
Arguments for Using Direct Oral Anticoagulants in Cancer-Related Venous Thromboembolism

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
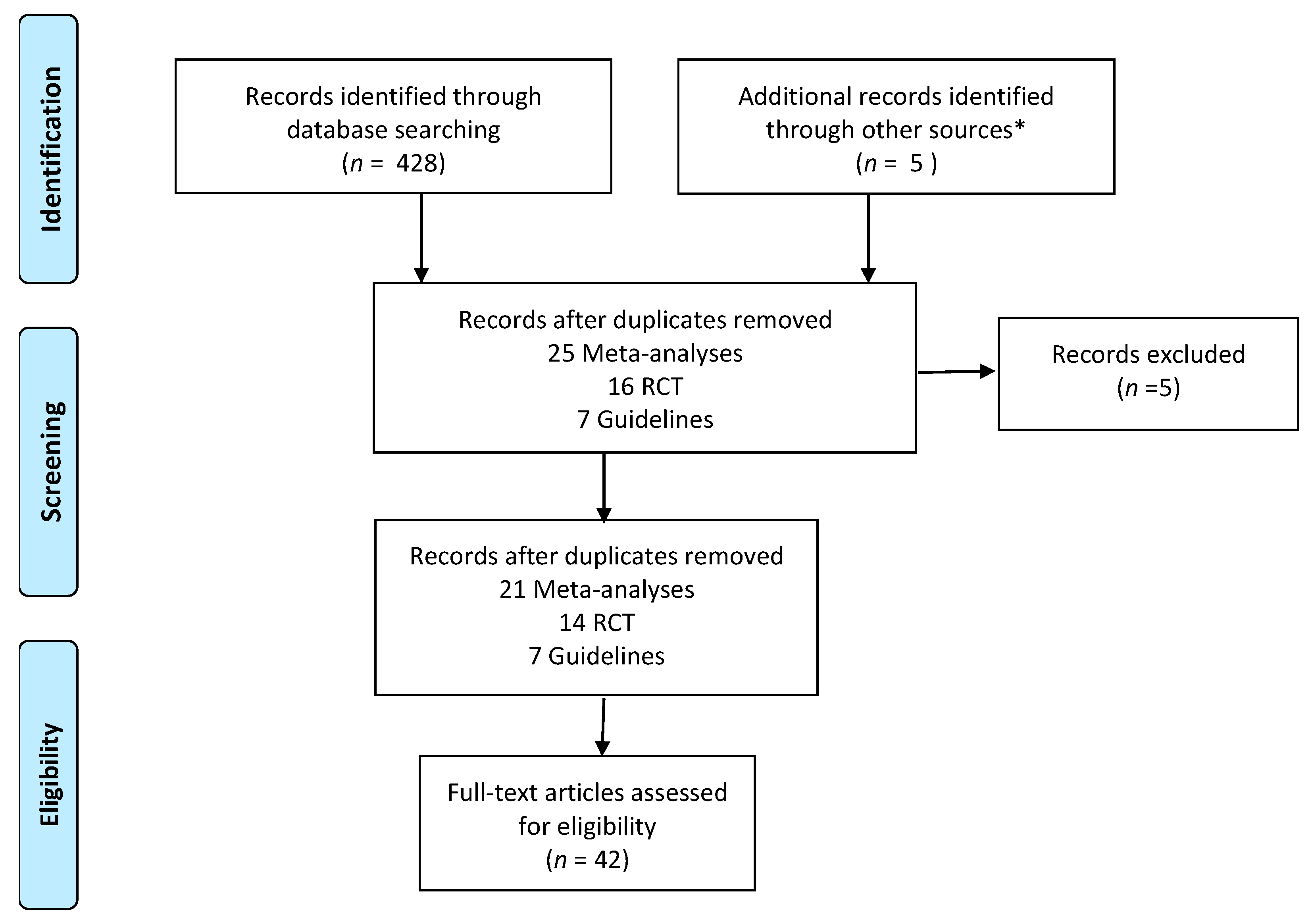
2.1. Search Strategy
2.2. Information Sources
2.3. Eligibility Criteria
3. Results
3.1. Meta-Analyses
3.2. Randomized Controlled Studies
3.3. Guidelines Published in the Past 6 Years
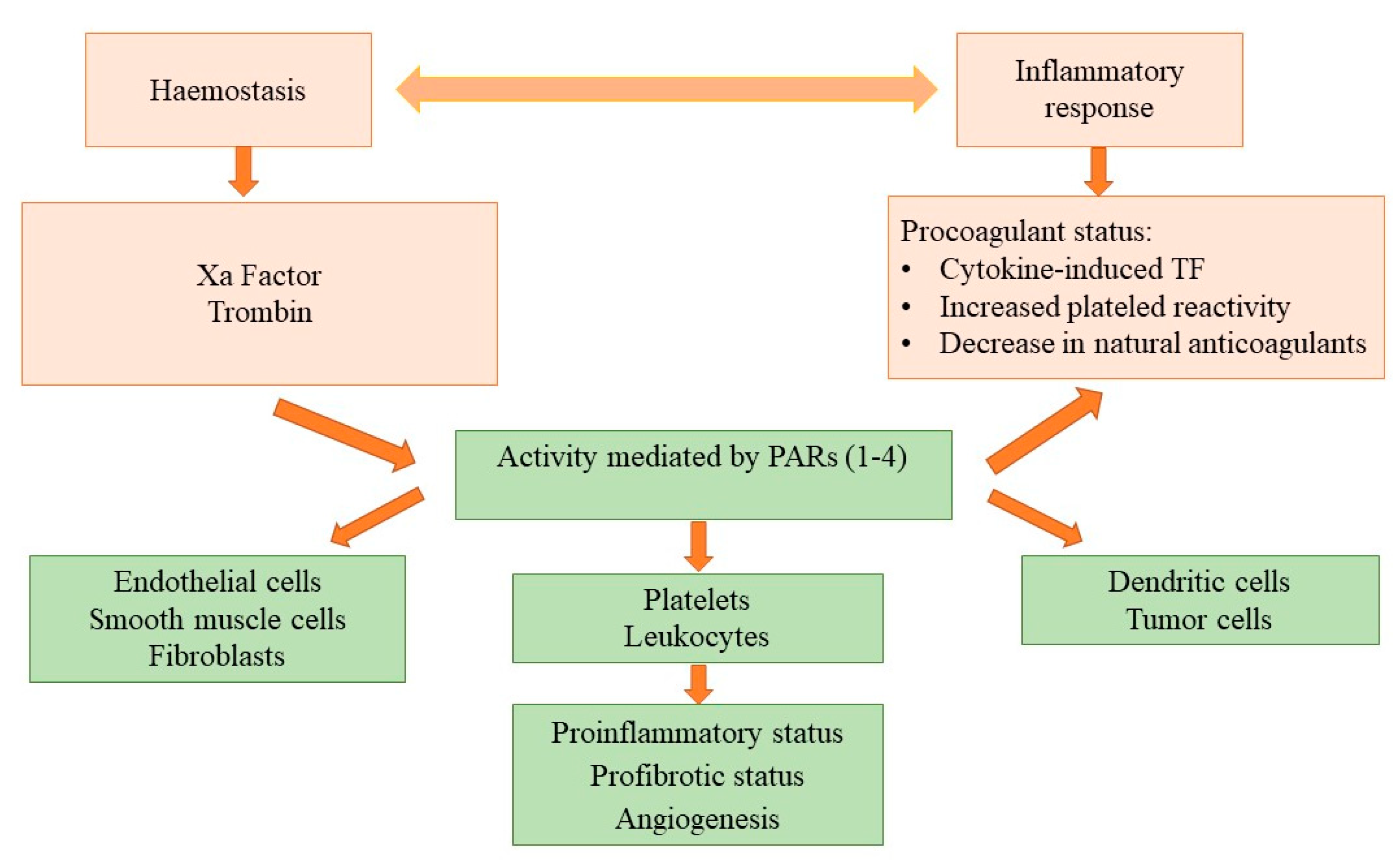
3.4. DOACs beyond Anticoagulation: A Potential Antineoplastic Effect
4. Discussion
4.1. Meta-Analysis
4.2. Randomized Controlled Trials
4.3. Guidelines
4.4. DOACs beyond Anticoagulation: A Potential Antineoplastic Effect?
4.5. Some Practical Considerations on the Use of DOACs in Cancer Patients
4.5.1. The Length of the Treatment
4.5.2. High Risk of Major Bleeding
4.5.3. Renal Impairment
4.5.4. Liver and Gastrointestinal Diseases
4.5.5. Interaction with Other Drugs
4.5.6. Extreme Weight
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borovac, J.A.; D’Amario, D.; Bozic, J.; Glavas, D. Sympathetic Nervous System Activation and Heart Failure: Current State of Evidence and the Pathophysiology in the Light of Novel Biomarkers. World J. Cardiol. 2020, 12, 373–408. [Google Scholar] [CrossRef] [PubMed]
- Timp, J.; Braekkan, S.; Versteeg, H.; Cannegieter, S. Epidemiology of cancer-associated venous thrombosis. Blood J. Am. Soc. Hematol. 2013, 122, 1712–1723. [Google Scholar] [CrossRef] [PubMed]
- Mosarla, R.C.; Vaduganathan, M.; Qamar, A.; Moslehi, J.; Piazza, G.; Giugliano, R.P. Anticoagulation Strategies in Patients With Cancer: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 1336–1349. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Schaefer, J.K.; Li, M.; Wu, Z.; Basu, T.; Dorsch, M.P.; Barnes, G.D.; Carrier, M.; Griggs, J.J.; Sood, S.L. Anticoagulant medication adherence for cancer-associated thrombosis: A comparison of LMWH to DOACs. J. Thromb. Haemost. 2021, 19, 212–220. [Google Scholar] [CrossRef]
- Liberati, A.; Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P (Preferred Reporting Items for Systematic review and Meta-Analysis Protocols) 2015 checklist: Recommended items to address in a systematic review protocol. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef]
- Sardar, P.; Chatterjee, S.; Herzog, E.; Pekler, G.; Mushiyev, S.; Pastori, L.J.; Visco, F.; Aronow, W.S. New oral anticoagulants in patients with cancer: Current state of evidence. Am. J. Ther. 2015, 22, 460–468. [Google Scholar] [CrossRef]
- Posch, F.; Königsbrügge, O.; Zielinski, C.; Pabinger, I.; Ay, C. Treatment of venous thromboembolism in patients with cancer: A network meta-analysis comparing efficacy and safety of anticoagulants. Thromb. Res. 2015, 136, 582–589. [Google Scholar] [CrossRef]
- Mantha, S.; Ansell, J. Indirect comparison of dabigatran, rivaroxaban, apixaban and edoxaban for the treatment of acute venous thromboembolism. J. Thromb. Thrombolysis 2015, 39, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Boonyawat, K.; Caron, F.; Li, A.; Chai-Adisaksopha, C.; Lim, W.; Iorio, A.; Lopes, R.D.; Garcia, D.; Crowther, M.A. Association of body weight with efficacy and safety outcomes in phase III randomized controlled trials of direct oral anticoagulants: A systematic review and meta-analysis. J. Thromb. Haemost. 2017, 15, 1322–1333. [Google Scholar] [CrossRef] [PubMed]
- Kahale, L.A.; Hakoum, M.B.; Tsolakian, I.G.; Matar, C.F.; Barba, M.; Yosuico, V.E.D.; Terrenato, I.; Sperati, F.; Schünemann, H.; Akl, E.A. Oral anticoagulation in people with cancer who have no therapeutic or prophylactic indication for anticoagulation. Cochrane Database Syst. Rev. 2017, 12, CD006466. [Google Scholar] [CrossRef]
- Hakoum, M.B.; Kahale, L.A.; Tsolakian, I.G.; Matar, C.F.; Yosuico, V.E.; Terrenato, I.; Sperati, F.; Barba, M.; Schünemann, H.; Akl, E.A. Anticoagulation for the initial treatment of venous thromboembolism in people with cancer (Review). Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Vedovati, M.C.; Giustozzi, M.; Bonitta, G.; Agnelli, G.; Becattini, C. Efficacy and safety of anticoagulant agents in patients with venous thromboembolism and cancer: A network meta-analysis. Thromb. Res. 2018, 170, 175–180. [Google Scholar] [CrossRef]
- Xing, J.; Yin, X.; Chen, D. Rivaroxaban versus enoxaparin for the prevention of recurrent venous thromboembolism in patients with cancer: A meta-analysis. Medicine 2018, 97, e11384. [Google Scholar] [CrossRef]
- Martinez, B.K.; Sheth, J.; Patel, N.; Baker, W.L.; Coleman, C.I. Systematic Review and Meta-Analysis of Real-World Studies Evaluating Rivaroxaban for Cancer-Associated Venous Thrombosis. Pharmacotherapy 2018, 38, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Kim, J.-C.; Cho, J.; Lim, J.H.; Lee, M.H. Systematic literature review and network meta-analysis of oral anticoagulants for the treatment of venous thromboembolism in patients with cancer. Ann. Oncol. 2018, 29, viii615. [Google Scholar] [CrossRef]
- Hong, Y.; Mansour, S.; Alotaibi, G.; Wu, C.; McMurtry, M.S. Effect of anticoagulants on admission rates and length of hospital stay for acute venous thromboembolism: A systematic review of randomized control trials. Crit. Rev. Oncol. Hematol. 2018, 125, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Outes, A.; Terleira-Fernández, A.I.; Lecumberri, R.; Suárez-Gea, M.L.; Calvo-Rojas, G.; Vargas-Castrillón, E. Causes of Death in Patients with Venous Thromboembolism Anticoagulated with Direct Oral Anticoagulants: A Systematic Review and Meta-Analysis. Semin. Thromb. Hemost. 2018, 44, 377–387. [Google Scholar] [CrossRef]
- Li, A.; Garcia, D.A.; Lyman, G.H.; Carrier, M. Direct oral anticoagulant (DOAC) versus low-molecular-weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): A systematic review and meta-analysis. Thromb. Res. 2018, 173, 158–163. [Google Scholar] [CrossRef]
- Rossel, A.; Robert-Ebadi, H.; Combescure, C.; Grosgurin, O.; Stirnemann, J.; Addeo, A.; Garin, N.; Agoritsas, T.; Reny, J.L.; Marti, C. Anticoagulant therapy for acute venous thrombo-embolism in cancer patients: A systematic review and network meta-analysis. PLoS ONE 2019, 14, e0213940. [Google Scholar] [CrossRef] [PubMed]
- Kirkilesis, G.I.; Kakkos, S.K.; Tsolakis, I.A. Editor’s Choice—A Systematic Review and Meta-Analysis of the Efficacy and Safety of Anticoagulation in the Treatment of Venous Thromboembolism in Patients with Cancer. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 685–701. [Google Scholar] [CrossRef]
- Camilli, M.; Lombardi, M.; Vescovo, G.M.; Del Buono, M.G.; Galli, M.; Aspromonte, N.; Zoccai, G.B.; Niccoli, G.; Montone, R.A.; Crea, F.; et al. Efficacy and safety of novel oral anticoagulants versus low molecular weight heparin in cancer patients with venous thromboembolism: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2020, 154, 1–9. [Google Scholar] [CrossRef]
- Desai, R.; Koipallil, G.K.; Thomas, N.; Mhaskar, R.; Visweshwar, N.; Laber, D.; Patel, A.; Jaglal, M. Efficacy and safety of direct oral anticoagulants for secondary prevention of cancer associated thrombosis: A meta-analysis of randomized controlled trials. Sci. Rep. 2020, 10, 773. [Google Scholar] [CrossRef]
- Sabatino, J.; De Rosa, S.; Polimeni, A.; Sorrentino, S.; Indolfi, C. Direct Oral Anticoagulants in Patients With Active Cancer: A Systematic Review and Meta-Analysis. JACC CardioOncology 2020, 2, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Gyawali, B. Assessing the benefits and harms of direct oral anticoagulants in patients with cancer for the prophylaxis and treatment of venous thromboembolism: A systematic review and meta-analysis. Ecancermedicalscience 2020, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Moik, F.; Posch, F.; Zielinski, C.; Pabinger, I.; Ay, C. Direct oral anticoagulants compared to low-molecular-weight heparin for the treatment of cancer-associated thrombosis: Updated systematic review and meta-analysis of randomized controlled trials. Res. Pract. Thromb. Haemost. 2020, 4, 550–561. [Google Scholar] [CrossRef]
- Goldhaber, S.Z.; Schellong, S.; Kakkar, A.; Eriksson, H.; Feuring, M.; Kreuzer, J.; Fraessdorf, M.; Schulman, S. Treatment of acute pulmonary embolism with dabigatran versus warfarin: A pooled analysis of data from RE-COVER and RE-COVER II. Thromb. Haemost. 2016, 116, 714–721. [Google Scholar] [CrossRef]
- Cohen, A.T.; Bauersachs, R. Rivaroxaban and the Einstein clinical trial programme. Blood Coagul. Fibrinolysis 2019, 30, 85–95. [Google Scholar] [CrossRef]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Gallus, A.S.; Lee, T.C.; Pak, R.; Raskob, G.E.; Weitz, J.I.; Yamabe, T. Oral apixaban for the treatment of venous thromboembolism in cancer patients: Results from the AMPLIFY trial. J. Thromb. Haemost. 2015, 13, 2187–2191. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; Van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an oral factor xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: Results of a randomized trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Ageno, W.; Mantovani, L.G.; Haas, S.; Kreutz, R.; Monje, D.; Schneider, J.; van Eickels, M.; Gebel, M.; Turpie, A.G.G. Subgroup Analysis of Patients with Cancer in XALIA: A Noninterventional Study of Rivaroxaban versus Standard Anticoagulation for VTE. TH Open Companion J. Thromb. Haemost. 2017, 1, e33–e42. [Google Scholar] [CrossRef][Green Version]
- Soff, G.A.; Mones, J.; Wilkins, C.; Devlin, S.; Haegler-Laube, E.; Wills, J.; Sarasohn, D.M.; Juluru, K.; Singer, M.; Miao, Y.; et al. Rivaroxaban treatment of cancer-associated venous thromboembolism: Memorial Sloan Kettering Cancer Center institutional experience. Res. Pract. Thromb. Haemost. 2019, 3, 349–356. [Google Scholar] [CrossRef] [PubMed]
- McBane, R.D.; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. J. Thromb. Haemost. 2020, 18, 411–421. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Grandoni, F.; Alberio, L. Direct oral anticoagulant drugs: On the treatment of cancer-related venous thromboembolism and their potential anti-neoplastic effect. Cancers 2019, 11, 46. [Google Scholar] [CrossRef]
- Riess, H.; Sinn, M.; Kreher, S. CONKO-011: Evaluation of patient satisfaction with the treatment of acute venous thromboembolism with rivaroxaban or low molecular weight heparin in cancer patients. A randomized phase III study. Dtsch. Med. Wochenschr. 2015, 140, S22–S23. [Google Scholar] [CrossRef]
- CASTA-DIVA. ClinicalTrials.gov Identifier: NCT02746185. Available online: https://clinicaltrials.gov/ct2/show/NCT02746185 (accessed on 31 January 2018).
- Khorana, A.A.; Weitz, J.I. Treatment Challenges in Venous Thromboembolism: An Appraisal of Rivaroxaban Studies. Thromb. Haemost. 2018, 118, S23–S33. [Google Scholar] [CrossRef]
- Carrier, M.; Blais, N.; Crowther, M.; Kavan, P.; Le Gal, G.; Moodley, O.; Shivakumar, S.; Tagalakis, V.; Wu, C.; Lee, A.Y.Y. Treatment algorithm in cancer-associated thrombosis: Canadian expert consensus. Curr. Oncol. 2018, 25, 329–337. [Google Scholar] [CrossRef]
- Khorana, A.A.; Noble, S.; Lee, A.Y.Y.; Soff, G.; Meyer, G.; O’Connell, C.; Carrier, M. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2019, 41, 1–61. [Google Scholar] [CrossRef] [PubMed]
- Franco-Moreno, A.; Cabezon-Gutierrez, L.; Palka-Kotlowsa, M.; Villamayor-Delgado, M.; Garcia-Navarro, M. Evaluation of direct oral anticoagulants for the treatment of cancer-associated thrombosis: An update. J. Thromb. Thrombolysis 2019, 47, 409–419. [Google Scholar] [CrossRef]
- Verso, M.; Di Nisio, M. Management of venous thromboembolism in cancer patients: Considerations about the clinical practice guideline update of the American society of clinical oncology. Eur. J. Intern. Med. 2020, 71, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.A.; Gibbs, H.; Merriman, E.; Curnow, J.L.; Young, L.; Bennett, A.; Wee, T.C.; Chunilal, S.D.; Ward, C.M.; Baker, R.; et al. New guidelines from the Thrombosis and Haemostasis Society of Australia and New Zealand for the diagnosis and management of venous thromboembolism. Med. J. Aust. 2019, 210, 227–235. [Google Scholar] [CrossRef]
- Streiff, M.B.; Holmstrom, B.; Angelini, D.; Ashrani, A.; Bockenstedt, P.L.; Chesney, C.; Fanikos, J.; Fenninger, R.B.; Fogerty, A.E.; Gao, S.; et al. NCCN Guidelines® insights cancer-associated venous thromboembolic disease, version 2.2018 featured updates to the NCCN guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2018, 16, 1289–1303. [Google Scholar] [CrossRef] [PubMed]
- Najidh, S.; Versteeg, H.H.; Buijs, J.T. A systematic review on the effects of direct oral anticoagulants on cancer growth and metastasis in animal models. Thromb. Res. 2020, 187, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Featherby, S.; Xiao, Y.P.; Ettelaie, C.; Nikitenko, L.L.; Greenman, J.; Maraveyas, A. Low molecular weight heparin and direct oral anticoagulants influence tumour formation, growth, invasion and vascularisation by separate mechanisms. Sci. Rep. 2019, 9, 1–13. [Google Scholar] [CrossRef]
- Cîmpan, P.L.; Chira, R.I.; Mocan, M.; Anton, F.P.; Farcaş, A.D. Oral Anticoagulant Therapy—When Art Meets Science. J. Clin. Med. 2019, 8, 1747. [Google Scholar] [CrossRef]
- Holster, I.L.; Valkhoff, V.E.; Kuipers, E.J.; Tjwa, E.T.T.L. New oral anticoagulants increase risk for gastrointestinal bleeding: A systematic review and meta-analysis. Gastroenterology 2013, 145, 105–112.e15. [Google Scholar] [CrossRef]
- Angelini, D.E.; Radivoyevitch, T.; McCrae, K.R.; Khorana, A.A. Bleeding incidence and risk factors among cancer patients treated with anticoagulation. Am. J. Hematol. 2019, 94, 780–785. [Google Scholar] [CrossRef]
- Young, A. Cancer Associated Thrombosis: Scope of the Problem; Patient Perspective; 2019. Available online: https://thrombosisuk.org/ (accessed on 31 January 2018).
- Meyer, G. Low-molecular weight heparin or direct oral anticoagulants for the treatment of cancer associated thrombosis. Are we at the crossroad? Thromb. Res. 2019, 173, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2019, 38, 496–520. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Goldhaber, S.Z.; Kearon, C.; Kakkar, A.K.; Schellong, S.; Eriksson, H.; Hantel, S.; Feuring, M.; Kreuzer, J. Treatment with dabigatran or warfarin in patients with venous thromboembolism and cancer. Thromb. Haemost. 2015, 114, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Prins, M.H.; Lensing, A.W.A.; Brighton, T.A.; Lyons, R.M.; Rehm, J.; Trajanovic, M.; Davidson, B.L.; Beyer-Westendorf, J.; Pap, Á.F.; Berkowitz, S.D.; et al. Oral rivaroxaban versus enoxaparin with vitamin K antagonist for the treatment of symptomatic venous thromboembolism in patients with cancer (EINSTEIN-DVT and EINSTEIN-PE): A pooled subgroup analysis of two randomised controlled trials. Lancet. Haematol. 2014, 1, e37–e46. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Segers, A.; Angchaisuksiri, P.; Oh, D.; Boda, Z.; Lyons, R.M.; Meijer, K.; Gudz, I.; Weitz, J.I.; et al. Edoxaban for venous thromboembolism in patients with cancer: Results from a non-inferiority subgroup analysis of the Hokusai-VTE randomised, double-blind, double-dummy trial. Lancet. Haematol. 2016, 3, e379–e387. [Google Scholar] [CrossRef]
- Ramacciotti, E.; Agati, L.B.; Caffaro, R.A.; Volpiani, G.G.; Lopes, R.D.; Comerota, A.J.; Fareed, J. Direct Oral Anticoagulants and Cancer-Associated Thrombosis Management. Where Do We Stand in 2019? Clin. Appl. Thromb. 2019, 25, 1–7. [Google Scholar] [CrossRef]
- Carrier, M.; Soff, G.; Le Gal, G. Treatment of Venous Thromboembolism in Cancer. Historical Perspective and Evolving Role of the Direct Oral Anticoagulants. Cancer Treat. Res. 2019, 179, 103–115. [Google Scholar] [CrossRef]
- Fokin, A.A.; Bagaev, K.V. Venous thromboembolic complications in oncological patients: Present-day possibilities of effective and safe anticoagulant therapy. Angiol. Sosud. Khir. 2019, 25, 19–23. [Google Scholar] [CrossRef]
- Kim, S.A.; Yhim, H.Y.; Bang, S.M. Current management of cancer-associated venous thromboembolism: Focus on direct oral anticoagulants. J. Korean Med. Sci. 2019, 34. [Google Scholar] [CrossRef]
- Graf, C.; Wilgenbus, P.; Pagel, S.; Pott, J.; Marini, F.; Reyda, S.; Kitano, M.; Macher-Göppinger, S.; Weiler, H.; Ruf, W. Myeloid cell-synthesized coagulation factor X dampens antitumor immunity. Sci. Immunol. 2019, 4, 1–14. [Google Scholar] [CrossRef]
- Maqsood, A.; Hisada, Y.; Garratt, K.B.; Homeister, J.; Mackman, N. Rivaroxaban does not affect growth of human pancreatic tumors in mice. J. Thromb. Haemost. 2019, 17, 2169–2173. [Google Scholar] [CrossRef] [PubMed]
- Ay, C.; Beyer-Westendorf, J.; Pabinger, I. Treatment of cancer-associated venous thromboembolism in the age of direct oral anticoagulants. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Delluc, A.; Miranda, S.; Den Exter, P.; Louzada, M.; Alatri, A.; Ahn, S.; Monreal, M.; Khorana, A.; Huisman, M.V.; Wells, P.S.; et al. Accuracy of the Ottawa score in risk stratification of recurrent venous thromboembolism in patients with cancer-associated venous thromboembolism: A systematic review and meta-analysis. Haematologica 2020, 105, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Decousus, H.; Tapson, V.F.; Bergmann, J.F.; Chong, B.H.; Froehlich, J.B.; Kakkar, A.K.; Merli, G.J.; Monreal, M.; Nakamura, M.; Pavanello, R.; et al. Factors at admission associated with bleeding risk in medical patients: Findings from the improve investigators. Chest 2011, 139, 69–79. [Google Scholar] [CrossRef]
- Moik, F.; Pabinger, I.; Ay, C. How i treat cancer-associated thrombosis. ESMO Open 2020, 4, 1–8. [Google Scholar] [CrossRef]
- Grandone, E.; Aucella, F.; Barcellona, D.; Brunori, G.; Forneris, G.; Gresele, P.; Marietta, M.; Poli, D.; Testa, S.; Tripodi, A.; et al. Position paper on the safety/efficacy profile of Direct Oral Anticoagulants in patients with Chronic Kidney Disease: Consensus document of Società Italiana di Nefrologia (SIN), Federazione Centri per la diagnosi della trombosi e la Sorveglianza delle tera. J. Nephrol. 2021, 34, 31–38. [Google Scholar] [CrossRef]
- Riess, H.; Prandoni, P.; Harder, S.; Kreher, S.; Bauersachs, R. Direct oral anticoagulants for the treatment of venous thromboembolism in cancer patients: Potential for drug–drug interactions. Crit. Rev. Oncol. Hematol. 2018, 132, 169–179. [Google Scholar] [CrossRef]
- Bellesoeur, A.; Thomas-Schoemann, A.; Allard, M.; Smadja, D.; Vidal, M.; Alexandre, J.; Goldwasser, F.; Blanchet, B. Pharmacokinetic variability of anticoagulants in patients with cancer-associated thrombosis: Clinical consequences. Crit. Rev. Oncol. Hematol. 2018, 129, 102–112. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Meta-Analysis | Publication Year | Results |
|---|---|---|
| 1. Sardar, P. [7] | 2015; 19,832 pts and 1197 pts. | DOACs administered in patients with cancer were found to be as safe and efficient as is the case in patients without cancer. Rivaroxaban might be effective and safe in patients with cancer, as compared to VKA [6]. |
| 2. Posch, F. [8] | 2015; 3242 pts | DOACs have similar efficacity and safety to LMWH in patients with cancer [7]. |
| 3. Mantha, S. [9] | 2015 | Apixaban appears to be safer than other oral anticoagulants, with a lower risk of bleeding in patients with cancer [8]. |
| 4. Boonyawat, K. [10] | 2017; 98.244 pts | When the influence of body weight on DOAC efficiency was assessed, the results showed that it is not recommended to adjust the doses of DOACs outside the already known limits [9]. |
| 5. Kahale, LA. [11] | 2017; 1486 pts | DOACs do not decrease mortality in cancer patients but may be responsible for more bleeding events [10]. |
| 6. Kahale, LA. [12] | 2018; 5167 | For long-term therapy for cancer-associated thrombotic events, DOACs, as compared to LMWH, may have an efficient antithrombotic effect, but safety issues arise because of an increased risk of major bleeding [11]. |
| 7. Vedovati, MC. [13] | 2018; 1430 pts | In patients with cancer and VTE, DOACs were showed to be safe and efficient as compared to LMWHs [12]. |
| 8. Xing, J. [14] | 2018; 667 pts | Rivaroxaban proved to be efficient and safe as compared to LWMH (enoxaparin for the prevention of recurrent thrombotic events in neoplastic patients). Thus, rivaroxaban was recommended as a therapeutic option for cancer-associated VTE [13]. |
| 9. Martinez, BK. [15] | 2018; 949 pts | Rivaroxaban demonstrated similar levels of safety (rate of major bleeding) and efficiency (recurrent VTE) to the other anticoagulants for patients with cancer-associated VTE. The mortality was lower than reported in many anticoagulation CAT trials [14]. |
| 10. Park, H. [16] | 2018 | For the treatment of cancer-associated VTE, DOACs proved to be safer and more efficient as compared to VKA. DOACs could be one of the standard therapeutic options in neoplastic patients. Among DOACs, apixaban exhibited a better outcome [15]. |
| 11. Hong, Y. [17] | 2018 | Rivaroxaban was associated with a lower hospital admission rate as compared to LWMH [16]. |
| 12. Gómez-Outes, A. [18] | 2018; 29,844 pts | The type of anticoagulation made no difference in the overall survival or causes of death, while the presence of active cancer was associated with a poor outcome and a higher mortality rate [17]. |
| 13. Li, A. [19] | 2019 | DOACs proved to be more effective than LMWHs in secondary prevention of VTE. Unfortunately, DOACs had a low safety profile as a result of increasing the risk of major bleeding and CRNMB, even though the absolute risk differences were small (2–3%). Better compliance with DOACs than LMWHs was hypothesized to explain the differences in bleeding events [18]. |
| 14. Rossel, A. [20] | 2019; 4667 pts | DOACs proved efficient in secondary prevention of VTE in neoplastic patients but showed a low safety profile with an increased risk of bleeding as compared to LMWH [19]. |
| 15. Kirkilesis, GI. [21] | 2019; 6980 pts | DOACs were more effective than LMWHs in preventing VTE recurrence but may carry a higher risk of major bleeding [20]. |
| 16. Massimiliano, Camilli [22] | 2020, 2894 pts | As compared to LMWH, DOACs were associated with a significantly lower risk of VTE recurrence and were not associated with an increased risk of major bleeding; however, they were associated with an increased risk of nonmajor bleeding and gastrointestinal bleeding [21]. |
| 17. Desai, R. [23] | 2020, 18,945 pts | DOACs proved to be more effective in secondary prevention of VTE and were associated with a small risk of CRNMB. DOACs were considered to only be safe in the appropriately selected neoplastic patients [22]. |
| 19. Sabatino, I. [24] | 2020; 2907 pts | DOACs demonstrated similar efficiency and safety to dalteparin in preventing CAT VTE recurrence. However, DOACs were associated with higher rates of nonmajor bleeding as compared with dalteparin, primarily in patients with gastrointestinal malignancies [23]. |
| 20. Desai, A. [25] | 2020; 4341 pts | DOACs were efficient in terms of lowering the risk of VTE or recurrent VTE in patients with cancer but demonstrated safety issues regarding the increased risk in major and nonmajor bleeding events without influencing the survival rate [24]. |
| 21. Molik, F. [26] | 2020; 2894 pts | DOACs for VTE treatment and secondary prophylaxis in neoplastic patients proved to be more effective than LMWH but with safety issues related to major and nonmajor bleeding events, especially in those with digestive cancers [25]. |
| Name of Study | DOAC | Active Cancer Randomization (n) | Efficacy End Point (Recurrent VTE) Rate HR (95% CI) | Safety End Point (Major Bleeding) Rate HR (95% CI) |
|---|---|---|---|---|
| DOAC vs. VKA | ||||
| 1. RE-COVER I/II [27] | Dabigatran | 114 vs. 107 | 3.5% vs. 4.7% 0.74 (0.20–2.7) | 13% vs. 9% 1.48 (0.64–3.4) |
| 2. EINSTEIN-DVT/PE [28] | Rivaroxaban | 258 vs. 204 | 2% vs. 4% 0.62 (0.21–1.79) | 12% vs. 13% 0.82 (0.48–1.38) |
| 3. AMPLIFY [29] | Apixaban | 88 vs. 81 | 3.7% vs. 6.4% 0.56 (0.13–2.37) | 2.3% vs. 5% 0.45 (0.08–2.46) |
| 4. HOKUSAI-VTE [30] | Edoxaban | 85 vs. 77 | 2% vs. 9% 0.30 (0.06–1.51) | 19% vs. 26% 0.66 (0.34–1.27) |
| DOAC vs. LMWH | ||||
| 5. SELECT-D [31] | Rivaroxaban | 203 vs. 203 | 4% vs. 11% 0.43 (0.19–0.99) | 6% vs. 4% 1.83 (0.68–4.96) |
| 6. XALIA [32] | Rivaroxaban | 146 vs. 223 | 3.4% vs. 4.5% | 1.4% vs. 3.6% |
| 7. MSK [33] | Rivaroxaban | 200 | 4.4% | 2.2% |
| 8. ADAM-VTE [34] | Apixaban | 145 vs. 142 | 3.4% vs. 14.1% 0.26 (0.09–0.80) | 0% vs. 2.1% p = 0.9956 |
| 9. HOKUSAI-VTE CANCER [30] | Edoxaban | 522 vs. 524 | 7.9 % vs. 11.3% p = 0.09 | 6.9% vs. 4% p = 0.04 |
| 10. CARAVAGGIO [35] | Apixaban | 576 vs. 579 | 5.6% vs. 7.9% 0.63 (0.37–1.07) | 3.8% vs. 4.0% 0.82 (0.40–1.69) |
| 11. CANVAS [36] | Rivaroxaban, Apixaban, Edoxaban, Dabigatran | 811 | ongoing study | ongoing study |
| 12. CONKO-011 [37] | Rivaroxaban | 450 | ongoing study | ongoing study |
| 13. CASTA-DIVA [38] | Rivaroxaban | 159 | ongoing study | ongoing study |
| 14. COSIMO [39] | Rivaroxaban | 528 | ongoing study | ongoing study |
| Society | Recommendations |
|---|---|
| 1. Treatment algorithm in cancer-associated thrombosis: Canadian expert consensus (2018) [40] | 1. Does not mention anticoagulation counterindications. 2. DOACs are preferred to LMWH if the hemorrhagic risk is low, in the absence of gastrointestinal tumors, genitourinary tumors, and if there are no drug interactions. 3. The treatment is recommended for 3 months with re-evaluation at the end of the treatment for cancer evolution and type (active/inactive). |
| 2. ISTH (2018) [41] | 1. We suggest the use of specific DOACs (edoxaban or rivaroxaban) for acute VTE in patients with cancer who present a low risk of bleeding and no drug–drug interactions with current systemic therapy. LMWHs are considered an acceptable alternative. 2. Currently, edoxaban and rivaroxaban are the only DOACs with RCT evidence when compared to LMWH in cancer populations. 3. We suggest the use of LMWHs in cancer patients with an acute diagnosis of VTE and high risk of bleeding (luminal gastrointestinal cancer, genitourinary tract cancer, bladder or nephrostomy tubes, or in patients with active gastrointestinal mucosal abnormalities, such as duodenal ulcers, gastritis, esophagitis, or colitis). 4. We recommended individualized treatment by including patients’ preferences and values. |
| 3. ESC (2019) [42] | 1. Weight-adjusted subcutaneous LMWH should be considered for the first 6 months over VKAs (IIa A). 2. Edoxaban should be considered as an alternative to LWMH in patients without gastrointestinal cancer (IIa B). 3. Rivaroxaban should be considered as an alternative to LWMH in patients without gastrointestinal cancer (IIa C). 4. Extended anticoagulation (> 6 months) should be considered for an indefinite period or until cancer is cured (IIa B). 5. Incidental PE should be managed as symptomatic PE if it involves segmental or more proximal branches, multiple subsegmental vessels, or a subsegmental vessel in association with confirmed DVT. |
| 4. ACCP (2019) [43] | 1. We suggest the use of specific DOACs for cancer patients with an acute diagnosis of VTE, low risk of bleeding, and no drug–drug interactions with current systemic therapy. LMWHs are an acceptable alternative. 2. Currently, edoxaban and rivaroxaban are the only DOACs with RCT evidence when compared to LMWH in cancer populations. 3. We suggest the use of LMWHs for cancer patients with an acute diagnosis of VTE and a high risk of bleeding (luminal gastrointestinal cancer and genitourinary tract cancer). |
| 5. ASCO (2019) [44] | 1. Initial anticoagulation may involve LMWH, UFH, fondaparinux, or rivaroxaban. LMWH is preferred over UFH for the initial 5–10 days of anticoagulation (evidence quality: high; strength of recommendation: strong) in patients initiating treatment with parenteral anticoagulation. 2. For long-term anticoagulation treatment, LMWH, edoxaban, or rivaroxaban are preferred for at least 6 months because of improved efficacy over VKAs (evidence quality: high; strength of recommendation: strong). 3. Anticoagulation with LMWH, DOACs, or VKAs beyond the initial 6 months should be offered to patients with active cancer, such as those with metastatic disease or those receiving chemotherapy. 4. The insertion of a vena cava filter may be offered as an adjunct to anticoagulation in patients with progression of thrombosis despite optimal anticoagulant therapy. 5. Incidental PE and deep vein thrombosis should be treated in the same manner as symptomatic VTE, given their similar clinical outcomes when compared to cancer patients with symptomatic events. 6. Anticoagulant use is not recommended in order to improve survival in patients with cancer without VTE. |
| 6. Thrombosis and Hemostasis Society of Australia and New Zealand (2019) [45] | 1. For DVT or PE that is provoked by active cancer, treatment with therapeutic LMWH for at least 6 months should be administered (evidence: high; strength of recommendation: strong). 2. Patients with incidental PE should be treated in a similar way to patients with symptomatic cancer-associated thrombosis. 3. Edoxaban and rivaroxaban have been shown to be as efficacious as dalteparin in cancer-related thrombosis, but they are associated with an increased risk of major bleeding or CRNMB and, therefore, can be considered when appropriate. |
| 7. NCCN Guidelines Insights Cancer-Associated Venous Thromboembolic Disease (2019) [46] | 1. For noncatheter-associated DVT or PE, indefinite anticoagulation should be recommended while cancer is active, under treatment, or if risk factors for recurrence persist. 2. Apixaban is an option for anticoagulation in patients with cancer and should be limited to patients who refuse or have compelling reasons to avoid LMWH. 3. LMWH/UFH plus dabigatran is a potential treatment option for cancer-associated VTE and should be limited to those patients who refuse or have compelling reasons to avoid long-term LMWH. 4. LMWH followed by edoxaban is the first option for anticoagulation in cancer-associated VTE. 5. Rivaroxaban is an option for anticoagulation treatment of VTE in patients with cancer. Unlike single-agent apixaban, it is not limited to patients with compelling reasons to avoid LMWH. 6. For catheter-associated thrombosis, anticoagulant therapy should be administered if a catheter is in place. The recommended total duration of the therapy is at least 3 months. |
| Authors | Cancer Model/No. of Animals (Mice) Per Experimental Group | Treatment (Dose, Mode, Duration, and Timing) | Results |
|---|---|---|---|
| DeFeo et al. (2010) [47] | syngeneic; orthotopic breast cancer model/4–10 | Dabigatran [45 mg/kg body weight twice a day (Mon–Fri) or 60 mg/kg once a day (Sat, Sun) by oral gavage for 4 weeks, beginning 1 day before tumor cell injection] | Reduced liver micrometastases (no significant effect on lung micrometastases) |
| Graf et al. (2019) [47] | syngeneic; s.c. fibrosarcoma model/9 | Rivaroxaban [0.4 mg/g chow diet for 8 days, started 14 days after cancer cell inoculation] | ±50% reduction in tumor weight ±70% reduction in no. of macroscopic lung metastases |
| syngeneic; s.c. colorectal cancer model/9–11 | Rivaroxaban [0.4 mg/g chow diet for 9 days, started 12 days after cancer cell inoculation] | ±40% reduction in tumor volume | |
| spontaneous; breast cancer model/28 | Rivaroxaban [0.4 mg/g chow diet for 7 weeks, started from week 13 after birth] | reduction in no. of lung metastases | |
| Sophie Featherby (2019) [48] | syngeneic the chorioallantoic membrane (CAM) model/3 | Apixaban (1 µg/mL) Rivaroxaban (0.6 µg/mL) | Apixaban (1 µg/mL) partially reduced the growth of the implanted tumors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiorescu, R.M.; Mocan, M.; Stoia, M.A.; Barta, A.; Goidescu, C.M.; Chiorescu, S.; Farcaş, A.D. Arguments for Using Direct Oral Anticoagulants in Cancer-Related Venous Thromboembolism. Healthcare 2021, 9, 1287. https://doi.org/10.3390/healthcare9101287
Chiorescu RM, Mocan M, Stoia MA, Barta A, Goidescu CM, Chiorescu S, Farcaş AD. Arguments for Using Direct Oral Anticoagulants in Cancer-Related Venous Thromboembolism. Healthcare. 2021; 9(10):1287. https://doi.org/10.3390/healthcare9101287
Chicago/Turabian StyleChiorescu, Roxana Mihaela, Mihaela Mocan, Mirela Anca Stoia, Anamaria Barta, Cerasela Mihaela Goidescu, Stefan Chiorescu, and Anca Daniela Farcaş. 2021. "Arguments for Using Direct Oral Anticoagulants in Cancer-Related Venous Thromboembolism" Healthcare 9, no. 10: 1287. https://doi.org/10.3390/healthcare9101287
APA StyleChiorescu, R. M., Mocan, M., Stoia, M. A., Barta, A., Goidescu, C. M., Chiorescu, S., & Farcaş, A. D. (2021). Arguments for Using Direct Oral Anticoagulants in Cancer-Related Venous Thromboembolism. Healthcare, 9(10), 1287. https://doi.org/10.3390/healthcare9101287