
Opportunities and Problems of the Consensus Conferences in the Care Robotics


Abstract
:1. Introduction
- Robotic surgery
- Care and socially assistive robots
- Rehabilitation systems
- Training for health and care workers
1.1. The Care Robots: Advantages and Disadvantages
1.2. The Strong Need of the Agreement Initiatives in Care Robotics
1.3. The Purpose and Structure of the Study
2. The Consensus Conferences: Brief Reminder and Relevance
2.1. An Organizing Committee Starts the Work of the Conference
2.2. The Working Groups (WG) Plays a Fundamental Role
3. The Consensus Conferences and the Care Robots: State of Application, Opportunities, and Problems
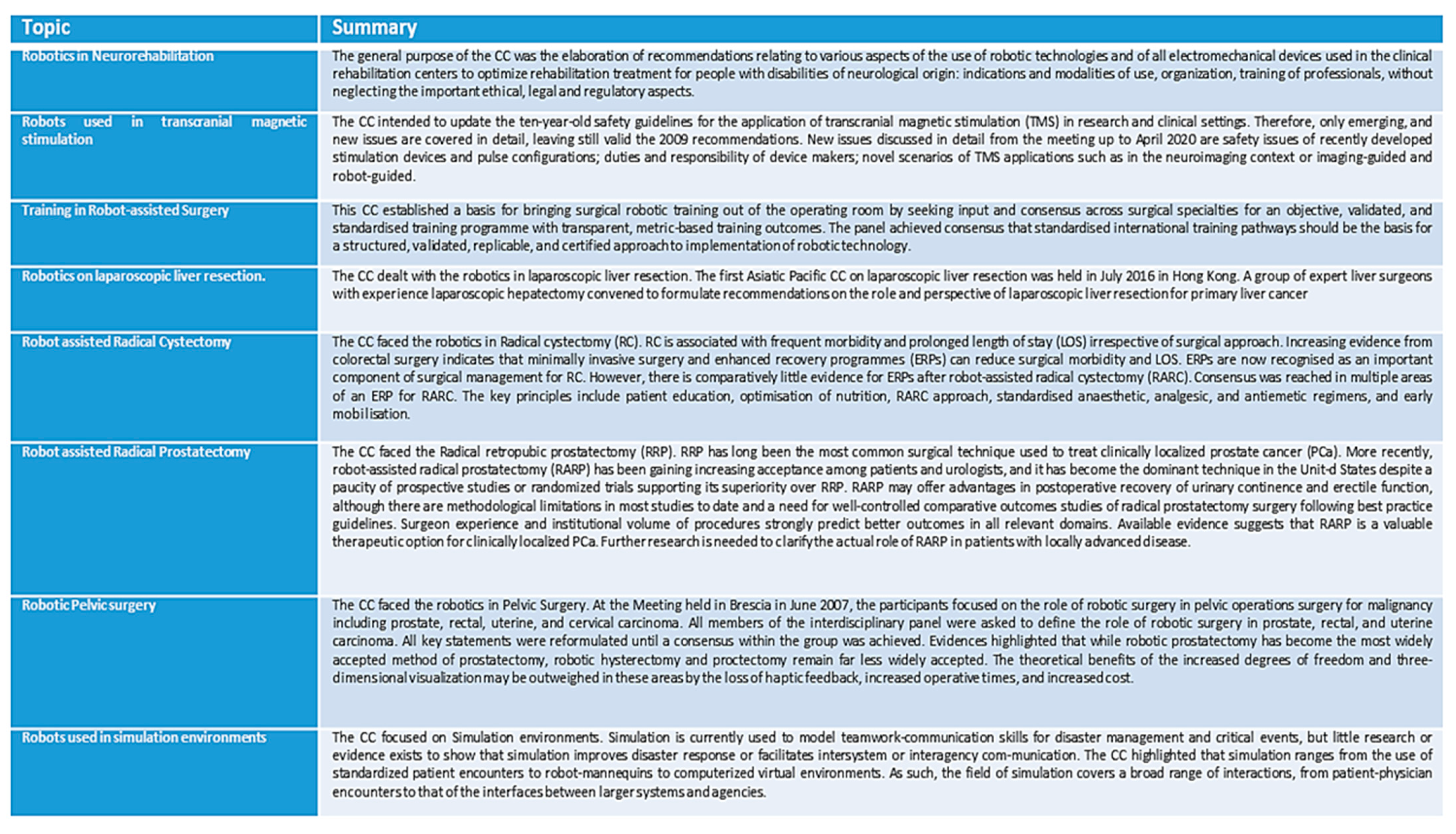
3.1. The State of Application
- With the key: (consensus conference) AND (surgery) [Title/Abstract]) [41] 1.676 results.
- With the key: (consensus conference) AND (rehabilitation) [Title/Abstract]) [42] 372 results.
- With the key: (consensus conference) AND (assistance) [Title/Abstract]) [43] 94 results.
- With the key: (consensus conference) AND (training) [Title/Abstract]) [44] 800 results.
3.2. Opportunities and Emerging Problems
3.3. Aspects Not Adequately Explored in the Consensus Conferences in Robotics
- The implications with ethics, regulatory aspects and in the new emerging risks (for example Cybersecurity).Ethics has an important role and a peculiarity on the CRs, such as on the SRs. The ethical issues on CRs have identified two macro-sectors [5,6]. The first macro-sector is the ethics in a responsible research and innovation [5]. The second macro-sector is the ethics problem encountered while building moral CRs [6]. There are shadows in EU Medical Device (MD) regulations [52]. First, they focus a lot on manufacturers and little on recipients/users. Second, the intended use and certification [53], must be aligned, and this is not always easily feasible in the field of the medical devices; for this reason the health domain supervisory systems are always active with monitoring actions. There are limits in the application of specific Cyb certifications. They are voluntary, as in the case of the Cybersecurity ACT [54]. The CRs would need an ad hoc regulatory framework, in consideration of the peculiarities [8].
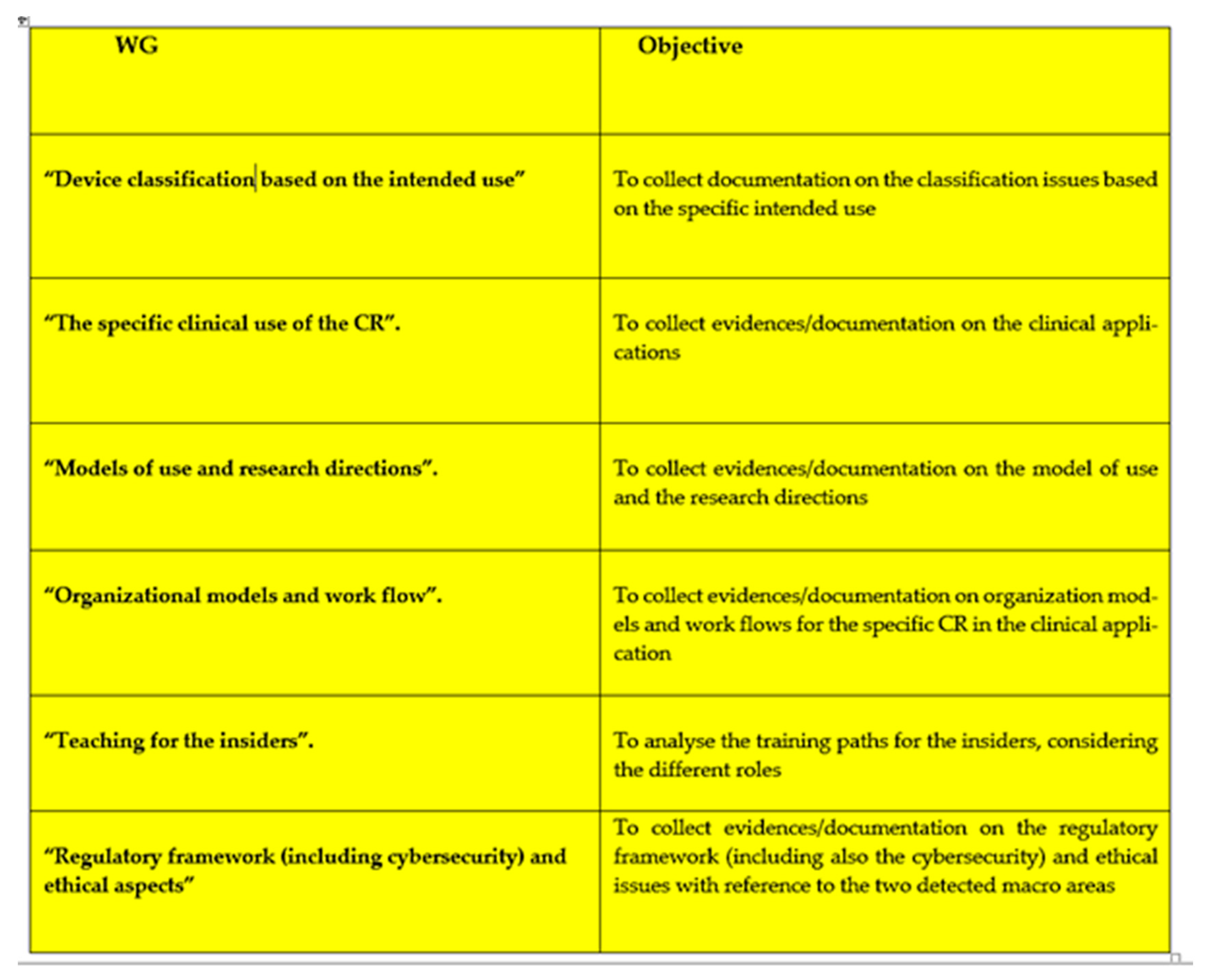
- How to organize the WGs considering the peculiarity of the CR. The organization of the WGs has a basic importance. The principal question, to be answered by the CC, is, indeed, divided into articulated sub-questions. In robotics, as in other fields, the success of a CC depends on how the sub-questions assigned to each WG are articulated.
- Definitions and classification criteria for the devices based on the intended use.
- Indications on the specific clinical use of devices in clinical applications.
- Scientific References and consolidated experience for the development of the CRs.
- Organizational contexts and changes in the workflow.
- Regulatory framework (including the cybersecurity) and ethical issues for the devices.
4. Conclusions
Final Reflection
- Initiatives of greater diffusion of the methodology through tools that give it wide visibility.
- Census and categorization of the past and ongoing CCs.
- Coordination and initiation of CC programs at both national and international level involving the greatest number of experts.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Summary of the Highlights from the Studies from Pubmed
Appendix A.2. The WGs Architecture for a Consensus Conference on the CRs in a Defined Clinical Application
References
- Dolic, Z.; Castro, R.; Moarcas, A. Robots in Healthcare: A Solution or a Problem? Study for the Committee on Environment, Public Health, and Food Safety. Luxembourg: Policy Department for Economic, Scientific and Quality of Life Policies, European Parliament. 2019. Available online: https://www.europarl.europa.eu/RegData/etudes/IDAN/2019/638391/IPOL_IDA(2019)638391_EN.pdf (accessed on 20 November 2021).
- Available online: https://www.granta-automation.co.uk/news/advantages-and-disadvantages-of-robotic-automation/ (accessed on 20 November 2021).
- Available online: https://www.futurelearn.com/info/courses/begin-robotics/0/steps/2845 (accessed on 20 November 2021).
- Available online: https://www.delveinsight.com/blog/robotics-in-healthcare (accessed on 20 November 2021).
- Stahl, B.C.; Coeckelbergh, M. Ethics of healthcare robotics: Towards responsible research and innovation. Robot. Auton. Syst. 2016, 86, 152–161. [Google Scholar] [CrossRef]
- Gordon, J.-S. Building Moral Robots: Ethical Pitfalls and Challenges. Sci. Eng. Ethic 2020, 26, 141–157. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=robot%5BTitle%2FAbstract%5D&sort=date (accessed on 8 September 2021).
- Fosch-Villaronga, E.; Mahler, T. Cybersecurity, safety and robots: Strengthening the link between cybersecurity and safety in the context of care robots. Comput. Law Secur. Rev. 2021, 41, 105528. [Google Scholar] [CrossRef]
- Yaacoub, J.-P.A.; Noura, H.N.; Salman, O.; Chehab, A. Robotics cyber security: Vulnerabilities, attacks, countermeasures, and recommendations. Int. J. Inf. Secur. 2021, 1–44. [Google Scholar] [CrossRef]
- Available online: http://www.rssp.salute.gov.it/rssp2012/paginaCapitoloRssp2012.jsp?sezione=ssn&capitolo=modelli&lingua=italiano (accessed on 8 September 2021).
- Cochrane, A.L. Effectiveness and Efficiency: Random Reflections on Health Services; Nuffield Provincial Hospital Trust: London, UK, 1972. [Google Scholar]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.M.; Haynes, R.B.; Richardson, W.S. Evidence-based medicine: What it is and what it isn’t. Br. Med. J. 1996, 312, 71–72. [Google Scholar] [CrossRef] [Green Version]
- Haynes, R.B.; Sackett, D.L. Richardson W. Evidence-based medicine: How to practice & teach EBM. Can. Med. Assoc. J. 1997, 157, 788. [Google Scholar]
- Available online: https://www.ebm-guidelines.com/dtk/ebmg/home (accessed on 20 November 2021).
- Luce, B.R.; Drummond, M.; Jönsson, B.; Neumann, P.J.; Schwartz, J.S.; Siebert, U.; Sullivan, S.D. EBM, HTA, and CER: Clearing the Confusion. Milbank Q. 2010, 88, 256–276. [Google Scholar] [CrossRef] [Green Version]
- Office of Technology Assessment. 1978. Assessing the Efficacy and Safety of Medical Technologies. September. NTIS order #PB-286929. Available online: http://www.fas.org/ota/reports/7805.pdf (accessed on 25 November 2009).
- INAHTA (International Network of Agencies for Health Technology Assessment). 2009. HTA Resources. Available online: http://www.inahta.org/HTA/ (accessed on 25 November 2009).
- Candiani, G.; Colombo, C.; Draghini, R.; Magrini, M.; Mosconi, P.; Nonino, F.; Satolli, R. Come Organizzare Una Conferenza di Consenso; Manuale Metodologico; ISS-SNLG: Roma, Italy, 2009. [Google Scholar]
- Arcelloni, M.C.; Broggi, F.; Cortese, S.; Della Corte, G.; Pirozzolo, V. CONSENSUS CONFERENCE: UNO STRUMENTO PER LA PRATICA CLINICA Riferimenti storico-metodologici e stato dell’arte dei lavori italiani sul Disturbo Primario del Linguaggio e sui Disturbi Specifici dell’Apprendimento. Available online: https://rivistedigitali.erickson.it/il-tnpee/archivio/vol-1-n-1/riferimenti-storico-metodologici-e-stato-dellarte-dei-lavori-italiani-sul-disturbo-primario-del-linguaggio-e-sui-disturbi-specifici-dellapprendimento/ (accessed on 20 November 2021).
- McGlynn, E.A.; Kosecoff, J.; Brook, R.H. Format and Conduct of Consensus Development Conferences. Int. J. Technol. Assess. Heal. Care 1990, 6, 450–469. [Google Scholar] [CrossRef]
- Agence Nationale d’Accréditation et d’Évaluation en Santé; Les Conférences de consensus. Base Méthodologique Pour Leur Réalisation en France; ANAES: Paris, France, 1999. [Google Scholar]
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28consensus+conference%29+AND+%28robot%5BTitle%2FAbstract%5D%29&sort=date (accessed on 20 November 2021).
- Gimigliano, F.; Palomba, A.; Arienti, C.; Morone, G.; Perrero, L.; Agostini, M.; Aprile, I.; Paci, M.; Casanova, E.; Marino, D.; et al. Robot-assisted arm therapy inneurological health conditions: Rationale and methodology for the evidencesynthesis in the CICERONE Italian Consensus Conference. Eur. J. Phys. Rehabil. Med. 2021, 57, 824–830. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Sorrentino, G.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; et al. Robotic-assisted gait rehabilitation following stroke: A systematic review of current guidelines and practical clinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 460–471. [Google Scholar] [CrossRef]
- Morone, G.; Palomba, A.; Martino Cinnera, A.; Agostini, M.; Aprile, I.; Arienti, C.; Paci, M.; Casanova, E.; Marino, D.; LARosa, G.; et al. “CICERONE” Italian Consensus Conference on Robotic in Neurorehabilitation.Systematic review of guidelines to identify recommendations for upper limb robotic rehabilitation after stroke. Eur. J. Phys. Rehabil. Med. 2021, 57, 238–245. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Basis of this article began with a Consensus Statement from the IFCN Workshop on “Present, Future of TMS: Safety, Ethical Guidelines”, Siena, October 17–20, 2018, updating through April 2020. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Cocchi, I.; Paolucci, S.; Iosa, M. Robot-assisted therapy for arm recovery for stroke patients: State of the art and clinical implication. Expert Rev. Med. Devices 2020, 17, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Vanlander, A.E.; Mazzone, E.; Collins, J.W.; Mottrie, A.M.; Rogiers, X.M.; van der Poel, H.G.; Van Herzeele, I.; Satava, R.M.; Gallagher, A.G. Orsi Consensus Meeting on European Robotic Training (OCERT): Results from the First Multispecialty Consensus Meeting on Training in Robot-assisted Surgery. Eur. Urol. 2020, 78, 713–716. [Google Scholar] [CrossRef]
- Collins, J.W.; Levy, J.; Stefanidis, D.; Gallagher, A.; Coleman, M.; Cecil, T.; Ericsson, A.; Mottrie, A.; Wiklund, P.; Ahmed, K.; et al. Utilising the Delphi Process to Develop a Proficiency-based Progression Train-the-trainer Course for Robotic Surgery Training. Eur. Urol. 2019, 75, 775–785. [Google Scholar] [CrossRef]
- Cheung, T.T.; Han, H.S.; She, W.H.; Chen, K.H.; Chow, P.K.H.; Yoong, B.K.; Lee, K.F.; Kubo, S.; Tang, C.N.; Wakabayashi, G. The Asia Pacific Consensus Statement on Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Report from the 7th Asia-Pacific Primary Liver Cancer Expert Meeting Held in Hong Kong. Liver Cancer 2018, 7, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Montagnini, A.L.; Røsok, B.I.; Asbun, H.J.; Barkun, J.; Besselink, M.G.; Boggi, U.; Conlon, K.C.; Fingerhut, A.; Han, H.S.; Hansen, P.D.; et al. Standardizing terminology for minimally invasive pancreatic resection. HPB 2017, 19, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.W.; Patel, H.; Adding, C.; Annerstedt, M.; Dasgupta, P.; Khan, S.M.; Artibani, W.; Gaston, R.; Piechaud, T.; Catto, J.W.; et al. Enhanced Recovery After Robot-assisted Radical Cystectomy: EAU Robotic Urology Section Scientific Working Group Consensus View. Eur. Urol. 2016, 70, 649–660. [Google Scholar] [CrossRef]
- Chan, K.G.; Guru, K.; Wiklund, P.; Catto, J.; Yuh, B.; Novara, G.; Murphy, D.G.; Al-Tartir, T.; Collins, J.W.; Zhumkhawala, A.; et al. Pasadena Consensus Panel. Robot- assisted radical cystectomy and urinary diversion: Technical recommendations from the Pasadena Consensus Panel. Eur. Urol. 2015, 3, 423–431. [Google Scholar] [CrossRef]
- Wilson, T.G.; Guru, K.; Rosen, R.C.; Wiklund, P.; Annerstedt, M.; Bochner, B.H.; Chan, K.G.; Montorsi, F.; Mottrie, A.; Murphy, D.; et al. Best practices in robot-assisted radical cystectomy and urinary reconstruction: Recommendations of the Pasadena Consensus Panel. Eur. Urol. 2015, 67, 363–375. [Google Scholar] [CrossRef]
- Ficarra, V.; Wiklund, P.N.; Rochat, C.H.; Dasgupta, P.; Challacombe, B.J.; Sooriakumaran, P.; Siemer, S.; Suardi, N.; Novara, G.; Mottrie, A. The European Association of Urology Robotic Urology Section (ERUS) survey of robot-assisted radical prostatectomy (RARP). BJU Int. 2013, 111, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montorsi, F.; Wilson, T.G.; Rosen, R.C.; Ahlering, T.E.; Artibani, W.; Carroll, P.R.; Costello, A.; Eastham, J.A.; Ficarra, V.; Guazzoni, G.; et al. Best practices in robot-assisted radical prostatectomy: Recommendations of the Pasadena Consensus Panel. Eur. Urol. 2012, 62, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Pelton, T.; van Vliet, P.; Hollands, K. Interventions for improving coordination of reach to grasp following stroke: A systematic review. JBI Libr. Syst. Rev. 2011, 9, 1226–1270. [Google Scholar] [CrossRef] [PubMed]
- Wexner, S.D.; Bergamaschi, R.; Lacy, A.; Udo, J.; Brölmann, H.; Kennedy, R.H.; John, H. The current status of robotic pelvic surgery: Results of a multinational interdisciplinary consensus conference. Surg Endosc. 2009, 23, 438–443. [Google Scholar] [CrossRef]
- Kaji, A.H.; Bair, A.; Okuda, Y.; Kobayashi, L.; Khare, R.; Vozenilek, J. Defining systems expertise: Effective simulation at the organizational level--implications for patient safety, disaster surge capacity, and facilitating the systems interface. Acad. Emerg. Med. 2008, 15, 1098–1103. [Google Scholar] [CrossRef]
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=consensus+conference&sort=date&size=200 (accessed on 20 November 2021).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28consensus+conference%29+AND+%28surgery%5BTitle%2FAbstract%5D%29&sort=date (accessed on 20 November 2021).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28consensus+conference%29+AND+%28rehabilitation%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 20 November 2021).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28consensus+conference%29+AND+%28assistance%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 20 November 2021).
- Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28consensus+conference%29+AND+%28training+%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 20 November 2021).
- Available online: https://www.simfer.it/conferenza-di-consenso-sulla-robotica-23-e-28-ottobre-2020/ (accessed on 20 November 2021).
- Available online: https://www.iss.it/news/-/asset_publisher/gJ3hFqMQsykM/content/riabilitazione-assistita-da-robot-all-iss-la-consensus-conference (accessed on 20 November 2021).
- Available online: https://springerhealthcare.it/mr/archivio/la-conferenza-italiana-di-consenso-sulla-robotica-in-riabilitazione/ (accessed on 20 November 2021).
- Available online: https://www.atia.org/home/at-resources/what-is-at/ (accessed on 20 November 2021).
- Available online: https://www.who.int/health-topics/assistive-technology#tab=tab_1 (accessed on 20 November 2021).
- Available online: https://fli.it/tag/consensus-conference/ (accessed on 20 November 2021).
- Available online: https://www.sidin.org/2020/07/consensus-conference-2020-progetto-cad/ (accessed on 20 November 2021).
- Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on medical devices, amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and repealing Council Directives 90/385/EEC and 93/42/EEC.2017. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32017R0745 (accessed on 20 November 2021).
- Boldrini, P.; Bonaiuti, D.; Mazzoleni, S.; Posteraro, F. Rehabilitation assisted by robotic and electromechanical devices for people with neurological disabilities: Contributions for the preparation of a national conference in Italy. Eur. J. Phys. Rehabil. Med. 2021, 57, 458–459. [Google Scholar] [CrossRef]
- Available online: https://digital-strategy.ec.europa.eu/en/policies/cybersecurity-act (accessed on 20 November 2021).

| Reference | Application |
|---|---|
| [23,24,25] | Robotics in neurorehabilitation |
| [26] | Robots used in transcranial magnetic stimulation |
| [28] | Training in robot-assisted Surgery |
| [30] | Robotics on laparoscopic liver resection. |
| [32,33,34] | Robot assisted radical cystectomy |
| [35,36] | Robot assisted radical prostatectomy |
| [38] | Robotic pelvic surgery |
| [39] | Robots used in simulation environments |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maccioni, G.; Ruscitto, S.; Gulino, R.A.; Giansanti, D. Opportunities and Problems of the Consensus Conferences in the Care Robotics. Healthcare 2021, 9, 1624. https://doi.org/10.3390/healthcare9121624
Maccioni G, Ruscitto S, Gulino RA, Giansanti D. Opportunities and Problems of the Consensus Conferences in the Care Robotics. Healthcare. 2021; 9(12):1624. https://doi.org/10.3390/healthcare9121624
Chicago/Turabian StyleMaccioni, Giovanni, Selene Ruscitto, Rosario Alfio Gulino, and Daniele Giansanti. 2021. "Opportunities and Problems of the Consensus Conferences in the Care Robotics" Healthcare 9, no. 12: 1624. https://doi.org/10.3390/healthcare9121624
APA StyleMaccioni, G., Ruscitto, S., Gulino, R. A., & Giansanti, D. (2021). Opportunities and Problems of the Consensus Conferences in the Care Robotics. Healthcare, 9(12), 1624. https://doi.org/10.3390/healthcare9121624