0.630 c |
| CCI, median (IQR) | 1 (0–2) | 1 (0–2) | 1 (1–2) | 0.225 b |
| Admission FIM score, median (IQR) | 63 (46–81) | 71 (55–85.5) | 46 (33.3–64.5) | <0.001 b |
| Admission MNA-SF score, median (IQR) | 5 (4–6) | 5 (4–6.5) | 4 (3–5.8) | <0.001 b |
| Admission FILS score, median (IQR) | 9 (8–10) | 9 (8–10) | 8 (7–9.8) | <0.001 b |
| Energy intake, kcal/day, median (IQR) | 1400 (1160–1400) | 1400 (1260–1490) | 1200 (1008.5–1400) | <0.001 b |
| Daily rehabilitation dose, min/day, median (IQR) | 109.5 (94.6–116.2) | 110.6 (103.3–117.9) | 101.11 (77.4–113) | 0.008 b |
| Hospital stay, days median (IQR) | 71 (50.5–85) | 73 (50.5–85) | 67.5 (50–84.8) | 0.696 b |
| Number of hospital beds, median (IQR) | 104 (50.5–206) | 206 (60–206) | 60 (40–206) | 0.012 b |
| Variables | Age | CCI | Admission FIM | Admission MNA-SF® | Admission FILS | Energy Intake | Daily Rehabilitation Dose | Length of Hospital Stay | Number of Hospital Beds |
|---|---|---|---|---|---|---|---|---|---|
| Age | 1 | −0.079 | −0.303 ** | −0.159 | −0.216 ** | −0.210 * | 0.028 | 0.295 ** | 0.061 |
| CCI | 1 | −0.125 | −0.058 | −0.128 | −0.020 | 0.018 | 0.050 | −0.032 | |
| Admission FIM | 1 | 0.359 ** | 0.514 ** | 0.330 ** | 0.173 * | −0.315 ** | 0.255 ** | ||
| Admission MNA-SF® | 1 | 0.413 ** | 0.270 ** | 0.062 | −0.174 * | −0.120 | |||
| Admission FILS | 1 | 0.357 ** | 0.055 | −0.160 | 0.074 | ||||
| Energy intake | 1 | 0.151 | −0.091 | 0.283 ** | |||||
| Daily rehabilitation dose | 1 | 0.135 | 0.315 ** | ||||||
| Length of hospital stay | 1 | 0.045 | |||||||
| Number of hospital beds | 1 |
| Variables | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.970 | 0.914 | 1.030 | 0.321 |
| Sex | 0.448 | 0.140 | 1.438 | 0.177 |
| CCI | 0.866 | 0.588 | 1.275 | 0.467 |
| Admission FIM score | 1.042 | 1.016 | 1.068 | 0.001 |
| Admission MNA-SF score | 1.349 | 0.991 | 1.837 | 0.057 |
| Admission FILS score | 0.987 | 0.684 | 1.423 | 0.944 |
| Energy intake | 1.002 | 1.000 | 1.004 | 0.048 |
| Daily rehabilitation dose | 1.023 | 1.002 | 1.045 | 0.031 |
| Length of hospital stay | 1.026 | 1.003 | 1.049 | 0.023 |
| Center | 1.234 | 0.976 | 1.562 | 0.079 |
| Number of hospital beds | 1.001 | 0.995 | 1.008 | 0.742 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, Y.; Wakabayashi, H.; Nishioka, S.; Nomura, S.; Momosaki, R. Impact of Rehabilitation Dose on Nutritional Status at Discharge from a Convalescent Rehabilitation Ward in Malnourished Patients with Hip Fracture. Healthcare 2021, 9, 722. https://doi.org/10.3390/healthcare9060722
Ito Y, Wakabayashi H, Nishioka S, Nomura S, Momosaki R. Impact of Rehabilitation Dose on Nutritional Status at Discharge from a Convalescent Rehabilitation Ward in Malnourished Patients with Hip Fracture. Healthcare. 2021; 9(6):722. https://doi.org/10.3390/healthcare9060722
Chicago/Turabian StyleIto, Yusuke, Hidetaka Wakabayashi, Shinta Nishioka, Shin Nomura, and Ryo Momosaki. 2021. "Impact of Rehabilitation Dose on Nutritional Status at Discharge from a Convalescent Rehabilitation Ward in Malnourished Patients with Hip Fracture" Healthcare 9, no. 6: 722. https://doi.org/10.3390/healthcare9060722
APA StyleIto, Y., Wakabayashi, H., Nishioka, S., Nomura, S., & Momosaki, R. (2021). Impact of Rehabilitation Dose on Nutritional Status at Discharge from a Convalescent Rehabilitation Ward in Malnourished Patients with Hip Fracture. Healthcare, 9(6), 722. https://doi.org/10.3390/healthcare9060722