
Patient Throughput Initiatives in Ambulatory Care Organizations during the COVID-19 Pandemic: A Systematic Review

 ,
,
Abstract
:1. Introduction
1.1. Rationale
- Frequency of patients seen
- Type of patients seen (example: routine vs. acute, primary care vs. specialty)
- Best practices to provide continuity of care during the pandemic and public health initiatives that potentially restrict normal (non-pandemic) clinic operations
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search
2.4. Initial Study Selection
3. Results
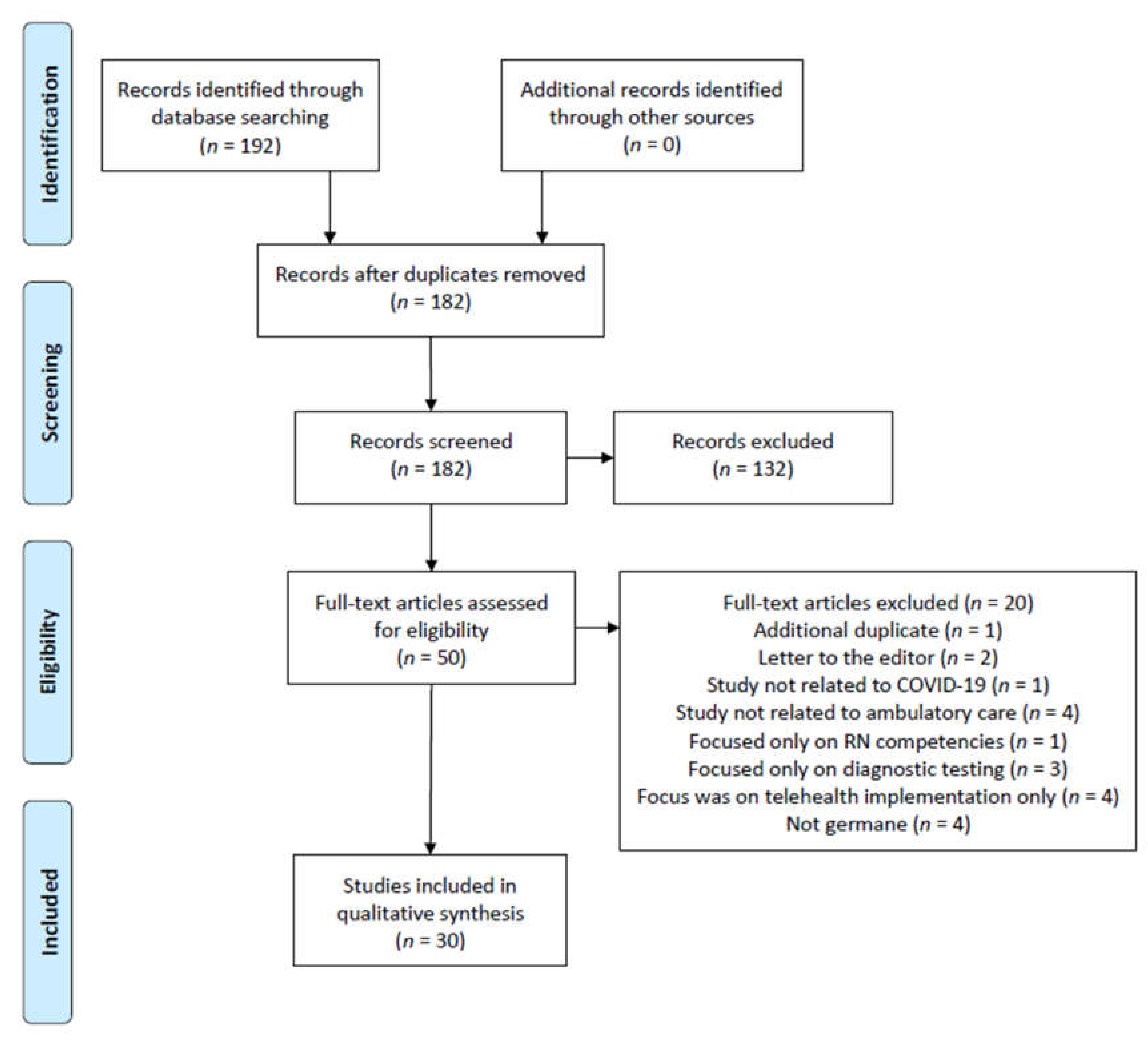
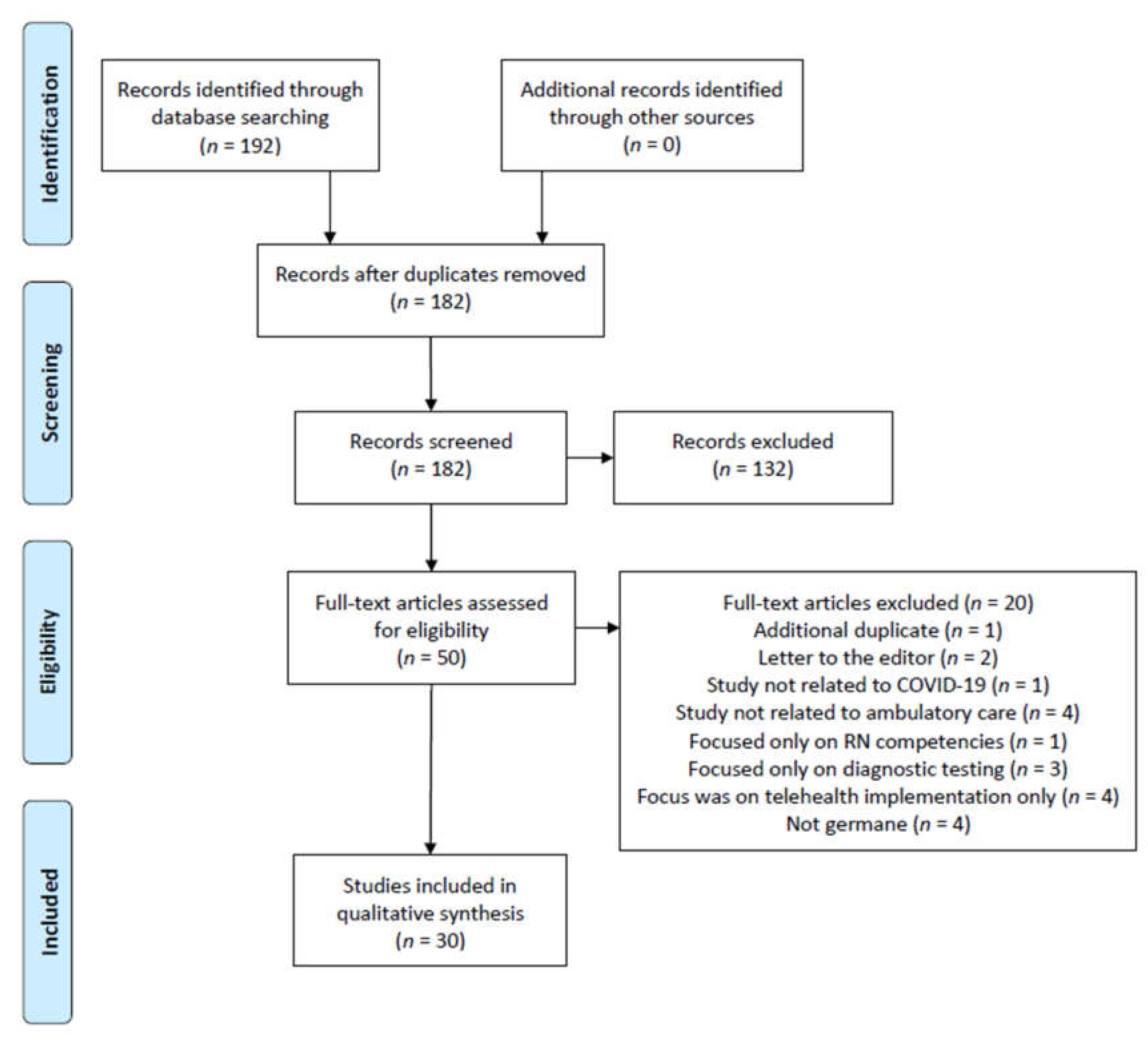
3.1. Study Selection/Exclusion
- an additional duplicate article identified (one article)
- letter to the editor (two articles)
- the article was not related to COVID-19 throughput analysis (one article)
- the article was not focused on ambulatory (outpatient) care (four articles)
- the article was a general nursing competency summary (one article)
- the article focused solely on diagnostic testing results (three articles)
- the article focused specifically on implementation of telehealth resources (four articles)
- the article was overall not germane to this review’s research topic (four articles)
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Additional Analysis
4. Discussion
4.1. Summary of Evidence
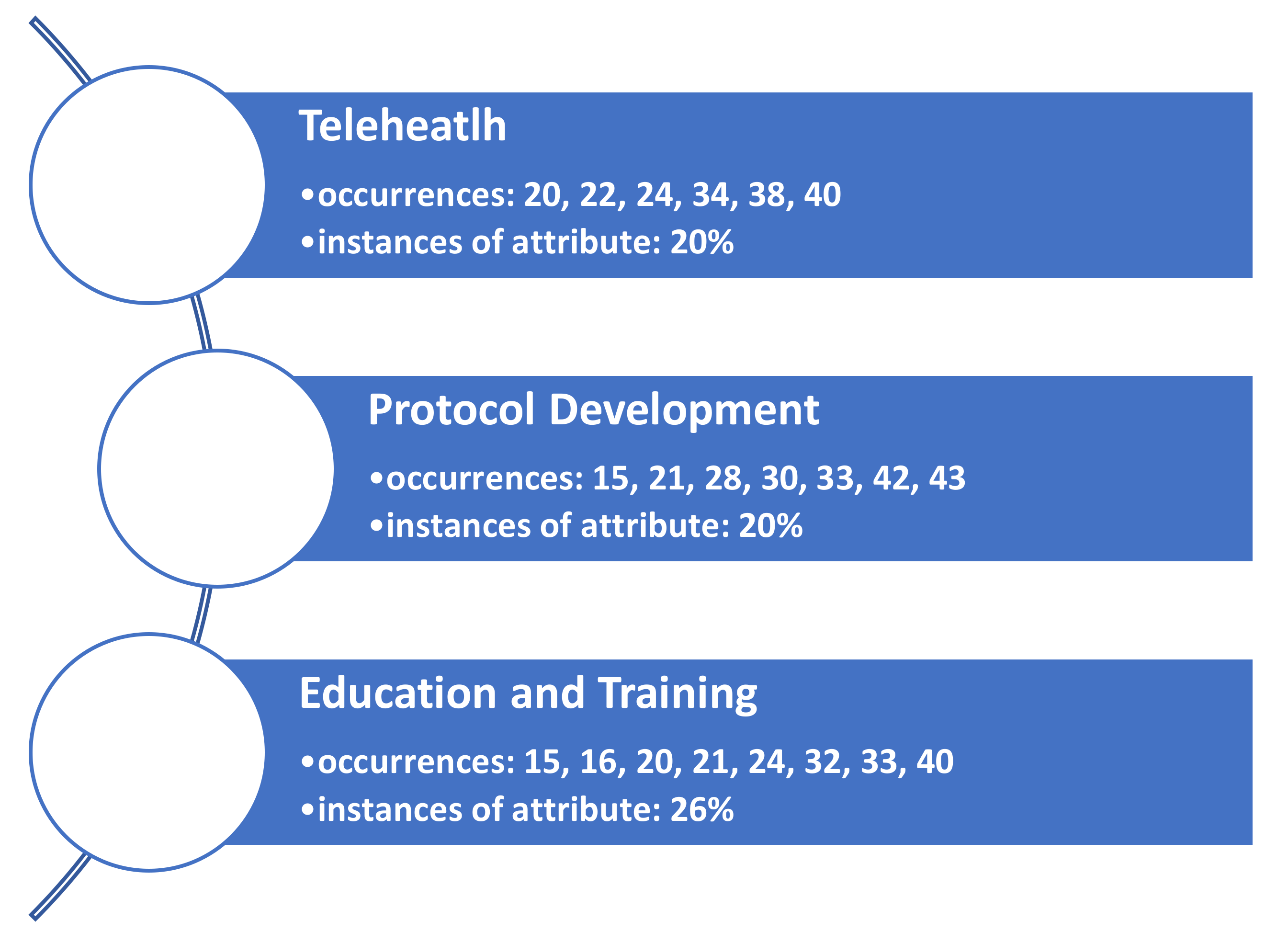
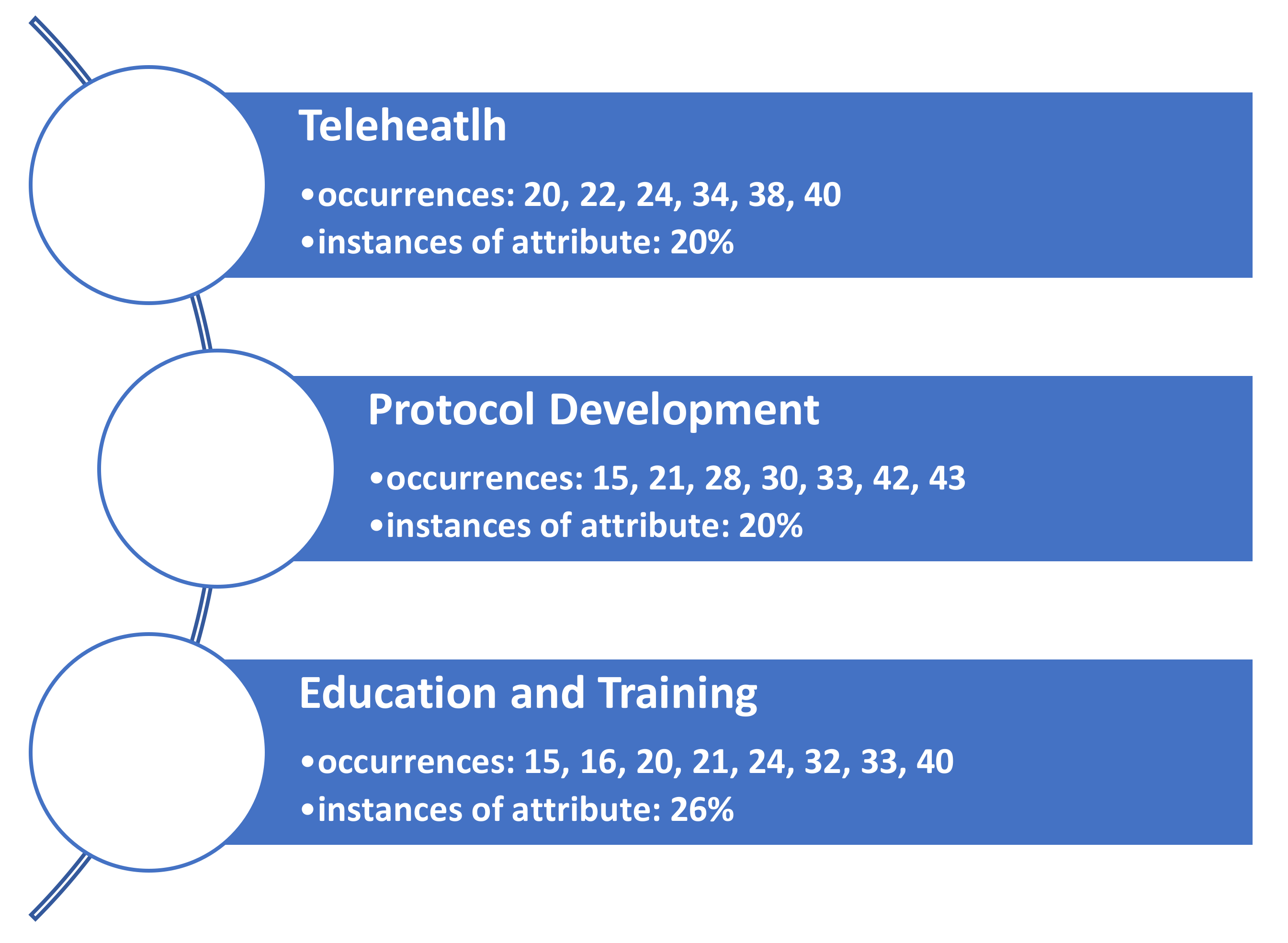
4.2. Facilitator to Patient Throughput: Telehealth
4.3. Facilitator to Patient Throughput: Protocol Development
4.4. Facilitator to Patient Throughput: Education and Training
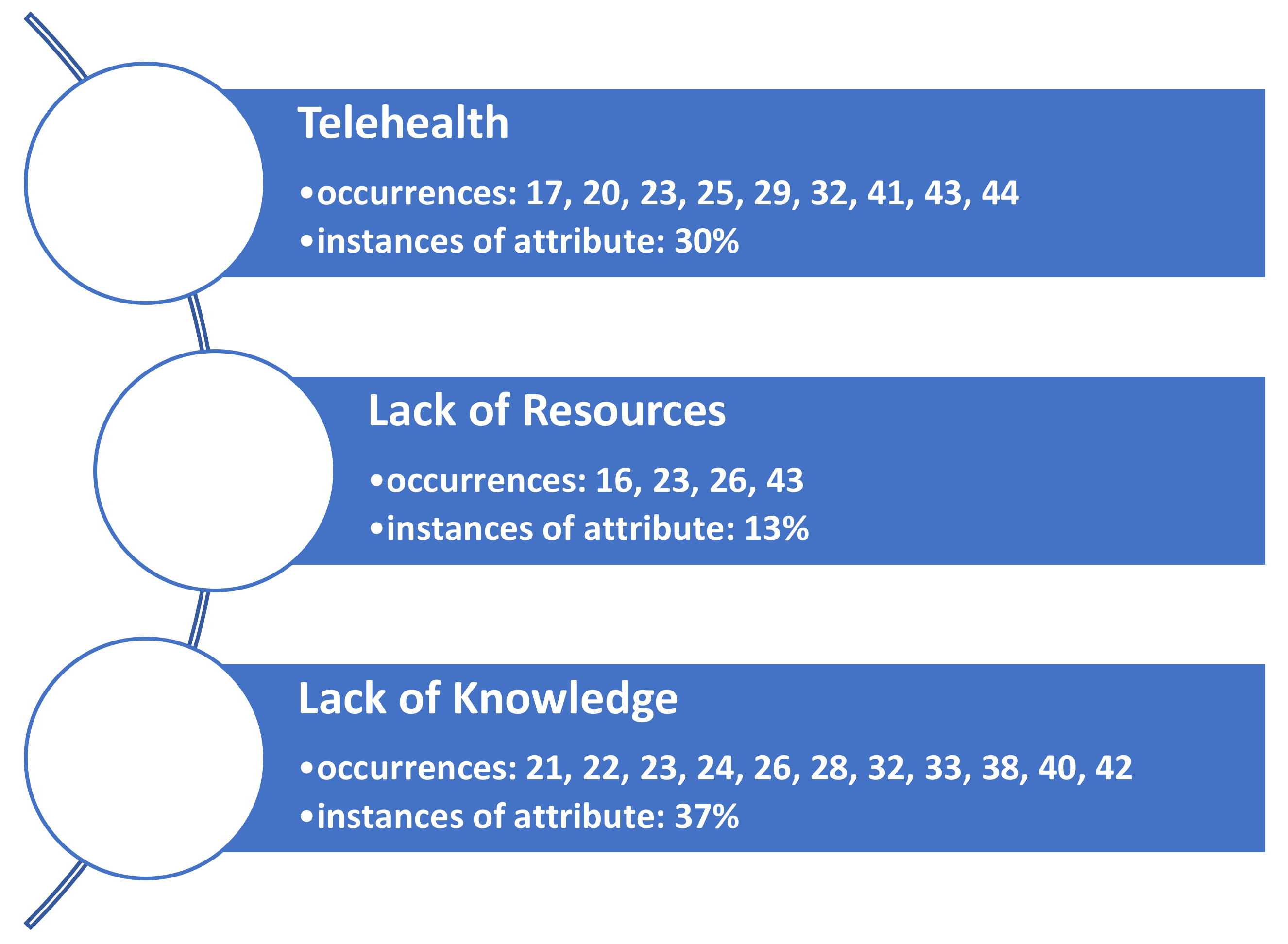
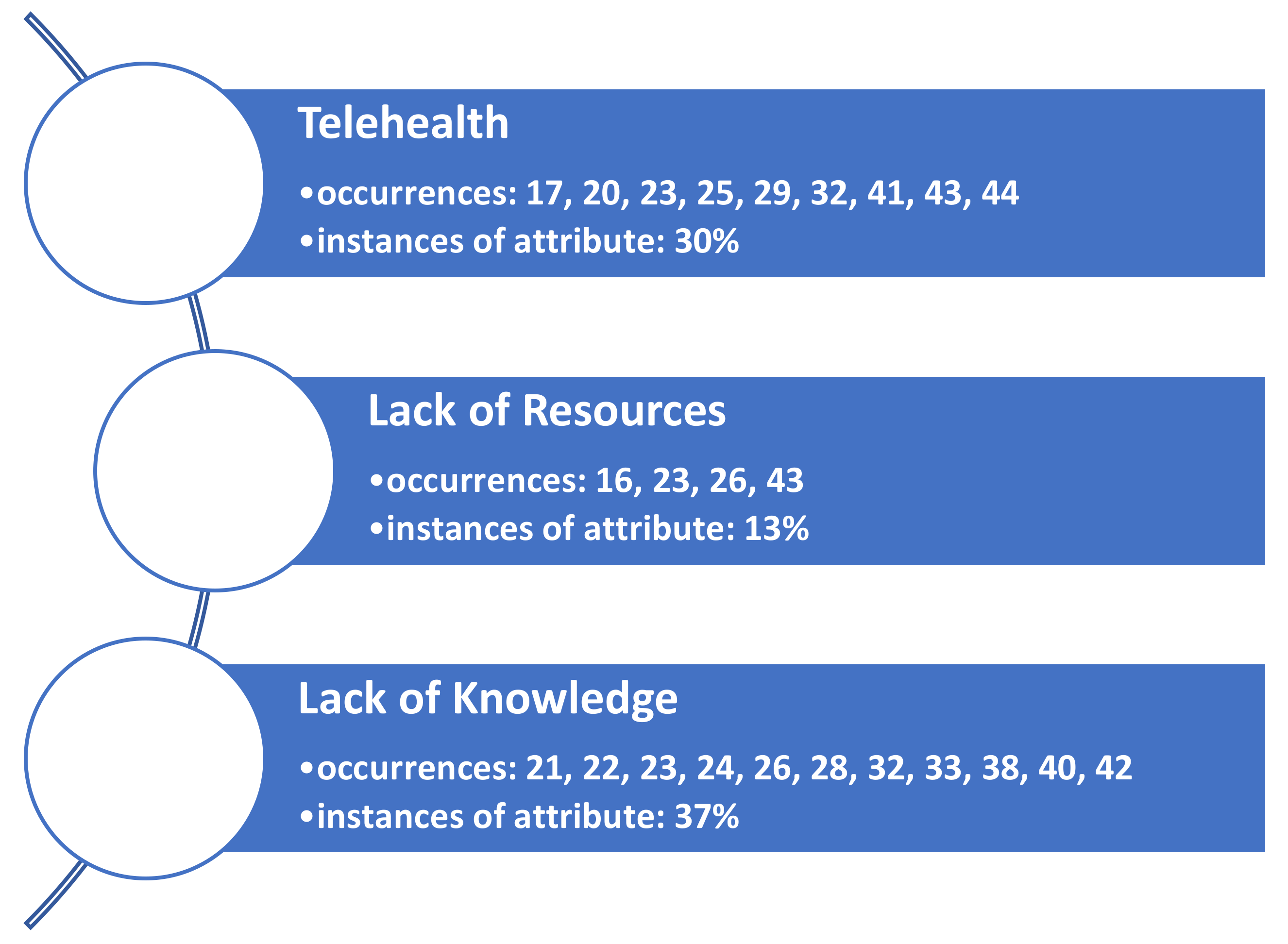
4.5. Barrier to Patient Throughput: Telehealth
4.6. Barrier to Patient Throughput: Lack of Resources
4.7. Barrier to Patient Throughput: Lack of Knowledge
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 15 July 2021).
- Walker, C.; Kappus, K.; Hall, N. Strategies for Improving Patient Throughput in an Acute Care Setting Resulting in Improved Outcomes: A Systematic Review. Nurs. Econ. 2016, 34, 277–288. [Google Scholar]
- Tlapa, D.; Zepeda-Lugo, C.A.; Tortorella, G.L.; Baez-Lopez, Y.A.; Limon-Romero, J.; Alvarado-Iniesta, A.; Rodriguez-Borbon, M.I. Effects of Lean Healthcare on Patient Flow: A Systematic Review. Value Health 2020, 23, 260–273. [Google Scholar] [CrossRef] [Green Version]
- Heaton, H.A.; Castaneda-Guarderas, A.; Trotter, E.R.; Erwin, P.J.; Bellolio, M.F. Effect of scribes on patient throughput, revenue, and patient and provider satisfaction: A systematic review and meta-analysis. Am. J. Emerg. Med. 2016, 34, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Palter, J.; Westrick, J.; Peksa, G.D. Effect of Medical Scribes on Throughput, Revenue, and Patient and Provider Satisfaction: A Systematic Review and Meta-analysis. Ann. Emerg. Med. 2021, 77, 180–189. [Google Scholar] [CrossRef]
- Gualandi, R.; Masella, C.; Tartaglini, D. Improving hospital patient flow: A systematic review. Bus. Process. Manag. J. 2020, 26, 1541–1575. [Google Scholar] [CrossRef]
- Elder, E.; Johnston, A.; Crilly, J. Review article: Systematic review of three key strategies designed to improve patient flow through the emergency department. Emerg. Med. Australas. 2015, 27, 394–404. [Google Scholar] [CrossRef]
- Sobolev, B.; Sanchez, V.; Vasilakis, C. Systematic Review of the Use of Computer Simulation Modeling of Patient Flow in Surgical Care. J. Med Syst. 2011, 35, 1–16. [Google Scholar] [CrossRef]
- Oredsson, S.; Jonsson, H.; Rognes, J.; Lind, L.; Göransson, K.E.; Ehrenberg, A.; Asplund, K.; Castrén, M.; Farrohknia, N. A systematic review of triage-related interventions to improve patient flow in emergency departments. Scand. J. Trauma Resusc. Emerg. Med. 2011, 19, 43. [Google Scholar] [CrossRef] [Green Version]
- Benabbas, R.; Shah, R.; Zonnoor, B.; Mehta, N.; Sinert, R. Impact of triage liaison provider on emergency department throughput: A systematic review and meta-analysis. Am. J. Emerg. Med. 2020, 38, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Rafferty, A.M.; Boiko, O. The role and contribution of nurses to patient flow management in acute hospitals: A systematic review of mixed methods studies. Int. J. Nurs. Stud. 2020, 110, 103709. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Johns Hopkins Medicine. Johns Hopkins Evidence-Based Practice Model. Available online: https://www.hopkinsmedicine.org/evidence-based-practice/ijhn_2017_ebp.html (accessed on 26 September 2021).
- Akuamoa-Boateng, D.; Wegen, S.; Ferdinandus, J.; Marksteder, R.; Baues, C.; Marnitz, S. Managing patient flows in radiation oncology during the COVID-19 pandemic: Reworking existing treatment designs to prevent infections at a German hot spot area University Hospital. Strahlenther. Und Onkol. 2020, 196, 1080–1085. [Google Scholar] [CrossRef]
- Anderson, S.L.; Bianco, J.; DeRemer, C.E. Adapting ambulatory care learning environments in response to the COVID-19 pandemic. Am. J. Health-Syst. Pharm. 2021, 78, 467–471. [Google Scholar] [CrossRef]
- Aquilanti, L.; Gallegati, S.; Temperini, V.; Ferrante, L.; Skrami, E.; Procaccini, M.; Rappelli, G. Italian Response to Coronavirus Pandemic in Dental Care Access: The DeCADE Study. Int. J. Environ. Res. Public Health 2020, 17, 6977. [Google Scholar] [CrossRef]
- Atchley, M.D.; Kroll, N.P.; Etcher, L. Reducing the wait: When time is priceless. Nurse Pract. 2021, 46, 50–55. [Google Scholar] [CrossRef]
- Baughman, A.W.; Hirschberg, R.E.; Lucas, L.J.; Suarez, E.D.; Stockmann, D.; Hutton Johnson, S.; Hutter, M.M.; Murphy, D.J.; Marsh, R.H.; Thompson, R.W.; et al. Pandemic Care Through Collaboration: Lessons From a COVID-19 Field Hospital. J. Am. Med Dir. Assoc. 2020, 21, 1563–1567. [Google Scholar] [CrossRef]
- Beattie, M.; Morrison, C.; MacGilleEathain, R.; Gray, N.; Anderson, J. Near Me at Home: Codesigning the use of video consultations for outpatient appointments in patients’ homes. BMJ Open Qual. 2020, 9, e001035. [Google Scholar] [CrossRef]
- Casiraghi, A.; Domenicucci, M.; Cattaneo, S.; Maggini, E.; Albertini, F.; Avanzini, S.; Pansi Marini, M.; Galante, C.; Guizzi, P.; Milano, G. Operational strategies of a trauma hub in early coronavirus disease 2019 pandemic. Int. Orthop. 2020, 44, 1511–1518. [Google Scholar] [CrossRef]
- Darr, A.; Senior, A.; Argyriou, K.; Limbrick, J.; Nie, H.; Kantczak, A.; Stephenson, K.; Parmar, A.; Grainger, J. The impact of the coronavirus (COVID-19) pandemic on elective paediatric otolaryngology outpatient services—An analysis of virtual outpatient clinics in a tertiary referral centre using the modified paediatric otolaryngology telemedicine satisfaction survey (POTSS). Int. J. Pediatric Otorhinolaryngol. 2020, 138, 110383. [Google Scholar]
- Das, A. Impact of the COVID-19 pandemic on the workflow of an ambulatory endoscopy center: An assessment by discrete event simulation. Gastrointest. Endosc. 2020, 92, 914–924. [Google Scholar] [CrossRef]
- De Biase, G.; Freeman, W.D.; Bydon, M.; Smith, N.; Jerreld, D.; Pascual, J.; Casler, J.; Hasse, C.; Quiñones-Hinojosa, A.; Abode-Iyamah, K. Telemedicine Utilization in Neurosurgery During the COVID-19 Pandemic: A Glimpse Into the Future? Mayo Clinic Proceedings. Innov. Qual. Outcomes 2020, 4, 736–744. [Google Scholar] [CrossRef]
- Dos Santos, C.P.R.S.; Fernandes, A.F.C.; Silva, D.M.D.; Castro, R.C.M.B. Restructuring service at a mastology outpatient clinic during the COVID-19 pandemic. Rev. Bras. Enferm. 2021, 74 (Suppl. 1), 1–4. [Google Scholar]
- Fu, R.; Wu, L.; Zhang, C.; Chu, Q.; Hu, J.; Lin, G.; Yang, L.; Li, J.-S.; Yang, X.-N.; Yang, J.-J.; et al. Real-World Scenario of Patients With Lung Cancer Amid the Coronavirus Disease 2019 Pandemic in the People’s Republic of China. JTO Clin. Res. Rep. 2020, 1, 100053. [Google Scholar] [CrossRef]
- George, J.M.; Xu, Y.; Nursa’adah, B.J.; Lim, S.F.; Low, L.L.; Chan, D.X.H. Collaboration between a tertiary pain centre and community teams during the pandemic. Br. J. Community Nurs. 2020, 25, 480–488. [Google Scholar] [CrossRef]
- Gharaibeh, M.A.; Al Mohammad, B.; Gharaibeh, B.; Khasawneh, L.; Al-Naser, S. Guidelines for the orthopedic surgeon in the era of COVID-19. Orthop. Rev. 2020, 12, 191–195. [Google Scholar]
- Hockaday, S.; Krause, K.; Sobieski, C.; Li, J.N.; Hurst, R.; Ryan, B.; Leader, M.; Smith, D.; Fowler, R.; Tran, A.; et al. Protocols for Personal Protective Equipment in a COVID-19 Medical Shelter. Disaster Med. Public Health Prep. 2020, 14, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Jänig, C.; Forklage, R.; Gurney, J.M.; Groth, R.; Wirth, C.; van de Krol, H.; Schmidbauer, W.; Güsgen, C. Triage Decisions in the Context of COVID-19: Old Burden, New Challenge-The Structured Approach for Intensive Care Unit Triage (SAINT) Protocol. Mil. Med. 2021, 186, e300–e304. [Google Scholar] [CrossRef] [PubMed]
- Küçük, A.; Demirci, M.; Kerman, G.; Soner Özsoy, V. Evaluating of hospital appointment systems in Turkey: Challenges and opportunities. Health Policy Technol. 2021, 10, 69–74. [Google Scholar] [CrossRef]
- Kyari, F.; Watts, E. How to adapt your eye service in the time of COVID-19. Community Eye Health J. 2020, 33, 14. [Google Scholar]
- Lou, T.; Ren, Z.; Sun, Z.; Wang, W.; Fan, C. Full recovery of elective orthopedic surgery in the age of COVID-19: An 8-month retrospective cohort study. J. Orthop. Surg. Res. 2021, 16, 154. [Google Scholar] [CrossRef]
- Lynch, M.E.; Williamson, O.D.; Banfield, J.C. COVID-19 impact and response by Canadian pain clinics: A national survey of adult pain clinics. Can. J. Pain 2020, 4, 204–209. [Google Scholar] [CrossRef]
- Mason, T.; Bennett, R.; White, A.; Rembielak, A. Changing radiotherapy review practice in response to COVID-19 in a radiotherapy satellite centre. J. Radiother. Pract. 2020, 19, 312–314. [Google Scholar] [CrossRef]
- Mukerji, S.S.; Liu, Y.-C.; Musso, M.F. Pediatric otolaryngology workflow changes in a community hospital setting to decrease exposure to novel coronavirus. Int. J. Pediatric Otorhinolaryngol. 2020, 136, 110169. [Google Scholar] [CrossRef]
- Raidla, A.; Darro, K.; Carlson, T.; Khorram-Manesh, A.; Berlin, J.; Carlström, E. Outcomes of Establishing an Urgent Care Centre in the Same Location as an Emergency Department. Sustainability 2020, 12, 8190. [Google Scholar] [CrossRef]
- Rodler, S.; Apfelbeck, M.; Stief, C.; Heinemann, V.; Casuscelli, J. Lessons from the coronavirus disease 2019 pandemic: Will virtual patient management reshape uro-oncology in Germany? Eur. J. Cancer 2020, 132, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Sacchelli, L.; Evangelista, V.; Di Altobrando, A.; Lacava, R.; Rucci, P.; Rosa, S.; Patrizi, A.; Bardazzi, F. How infodemic during the COVID-19 outbreak influenced common clinical practice in an Outpatient Service of Severe Psoriasis. Dermatol. Ther. 2020, 33, e14065. [Google Scholar] [CrossRef]
- Segal, E.M.; Alwan, L.; Pitney, C.; Taketa, C.; Indorf, A.; Held, L.; Lee, K.S.; Son, M.; Chi, M.; Diamantides, E.; et al. Establishing clinical pharmacist telehealth services during the COVID-19 pandemic. Am. J. Health-Syst. Pharm. 2020, 77, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- Tam, D.Y.; Naimark, D.; Natarajan, M.K.; Woodward, G.; Oakes, G.; Rahal, M.; Barrett, K.; Khan, Y.A.; Ximenes, R.; Mac, S.; et al. The Use of Decision Modelling to Inform Timely Policy Decisions on Cardiac Resource Capacity During the COVID-19 Pandemic. Can. J. Cardiol. 2020, 36, 1308–1312. [Google Scholar] [CrossRef]
- Thorakkattil, S.A.; Nemr, H.S.; Al-Ghamdi, F.H.; Jabbour, R.J.; Al-Qaaneh, A.M. Structural and operational redesigning of patient-centered ambulatory care pharmacy services and its effectiveness during the COVID-19 pandemic. Res. Soc. Adm. Pharm. 2021, 17, 1838–1844. [Google Scholar] [CrossRef]
- Wang, J.; Zong, L.; Zhang, J.; Sun, H.; Harold Walline, J.; Sun, P.; Xu, S.; Li, Y.; Wang, C.; Liu, J.; et al. Identifying the effects of an upgraded “fever clinic” on COVID-19 control and the workload of emergency department: Retrospective study in a tertiary hospital in China. BMJ Open 2020, 10, e039177. [Google Scholar] [CrossRef]
- Waya, J.L.L.; Ameh, D.; Mogga, J.L.K.; Wamala, J.F.; Olu, O.O. COVID-19 case management strategies: What are the options for Africa? Infect. Dis. Poverty 2021, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Lieneck, C.; Weaver, E.; Maryon, T. Pandemic Pause: Systematic Review of Cost Variables for Ambulatory Care Organizations Participating in Accountable Care Organizations. Healthcare 2021, 9, 198. [Google Scholar] [CrossRef] [PubMed]
- Lieneck, C.; Weaver, E.; Maryon, T. Outpatient Telehealth Implementation in the United States during the COVID-19 Global Pan-demic: A Systematic Review. Medicina 2021, 57, 462. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Search Variable | Development Method | Database Usage |
|---|---|---|
| Ambulatory Care | MeSH (exploded) | Subject Terms (SU) |
| Patient Throughput | Google search | All Text (TX) |
| COVID-19 | EBSCO research database popular terms list | Subject Terms (SU) |
| Article Assignment | Reviewer 1 | Reviewer 2 | Reviewer 3 | Reviewer 4 | Reviewer 5 | Reviewer 6 | Reviewer 7 |
|---|---|---|---|---|---|---|---|
| Articles 1–10 | X | X | X | X | X | X | |
| Articles 11–20 | X | X | X | X | X | X | |
| Articles 21–30 | X | X | X | X | X | ||
| Articles 31–40 | X | X | X | X | |||
| Articles 41–50 | X | X | X | X |
| Author(s) | Participant(s) | JHNEBP Study Design * | Facilitators Leading to an Increase in Patient Throughput in Ambulatory Care Organizations during COVID-19 | Barriers Leading to a Decrease in Patient Throughput in Ambulatory Care Organizations during COVID-19 |
|---|---|---|---|---|
| Akuamoa-Boateng et al. [14] | German University Hospital radiation oncology clinic | 3 |
|
|
| Anderson et al. [15] | Ambulatory care pharmacy preceptors in the U.S. | 3 |
|
|
| Aquilanti et al. [16] | Dental patients in Italy | 3 |
|
|
| Atchley et al. [17] | U.S. nurse practitioner outpatient clinics | 3 |
|
|
| Baughman et al. [18] | Boston post-acute care facilities and surrounding healthcare organizations | 3 |
|
|
| Beattie et al. [19] | Inner Hebrides of Scotland outpatient clinics | 3 |
|
|
| Casiraghi et al. [20] | Spedali Civili Italian hospital trauma department patients | 3 |
|
|
| Darr et al. [21] | NHS tertiary pediatric referral center | 2 |
|
|
| Das [22] | Community-based ambulatory endoscopy center in the U.S. | 3 |
|
|
| De Biase et al. [23] | Tertiary institution neurology clinic (U.S) | 2 |
|
|
| dos Santos et al. [24] | Public university service mastology outpatient clinic in Ceará | 3 |
|
|
| Fu et al. [25] | Lung Cancer patients at a health system clinic in the People’s Republic of China | 2 |
|
|
| George et al. [26] | Singapore community health pain management clinics | 3 |
|
|
| Gharaibeh et al. [27] | International orthopedic clinics | 3 |
|
|
| Hockaday et al. [28] | Federal Medical Station for COVID patients in Dallas, TX, USA | 3 |
|
|
| Janig et al. [29] | Military medical treatment facilities | 3 |
|
|
| Küçük et al. [30] | Health Ministry of Turkey EHR/EMR data from multiple healthcare organizations | 2 |
|
|
| Kyari & Watts [31] | U.S. outpatient eye clinics | 3 |
|
|
| Lou et al. [32] | Orthopedic surgery institution in Shanghai, China | 3 |
|
|
| Lynch et al. [33] | Representatives from adult pain clinics in Canada | 2 |
|
|
| Mason et al. [34] | Radiotherapy patients at the The Christie at Oldham satellite center in the UK | 3 |
|
|
| Mukerji et al. [35] | Otolaryngology clinic at a U.S. community pediatric hospital | 3 |
|
|
| Raidla et al. [36] | Hospital system in Sweden | 2 |
|
|
| Rodler et al. [37] | Patients currently being treated for genitourinary cancers at a single German hospital | 2 |
|
|
| Sacchelli et al. [38] | Psoriasis patients in ambulatory care clinics in Italy | 2 |
|
|
| Segal et al. [39] | Washington state pharmacy service for multiple ambulatory care clinics | 3 |
|
|
| Tam et al. [40] | Cardiac health system in Ontario that has outpatient clinics | 3 |
|
|
| Thorakkattil et al. [41] | Johns Hopkins Aramco Health Care (JHAH) ambulatory care pharmacy services in Saudi Arabia | 2 |
|
|
| Wang et al. [42] | Outpatient fever clinics located at the Union Medical College Hospital (China) | 3 |
|
|
| Waya et al. [43] | African healthcare organizations | 3 |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieneck, C.; Ramamonjiarivelo, Z.; Cox, J.; Dominguez, J.; Gersbach, K.; Heredia, E.; Khan, A. Patient Throughput Initiatives in Ambulatory Care Organizations during the COVID-19 Pandemic: A Systematic Review. Healthcare 2021, 9, 1474. https://doi.org/10.3390/healthcare9111474
Lieneck C, Ramamonjiarivelo Z, Cox J, Dominguez J, Gersbach K, Heredia E, Khan A. Patient Throughput Initiatives in Ambulatory Care Organizations during the COVID-19 Pandemic: A Systematic Review. Healthcare. 2021; 9(11):1474. https://doi.org/10.3390/healthcare9111474
Chicago/Turabian StyleLieneck, Cristian, Zo Ramamonjiarivelo, Jennifer Cox, Jack Dominguez, Kendal Gersbach, Edward Heredia, and Afroza Khan. 2021. "Patient Throughput Initiatives in Ambulatory Care Organizations during the COVID-19 Pandemic: A Systematic Review" Healthcare 9, no. 11: 1474. https://doi.org/10.3390/healthcare9111474
APA StyleLieneck, C., Ramamonjiarivelo, Z., Cox, J., Dominguez, J., Gersbach, K., Heredia, E., & Khan, A. (2021). Patient Throughput Initiatives in Ambulatory Care Organizations during the COVID-19 Pandemic: A Systematic Review. Healthcare, 9(11), 1474. https://doi.org/10.3390/healthcare9111474