
Work Stress, Mental Health and Validation of Professional Stress Scale (PSS) in an Italian-Speaking Teachers Sample


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Sample
2.3. Data Collection Instrument
2.4. Ethics
2.5. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Reliability Analysis
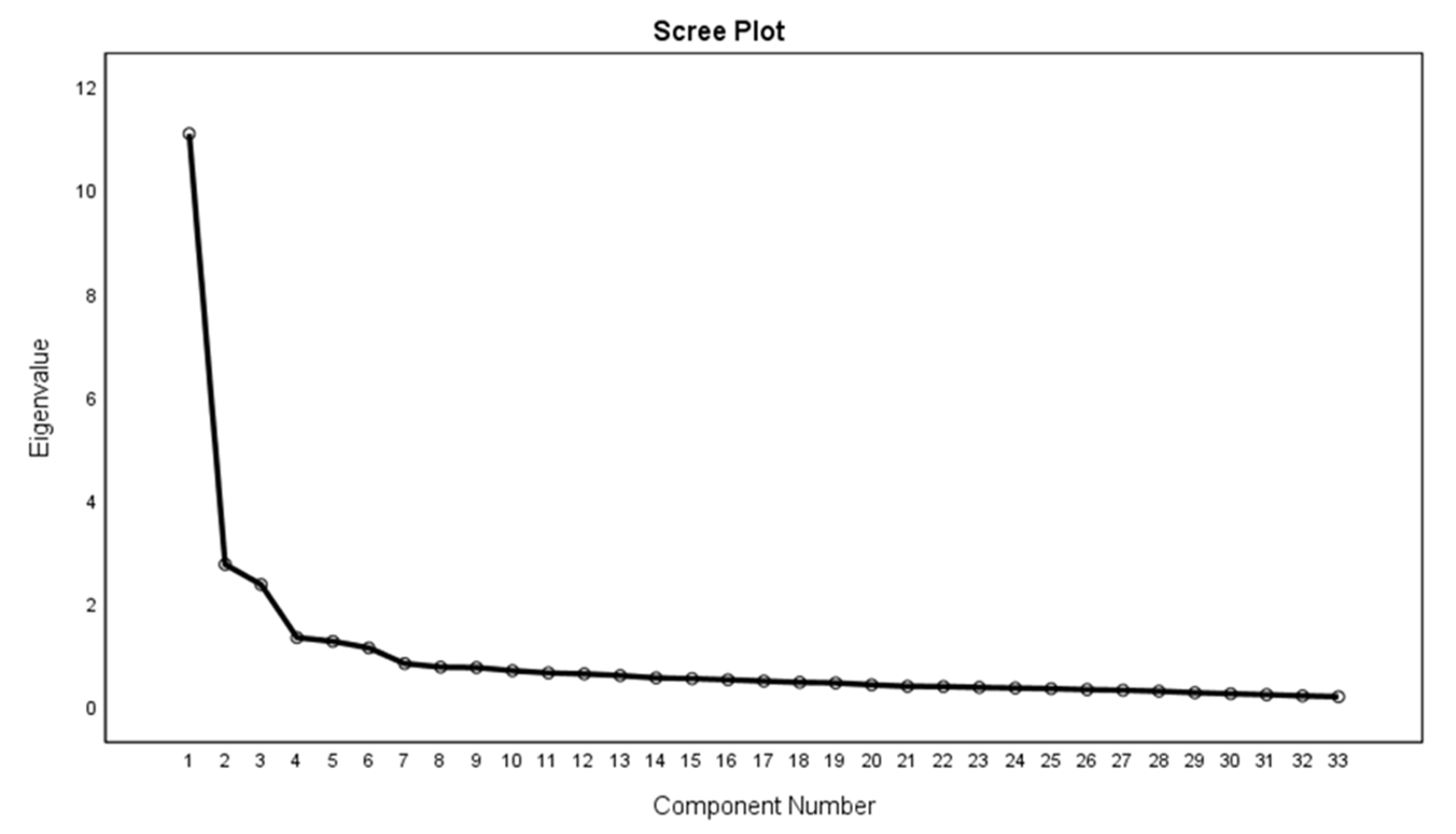
3.3. Factor Analysis
Extraction Method: Principal Component Analysis
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ganster, D.; Schaubroeck, J. Work Stress and Employee Health. J. Manag. 1991, 17, 235–271. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Xu, J.; You, H.; Li, Y.; Liang, Y.; Li, S.; Ma, L.; Lau, J.T.-F.; Hao, Y.; et al. Prevalence of mental health problems and associated factors among front-line public health workers during the COVID-19 pandemic in China: An effort–reward imbalance model-informed study. BMC Psychol. 2021, 9, 1. [Google Scholar] [CrossRef]
- American Heart Association. Mental Health: A Workforce Crisis; American Heart Association: Chicago, IL, USA, 2019. [Google Scholar]
- Goh, J.; Pfeffer, J.; Zenios, S.A. The Relationship between Workplace Stressors and Mortality and Health Costs in the United States. Manag. Sci. 2016, 62, 608–628. [Google Scholar] [CrossRef] [Green Version]
- Lait, J.; Wallace, J.E. Stress at Work: A Study of Organizational-Professional Conflict and Unmet Expectations. Articles 2002, 57, 463–490. [Google Scholar] [CrossRef] [Green Version]
- Limone, P.; Toto, G.A. Psychological and Emotional Effects of Digital Technology on Children in COVID-19 Pandemic. Brain Sci. 2021, 11, 1126. [Google Scholar] [CrossRef]
- Mihăilă, T. Perceived stress scale as a predictor of professional behavior and aspects of wellbeing. Rom J. Cogn. Behav. Ther. Hypn. 2015, 2, 1–14. [Google Scholar]
- Schmitt, J.B.; Breuer, J.; Wulf, T. From cognitive overload to digital detox: Psychological implications of telework during the COVID-19 pandemic. Comput. Hum. Behav. 2021, 124, 106899. [Google Scholar] [CrossRef] [PubMed]
- Sadovyy, M.; Sánchez-Gómez, M.; Bresó, E. COVID-19: How the stress generated by the pandemic may affect work performance through the moderating role of emotional intelligence. Pers. Individ. Differ. 2021, 180, 110986. [Google Scholar] [CrossRef]
- Dreher, A.; Flake, F.; Pietrowsky, R.; Loerbroks, A. Attitudes and stressors related to the SARS-CoV-2 pandemic among emergency medical services workers in Germany: A cross-sectional study. BMC Health Serv. Res. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Voltmer, E.; Köslich-Strumann, S.; Voltmer, J.B.; Kötter, T. Stress and behavior patterns throughout medical education–a six year longitudinal study. BMC Med. Educ. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Kern, M.; Zapf, D. Ready for change? A longitudinal examination of challenge stressors in the context of organizational change. J. Occup. Health Psychol. 2021, 26, 204–223. [Google Scholar] [CrossRef] [PubMed]
- Useche, S.A.; Alonso, F.; Cendales, B.; Montoro, L.; Llamazares, J. Measuring job stress in transportation workers: Psychometric properties, convergent validity and reliability of the ERI and JCQ among professional drivers. BMC Public Health 2021, 21, 1–19. [Google Scholar] [CrossRef]
- Russell, A.T.; Pasnau, R.O.; Taintor, Z.C. Emotional problems of residents in psychiatry. Am. J. Psychiatry 1975, 132, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Cushway, D. Stress in clinical psychology trainees. Br. J. Clin. Psychol. 1992, 31, 169–179. [Google Scholar] [CrossRef]
- Travers, C.; Firth-Cozens, J. Experiences of mental health work, hospital closure, stress and social support. In Proceedings of the British Psychological Society, Annual Occupational Psychology Conference, Bowness-on-Windermere, UK, 21 December 1989. [Google Scholar]
- Sutherland, V.J.; Cooper, C.L. Understanding Stress: A Psychological Perspective for Health Professionals; Chapman & Hall/CRC: Boca Raton, FL, USA, 1990. [Google Scholar]
- Kern, M.; Heissler, C.; Zapf, D. Social Job Stressors can Foster Employee Well-Being: Introducing the Concept of Social Challenge Stressors. J. Bus. Psychol. 2020, 36, 771–792. [Google Scholar] [CrossRef]
- Hellman, I.D.; Morrison, T.L.; Abramowitz, S.I. Therapist flexibility/rigidity and work stress. Prof. Psychol. Res. Pract. 1987, 18, 21. [Google Scholar] [CrossRef]
- Cushway, D.; Tyler, P. Stress in clinical psychologists. Int. J. Soc. Psychiatry 1996, 42, 141–149. [Google Scholar] [CrossRef]
- Irawanto, D.W.; Novianti, K.R.; Roz, K. Work from Home: Measuring Satisfaction between Work–Life Balance and Work Stress during the COVID-19 Pandemic in Indonesia. Economies 2021, 9, 96. [Google Scholar] [CrossRef]
- Oksanen, A.; Oksa, R.; Savela, N.; Mantere, E.; Savolainen, I.; Kaakinen, M. COVID-19 Crisis and Digital Stressors at Work: A Longitudinal Study on the Finnish Working Population. Comput. Hum. Behav. 2021, 122, 106853. [Google Scholar] [CrossRef]
- Sancho-Gil, J.M.; Rivera-Vargas, P.; Miño-Puigcercós, R. Moving beyond the predictable failure of Ed-Tech initiatives. Learn. Media Technol. 2019, 45, 61–75. [Google Scholar] [CrossRef]
- Hong, X.; Liu, Q.; Zhang, M. Dual Stressors and Female Pre-school Teachers’ Job Satisfaction during the COVID-19: The Mediation of Work-Family Conflict. Front. Psychol. 2021, 12, 691498. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Zhuo, Y.; Qi, X.; Wu, H.; Liu, Y.; Li, J.; Jin, C. The Role of Personal Biological Resource in the Job Demands-Control-Support Model: Evidence from Stress Reactivity. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Elfering, A.; Kottwitz, M.U.; Semmer, N.K. Battery Discharge from Monday to Friday: Background Social Stress at Work is Associated with more Rapid Accumulation of Fatigue. Sleep Vigil. 2021, 5, 49–60. [Google Scholar] [CrossRef]
- Wang, J.; Song, B.; Shao, Y.; Zhu, J. Effect of Online Psychological Intervention on Burnout in Medical Residents from Different Majors: An Exploratory Study. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Liu, T.; Wilczyńska, D.; Lipowski, M.; Zhao, Z. Optimization of a Sports Activity Development Model Using Artificial Intelligence under New Curriculum Reform. Int. J. Environ. Res. Public Health 2021, 18, 9049. [Google Scholar] [CrossRef]
- Chen, S.; Grupe, D.W. Trait Mindfulness Moderates the Association Between Stressor Exposure and Perceived Stress in Law Enforcement Officers. Mindfulness 2021, 12, 2325–2338. [Google Scholar] [CrossRef]
- Wemken, G.; Janurek, J.; Junker, N.M.; Häusser, J.A. The impact of social comparisons of job demands and job control on well-being. Appl. Psychol. Health Well-Being 2021, 13, 419–436. [Google Scholar] [CrossRef]
- Reis, D.; Hart, A.; Lehr, D.; Friese, M. Promoting recovery in daily life: Study protocol for a randomized controlled trial. BMC Psychol. 2021, 9, 1–15. [Google Scholar] [CrossRef]
- Mucci, N.; Giorgi, G.; Cupelli, V.; Gioffrè, P.A.; Rosati, M.V.; Tomei, F.; Tomei, G.; Breso-Esteve, E.; Arcangeli, G. Work-related stress assessment in a population of Italian workers. The Stress Questionnaire. Sci. Total Environ. 2015, 502, 673–679. [Google Scholar] [CrossRef]
- Zefferino, R.; Facciorusso, A.; Lasalvia, M.; Narciso, M.; Nuzzaco, A.; Lucchini, R.; Abbate, N.L. Salivary markers of work stress in an emergency team of urban police (1^ o step). G. Ital. Di Med. Del Lav. Ed Ergon. 2006, 28, 472. [Google Scholar]
- Zefferino, R. Obiettivare lo stress: Uno sguardo al passato, valutando il presente… una scommessa per il futuro. G Ital. Med. Lav. Erg. 2009, 31, 281–286. [Google Scholar]
- Hair, J.F.; Celsi, M.; Ortinau, D.J.; Bush, R.P. Essentials of Marketing Research; McGraw-Hill/Irwin: New York, NY, USA, 2010; Volume 2. [Google Scholar]
- Dias, R.D.; Neto, A.S. Stress levels during emergency care: A comparison between reality and simulated scenarios. J. Crit. Care 2016, 33, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Giessing, L.; Frenkel, M.O.; Zinner, C.; Rummel, J.; Nieuwenhuys, A.; Kasperk, C.; Brune, M.; Engel, F.A.; Plessner, H. Effects of Coping-Related Traits and Psychophysiological Stress Responses on Police Recruits’ Shooting Behavior in Reality-Based Scenarios. Front. Psychol. 2019, 10, 1523. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, E.; De Souza, F.T.A.; Ferreira, E.; Souza, R.P.; Macedo, S.C.; Friedman, E.; Gomez, M.V.; Gomes, C.; Gomez, R.S. Cell phone use is associated with an inflammatory cytokine profile of parotid gland saliva. J. Oral Pathol. Med. 2016, 45, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.; Burnard, P. A systematic review of stress and stress management interventions for mental health nurses. J. Adv. Nurs. 2003, 42, 169–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.S.; Ryu, V.; Lee, J.H.; Hong, H.; Han, H.; Park, S. Psychometric Properties of the Korean Version of the Mental Health Professionals Stress Scale. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef]
- Lo, H.H.M.; Ngai, S.; Yam, K. Effects of Mindfulness-Based Stress Reduction on Health and Social Care Education: A Cohort-Controlled Study. Mindfulness 2021, 12, 2050–2058. [Google Scholar] [CrossRef]
- Klinefelter, Z.; Sinclair, R.R.; Britt, T.W.; Sawhney, G.; Black, K.J.; Munc, A. Psychosocial Safety Climate and Stigma: Reporting Stress-related Concerns at Work. Stress Health 2020, 37, 488–503. [Google Scholar] [CrossRef]

{kind=link}
| Cronbach’s Alpha | Cronbach’s Alpha Based on Standardized Items | No of Items |
|---|---|---|
| 0.936 | 0.936 | 33 |
| Item | N | Mean | Std. Deviation | Scale Mean If Item Deleted | Scale Variance If Item Deleted | Corrected Item Total Correlation | Cronbach’s Alpha if Item Deleted | Loadings |
|---|---|---|---|---|---|---|---|---|
| 1 | 1106 | 2.30 | 0.794 | 45.44 | 287.383 | 0.403 | 0.935 | 0.578 |
| 2 | 1106 | 2.19 | 0.873 | 45.56 | 284.850 | 0.450 | 0.935 | 0.615 |
| 3 | 1106 | 1.90 | 0.901 | 45.85 | 283.228 | 0.489 | 0.935 | 0.538 |
| 4 | 1106 | 1.89 | 0.940 | 45.86 | 283.835 | 0.447 | 0.935 | 0.680 |
| 5 | 1106 | 1.75 | 0.942 | 45.99 | 281.950 | 0.507 | 0.935 | 0.551 |
| 6 | 1106 | 1.38 | 0.868 | 46.36 | 282.821 | 0.524 | 0.934 | 0.433 |
| 7 | 1106 | 1.54 | 0.916 | 46.20 | 278.040 | 0.655 | 0.933 | 0.595 |
| 8 | 1106 | 1.29 | 0.981 | 46.45 | 278.168 | 0.603 | 0.934 | 0.626 |
| 9 | 1106 | 1.42 | 0.900 | 46.32 | 277.754 | 0.677 | 0.933 | 0.699 |
| 10 | 1106 | 1.37 | 0.907 | 46.37 | 277.327 | 0.686 | 0.933 | 0.741 |
| 11 | 1106 | 1.42 | 0.935 | 46.32 | 276.562 | 0.689 | 0.933 | 0.716 |
| 12 | 1106 | 1.36 | 0.918 | 46.39 | 276.822 | 0.694 | 0.933 | 0.737 |
| 13 | 1106 | 1.35 | 0.948 | 46.39 | 277.218 | 0.658 | 0.933 | 0.664 |
| 14 | 1106 | 1.62 | 0.990 | 46.12 | 279.618 | 0.552 | 0.934 | 0.601 |
| 15 | 1106 | 1.79 | 0.956 | 45.96 | 279.093 | 0.590 | 0.934 | 0.734 |
| 16 | 1106 | 1.32 | 0.980 | 46.43 | 280.245 | 0.538 | 0.934 | 0.680 |
| 17 | 1106 | 1.43 | 0.939 | 46.31 | 278.564 | 0.620 | 0.933 | 0.660 |
| 18 | 1106 | 0.97 | 0.883 | 46.77 | 280.074 | 0.610 | 0.934 | 0.604 |
| 19 | 1106 | 1.01 | 0.949 | 46.74 | 279.644 | 0.577 | 0.934 | 0.596 |
| 20 | 1106 | 0.46 | 0.755 | 47.29 | 287.191 | 0.434 | 0.935 | 0.583 |
| 21 | 1106 | 1.19 | 0.926 | 46.55 | 280.800 | 0.555 | 0.934 | 0.531 |
| 22 | 1106 | 1.42 | 0.905 | 46.33 | 281.707 | 0.538 | 0.934 | 0.519 |
| 23 | 1106 | 0.99 | 0.833 | 0.558 | ||||
| 24 | 1106 | 1.25 | 0.927 | 0.756 |
| Test | |||||||
|---|---|---|---|---|---|---|---|
| Eigen Value | 11.1 | 2.8 | 2.4 | 1.4 | 1.3 | 1.2 | |
| Percentage of Variance | 33.7 | 8.4 | 7.2 | 4.1 | 3.9 | 3.5 | |
| Total Variance Explained | 60.8 | ||||||
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy | 0.943 | ||||||
| Approx. Chi-Square (BTS) | 18,361.702 | ||||||
| Df | 528 | ||||||
| Sig. | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limone, P.; Zefferino, R.; Toto, G.A.; Tomei, G. Work Stress, Mental Health and Validation of Professional Stress Scale (PSS) in an Italian-Speaking Teachers Sample. Healthcare 2021, 9, 1434. https://doi.org/10.3390/healthcare9111434
Limone P, Zefferino R, Toto GA, Tomei G. Work Stress, Mental Health and Validation of Professional Stress Scale (PSS) in an Italian-Speaking Teachers Sample. Healthcare. 2021; 9(11):1434. https://doi.org/10.3390/healthcare9111434
Chicago/Turabian StyleLimone, Pierpaolo, Roberto Zefferino, Giusi Antonia Toto, and Gianfranco Tomei. 2021. "Work Stress, Mental Health and Validation of Professional Stress Scale (PSS) in an Italian-Speaking Teachers Sample" Healthcare 9, no. 11: 1434. https://doi.org/10.3390/healthcare9111434
APA StyleLimone, P., Zefferino, R., Toto, G. A., & Tomei, G. (2021). Work Stress, Mental Health and Validation of Professional Stress Scale (PSS) in an Italian-Speaking Teachers Sample. Healthcare, 9(11), 1434. https://doi.org/10.3390/healthcare9111434